
Abstract
Risky sexual behavior and substance use appear to be interconnected behaviors among adolescents, but data are scarce regarding the extent to which sexual risk behavior is associated with high levels of marijuana and alcohol use, both separately and in combination. 301 adolescents were recruited from a short-term detention facility, and substance use and risky sexual behavior were assessed. We found that adolescents who frequently used marijuana, but not alcohol, reported significantly less risky sex as well as greater intentions to use condoms than either adolescents who frequently used alcohol, but not marijuana, or adolescents who frequently used both substances. Substance use status as a predictor of future risky sexual behavior followed a similar pattern. When designing interventions to reduce substance use in the context of risky sex, it might be especially effective to target efforts toward reducing harm associated with alcohol use, either alone or in combination with marijuana use.
Resumen
El comportamiento sexual riesgoso y el uso de sustancias parecen ser comportamientos interconectados entre los adolescentes, pero son escasos los datos con respecto al grado hasta el cual el comportamiento sexual riesgoso está asociado con altos niveles de consumo de marihuana y alcohol, tanto por separado como en combinación. Se reclutó a 301 adolescentes de un centro de detención a corto plazo y se evaluó el uso de sustancias y el comportamiento sexual riesgoso. Encontramos que los adolescentes que usaban con frecuencia marihuana, pero no alcohol, reportaron relaciones sexuales significativamente menos riesgosas así como mayores intenciones de usar condones que adolescentes que usaban alcohol con frecuencia, pero no marihuana, o adolescentes que usaban con frecuencia ambas sustancias. El estado de uso de sustancias como predictor de futuros comportamientos sexuales riesgosos mostró un patrón similar. Al diseñar intervenciones para reducir el uso de sustancias en el contexto de las relaciones sexuales de riesgo, podría ser especialmente eficaz centrarse en los esfuerzos para reducir el daño asociado con el consumo de alcohol, solo o en combinación con el consumo de marihuana.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescents and young adults are one of the only segments of the population for whom acquisition of sexually transmitted infections (STI) including human immunodeficiency virus (HIV) is not decreasing, with 22% of new HIV diagnoses and 50% of all new STI diagnoses occurring in individuals aged 13–24 [1]. Economically disadvantaged and/or minority youth are at disproportionate risk for acquiring HIV; individuals at or below the poverty threshold are more than twice as likely to test positive for HIV, and black and Latino youth encompass the majority of new HIV diagnoses among this age group [1]. Rates of risky sexual behavior and its health consequences are particularly high for adolescents involved with the juvenile justice system, who frequently come from disadvantaged circumstances [2] or are of minority backgrounds [3].
Perhaps unsurprisingly, risky sexual behavior and substance use are interconnected, particularly among adolescents. A recent meta-analysis of 87 studies by Ritchwood et al. [4] showed that both alcohol and marijuana use were independently associated with risky sexual behaviors including condomless sex and a higher number of sexual partners in adolescents. This is important, as marijuana and alcohol are the two substances most widely used by adolescents. Recent national survey results from the National Institute on Drug Abuse demonstrate that after declining for about a decade, adolescent marijuana use has remained steady for the past several years, with 31% of 8th–12th graders reporting ever having used marijuana [5]. However, perceived risk of marijuana use (i.e., the proportion of adolescents “seeing great risk from using marijuana”) has been declining steeply, a phenomenon some attribute to the increasing public acceptance of marijuana use and the legalization of marijuana for medical and recreational use in many states [6]. Adolescent alcohol use has also declined since the 1990s; nevertheless, 46.4% of 8th–12th graders still report that they have had alcohol. As with risky sexual behavior, adolescents involved in the juvenile justice system are at much greater risk for abusing marijuana and alcohol, with a recent study showing that 90.1% report having ever used alcohol and 84.1% reported having ever used marijuana [7]. Further, substance use disorders affect approximately 50% of justice-involved youth [8, 9].
