
Abstract
Mental health comorbidities are prevalent among young Black gay, bisexual, and other men who have sex with men (YB-GBMSM) living with HIV and can adversely impact HIV-related outcomes. We conducted a cross-sectional survey study with 100 YB-GBMSM recruited from two HIV care centers in Atlanta, and constructed multivariable logistic and linear regression models to examine correlates of depression, anxiety, trauma symptoms, and general well-being. In adjusted models, full-time employment was associated with fewer depressive symptoms, while HIV stigma and substance use were associated with higher levels of depressive symptoms. Younger age and full-time employment were negatively associated with severe anxiety, while HIV stigma was positively associated with severe anxiety and trauma symptoms. Trust in physicians, lower HIV stigma, full-time employment, and lack of substance use were associated with higher average general well-being scores. In conclusion, we found high frequency of depressive, anxiety, and trauma-related symptoms among this sample of YB-GBMSM living with HIV. Unemployment, substance use, and HIV stigma emerged as particularly salient correlates of psychological morbidity, suggesting a need for structural and community-level interventions to address mental health in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
HIV disproportionately impacts young Black gay, bisexual, and other men who have sex with men (YB-GBMSM) in the United States (US). According to projections, an estimated 40% of YB-GBMSM could be living with HIV by the time they turn 30 years of age [1]. Although current HIV treatments effectively prevent morbidity and mortality [2, 3], YB-GBMSM are at high risk for disengagement across the HIV care continuum, leading to lower rates of viral suppression than other demographic groups [4, 5], and increased risk of downstream adverse health outcomes.
YB-GBMSM who are living with HIV, particularly in the Southern US, face myriad obstacles to their health and well-being. Myers’ Lifespan Biopsychosocial Model of Cumulative Vulnerability and Minority Health postulates that race/ethnicity and socioeconomic factors shape exposure to psychosocial adversities (e.g., life events and stressors), which in turn operate through psychosocial reserve capacity, health behaviors, and healthcare access to influence health status among minority populations [6]. In line with this model, key barriers known to deter sustained HIV care engagement and contribute to compromised health outcomes among YB-GBMSM include structural factors such as systemic racism within and outside of healthcare settings, and conservative cultural norms that promote pervasive stigma against sexual minorities and/or people living with HIV [7,8,9]. The US South also has higher rates of poverty and lower health service accessibility relative to the rest of the country, with Black communities often experiencing a disproportionate burden of these problems. Collectively, structural barriers and intersectional stigmas also contribute to the psychological stress burden of YB-GBMSM living with HIV, thereby increasing vulnerability to co-occurring mental health conditions that may further complicate their engagement in HIV care [9,10,11,12,13].
Mental health comorbidities, including depression, anxiety, and trauma and stress-related symptoms, are prevalent among people living with HIV [14,15,16,17]. These problems can adversely affect clinical management of HIV disease across the continuum of care. For example, depression impedes medication adherence [18,19,20], retention in care [21], and viral suppression [20, 22,23,24]. Anxiety and trauma/stress-related symptoms similarly complicate HIV care engagement and health outcomes [16, 17]. To date, most of the research in this area has focused on general adult HIV populations, with comparatively little systematic investigation of mental health problems specifically among YB-GBMSM living with HIV [25,26,27]. Given the unique challenges and barriers affecting HIV care engagement among YB-GBMSM, and the importance of addressing co-occurring mental health conditions as a component of comprehensive HIV health service delivery for this population, we sought to quantify prevalence and correlates of depression, anxiety, traumatic stress, and general psychological distress and well-being in a sample of YB-GBMSM engaged in HIV care.
A secondary study aim was to explore potential correlates of mental health outcomes in our population of interest. For this purpose, we examined factors relating to the major constructs of the lifespan biopsychosocial model, including socioeconomic status (SES), psychosocial adversities, psychosocial reserve capacity, health behaviors, and factors relating to healthcare access. We hypothesized that lower SES (including income, employment, and education factors) and/or housing instability as well as HIV stigma would expose YB-GBMSM to psychological adversity, which along with substance use (as a health behaviors factor), and discrimination in medical settings and low trust in physicians (as healthcare access factors) would be associated with adverse mental health outcomes (depressive symptoms, anxiety symptoms, trauma symptoms) and negatively associated with general well-being (see Fig. 1). We also hypothesized that religious involvement as a psychosocial reserve capacity factor would serve as a potential buffer associated with positive mental health outcomes.

