
Abstract
Short-term heart rate variability (HRV) is increasingly used to assess autonomic nervous system activity and found to be useful for monitoring and providing care due to its quick measurement. With evidence of low HRV associated with chronic diseases, mental disorders, and an increased risk of cardiovascular disease, having normative data of HRV across the age spectrum would be useful for monitoring health and well-being of a population. This study examines HRV of healthy Singapore sample, with ages ranging from 10 to 89 years. Short-term HRV of five minutes was measured from 2,143 participants. 974 males and 1,169 females, and overall HRV was found to be 42.4ms (RMSSD) and 52.0 ms (SDNN) with a further breakdown of HRV by age and gender. Overall HRV declined with age and gender, although gender differences dissipated in the 60s age range onwards, with the 50s age range having the sharpest decline in HRV. Short-term HRV norms were similar to Nunan et al.’s (2010) systematic review in various populations and less similar to Choi et al.’s (2020) study on Koreans.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Stress affects one’s well-being through thoughts, feelings, behaviours, and physiology (Harrington, 2013). It is constantly associated with lifestyle diseases, mental illnesses, and poor performance (Britt et al., 2005; Ramón-Arbués et al., 2020). Yet, stress is characteristic of a Singaporean’s life, permeating across students, working adults, and older adults alike (Cigna 360 Well-being, 2019). In 2019, Singapore reported an annual healthcare expenditure of $3.1 billion on stress-related illnesses (Goh, 2019), which has been further exacerbated by the COVID-19 pandemic (Teo, 2020). Hence, it is necessary to identify reliable measures to monitor stress levels in Singapore to reduce the country’s medical burden.
Stress may be a perception, but it manifests in a person’s physiological state. An objective way of measuring this is via heart rate variability (HRV), which is an indicator of an individual’s emotional response (Appelhans & Luecken, 2006) through the autonomic nervous system’s (ANS’s) ability to adapt to the demands of stress (Wheat & Larkin, 2010). HRV is a reliable indicator of this adaptability as it measures the changes in time between heartbeats (McCraty & Shaffer, 2015). A healthy heart beats with variation, and external demands require the autonomic system to adjust and adapt quickly from homeostasis to meet physical and psychological challenges (Shaffer et al., 2014). Research has established that having high HRV suggests a responsive ANS that copes well with demands of stress, whereas low HRV likely indicates poor responsiveness of the ANS that impedes stress coping (Kim et al., 2018).
Further research has looked at HRV as reflective of cardiac vagal control, which is related to self-regulation and health using the neurovisceral integration model (Thayer et al., 2009); and social interactions using the polyvagal theory (Porges, 2007). Laborde et al. (2018) developed a unifying framework of factors to explain how HRV is related to cardiac vagal control. This framework depicts how three factors, namely, the person, the environment, and the person/environment relationship influence our central autonomic network, which in turn influences our cardiac vagal tone and HRV (Laborde et al., 2018). In sum, HRV is a reliable and objective method to evaluate one’s stress and well-being through the responsiveness of the ANS and the impact on the cardiac vagal tone.
Common indices of HRV are time-domain metrics, which quantify the variability in measurements of the time between successive heartbeats and frequency-domain measurements that estimate absolute or relative power in different frequency bands (Shaffer & Ginsberg, 2017). Based on recommendations by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (Task Force, 1996), the most used time-domain parameters include the standard deviation of all normal-to-normal intervals (SDNN) for overall HRV and the square root of the mean squared differences of consecutive normal-to-normal intervals (RMSSD) for short-term HRV.
The duration of HRV recording is dictated by the nature of the investigation and the metrics used (Task Force, 1996). For instance, 24-hour long-term HRV recording epochs are the “gold standard” for clinical evaluation (Task Force, 1996); five-minute short-term HRV recordings are considered acceptable in evaluating HRV for SDNN, RMSSD, and frequency methods (Task Force, 1996); RMSSD is the most reliable and valid indicator for ultra-short-term (i.e., less than 5 min) HRV recordings for athletes (Esco & Flatt, 2014; Nussinovitch et al., 2011). A high HRV is reflected in increasing values of SDNN and RMSSD, indicating physiological resilience against stress (Kim et al., 2018). HRV has been identified as a powerful predictor of prognosis for the general population (Tsuji et al., 1996) and those with heart conditions (La Rovere et al., 2003) As such, short-term HRV measurements using SDNN, RMSSD, and frequency data would be the most practical indices for tracking the overall health and well-being of Singaporeans.
