
Abstract
This study examined the role of gender on short-term heart rate variability (HRV) and the correlation between subjective ratings of stress and HRV in healthy adults. Standardized short-term HRV measurement and self-administered stress response inventory (SRI) were obtained in 441 healthy women and 1440 healthy men. Hierarchical multiple regressions suggested that there was no gender by stress interaction in explaining HRV. However, there were significant gender differences in the associations between stress and HRV (the standard deviation of the NN interval (SDNN), high frequency (HF), low frequency (LF)/HF (F(1, 1878) = 7.706, p < .01; F(1, 1878) = 29.132, p < .01; F(1, 1878) = 49.685, p < .01). In men, only HF (r = −.56, p = .031) showed such an association; whereas in women, the SRI total scores were negatively correlated with SDNN (r = −.103, p = .032), total power (TP) (r = −.104, p = .030), and HF (r = −.129, p = .007), and positively correlated with LF/HF (r = .111, p = .020) when adjusted for age, alcohol drinking, smoking, and caffeine intake. There are gender differences in the association between psychological stress response and HRV. Gender also showed a significant impact on short-term HRV measurement. Given that both clinicians and researchers are increasingly relying on HRV assessment, our work suggest that gender based norms are very important.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There are many ways of characterizing physiologic responses to stressors (Burchfield 1979). One of the more intriguing ones is to examine heart rate variability (HRV), because such measures provide a perspective on both sympathetic and parasympathetic nervous system functioning (Friedman and Thayer 1998). HRV is defined as ‘the amount of fluctuations from the mean heart rate’ and is primarily controlled by the continuous interplay of the autonomic nervous system (ANS). Two frequency components are usually distinguished in short-term HRV: the high frequency (HF) and the low frequency (LF) components (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996a, b).
Several studies have investigated the relationship between stress and HRV. Sloan and his colleagues (Sloan et al. 1994) reported that psychological stress was significantly associated with an increase in the LF/HF which suggests an increase in the relative predominance of sympathetic nervous system activity. Dishman and his colleagues (Dishman et al. 2000) reported that there was an inverse relationship between perceived emotional stress during the past week and the normalized HF component of the HRV, which suggests a lower cardiac vagal component of the HRV in those who perceived more stress. However, most such studies have been conducted in relatively small samples. A study with larger sample size has the advantage of being able to control for other sources of variance, such as obesity, etc.
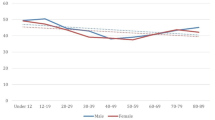
There may be gender differences in terms of autonomic regulation of heart rate responses to stressors. However, there are few studies examining this issue and the findings are not consistent. For example, a recent study using stimulation tests showed differential pattern by gender (Zhang 2007). Another study showed that HRV indices decreased with increasing age, but differed by gender, and the HF, root mean square of successive differences (RMSSD) and the percentage of successive RR interval differences >50 ms (PNN50) were greater in women in all age groups (Antelmi et al. 2004). Sato and Miyake found that male participants were more sympathetic dominant than the female participants (Sato and Miyake 2004). Also for healthy subjects, LF power, and the LF/HF were significantly higher for male than for female (Bigger et al. 1995). These findings suggest that HRV assessment should be indexed according to gender (Zhang 2007).
This paper examined the relationship between stress and HRV in men and women; however, such an analysis is complicated by the fact that women are more likely to report symptoms of emotional distress than men are. In addition, women scored significantly higher than the men on somatic symptoms and psychological stress (Matud 2004).
Recently, many health promotion centers in Korea have attempted to measure both psychological stress and autonomic nervous function during routine medical check-ups with a view to applying these data to patients’ medical care. The authors evaluated the effects of gender on the association between psychological stress response and various parameters of the short-term HRV measurements in a large sample of healthy controls. We also analyzed the impact of gender on short-term HRV measurements and the correlation between psychological stress and the HRV measurements.