Conceptual model (based on lifespan biopsychosocial model)
Methods
We conducted a cross-sectional survey among 100 YB-GBMSM living with HIV recruited from two HIV care centers in Atlanta, Georgia between November 2019 and July 2020. YB-GBMSM patients were recruited from the two clinics by either: (1) directly approaching them in the clinic before or after appointments, with the permission of their clinical providers; or (2) by phone when referred to us by clinic staff, or (3) contacting individuals who had participated in prior studies and expressed interest in future research involvement. Eligible individuals were between 18 and 29 years of age and self-reported Black race, male gender identity, any history of consensual sex with men, living with HIV, and receiving care at one of the two participating clinics. Patients recruited by phone were screened and, if eligible, e-mailed a link to a REDCap [28] survey for self-administration at their convenience. Those recruited and screened in-person completed electronic informed consent and self-administered the survey on a study laptop or tablet. All participants received a $25 gift card upon completion of the survey. The study received institutional review board approval.
Mental Health Symptom Measures
Depressive Symptoms
We measured depressive symptoms using the Centers for Epidemiologic Studies Depression-Revised (CESD-R) scale [29, 30]. The CESD-R is a 20-item self-report index that requires participants to characterize their frequency of depressive symptoms in nine different symptom groups. A CESD style score was calculated using a 4-point Likert scale ranging from 0 (not at all or less than 1 day last week) to 3 (5–7 days or nearly every day for 2 weeks). A score of ≥ 16 is consistent with clinically significant depressive symptoms. The CESD-R has demonstrated sound reliability and validity in many studies of ethnic minority youth [31] and people living with HIV [22, 23], and was found to be reliable in our sample as well (Cronbach’s α = 0.97).
Anxiety Symptoms
We measured anxiety using the Generalized Anxiety Disorder-7 (GAD-7) scale [32]. The GAD-7 is a 7-item Likert scale instrument with response options ranging from 0 (not at all) to 3 (nearly every day). A total score (the sum of item scores) of 0–4 is characterized as minimal anxiety, 5–9 is mild anxiety, 10–14 is moderate, and 15–21 is severe anxiety. The GAD-7 has been used in similar populations [23] and reliability was excellent in our sample (Cronbach’s α = 0.94).
Trauma and Stress-Related Symptoms
We used the abbreviated post-traumatic stress disorder (PTSD) Checklist- civilian version (PCL-C) to assess symptoms of PTSD. Specifically, we used a two-item version that has been demonstrated to perform well as a short screening instrument in primary care clinic settings [33]. Participants are asked two questions (one about repeated, disturbing thoughts or memories; and the other about feeling upset when reminded of a stressful event from the past) on a Likert scale ranging from 1 (not at all) to 5 (extremely). A score of ≥ 4 corresponds to a positive screen for trauma-/stress-related symptoms. Reliability was very good in this study sample (Cronbach’s α = 0.82).
General Well-Being
The General Well-Being Schedule (GWB) includes 18 items assessing feelings of psychological well-being and distress over the past month [34]. The first 14 items use a six-point Likert scale, while the last four items use a 0–10 rating scale. Lower sum scores represent greater distress, and established cutoffs for total scores include 0–25 for severe distress, 26–40 for serious distress, 41–55 for distress, 56–70 for stress problem, 71–75 for marginal, 76–80 for low positive, and 81–110 for positive well-being. The GWB has previously been used in research with diverse populations, including Black women [35]. Reliability was very good in our study sample (Cronbach’s α = 0.84).
Measures—Demographics and Covariates
Socio-Demographic Factors
The lifespan biopsychosocial model emphasizes the central role of demographic and socioeconomic factors in influencing health status of minority populations. We therefore asked participants to provide their date of birth and to report their sexual orientation, education level, incarceration history, and income range. Participants characterized their current employment status as employed full-time, employed part-time, or unemployed. Housing instability was assessed in two different ways. We asked participants whether or not they had been homeless in the last 3 months, and also asked them how many times they had moved within the last 6 months.
HIV Stigma
Given the well-documented effects of HIV stigma on health outcomes in YB-GBMSM [36,37,38], we added HIV stigma as a factor in our model, proposed to predispose to psychological adversity. HIV stigma was measured using the revised HIV stigma scale for youth [39], a 10-item index that asks participants to rate their agreement with statements about attitudes towards people with HIV, disclosure concerns, and negative self-image. The scale utilizes a 4-point Likert response ranging from 1 (strongly agree) to 4 (strongly disagree) and was reliable in our sample (Cronbach’s α = 0.90).