Similar to heart rate (HR) measurements, HRV is commonly measured using two modalities - electrocardiography (ECG) and photoplethysmography (PPG). Although ECG is the gold standard for measuring HRV, using chemical/electric signals via electrodes with gel makes it cumbersome, costly, and impractical for use in this time-use study (Gilgen-Ammann et al., 2019). In contrast, PPG offers more flexibility and practicality for field settings as it measures HRV using light signals that are common in commercial portable devices, such as finger sensors, smartwatches, smartphone apps and chest bands (Allen, 2007). Additionally, PPG shows similar accuracy compared to ECG for measuring HRV in healthy individuals at rest (Dobbs et al., 2019).
To date, there is no short-term HRV normative data in Singapore. Previous research that measured HRV in Singapore looked at specific groups of people, such as athletes (Ortega & Wang, 2018) and clinical patients (Liu et al., 2021), rather than a broader population. The closest reference for HRV norms in Asia would be a Korean study by Choi, Cha, and Park (2020), albeit having a small sample population. While the study found similar trends of decreasing HRV indices with age that conformed to norms from Western literature, the lack of significant gender differences in any HRV parameters contradicted Western normative data (Koenig & Thayer, 2016; Schroeder et al., 2003). The authors argued that different dietary and lifestyles could affect physiological conditions.
Since lifestyle and environmental factors, such as level of physical activity, stress levels, working time, and exposure to electromagnetic fields generated by electronic devices could affect HRV (Ernst, 2017; Fatisson et al., 2016) and HRV is predictive of both morbidity and mortality (Shaffer & Ginsberg, 2017), HRV indices would provide useful normative data for monitoring health and well-being. This study seeks to identify HRV norms in the Singapore population by employing a short-term HRV time domain measurement using a PPG sensor.
Method
Participants
The national household listing was purchased from the Singapore Department of Statistics and provided the framework for fieldwork operation. Interviewees included all household members aged 10 and above. Respondents between the age of 10 to 20 required written parental consent before seeking assent from the child.
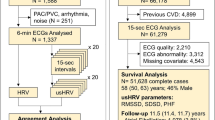
A total of 2,153 out of 3,031 responses was included in this research report. The survey was conducted from November 2021 to December 2022, where 54.9% of the respondents were female, and 45.1% were male. The data of 878 respondents were excluded due to reports of hypertension, diabetes, high cholesterol, obesity, gout, haemorrhoids, urinary incontinence, self-reports of less than four hours of sleep or having too much movement during measurement. Table 1 shows the details of the age ranges for the participants, with participants ranging from 10 to 89 years of age.
Materials and Procedure
A PPG sensor, CorSense, and its accompanying smartphone app (Elite HRV, North Carolina, United States) were used to measure HR and HRV as part of a door-to-door interview study. Elite HRV has proven good validity and reliability in short-term HRV measurements (Chhetri, Shreshtha, & Mahotra, 2022; Moya-Ramon et al., 2022). CorSense utilises an array of optical sensors (i.e., LED emitters, visible spectrum photo detectors, & an infrared detector) to detect RR intervals, which are then received by Bluetooth and processed by the Elite HRV smartphone app (Plews et al., 2017). Due to the scale of the sample and length of survey, interviewers were tasked only to collect the processed values from the Elite HRV app to reduce measurement time and error. The Elite HRV app cleans spurious artifacts and applies natural log and standard deviations to RMSSD and SDNN readings respectively.
Households selected for the survey first received a letter of invitation to participate from the Singapore University of Social Sciences, stating the purpose and contact details of the research. Subsequently, a trained interviewer visited the household in the following one to two weeks to interview the family members. Each interview took approximately 50 min per respondent, and each participant received a supermarket voucher upon completing the survey. HR and HRV data were measured from participants in a standardised seated position, using Elite HRV’s PPG sensor on the participant’s right-hand index finger for five minutes at a specific time point during the interview. Participants were required to be still and quiet and breathe normally during the heart rate measurement. If there were excessive movements during the heart rate data collection, the data was discarded. Participation was strictly voluntary; respondents could choose to withdraw at any time. However, withdrawal before the completion of the survey would deny the participant the incentive.