Methods
Subjects
1970 male and female 18–65 years of age were recruited while they were visiting five health promotion centers for annual medical check-up in South Korea. All participants provided written informed consent after being given a complete explanation of this study and were screened for medications and medical and psychiatric conditions. Sixty-five participants who had past or current histories of major medical disorders were excluded (hypertension 47, myocardial infarction or angina 2, valvular heart disease 1, diabetes mellitus 11, cancer 2, and hyperthyroidism 2). Seven participants who had histories of major psychiatric disorders were also excluded (depression 6 and panic disorder 1). Psychiatric diagnoses were assessed using the Mini-International-Neuropsychiatric Interview (M.I.N.I.) (Sheehan et al. 1998) by an experienced psychiatrist. After the measurement of the HRV, 17 participants who had abnormally high standard deviation of the NN interval in the HRV (≥100, 3 standard deviations), were excluded from the analysis. However, the analysis included normal subjects who have possibility to show artefacts which are well-known to seriously impact spectral analysis of HRV. Since this study obtains sufficient examples, even if ectopic beats are shown in some cases during any given 5 min recording, artefacts problems would be compensated. Therefore, the final analysis included 441 women and 1440 men who had complete measurements of HRV and self-rating scales of the psychological stress. The study was approved by Institutional Review Board of the Inje University Seoul Paik Hospital.
Measurement of Heart Rate Variability
All subjects were instructed not to consume alcohol or caffeinated beverages after 10 p.m. on the night before HRV measurement. In addition, they refrained from smoking 1 h prior to measurement. To control for diurnal variation, HRV was measured between 8 and 12 a.m. HRV was recorded using SA-2000E model (Medi-core, Seoul, Korea). Each subject was comfortably seated on a chair, and electrodes were placed on their wrists and left foot to derive HRV for five minutes, and subjects were guided to breathe in their usual rate during the HRV measurement.
The following HRV measures were obtained. The standard deviation of the normal-to-normal interval (SDNN) was used to estimate long-term components of the HRV. It is calculated by statistical time domain measures. Total power (TP), LF, HF components of the HRV were calculated by frequency domain spectral analysis (Slaap et al. 2002). TP means the variance of NN interval over temporal segment. The LF/HF ratio was calculated because it has been suggested to reflect sympatho-vagal balance or to reflect sympathetic modulations (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996a).
Assessment of Psychological Stress Responses
Psychological responses to stressors were measured with the Stress Response Inventory (SRI) (Koh et al. 2001) which is a self-administered questionnaire including emotional, somatic, cognitive and behavioral stress responses. SRI consists of 39 items, which are expressed as Likert points: ‘Not at all’ (0 point), ‘Somewhat’ (1 point), ‘Moderately’ (2 points), ‘Very much’ (3 points), and ‘Absolutely’ (4 points). It contains seven subscales: tension, aggression, somatization, anger, depression, fatigue and frustration. High scores on the SRI indicate more subjective stress. Cronbach’s α for the seven subscales ranged between 0.76–0.91 and 0.97 for total scores. SRI is regarded as a reliable and valid measure of stress (Kim et al. 2007; Koh et al. 2006; Lee et al. 2008). All participants filled out the SRI following measurement of the HRV.
Statistical Analysis
As the HRV variables were skewed from normal distribution, natural log transformation was done before statistical analysis. Partial correlation analysis was used to adjust for age, alcohol drinking, smoking, and caffeine intake in order to determine the relationship between the SRI scores and the HRV variables.
Hierarchical regressions were done to test explicitly whether there was a significant interaction effect of SRI score and gender on HRV. We treated HRV as a dependent variable, SRI as an independent variable, and gender as a dummy variable. First, the SRI score was entered into the equation, then gender, and finally, the interaction of SRI score and gender. The hierarchical procedure enabled an examination of unique contribution of gender above that obtained using SRI score as well as the contribution of the interaction. All statistical analysis was performed using the SPSS 12.0 for Windows (SPSS Inc., Korea) program.
Results
The mean age of subjects was 40.31 ± 8.57 years (ranged from 18 to 65). The mean age of women subjects was 36.74 ± 9.01 years and that of men was 41.4 ± 8.1 years. Ninety-four percent of the subjects had educational attainments equal to and higher than those of high school graduate. Among 441 women subjects, 143 (32.4 %) were smokers, 145 (32.9 %) reported drinking alcohol more than once a month, and 325 (73.7 %) consumed coffee regularly. And 1440 men subjects, 990 (68.8 %) were smokers, 969 (67.3 %) reported drinking alcohol more than once a month, and 1158 (80.4 %) consumed coffee regularly (Table 1). (χ 2 = 185.968, p < .01; χ 2 = 165.549, p < .01; χ 2 = 9.141, p < .01) Also, the SRI scores were presented in Table 2.