Health Behaviors: Substance Use
Substance use was assessed using the NIDA-Modified Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) V2.0 for participants reporting substance use in the past year. In the NIDA-Modified ASSIST, participants report use of cannabis, cocaine, prescription stimulants, methamphetamine, inhalants, sedatives, hallucinogens, street opioids, prescription opioids, and other not-listed substances in the past 3 months. Positive substance use was coded for participants that endorsed use of any substance in the past 3 months.
Psychosocial Reserve Capacity: Religious Involvement
Religious involvement was construed as a psychosocial reserve capacity factor and measured using the Duke University Religion Index (DUREL), a five-item instrument meant to capture three dimensions: organizational religious activity, non-organizational religious activity, and intrinsic or subjective religiosity. Two items are rated on a 6-point Likert scale, and the other three items are coded on a 5-point Likert scale and summed to provide the intrinsic or subjective religiosity subscale score. Reliability in our sample was adequate (Cronbach’s α = 0.74).
Healthcare Access: Trust in Physicians and Discrimination in Medical Settings
Based on the assumption that acceptability is a key component of access to care, we examined trust in physicians and discrimination in medical settings as healthcare access factors. The Trust in Physician scale is an 11-item instrument that asks participants to rate their agreement with statements about their feelings towards their physicians on a 5-point Likert scale (from 1 = totally disagree to 5 = totally agree). Although the measure was developed in a predominantly white and middle-aged sample, reliability was adequate in our sample (Cronbach’s α = 0.76).
The widely used Every Day Discrimination Scale has been adapted to specifically focus on discrimination in medical settings among Black Americans [40, 41]. We used this Discrimination in Medical Settings (DMS) scale, which is a 7-item measure asking respondents to rate the frequency of their experiences of mistreatment in medical settings using a 5-point Likert scale from 1 (never) to 5 (always). Reliability was very high in our sample (Cronbach’s α = 0.95).
Data Analysis
We used SAS v 9.4 (Cary, NC) to conduct all analyses. Some surveys contained single-item non-responses, skewing total scale scores. To reduce non-response bias, we used hot deck imputation to address these missing data and replaced the value of an item non-response with a response from a similar participant [42]. We used univariate (descriptive), bivariate, and multivariable analyses to examine distributions and associations between demographic, psychosocial, and mental health outcome measures. Descriptive analyses included frequencies and measures of central tendency and variability (Table 1). Bivariate analyses included linear and logistic regression. Associations that were significant at p < 0.20 in bivariate analyses were retained in the multivariable models. Separate multivariable regression models were developed for each mental health outcome (depressive symptoms, anxiety symptoms, trauma symptoms, and general well-being; Tables 2, 3, 4 and 5). Based on previous analyses using our outcome measures, we developed multivariable linear regression models of predictors of depressive symptoms and general well-being, and multivariable logistic regression models of predictors of anxiety and trauma symptoms, using no symptoms as the referent group.
Results
Demographics and Covariate Measures
The mean age of our sample was 25 years (SD = 3 years). Seventy-eight percent (78%) identified as gay, homosexual, or same gender loving, with the remainder self-identifying as bisexual (18%), and straight or questioning (3%). A large majority (93%) had at least a high school diploma/GED. Thirty-nine percent reported a household income of less than $10,000 annually. Thirty-eight percent of the sample had full-time employment, 22% were employed part time, and 39% were unemployed. Nearly half (49%) had moved at least once in the last 6 months, and 15% reported homelessness in the past 3 months. Half of the sample had ever been incarcerated, with 13% incarcerated within the last 3 months. Additional demographic details are presented along with summary statistics for religious involvement, trust in physicians, discrimination in medical settings, and HIV stigma scales in Table 1.
Depressive Symptoms
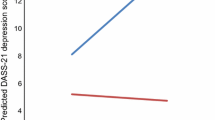
Forty-one percent (41%) of the sample reported significant depressive symptoms, defined as a CESD-style CESD-R score ≥ 16 (Table 2). In unadjusted linear regression analyses, being unemployed, having an incarceration history, experiencing higher levels of discrimination in medical settings, higher levels of HIV stigma, and substance abuse were associated with higher CESD-R scores (data not shown). In adjusted linear regression analyses, full-time employment and lack of substance use were significantly associated with lower depression scores, while higher HIV stigma lead to higher depression scores (Table 3).