Results
The average HR of all respondents was 83.7 bpm (SD = 11.0). The overall HRV means were 42.4 ms (SD = 17.0) for RMSSD and 52.0 ms (SD = 19.6) for SDNN. Since heart rate information may be affected by individual characteristics (e.g., age), it is critical to consider such factors during HR data analysis. Specifically, HRV indices correlate negatively with ageing and gender influences HRV (Umetani et al., 1998). Hence, HR data was broken down further by age group and gender as depicted in Tables 2 and 3 as well as Figs. 1 and 2. In sum, HRV trends for males and females gradually declined with ageing for SDNN and RMSSD.

HRV RMSSD by age and gender

HRV SDNN by age and gender
Discussion
This study addresses the need for a larger population study for short-term HRV across the full age spectrum (Taskforce, 1996). Overall, the means for HRV was similar to Nunan et al.’s (2010) systematic review of short-term HRV norms for healthy adults, as depicted in Table 4.
Table 5 shows a comparison of HRV SDNN by age and gender between the Singapore population and the Korean population. Singaporeans have higher HRV scores compared to Koreans. Generally, HRV scores were consistently higher across similar age ranges and both genders in Singapore compared to Korea, although our study includes more participants. Participants from the age range below 20 and above 70 were excluded from this portion of the analysis for a more even comparison.
Similar to past research, HRV time domain measurements declined with age, and women had lower HRV than men across the age ranges, but this difference dissipated from the 60s age range onwards, which is later than the 50s age range in Western populations (Almeida-Santos et al., 2016; Bonnemeier et al., 2003; Shaffer & Ginsberg, 2017; Umetani et al., 1998; Voss et al., 2015). This decrease in HRV is consistent with the decline in cardiac vagal modulation and degeneration of autonomic nervous system functioning that occurs naturally with ageing (Almeida-Santos et al., 2016; Bonnemeier et al., 2003). Further, Bonnemeier et al. (2003) pointed out that the most dramatic decrease in HRV occurs somewhere between the 20 to 30 s age range, but this study found the 50s age range to have the highest HRV decline for Singaporeans. A plausible explanation for this could be related to changes in the age of parenting, with a sandwiched generation of adults caring for both their own children and their own elderly parents (Tan, 2018). Over the last two decades, a delay in Singapore’s birth rate was observed from a birth rate peak in the age range of 25 to 29 in 1980 to a later birth rate peak of the 30 to 34 age range in 2021, signalling later childbirth and parenting in Singapore (Department of Statistics Singapore, 2021). Higher stress and lifestyle changes associated with parenting and caregiving may account for this HRV decline at a later age.
Overall, HRV was generally higher in Singapore compared to the Korean and Japanese across the genders and age ranges. East Asian countries like Japan and Korea tend to have longer working hours than Western countries, with death from overwork (termed karoshi in Japanese) evident in Japan and Korea (Cheng et al., 2012). The long working hours in Japan and Korea could result in higher stress levels, which may explain the lower HRV values for these two East Asian populations.
HRV studies on Korean and Japanese samples found that there were no significant gender differences, unlike the HRV studies on Western populations (Choi et al., 2020; Fukusaki et al., 2000). Interestingly, despite the Singapore sample being an Asian population (like Koreans and Japanese), the HRV gender differences in Singapore were evident and had more similarities with Western populations instead. Choi and colleagues (2020) attributed the lack of gender differences in HRV of the Korean (and potentially Japanese) sample to lifestyle and diet. As Koreans and Japanese are more similar in diet and lifestyle compared to Singaporeans, this could be a reason that differentiates the Singapore population from the Korean and Japanese populations. Further, Wee et al. (2006) found that Singaporean children/adolescents shared a similar notion of quality of life as their Western counterparts, which could potentially shape perspectives and resultant HRV indicators.
Limitations
The limitation in this study was the COVID-19 pandemic, which unfortunately hindered the data collection process. Nevertheless, the data collected during this period is unique as Singapore, like many other countries, was battling COVID-19 through lockdowns and restrictions on social gatherings. The unprecedented time may pose further stressors that may have influenced the findings of this study.
This study used purely time domain HRV. In future studies, it would be useful to explore IBI data and frequency domain measures of HRV like HF. Further, collecting IBI data would be useful in matching the data to Kubios HRV to ensure good validity of the data to confirm validity and reliability as shown by Moya-Roman et al. (2022) and Chhetri et al., 2022).