The partial correlations between SRI scores and HRV variables, with the adjustment of age, alcohol drinking, smoking, and caffeine intake were founded. In men, the correlation between SRI scores and HRV variables was significant only for HF (r = −.056, p = .031). However, in women, the SRI total scores were negatively correlated with SDNN (r = −.103, p = .032), TP (r = −.104, p = .030), and HF (r = −.129, p = .007), respectively, and positively correlated with LF/HF ratio (r = .111, p = .020).
In women, correlations between SRI subscale scores and HRV variables, SDNN and TP showed negative correlations with tension, somatization, anger, and fatigue. HF had negative correlations with tension, somatization, anger, fatigue, and frustration. LF/HF ratio had positive correlations with aggression, anger, depression, and fatigue.
Hierarchical regressions analyses are summarized in Table 3, 4, 5, 6 and 7. We analyzed the SRI-gender interaction in model 3 for all of the hierarchical regressions analyses and in no instance was this interaction significant (∆F(1, 1877) = .550, p > .05; ∆F(1, 1877) = .541, p > .05; ∆F(1, 1877) = .768, p > .05; ∆F(1, 1877) = .020, p > .05; ∆F(1, 1877) = 1.561, p > .05).
However, for SDNN, HF, LF/HF, the addition of gender in model 2 was significant (∆F(1, 1878) = 7.706, p < .01; ∆F(1, 1878) = 29.132, p < .01; ∆F(1, 1878) = 49.685, p < .01).
Discussion
This study focused on the effects of stress and gender on HRV based on previous studies which suggested that gender differences may affect the relationship between stress and HRV (Sloan et al. 1994). Hierarchical regression indicated that there was no significant interaction effect of SRI score and gender on HRV. However, gender accounted for unique variance in HRV except for TP and LF, which supports previous studies suggesting the significant effect of gender on HRV. When we separately analyzed the correlation between SRI scores and HRV variables for men and women, only HF was correlated with SRI scores in the men, whereas in the women, SRI scores were significantly correlated with many HRV variables although the correlation coefficients were not strong.
We focused on studying how stress responses are related to vagal activity in women because they have a higher prevalence of depressive disorders and anxiety disorders and because there was no significant correlation between SRI scores and HRV variables in men.
First, The SRI total scores were negatively correlated with the SDNN and TP. The SDNN, which is mathematically equal to TP of spectral analysis (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996b), may be associated with clinical conditions characterized by an autonomic imbalance in healthy women. Therefore, these results suggest that higher psychological stress levels are negatively correlated with lower SDNN, which indicates a diminished vagal and increased sympathetic modulation of sinus node (Lombardi 2002).
Secondly, the SRI total scores are negatively correlated with HF and positively correlated with LF/HF ratio. As the HF component is mediated by cardiac vagal tone, these results suggest that higher psychological stress levels are correlated with diminished cardiac vagal activities. Finally, The SRI total scores were not correlated with LF. Some studies suggest that LF, when expressed in normalized units, is a quantitative marker for sympathetic activity (Malliani et al. 1991; Rimoldi et al. 1990) whilst other studies found that LF would be mediated by both branches of ANS (Akselrod et al. 1981; Pomeranz et al. 1985). The meaning of HRV parameters related with sympathetic and parasympathetic nervous system functioning is controversial (Parati et al. 2006).
Koh et al. (2001) suggested that the SRI consists of seven subscales i.e. tension, aggression, somatization, anger, depression, fatigue and frustration. In this study, tension, somatization, anger and fatigue as stress responses were more related to HRV variables, while aggression, depression, and frustration are less related. These findings may be inconsistent with previous studies which showed that aggression, depression, and frustration were related to cardiac autonomic imbalance (Garcia-Leon 2003; Mezzacappa et al. 1996; Nahshoni et al. 2004). However, it is intriguing to note the methodological differences between our study and the previous studies, in that Mezzacappa et al. (1996) studied solely male adolescents and Garcia-Leon et al. (2003) studied HRV after subjects performed two cognitive tasks. We also noted the association between HRV and fatigue. Tran et al. (2009) recently reported that high fatigue levels were associated with increased low-frequency HRV, while indices of parasympathetic modulation such as RMSSD and pNN50 remained stable, suggesting that fatigue in healthy individuals may be associated with increased sympathetic arousal. In addition, employing multiple regression analyses, we found that the LF/HF ratio in response to stress was associated with emotional stability, warmth and tension, and was negatively associated with social boldness and self-reported levels of vigor (Tran et al. 2009).