Given that alcohol and marijuana are both commonly used by adolescents, and because use of these substances often co-occurs [9], it is important to examine the extent to which sexual risk behavior is associated with high levels of marijuana and alcohol use, both separately and in combination. Presently, there is no clear consensus in the literature about whether alcohol or marijuana use is more strongly associated with risky sex, or whether co-occurring use might be associated with the highest level of sexual risk. Hingson et al. [10] and Guo et al. [11] showed somewhat stronger associations between alcohol and risky sex than marijuana and risky sex. Others have found that condomless sex and other risky sexual behavior was more strongly associated with marijuana than alcohol [12,13,14], while the meta-analysis by Ritchwood et al. did not find significantly different effect sizes for alcohol versus marijuana use [4]. The picture is even less clear for a possible synergistic association of the co-occurring use of both substances. One study found that the use of both substances simultaneously did not seem to have stronger effects on condomless sex than using one or the other [15]. In addition, in a recent longitudinal study of low socioeconomic status African American youth, Ritchwood et al. found mostly redundant relationships between alcohol and marijuana use and sexual risk. That is, the use of either alcohol or marijuana similarly led to increased sexual risk. The addition of marijuana use on top of alcohol use did not increase risky sexual behavior in general, except for one significant interaction such that alcohol use increased instances of having sex while high [14]. Given the mixed findings, it is important to take a nuanced approach to understanding relationships between use of these substances and risky sexual behavior, especially in vulnerable adolescents, and those in the juvenile justice system are indeed vulnerable.
There are currently more than 31 million adolescents involved in the U.S. juvenile justice system [16]. Given disproportionately high rates of both risky sexual behavior and substance use, it is perhaps unsurprising that numerous studies have shown associations between substance use and risky sexual behavior, both at the global and event levels, in this population [12, 13, 17,18,19,20]. Thus, this is a critically important population in whom to examine and understand the pattern of relationships that exists between the most commonly used substances of abuse and sexual behaviors that place them at high risk of negative outcomes. Targeting adolescents who are most at risk, for both study and intervention, is an increasingly accepted strategy, as studies have shown this is likely to lead to more fruitful intervention efforts and a greater reduction of the overall problem at a societal level [21].
The aims of the current study were two-fold: first, to examine whether patterns of sexual risk as well as known antecedents of sexual risk, namely, condom use intentions, differ for groups of justice-involved adolescents who use high levels of marijuana, alcohol, or both substances; second, to examine whether frequency of alcohol use and frequency of marijuana use were uniquely related to lower intentions to use condoms and higher rates of risk behavior, and whether interactive effects occur with high frequency of use of both marijuana and alcohol. We were interested in the effects of frequency of substance use both in terms of frequency of overall use as well as the frequency of event-level substance use (i.e., the frequency of substance use during sex). Given mixed findings in the literature, we did not predict significant differences in either intentions or risky sexual behavior between adolescents who use marijuana more frequently versus those who use alcohol more frequently, only that higher frequency of use of either substance would be associated with lower intentions to use condoms and more frequent sexual risk behavior. While interactive effects have not been reliably observed in past research, given especially high levels of use in our unique sample, we predicted significant interactive effects for co-occurring use, such that those adolescents who frequently used both substances would report the lowest condom use intentions and the highest levels of sexual risk behavior. We conducted these analyses using both baseline risk behavior and intentions, and then again prospectively for risk behavior and intentions 3 months after baseline.
Method
Participants
Participants were drawn from a larger study of 460 adolescents who were residing in a short-term youth detention facility at the time of recruitment (for full details, see [22]). Requirements for eligibility in the larger study included that participants must: [1] be between the ages of 14 and 18, [2] speak English, [3] have a remaining term in detention of less than 1 month (due to the nature of the larger intervention study), and [4] be willing to sign a release form allowing access to their STI test results if they were tested at intake. Adolescent assent was obtained in person and parental consent was obtained via telephone.
Given that our hypotheses concerned risky sexual behavior in adolescents who report high levels of alcohol, marijuana, or co-occurring use, we examined a subset of these 460 adolescents by creating groups based on their level of substance use. That is, we grouped adolescents based on their reported use of both substances, and examined differences in these sexual risk outcomes, both cross-sectionally and after a three-month follow-up period to determine whether substance use status would prospectively predict risk behavior. Due to the prevalence of co-occurring alcohol and marijuana use, we were unable to create groups based on the exclusive use of alcohol or marijuana. Thus we selected groups on the basis that they were heavy users of one substance but only light users of the other, or were heavy users of both substances. We were able to categorize the majority (n = 301) of participants into one of these three groups (described below). For this subset, participants were an average of 15.79 years of age (SD = 1.15) and 20.6% female. Most participants were of self-reported minority group status; 65% were Hispanic, 6% were African American, 7% were Native American, 8% were other or mixed race, and the remaining 13% reported their ethnicity as White. Participants were paid US $20 for completing the baseline measures, and an additional $40 for completing the three-month follow-up measures utilized in these analyses. Due to high rates of suboptimal literacy in justice-involved populations and to ensure confidentiality of responses, questionnaires were administered via audio computer-assisted self-interviewing technology on laptop computers [23, 24].