Anxiety Symptoms
Forty-eight percent (48%) had symptoms of anxiety: 19% were categorized as mild anxiety, 15% with moderate anxiety, and 14% with severe anxiety symptoms (Table 2). No covariates were significantly associated with mild anxiety symptoms in unadjusted and adjusted logistic regression analyses (data not shown). Higher educational attainment, discrimination in medical settings, and HIV stigma were associated with severe anxiety symptoms in unadjusted logistic regression analyses. Full-time employment was negatively associated with both moderate and severe anxiety symptoms (data not shown). In adjusted logistic regression analyses, younger age predicted lower odds of severe anxiety, while HIV stigma and having a bachelor’s degree or more was associated with higher odds of severe anxiety. Multivariable logistic regression analyses are presented in Table 4.
Trauma-Related Symptoms
Forty-three percent (43%) screened positive for trauma/stress-related symptoms (Table 2). In unadjusted logistic regression analyses, employment status (OR 0.31, 95% CI 0.12–0.81) and HIV stigma (OR 1.87; 95% CI 1.10–3.17) were associated with trauma/stress-related symptoms; however, only HIV stigma remained significantly associated (OR 1.95, 95% CI 1.01–3.79) in multivariable logistic regression analyses (data not shown).
General Well-Being
In our sample, 35% of respondents were categorized as being in distress, serious distress, or severe distress, 37% as having a stress problem, 13% as marginal, and 15% as positive well-being. In unadjusted linear regression analyses, higher income, part-time employment, and trust in physicians lead to higher general well-being scores, while HIV stigma and discrimination in medical settings lead to lower general well-being scores. In adjusted logistic regression analyses, trust in physicians, lower HIV Stigma, full-time employment, and lack of substance use increased average general well-being scores (Table 5).
Discussion
We found a high frequency of depressive, anxiety, and trauma-related symptoms in this sample of YB-GBMSM living with HIV recruited from two Ryan White clinics in Atlanta, Georgia. We also found a high frequency of unemployment and criminal justice system involvement, as more than 40% of the study sample reported being unemployed at the time of the study, and nearly half of study sample reported having even been incarcerated. Biopsychosocial factors including employment, substance use, and HIV stigma emerged as correlates of depression, anxiety, and trauma-related symptoms, while employment and trust in physicians were significantly associated with general well-being. Our study is among the first to focus on mental health symptoms in a sample consisting exclusively of YB-GBMSM living with HIV. We believe that this focus is an important contribution to the literature, as this group faces unique challenges due to the intersecting stigmas and socio-demographic stressors encountered across their lifespans.
The high burden of mental health symptoms in our sample suggests an urgent need for interventions among YB-GBMSM that target not only HIV-related outcomes (e.g., viral suppression), but also mental health and general well-being. Although rates of psychological symptoms in our sample were high, they were also consistent with prior studies in similar populations. Other studies of YB-GBMSM living with HIV have found rates of depressive symptoms (similarly defined as CESD > 16) ranging from 47 to 58% [22, 23]. Anxiety was reported with higher frequency in our cohort than by that reported in other studies [19]; in general, anxiety and trauma are infrequently assessed in previous studies specific to YB-GBMSM. In previous studies of trauma experiences among slightly older samples of Black GBMSM living with HIV, 60% had experienced at least one interpersonal trauma and 40% met screening criteria for PTSD [43, 44]. Another study of behaviorally bisexual Black GBMSM reported PTSD in 20% of the sample. Our results in this younger cohort of Black GBMSM suggest that trauma experiences may be accrued at a young age, and should be investigated further in more detailed trauma inventories as well as qualitative studies.
The consistent association of employment with mental health outcomes was a main finding in our analysis, and highlights the important role of socioeconomic factors for mental health in this population. Many epidemiological studies control for employment as a demographic variable, but relatively few explore its role in-depth. Some studies have examined the importance of employment for Black GBMSM and/or young GBMSM more broadly—however, most of these observations have been related to associations between employment and HIV-related outcomes (e.g., sexual risk behavior or HIV status) as opposed to mental health outcomes such as those we describe here [45,46,47]. Several studies point specifically to risk pathways linking unemployment and/or financial hardship to engagement in transactional sex as a mechanism for increased HIV risk among GBMSM [48, 49]. The associations found in our analysis bring up another potential pathway—unemployment could be causing depression and anxiety that in turn adversely impact HIV care outcomes. Alternatively, those suffering from mental health challenges may be less likely to secure employment, and also to less likely to meet HIV clinical goals. Future longitudinal studies that include measures of employment, socioeconomic status, transactional sex, and mental health may help to elucidate the causal pathways between these constructs. Novel interventions to enhance employment opportunities as a means of HIV prevention among sexual minority youth of color also need to be developed and tested [50].