SRI measures different aspects of stress. Our findings suggest that the physical stress subscales of SRI were particularly related with HRV. Accordingly, more precise studies will be needed to determine the relationship between cognitive components of stress responses and cardiac autonomic imbalances. This study has strength in a relatively large sample size and we have made efforts to adjust for various confounding lifestyle factors such as alcohol drinking, smoking, and caffeine intake in the statistical analysis. These adjustments are important because previous studies demonstrated that HRV would be affected by alcohol, nicotine, and caffeine intake (Eryonucu et al. 2000; Rajan et al. 1998; Waring et al. 2003).
We should bear some limitations in mind in this study. First, the magnitude of the correlation coefficients was relatively low. Secondly, while acute intake of caffeine was refrained before measuring the HRV, chronic consumption of caffeine, which might affect the physiological level of autonomic function, could not be controlled. We merely assessed the caffeine use or not in the study and perhaps had we measured caffeine and smoking as continuous variables, the findings might be different. Further studies will be needed to involve detailed descriptions in these items such as the duration and amount of intake. Lastly, the administered psychometric instrument and medical and psychiatric histories were only self-reported, which may reflect a one-directional viewpoint.
Despite these limitations, this study suggests that the HRV may reflect the changes of autonomic nervous system responding to stress in healthy women. There was no significant interaction effect of SRI score-gender for this study, but this study can be of value because it used a relatively large sample to test the relationship between gender and HRV. It is quite interesting that many HRV variables showed significant correlations with SRI scores—but only in women. One can speculate that women perceive stress symptoms more readily than men and that men are less keen to report stress. Similarly, women are more likely to express emotional complaints and men, in contrast, are less likely to express full range of emotion. As a result, there is a range restriction of emotion expression in men. There may thus be less statistical power in perceiving the relationship between stress and HRV in men, because they are not as accurate in perceiving stress and are less responsive to stressors.
Women show a broader range of emotional expression, and it may facilitate the statistical detection of the relationship between stress and HRV. In contrast, the narrower range of emotional expression in men may make it less likely to perceive the relationship between stress and HRV.
In conclusion, gender difference should be considered when we measure, interpret, and apply the results of the short-term HRV and psychological stress response to manage stress levels among health adults. Further studies on important variables such as age, obesity, health-related habits, and the presence of chronic illness, are warranted.
References
Akselrod, S., Gordon, D., Ubel, F. A., Shannon, D. C., Berger, A. C., & Cohen, R. J. (1981). Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science, 213, 220–222.
Antelmi, I., De Paula, R., Shinzato, A., Peres, C., Mansur, A., & Grupi, C. (2004). Influence of age, gender, body mass index, and functional capacity on heart rate variability in a cohort of subjects without heart disease. The American Journal of cardiology, 93, 381–385.
Bigger, J. T, Jr, Fleiss, J. L., Steinman, R. C., Rolnitzky, L. M., Schneider, W. J., & Stein, P. K. (1995). RR variability in healthy, middle-aged persons compared with patients with chronic coronary heart disease or recent acute myocardial infarction. Circulation, 91, 1936–1943.
Burchfield, S. R. (1979). The stress response: A new perspective. Psychosomatic Medicine, 41, 661–672.
Dishman, R. K., Nakamura, Y., Garcia, M. E., Thompson, R. W., Dunn, A. L., & Blair, S. N. (2000). Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. International Journal of Psychophysiology, 37, 121–133.
Eryonucu, B., Bilge, M., Guler, N., Uzun, K., & Gencer, M. (2000). Effects of cigarette smoking on the circadian rhythm of heart rate variability. Acta Cardiologica, 55, 301–305.
Friedman, B. H., & Thayer, J. F. (1998). Anxiety and autonomic flexibility: A cardiovascular approach. Biological Psychology, 49, 303–323.
Garcia-Leon, A., del Paso, G. A. R., Robles, H., & Vila, J. (2003). Relative effects of harassment, frustration, and task characteristics on cardiovascular reactivity. International Journal of Psychophysiology, 47, 159–173.
Kim, J., Youn, C. H., Woo, J. M., Jung, S., & Kim, D. (2007). Association of heart rates with stress response inventory scores in different age groups. In Conference proceedings of IEEE engineering in medicine and biology society, 2007, (pp. 5752–5754).