Measures
Substance Use History
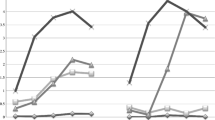
Participants were divided into groups (see Fig. 1) based on their response to the items, “In the last three months, how often did you smoke marijuana,” and “In the last three months, how often did you consume at least one alcoholic drink?” Responses to these items were scored on a 9-point Likert scale, with 1 representing “Never” and 9 representing “Every Day.” Participants also completed a Timeline Followback (TLFB) assessment of both substance use and risky sexual behavior in the past 30 days [25]. The TLFB is a calendar based interview assessment, in which a trained research assistant walks a participant back through the past 30 days and queries their use of any substances on each of those days both in terms of whether or not a substance was used and the quantity of the substance used (i.e., number of drinks on a drinking day).

Mean levels of marijuana and alcohol use frequency in each group. Frequency was determined by responses on a Likert scale, where 1 = never, 2 = occasionally, 3 = once a month, 4 = 2–3 times a month, 5 = 4–5 times a month, 6 = once a week, 7 = 2–3 times a week, 8 = 4–5 times a week, and 9 = Every day
Heavy Marijuana Users (“Marijuana Group”)
148 participants who reported marijuana use of 4–5 times per month or more and alcohol use of 2–3 times per month or less were placed in what we will heretofore refer to as the “marijuana group”. This cut-off point was chosen so that adolescents in this group were using marijuana at least every weekend. On average, participants in this group used marijuana slightly more than 4–5 times per week (M = 8.15, SD = 1.29), and used alcohol between “Occasionally” and “Once a Month” (M = 2.35, SD = 1.11).
Heavy Alcohol Users (“Alcohol Group”)
42 participants who reported alcohol use of 4–5 times per month or more and marijuana use of 2–3 times per month or less were placed in what we will refer to as the “alcohol group”. This cut-off point was chosen such that adolescents in this group were using alcohol at a minimum every weekend. On average, participants in this group used alcohol between “Once a week” and “2–3 times a week” (M = 6.50, SD = 1.27), and used marijuana “Occasionally” (M = 2.04, SD = 1.16).
Heavy Alcohol and Marijuana Users (“Both Group”)
111 participants who reported using both marijuana and alcohol at least 4–5 times per month or more were placed in what we will refer to as the “both group”. Participants in this group used marijuana between “4–5 times per week” and “Every Day” (M = 8.57, SD = 0.90), and used alcohol approximately “2–3 times a week” (M = 6.87, SD = 1.36).
Event-Level Substance Use Measures
We also examined event-level measures of substance use during sex. Participants responded to the questions, “Of all the times you’ve had sexual intercourse, how much of the time did you smoke marijuana before sex?” and “Of all the times you’ve had sexual intercourse, how much of the time did you drink alcohol before sex?”, also scored on a Likert scale, where 1 represented “Never” and 5 represented “Always”.
Sexual History and Risky Sexual Behavior
Participants were asked about sexual orientation, whether or not they have ever had sexual intercourse, age of first intercourse, condom use behavior, and lifetime number of partners. Risky sexual behavior was assessed through sexually experienced participants’ responses to the questions “On average, how often do you have sexual intercourse?” (6 point Likert scale ranging from “A Few Times per Year” to “Almost Every Day”) and “How much of the time have you used condoms when you’ve had sexual intercourse?” (5 point Likert scale ranging from “Never” to “Always). In line with prior work [24], a risky sex index was calculated by multiplying frequency of sex by the reverse-scored condom use measure resulting in a range of 1–30 where higher numbers indicate a higher frequency of condomless sex. Participants who said they have never had sex received a score of 0 on this index, reflecting no sexual risk.