Implications
HRV of the Singapore sample was clearly more similar to Western samples than other East Asian samples, with overall higher HRV values and marked gender differences noticeable in the Singapore sample. This unique physiological profile is worth further investigation, as Singapore is geographically Asian yet physiologically seemingly more Western than Asian (in terms of autonomic nervous system functioning).
Conclusion
In this study, we uncovered the pulse of Singapore; this is the first study to present HRV norms in the Singapore population. As expected, HRV declined with age and differed by gender up to the 40 years age group. However, it was interesting to see that the Singapore population had HRV norms that were higher than Korean norms despite being an Asian country.
References
Allen, J. (2007). Photoplethysmography and its application in clinical physiological measurement. Physiological Measurement, 28(3), https://doi.org/10.1088/0967-3334/28/3/R01. R1-R39.
Almeida-Santos, M. A., Barreto-Filho, J. A., Oliveira, J. L. M., Reis, F. P., Oliveira, C. C. C., & Sousa, A. C. S. (2016). Ageing, heart rate variability and patterns of autonomic regulation of the heart. Archives of Gerontology and Geriatrics, 63, 1–8. https://doi.org/10.1016/j.archger.2015.11.011.
Appelhans, B. M., & Luecken, L. J. (2006). Heart Rate Variability as an index of regulated emotional responding. Review of General Psychology, 10(3), 229–240. https://doi.org/10.1037/1089-2680.10.3.229.
Bonnemeier, H., Richardt, G., Potratz, J., Wiegand, U. K., Brandes, A., Kluge, N., & Katus, H. A. (2003). Circadian profile of cardiac autonomic nervous modulation in healthy subjects: Differing effects of aging and gender on heart rate variability. Journal of Cardiovascular Electrophysiology, 14(8), 791–799. https://doi.org/10.1046/j.1540-8167.2003.03078.x.
Britt, T. W., Castro, C. A., & Adler, A. B. (2005). Self-engagement, stressors, and health: A longitudinal study. Personality and Social Psychology Bulletin, 31(11), 1475–1486. https://doi.org/10.1177/0146167205276525.
Cheng, Y., Park, J., Kim, Y., & Kawakami, N. (2012). The recognition of occupational diseases attributed to heavy workloads: Experiences in Japan, Korea, and Taiwan. International Archives of Occupational and Environmental Health, 85(7), 791–799. https://doi.org/10.1007/s00420-011-0722-8.
Chhetri, P., Shrestha, L., & Mahotra, N. B. (2022). Validity of Elite-HRV smartphone application for measuring heart rate variability compared to Polar V8000 heart rate monitor. Journal of Nepal Health Research Council, 19(4), 809–813. https://doi.org/10.33314/jnhrc.v19i04.3949.
Choi, J., Cha, W., & Park, M. G. (2020). Declining trends of heart rate variability according to ageing in healthy Asian adults. Frontiers in Ageing Neuroscience. https://doi.org/10.3389/fnagi.2020.610626/full#B15.
Cigna 360 Well-Being Survey: Well and beyond (2019). Retrieved, 1 July 2020, from https://well-being.cigna.com/360Survey_Report.pdf.
Department of Statistics Singapore (2021). Resident households by household living arrangement and age group of youngest child. https://tablebuilder.singstat.gov.sg/table/TS/M810661.
Dobbs, W. C., Fedewa, M. V., MacDonald, H. V., Holmes, C. J., Cicone, Z. S., Plews, D. J., & Esco, M. R. (2019). The accuracy of acquiring heart rate variability from portable devices: A systematic review and meta-analysis. Sports Medicine, 49(3), 417–435. https://doi.org/10.1007/s40279-019-01061-5.
Ernst, G. (2017). Hidden signals—the history and methods of heart rate variability. Frontiers in Public Health, 5(265), 1–12. https://doi.org/10.3389/fpubh.2017.00265.
Esco, M. R., & Flatt, A. A. (2014). Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: Evaluating the agreement with accepted recommendations. Journal of Sports Science & Medicine, 13(3), 535–541. https://doi.org/10.3389/fpsyg.2021.621399.
Fatisson, J., Oswald, V., & Lalonde, F. (2016). Influence diagram of physiological and environmental factors affecting heart rate variability: An extended literature overview. Heart International, 11(1), e32–e40. https://doi.org/10.5301/heartint.5000232.