HIV stigma also emerged as a key predictor across mental health outcomes, supporting our addition of this construct as an antecedent of psychological adversity (along with race and SES) in our modified lifespan biopsychosocial model. This finding is consistent with many other studies demonstrating associations between HIV stigma and psychological distress, including among YB-GBMSM living with HIV [51]. Prior work suggests that the internalization of negative feelings about oneself is the most important component of HIV stigma for mental health [47, 52]. Although our current study did not specifically measure other concurrent types of minority stressors (e.g., internalized racism or homonegativity), other work has suggested that multiple minority statuses can interact synergistically to cause negative effects on physical and mental health [52]. Interventions to decrease internalized HIV stigma must be prioritized in order to optimize mental health outcomes for YB-GBMSM living with HIV.
It was notable that religious involvement was not associated with any of our mental health outcomes in adjusted analyses. One possibility is that religion may have mixed effects on mental health in this population. We initially hypothesized this effect to be primarily positive (with religion and spirituality serving as a coping mechanism), building on research demonstrating that Black Americans often utilize church-based support in dealing with mental health problems [53, 54] and that church involvement can sometimes support mental health service use [55]. However, research specifically among Black GBMSM has also demonstrated negative effects of conservative religious institutions which may exacerbate internalized homophobia and resultant psychological distress [9, 56, 57]. This complex and sometimes conflicting role of religion in our sample of young, Southern Black men, may have obscured any statistical relationship between religiosity and mental health in our sample.
Lack of substance use in our sample was associated with lower risk of depressive symptoms, and higher self-rating of general well-being. This finding is consistent with an established evidence base confirming the negative impact of substance use on depression among youth more generally [58]. Programming to prevent or treat problematic substance use in YB-GBMSM may, therefore, have dual impacts in addressing the negative ramifications for mood as well as the deleterious effects of substance use itself.
The addition of a measure of positive psychological symptoms (e.g., general well-being) was somewhat novel in our study, as studies of mental health among other sexual minority youth of color often focus primarily on negative psychological outcomes [59]. General well-being, like depression and anxiety, was associated with employment and substance use. However, trust in physicians was significantly associated with general well-being, but not with symptoms of depression, anxiety, or trauma. Related to this finding, others have found associations between trust in physicians and positive attitudes about HIV medications among YB-GBMSM living with HIV and other people living with HIV [7, 60]. Encouragingly, prior work has shown that the majority of patients trust their physicians even if they espouse mistrust towards the government or biomedical science more generally [61]. Interventions designed to enhance and build upon the patient-physician relationship are, therefore, promising avenues for enhancing general well-being, as well as medication use, among YB-GBMSM.
Limitations
As our study was conducted exclusively in clinical settings, the burden of symptoms may have been different (and potentially higher) among YB-GBMSM who are living with HIV but not engaged in HIV care. Our sample size was relatively small, so that we may have been underpowered to observe some associations that could emerge in larger studies in the future. It should be noted that positive screening tests do not all correspond to clinical diagnoses, and future studies should incorporate more rigorous diagnostic interviewing to help determine the true burden of psychological disorders in this population. Additionally, we did not include survey questions about time since HIV diagnosis, an established correlate of mental health comorbidities and would have provided additional context for our findings. Finally, the cross-sectional nature of the study precludes definitive assessment of the directionality of associations noted here. More in-depth exploration of the lifespan model in the future should also include assessment of these demographics and stressors from childhood, as well as examination of protective factors such as social support and resilience. Qualitative research would also be useful for helping to understand cultural factors with particular relevance for interventions targeting mental health among YB-GBMSM.
Conclusions
YB-GBMSM living with HIV bear a high burden of mental health symptoms, including symptoms of depression, anxiety, and trauma. Structural interventions to address socio-demographic vulnerabilities may be particularly impactful for improving mental health in this population. Additionally, HIV stigma remains a critically important barrier to optimal mental health for this group, and should be targeted in culturally-informed interventions.
Data Availability
Data will be made available upon request.
Code Availability
Not applicable.
References
Matthews DD, Herrick AL, Coulter RW, et al. Running backwards: consequences of current HIV incidence rates for the next generation of black MSM in the United States. AIDS Behav. 2016;20(1):7–16.
Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clin Infect Dis: Off publ Infect Dis Soc Am. 2013;57(8):1164–71.
Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.