Koh, K. B., Choe, E., Song, J. E., & Lee, E. H. (2006). Effect of coping on endocrinoimmune functions in different stress situations. Psychiatry Research, 143, 223–234.
Koh, K. B., Park, J. K., Kim, C. H., & Cho, S. (2001). Development of the stress response inventory and its application in clinical practice. Psychosomatic Medicine, 63, 668–678.
Lee, S. H., Choi, H., Kim, S., Choi, T. K., Lee, S., Kim, B., et al. (2008). Association between anger and first-onset primary spontaneous pneumothorax. General Hospital Psychiatry, 30, 331–336.
Lombardi, F. (2002). Clinical implications of present physiological understanding of HRV components. Cardiac Electrophysiology Review, 6, 245–249.
Malliani, A., Pagani, M., Lombardi, F., & Cerutti, S. (1991). Cardiovascular neural regulation explored in the frequency domain. Circulation, 84, 482–492.
Matud, M. (2004). Gender differences in stress and coping styles. Personality and Individual Differences, 37, 1401–1415.
Mezzacappa, E., Tremblay, R. E., Kindlon, D., Saul, J. P., Arseneault, L., Pihl, R. O., & Earls, F. (1996). Relationship of aggression and anxiety to autonomic regulation of heart rate variability in adolescent males. Annals of the New York Academy of Sciences, 794, 376–379.
Nahshoni, E., Aravot, D., Aizenberg, D., Sigler, M., Zalsman, G., Strasberg, B., et al. (2004). Heart rate variability in patients with major depression. Psychosomatics, 45, 129–134.
Parati, G., Mancia, G., Rienzo, M., Castiglioni, P., Taylor, J., & Studinger, P. (2006). Point: Counterpoint: Cardiovascular variability is/is not an index of autonomic control of circulation. Journal of Applied Physiology, 101, 676.
Pomeranz, B., Macaulay, R. J., Caudill, M. A., Kutz, I., Adam, D., Gordon, D., et al. (1985). Assessment of autonomic function in humans by heart rate spectral analysis. American Journal of Physiology, 248, H151–H153.
Rajan, I., Murthy, P. J., Ramakrishnan, A. G., Gangadhar, B. N., & Janakiramaiah, N. (1998). Heart rate variability as an index of cue reactivity in alcoholics. Biological Psychiatry, 43, 544–546.
Rimoldi, O., Pierini, S., Ferrari, A., Cerutti, S., Pagani, M., & Malliani, A. (1990). Analysis of short-term oscillations of R–R and arterial pressure in conscious dogs. American Journal of Physiology, 258, H967–H976.
Sato, N., & Miyake, S. (2004). Cardiovascular reactivity to mental stress: relationship with menstrual cycle and gender. Journal of Physiological Anthropology and Applied Human Science, 23, 215–223.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., et al. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59(Suppl 20), 22–33. (quiz 34–57).
Slaap, B., Boshuisen, M., Van Roon, A., & den Boer, J. (2002). Heart rate variability as predictor of nonresponse to mirtazapine in panic disorder: A preliminary study. International Clinical Psychopharmacology, 17, 69–74.
Sloan, R. P., Shapiro, P. A., Bagiella, E., Boni, S. M., Paik, M., Bigger, J. T, Jr, et al. (1994). Effect of mental stress throughout the day on cardiac autonomic control. Biological Psychology, 37, 89–99.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996a). Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. European Heart Journal, 17, 354–381.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996b). Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation, 93, 1043–1065.
Tran, Y. W. N., Tarvainen, M., Karjalainen, P., & Craig, A. (2009). The relationship between spectral changes in heart rate variability and fatigue. Journal of Psychophysiology, 23, 143–151.
Waring, W. S., Goudsmit, J., Marwick, J., Webb, D. J., & Maxwell, S. R. (2003). Acute caffeine intake influences central more than peripheral blood pressure in young adults. American Journal of Hypertension, 16, 919–924.
Zhang, J. (2007). Effect of age and sex on heart rate variability in healthy subjects. Journal of Manipulative and Physiological Therapeutics, 30, 374–379.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Woo, JM., Kim, TS. Gender Plays Significant Role in Short-Term Heart Rate Variability. Appl Psychophysiol Biofeedback 40, 297–303 (2015). https://doi.org/10.1007/s10484-015-9295-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-015-9295-8