Fukusaki, C., Kawakubo, K., & Yamamoto, Y. (2000). Assessment of the primary effect of aging on heart rate variability in humans. Clinical Autonomic Research, 10(3), 123–130. https://doi.org/10.1007/BF02278016.
Gilgen-Ammann, R., Schweizer, T., & Wyss, T. (2019). RR interval signal quality of a heart rate monitor and an ECG holter at rest and during exercise. European Journal of Applied Physiology, 119(7), 1525–1532. https://doi.org/10.1007/s00421-019-04142-5.
Goh, T. (2019, November 21). Singapore spends $3.1 billion on stress-related illnesses annually: Study. The Straits Times. https://www.straitstimes.com/singapore/health/singapore-spends-31-billion-on-stress-related-illnesses-annually-study
Harrington, R. (2013). Stress, health, and well-being: Thriving in the 21st century. Cengage Learning.
Kim, H. G., Cheon, E. J., Bai, D. S., Lee, Y. H., & Koo, B. H. (2018). Stress and heart rate variability: A Meta-analysis and review of the literature. Psychiatry Investigation, 15(3), 235–245. https://doi.org/10.30773/pi.2017.08.17.
Koenig, J., & Thayer, J. F. (2016). Sex differences in healthy human heart rate variability: A meta-analysis. Neuroscience & Biobehavioral Reviews, 64, 288–310. https://doi.org/10.1016/j.neubiorev.2016.03.007.
Laborde, S., Mosely, E., & Mertgen, A. (2018). A unifying conceptual framework of factors associated to cardiac vagal control. Heliyon, 4, e01002. https://doi.org/10.1016/j.heliyon.2018.e01002.
La Rovere, M. T., Pinna, G. D., Maestri, R., Mortara, A., Capomolla, S., Febo, O., Ferrari, R., Franchini, M., Gnemmi, M., Opasich, C., Riccardi, P. G., Traversi, E., & Cobelloe, F. (2003). Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation, 107, 565–570. https://doi.org/10.1161/01.cir.0000047275.25795.17.
Liu, N., Chee, M. L., Foo, M. Z. Q., Pong, J. Z., Guo, D., Koh, Z. X., Ho., A. F. W., Niu, C., Chong, S. L., & Ong, M. E. H. (2021). Heart rate n-variability (HRnV) measures for prediction of mortaility in sepsis patients presenting at the emergency department. PLoS One, 16(8), e0249868. https://doi.org/10.1371/journal.pone.0249868.
McCraty, R., & Shaffer, F. (2015). Heart rate variability: New perspectives on physiological mechanisms, assessment of self-regulatory capacity, and health risk. Global Advancements in Health and Medicine, 4(1), 46–61. https://doi.org/10.7453/gahmj.2014.073.
Moya-Ramon, M., Mateo-March, M., Pena-Gonzalez, I., Zabala, M., & Javaloyes, A. (2022). Validity and reliability of different smartphone applications to measure HRV during short and ultra short measurements in elite athletes. Computer Methods and Programs in Biomedicine, 217, 106696. https://doi.org/10.1016/j.cmpb.2022.106696.
Nunan, D., Sandercock, G. H., & Brodie, D. A. (2010). A quantitative systematic review of normal values of short-term heart rate variability in healthy adults. Pacing and Clinical Electrophysiology, 33(11), 1407–1417. https://doi.org/10.1111/j.1540-8159.2010.02841.x.
Nussinovitch, U., Elishkevitz, K. P., Katz, K., Nussinovitch, M., Segev, S., Volovitz, B., & Nussinovitch, N. (2011). Reliability of Ultra-Short ECG indices for heart rate variability. Annals of Noninvasive Electrocardiology: The Official Journal of the International Society for Holter and Noninvasive Electrocardiology Inc, 16(2), 117–122. https://doi.org/10.1111/j.1542-474X.2011.00417.x.
Ortega, E., & Wang, C. K. J. (2018). Pre-performance psychophysiological state: Heart rate variability as a predictor of shooting performance. Applied Psychophysiology and Biofeedback, 43(1), 75–85. https://doi.org/10.1007/s10484-017-9386-9.
Plews, D. J., Scott, B., Altini, M., Wood, M., Kilding, A. E., & Laursen, P. B. (2017). Comparison of heart-rate-variability recording with smartphone photoplethysmography, polar H7 chest strap, and electrocardiography. International Journal of Sports Physiology and Performance, 12(10), 1324–1328. https://doi.org/10.1123/ijspp.2016-0668.