Participants also completed a TLFB assessment of sexual behavior in the past 30 days [25]. From the TLFB, we calculated the percentage of time participants reported using a condom per intercourse occasion in the past 30 days. As a third measure of baseline risky sexual behavior, participants responded whether they had used a condom on their last intercourse occasion (coded dichotomously: yes/no).
Condom Use Intentions
We also examined whether intentions to use condoms differed between substance use groups or as a function of frequency of use of each substance, as intentions to use condoms are a known antecedent to condom use behavior and because intentions can be assessed even for participants who have not yet had sexual intercourse [26]. Based on prior work [17, 27], we evaluated intentions via four items assessing whether participants intend to: buy or get condoms in the next 3 months, carry condoms with them, talk to a partner about using condoms, and use a condom every time they have sex. Items are scored based on a four-point Likert scale (1 = “Will NOT happen” to 4 = “Will DEFINITELY happen”), with a participant’s mean calculated as a summary measure (α = 0.85).
Scenario Specific Condom Use Intentions
We also utilized scenarios to assess specific intentions for condom use in three different substance use situations. In one situation participants were told there would be alcohol use, in another they were told there would be marijuana use, and in a third substance use was not mentioned. All participants saw and responded to all three scenarios. Specifically, participants were told to “Imagine you are going to be hanging out [and drinking a lot of alcohol/smoking weed] tonight, and a girl or guy that you like, but with whom you haven’t had sex with yet, will be there. If you knew you were going to be hanging out with this person: How likely would you be to buy condoms before/discuss using condoms with them/carry condoms with you/use condoms if you had sex with them?” Responses are scored on a four-point Likert scale (“Will NOT happen” − “Will DEFINITELY happen”), and means are calculated for each scenario (alcohol-specific intentions α = 0.88, marijuana-specific intentions α = 0.87, no substance use intentions α = 0.86).
Sexually Transmitted Infection (STI) Outcomes
Participants provided a urine sample that was tested by our research team for Chlamydia trachomatis and Neisseria gonorrhoeae or results were obtained from a test performed by the detention center. Participants who tested positive for either STI were treated by our research team under the supervision of an adolescent medicine specialist (A.S.K.). Participants tested through the detention center were treated by their medical staff. Test results were coded dichotomously, such that participants who tested positive for either or both STIs were coded as “positive” and those who tested negative for both STIs were coded as “negative”. Though these young people are at risk for HIV, 81% of HIV infections in the 13–24 age group occur between the ages of 20 and 24 [1] and the elevated risk associated with justice involvement is typically seen in adult prison populations rather than juvenile justice settings [28]. As our juvenile sample was on the younger end of the age spectrum, we chose to test for STIs that were more common in this age group rather than testing for HIV, to allow for greater power to detect effects.
Follow-Up Measures
In addition to the baseline measures, participants answered the sexual history and condom use intentions measures at a three-month follow-up assessment; 92.2% of participants were retained at follow-up.
Procedure
Participants were recruited from a youth detention facility in the southwestern U.S. by trained research staff. Detention facility staff were not involved in recruitment, consent, or study procedures. Full assent was obtained from the adolescent him/herself and then parent or guardian consent was obtained via phone and audio-taped. This project was approved by the relevant institutional review board and the national Office of Human Research Protections. We also obtained a federal certificate of confidentiality from the National Institute of Alcoholism and Alcohol Abuse.
Results
Descriptive Statistics: Sample-Wide Sexual Risk Behavior
Most (94.22%) participants reported having had sexual intercourse. Average age of first intercourse was 12.97 (SD = 1.69), and average number of partners was 9.72 (SD = 11.65). For frequency of sex, participants scored an average of 3.39 (SD = 1.56), which corresponds to having sex in between “once a week” and “2–3 times a week”. Notably, only 11% reported having used condoms all the time. Thirty-six percent of participants reported that they had used a condom at their most recent sexual encounter, and 64.45% indicated that they were currently in a romantic relationship. Research on risky sexual behavior in adolescents and emerging adults (e.g., [29, 30]), as well as condom use intentions and behavior in high risk adolescents [31, 32], demonstrate important gender differences in condom use attitudes and behaviors. Thus, we include gender as a covariate in all analyses, and descriptive statistics are reported overall and by both user group and by gender in Table 1.