Singh S, Bradley H, Hu X, Skarbinski J, Hall HI, Lansky A. Men living with diagnosed HIV who have sex with men: progress along the continuum of HIV care–United States, 2010. MMWR Morb Mortal Wkly Rep. 2014;63(38):829–33.
Mustanski B, Morgan E, D’Aquila R, Birkett M, Janulis P, Newcomb ME. Individual and network factors associated with racial disparities in HIV among young men who have sex with men: results from the radar cohort study. J Acquir Immune Defic Syndr. 2018. https://doi.org/10.1097/QAI.0000000000001886.
Myers HF. Ethnicity- and socio-economic status-related stresses in context: an integrative review and conceptual model. J Behav Med. 2009;32(1):9–19.
Reif SS, Whetten K, Wilson ER, et al. HIV/AIDS in the Southern USA: a disproportionate epidemic. AIDS Care. 2014;26(3):351–9.
Adimora A. Drivers of the HIV epidemic in the Southern U.S. 20th Conference on retroviruses and opportunistic infections; 2013 March 5, 2013; Atlanta, GA.
Moore S, Jones M, Smith JC, et al. Homonegativity experienced over the life course by young black gay, bisexual and other men who have sex with men (YB-GBMSM) living with HIV in Atlanta, Georgia. AIDS Behav. 2019;23(3):266–75.
Quinn KG, Spector A, Takahashi L, Voisin DR. Conceptualizing the effects of continuous traumatic violence on HIV continuum of care outcomes for young black men who have sex with men in the United States. AIDS Behav. 2021;25(3):758–72.
Balaji AB, Oster AM, Viall AH, Heffelfinger JD, Mena LA, Toledo CA. Role flexing: how community, religion, and family shape the experiences of young black men who have sex with men. AIDS Patient Care STDS. 2012;26(12):730–7.
Eldahan AI, Pachankis JE, Jonathon Rendina H, Ventuneac A, Grov C, Parsons JT. Daily minority stress and affect among gay and bisexual men: a 30-day diary study. J Affect Disord. 2016;190:828–35.
Bauermeister JA, Muessig KE, Flores DD, et al. Stigma diminishes the protective effect of social support on psychological distress among young black men who have sex with men. AIDS Educ Prev. 2018;30(5):406–18.
Do AN, Rosenberg ES, Sullivan PS, et al. Excess burden of depression among HIV-infected persons receiving medical care in the united states: data from the medical monitoring project and the behavioral risk factor surveillance system. PLoS ONE. 2014;9(3):e92842.
Walsh ASJ, Wesley KL, Tan SY, et al. Screening for depression among youth with HIV in an integrated care setting. AIDS Care. 2017;29(7):851–7.
Beer L, Tie Y, Padilla M, Shouse RL, Medical MP. Generalized anxiety disorder symptoms among persons with diagnosed HIV in the United States. AIDS. 2019;33(11):1781–7.
Glynn TR, Mendez NA, Jones DL, et al. Trauma exposure, PTSD, and suboptimal HIV medication adherence among marginalized individuals connected to public HIV care in Miami. J Behav Med. 2021;44(2):147–58.
Brown LK, Whiteley L, Harper GW, Nichols S, Nieves A. Protocol team for the adolescent medicine trials network for HIV/AIDS interventions. Psychological symptoms among 2032 youth living with HIV: a multisite study. AIDS Patient Care STDs. 2015;29(4):212–9.
Rao D, Feldman BJ, Fredericksen RJ, et al. A structural equation model of HIV-related stigma, depressive symptoms, and medication adherence. AIDS Behav. 2012;16(3):711–6.
Carrico AW, Riley ED, Johnson MO, et al. Psychiatric risk factors for HIV disease progression: the role of inconsistent patterns of antiretroviral therapy utilization. J Acquir Immune Defic Syndr. 2011;56(2):146–50.
Traeger L, O’Cleirigh C, Skeer MR, Mayer KH, Safren SA. Risk factors for missed HIV primary care visits among men who have sex with men. J Behav Med. 2012;35(5):548–56.
Hussen SA, Easley KA, Smith JC, et al. Social capital, depressive symptoms, and HIV viral suppression among young black, gay, bisexual and other men who have sex with men living with HIV. AIDS Behav. 2018;22(9):3024–32.
Menza TW, Choi SK, LeGrand S, Muessig K, Hightow-Weidman L. Correlates of self-reported viral suppression among HIV-positive, young, black men who have sex with men participating in a randomized controlled trial of an internet-based HIV prevention intervention. Sex Transm Dis. 2018;45(2):118–26.