Porges, S. (2007). The polyvagal perspective. Biological Psychology, 74, 116–143. https://doi.org/10.1016/j.biopsycho.2006.06.009.
Ramón-Arbués, E., Gea-Caballero, V., Granada-López, J. M., Juárez-Vela, R., Pellicer-García, B., & Antón-Solanas, I. (2020). The prevalence of depression anxiety and stress and their associated factors in college students. International Journal of Environmental Research and Public Health, 17(19), 7001. https://doi.org/10.3390/ijerph17197001.
Schroeder, E. B., Liao, D., Chambless, L. E., Prineas, R. J., Evans, G. W., & Heiss, G. (2003). Hypertension blood pressure and heart rate variability. Hypertension, 42(6), 1106–1111. https://doi.org/10.1161/01.HYP.0000100444.71069.73.
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 358. https://doi.org/10.3389/fpubh.2017.00258.
Shaffer, F., McCraty, R., & Zerr, C. L. (2014). A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Frontiers in Psychology, 5(1040), 1–19. https://doi.org/10.3389/fpsyg.2014.01040.
Tan, P. L. (2018). Dual burdens of care: Sandwiched couples in East Asia. Journal of Aging and Health, 30(10), 1574–1594. https://doi.org/10.1177/0898264318796061.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996). Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. European Heart Journal, 17(3), 354–381. https://doi.org/10.1161/01.CIR.93.5.1043.
Teo, J. (2020, August 20). Some driven to breaking point by stress during Covid-19 pandemic.The Straits Times. https://www.straitstimes.com/singapore/health/driven-to-breaking-point-by-stress-during-pandemic.
Thayer, J. F., Hansen, A. L., Saus-Rose, E., & Johnsen, B. H. (2009). Heart rate variability, prefrontol neural function, and cognitive performance: The neurovosceral integrative perspective on self-regulation, adaption, and health. Annals in Behaviour Medicine, 37, 141–153. https://doi.org/10.1007/s12160-009-9101-z.
Tsuji, H., Larson, M. G., Venditti, F. J., Manders, E. S., Jr, Evans, J. C., Feldman, C. L., & Levy, D. (1996). Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study Circulation, 94, 2850–2855. https://doi.org/10.1161/01.cir.94.11.2850.
Umetani, K., Singer, D. H., McCraty, R., & Atkinson, M. (1998). Twenty-four hour time domain heart rate variability and heart rate: Relations to age and gender over nine decades. Journal of the American College of Cardiology, 31(3), 593–601. https://doi.org/10.1016/S0735-1097(97)00554-8.
Voss, A., Schroeder, R., Heitmann, A., Peters, A., & Perz, S. (2015). Short-term heart rate variability—influence of gender and age in healthy subjects. PloS One, 10(3), e0118308. https://doi.org/10.1371/journal.pone.0118308.
Wee, H. L, Chua, H. X., & Li, S. C. (2006). Meaning of health-related quality of life among children and adolescents in an Asian country: A focus group approach. Quality of Life Research, 15(5), 821–831. https://doi.org/10.1007/s11136-005-5092-9.
Wheat, A. L., & Larkin, K. T. (2010). Biofeedback of heart rate variability and related physiology: A critical review. Applied Psychophysiology and Biofeedback, 35, 229–242. https://doi.org/10.1007/s10484-010-9133-y.
Acknowledgements
This study was funded by the National Council of Social Services, Singapore, and Ngee Ann Kongi, Singapore, and is part of the NCSS-NAK 360 Panel Study. NCSS does not endorse any analysis, conclusions, methods, or results created wholly by the institution in any way, and that any such analysis, conclusion, methods, or results, are strictly the Institution’s own.
Author information
Authors and Affiliations
Contributions
The corresponding author wrote the main text in the manuscript and analysed the data.Bryan Chan prepared the figures and tables and analysed the data.Christine Ng wrote the main text in the manuscript and checked all references.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ortega, E., Bryan, C.Y.X. & Christine, N.S.C. The Pulse of Singapore: Short-Term HRV Norms. Appl Psychophysiol Biofeedback 49, 55–61 (2024). https://doi.org/10.1007/s10484-023-09603-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-023-09603-4