Bengtson AM, Pence BW, Mimiaga MJ, et al. Depressive symptoms and engagement in HIV care following ART initiation. Clin Infect Dis: Off Publ Infect Dis Soc Am. 2018;68(3):475–81.
McLean CP, Gay NG, Metzger DA, Foa EB, Penn Mental Health ARC. Psychiatric symptoms and barriers to care in HIV-infected individuals who are lost to care. J Int Assoc Provid AIDS Care. 2017;16(5):423–9.
Hatcher AM, Smout EM, Turan JM, Christofides N, Stockl H. Intimate partner violence and engagement in HIV care and treatment among women: a systematic review and meta-analysis. AIDS. 2015;29(16):2183–94.
van den Berg JJ, Neilands TB, Johnson MO, Chen B, Saberi P. Using path analysis to evaluate the healthcare empowerment model among persons living with HIV for antiretroviral therapy adherence. AIDS Patient Care STDS. 2016;30(11):497–505.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Van Dam NT, Earleywine M. Validation of the center for epidemiologic studies depression scale–revised (CESD-R): pragmatic depression assessment in the general population. Psychiatry Res. 2011;186(1):128–32.
Eaton WW, Muntaner C, Smith C, Tien A, Ybarra M. Center for epidemiologic studies depression scale: review and revision (CESD and CESD-R). In: Maurish ME, editor. The use of psychological testing for treatment planning and outcomes assessment. Mahwah, NJ: Lawrence Erlbaum; 2004. p. 363–77.
Skriner LC, Chu BC. Cross-ethnic measurement invariance of the SCARED and CES-D in a youth sample. Psychol Assess. 2014;26(1):332–7.
Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7.
Lang AJ, Stein MB. An abbreviated PTSD checklist for use as a screening instrument in primary care. Behav Res Ther. 2005;43(5):585–94.
Dupuy H, editor Self-representations of general psychologicl well-being of American adults. American Public Health Association meeting; 1978; Los Angeles, CA.
Taylor JE, Poston WS 2nd, Haddock CK, et al. Psychometric characteristics of the general well-being schedule (GWB) with African-American women. Qual Life Res. 2003;12(1):31–9.
Arnold EA, Rebchook GM, Kegeles SM. 'Triply cursed’: racism, homophobia and HIV-related stigma are barriers to regular HIV testing, treatment adherence and disclosure among young Black gay men. Cult Health Sex. 2014;16(6):710–22.
Arrington-Sanders R, Hailey-Fair K, Wirtz AL, et al. Role of structural marginalization, HIV stigma, and mistrust on HIV prevention and treatment among young black latinx men who have sex with men and transgender women: perspectives from youth service providers. AIDS Patient Care STDS. 2020;34(1):7–15.
Earnshaw VA, Eaton LA, Collier ZK, et al. HIV stigma, depressive symptoms, and substance use. AIDS Patient Care STDS. 2020;34(6):275–80.
Wright K, Naar-King S, Lam P, Templin T, Frey M. Stigma scale revised: reliability and validity of a brief measure of stigma for HIV+ youth. J Adolesc Health: Off Publ Soc Adolesc Med. 2007;40(1):96–8.
Williams DR, Yan Y, Jackson JS, Anderson NB. Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol. 1997;2(3):335–51.
Peek ME, Nunez-Smith M, Drum M, Lewis TT. Adapting the everyday discrimination scale to medical settings: reliability and validity testing in a sample of African American patients. Ethn Dis. 2011;21(4):502–9.
Andridge RR, Little RJ. A review of hot deck imputation for survey non-response. Int Stat Rev. 2010;78(1):40–64.
Fields EL, Bogart LM, Galvan FH, Wagner GJ, Klein DJ, Schuster MA. Association of discrimination-related trauma with sexual risk among HIV-positive African American men who have sex with men. Am J Public Health. 2013;103(5):875–80.
Bogart LM, Wagner GJ, Galvan FH, Landrine H, Klein DJ, Sticklor LA. Perceived discrimination and mental health symptoms among Black men with HIV. Cult Divers Ethn Minor Psychol. 2011;17(3):295–302.
Tobin KE, Cutchin M, Latkin CA, Takahashi LM. Social geographies of African American men who have sex with men (MSM): a qualitative exploration of the social, spatial and temporal context of HIV risk in Baltimore, Maryland. Health Place. 2013;22:1–6.
Gayles TA, Kuhns LM, Kwon S, Mustanski B, Garofalo R. Socioeconomic disconnection as a risk factor for increased HIV infection in young men who have sex with men. LGBT Health. 2016;3(3):219–24.
Hussen SA, Harper GW, Bauermeister JA, Hightow-Weidman LB. Psychosocial influences on engagement in care among HIV-positive young black gay/bisexual and other men who have sex with men. AIDS Patient Care STDS. 2015;29(2):77–85.
Duncan DT, Park SH, Schneider JA, et al. Financial hardship, condomless anal intercourse and HIV risk among men who have sex with men. AIDS Behav. 2017;21(12):3478–85.
Bauermeister JA, Eaton L, Meanley S, Pingel ES, Partnership U. Transactional sex with regular and casual partners among young men who have sex with men in the Detroit Metro area. Am J Mens Health. 2017;11(3):498–507.
Hill BJ, Motley DN, Rosentel K, et al. An employment intervention program (Work2Prevent) for young men who have sex with men and transgender youth of color (Phase 1): protocol for determining essential intervention components using qualitative interviews and focus groups. JMIR Res Protoc. 2020;9(8):e16384.
Boone MR, Cook SH, Wilson PA. Sexual identity and HIV status influence the relationship between internalized stigma and psychological distress in black gay and bisexual men. AIDS Care. 2016;28(6):764–70.
Rendina HJ, Gamarel KE, Pachankis JE, Ventuneac A, Grov C, Parsons JT. Extending the minority stress model to incorporate HIV-positive gay and bisexual men’s experiences: a longitudinal examination of mental health and sexual risk behavior. Ann Behav Med. 2017;51(2):147–58.
Chatters LM, Mattis JS, Woodward AT, Taylor RJ, Neighbors HW, Grayman NA. Use of ministers for a serious personal problem among African Americans: findings from the national survey of American life. Am J Orthopsychiatry. 2011;81(1):118–27.
Neighbors HW, Musick MA, Williams DR. The African American minister as a source of help for serious personal crises: bridge or barrier to mental health care? Health Educ Behav. 1998;25(6):759–77.
Turner N, Hastings JF, Neighbors HW. Mental health care treatment seeking among African Americans and Caribbean Blacks: what is the role of religiosity/spirituality? Aging Mental Health. 2018;23(7):905–11.
Jeffries WL 4th, Okeke JO, Gelaude DJ, Torrone EA, Gasiorowicz M, Oster AM, et al. An exploration of religion and spirituality among young, HIV-infected gay and bisexual men in the USA. Cult Health Sex. 2014;16(9):1070–83.
Watkins TL Jr, Simpson C, Cofield SS, Davies S, Kohler C, Usdan S. The relationship of religiosity, spirituality, substance abuse, and depression among black men who have sex with men (MSM). J Relig Health. 2016;55(1):255–68.
Cairns KE, Yap MB, Pilkington PD, Jorm AF. Risk and protective factors for depression that adolescents can modify: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2014;169:61–75.
Toomey RB, Huynh VW, Jones SK, Lee S, Revels-Macalinao M. Sexual minority youth of color: a content analysis and critical review of the literature. J Gay Lesbian Mental Health. 2017;21(1):3–31.
Gillman J, Davila J, Sansgiry S, et al. The effect of conspiracy beliefs and trust on HIV diagnosis, linkage, and retention in young MSM with HIV. J Health Care Poor Underserved. 2013;24(1):36–45.
Altice FL, Mostashari F, Friedland GH. Trust and the acceptance of and adherence to antiretroviral therapy. J Acquir Immune Defic Syndr. 2001;28(1):47–58.
Funding
This work was funded by the National Institutes of Health through a supplement to the Emory Center for AIDS Research (P30 AI040509).
Author information
Authors and Affiliations
Contributions
SAH, KD, DMC, SJM, MKA and EWF contributed to the initial conceptualization, design, and implementation of the study. SAH, KD, and DMC conducted data analysis. SAH led the writing of the initial draft of the paper. KD, DMC, SJM, ASK, RW, TL, MKA, and EWF all reviewed the paper, made revisions, and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests or relevant disclosures.
Ethical Approval
We received ethical approval from the Emory University Institutional Review Board and the Grady Research Oversight Committee.
Consent to Participate
All participants provided informed consent.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hussen, S.A., Doraivelu, K., Camp, D.M. et al. Burden and Correlates of Mental Health Symptoms Among Young Black Gay, Bisexual, and Other Men Who Have Sex with Men Engaged in HIV Care in Atlanta. AIDS Behav 26, 2844–2854 (2022). https://doi.org/10.1007/s10461-022-03629-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-022-03629-1