Substance Use Group Differences in Risky Sexual Behavior and Intentions
Our first research question concerned whether groups of adolescents who used mostly alcohol, marijuana, or both substances exhibited different levels of risky sexual behavior and/or intentions to use condoms. To test this question, for each continuous outcome variable of interest, we conducted an ANCOVA with the continuous risky sexual behavior (or intentions) measure as the dependent variable, and substance use group as the independent variable of interest, controlling for age, gender, and relationship status, as past work has demonstrated that these covariates are associated with risky sex [33]. For our dichotomous outcome variables of interest, we used comparable logistic regression models, with substance user group (contrast-coded) as the independent variable of interest, again covarying age, gender, and relationship status. Due to our use of planned pairwise comparisons to examine differences between the three groups, we used Bonferroni correction to protect the familywise error rate. Thus, for all pairwise group comparisons we adjusted the critical p value to 0.01 (0.05/3 pairwise comparisons). All tests of pairwise comparisons presented are adjusted for covariates. For group means, see Table 2.
Outcome: Baseline Risky Sexual Behavior Measures
For the ANCOVA examining the risky sex index measure as the dependent variable, the overall model was significant (F 5,286 = 6.59, p < 0.001). The both group reported more risky sex than the marijuana group (t = −2.52, p = 0.01). The alcohol group reported more risky sex than the marijuana group (t = −2.93, p = 0.0037). The alcohol and both groups were not significantly different from one another (t = 1.09, p = 0.28).
For the ANCOVA examining the TLFB measure of percent of times condoms were used per intercourse occasion as the outcome measure, the overall model was marginal (F 5,204 = 2.14, p = 0.062). Planned comparisons showed that the marijuana group reported more condom use on average than the both group (t = −2.71, p = 0.007). There were no other significant group differences.
In the logistic regression model examining condom use at last intercourse as the dependent variable, we found that adolescents in the marijuana group were significantly more likely than both the alcohol and both groups to report using a condom at last intercourse (adjusted odds ratio = 1.25, p = 0.01). There were no other significant group differences.
Outcome: STI Results
For the 297 participants who had valid baseline STI results, 28 tested positive for an STI, and 269 tested negative. In the logistic regression model examining group differences in STI diagnosis, the only significant independent variable was gender; consistent with the epidemiology of C. trachomatis and N. gonorrhoeae more generally [34]; young women were more likely to test positive for an STI than young men (adjusted odds ratio = 0.23, p = 0.0006). Substance use group was unrelated to STI diagnosis.
Outcome: Condom Use Intentions
In the ANCOVA examining condom use intentions as the dependent variable, we did not observe significant pairwise group differences in overall condom use intentions.
Outcome: Scenario Specific Condom Use Intentions
Since we had three measures of scenario-specific intentions for each participant (no alcohol or marijuana involved, marijuana scenario, alcohol scenario), in order to account for dependence in the data, we used a multivariate ANCOVA, with scenario type as a within-subjects factor and substance use group as the between-subjects factor, again covarying age, gender, and relationship status. For each effect in the MANCOVA we report the Wilk’s Lambda approximation of the multivariate F statistic. The multivariate test of group differences was significant (F 6,584 = 3.03, p = 0.006) and each univariate test of group differences was also significant (no alcohol or marijuana scenario F 2,294 = 4.43, p = 0.013, marijuana scenario F 2,294 = 6.05, p = 0.003, alcohol scenario F 2,294 = 5.70, p = 0.004), such that the marijuana group reported the highest intentions to use condoms across all scenarios compared to the other two groups.
Continuous Measures of Substance Use and Risky Sex
In order to examine whether higher frequency of use of either substance, or higher frequency of use of both substances was associated with risky sex, we estimated a linear regression model. Importantly, this allowed us to include our entire sample of 460 young people (less 21 participants with missing data on the relevant measures) across the full range of our substance use measures. For these analyses, we report unstandardized regression coefficients and use an alpha level of 0.05 to determine statistical significance as this analysis does not involve pairwise group comparisons.
We regressed risky sex on marijuana use frequency (mean-centered), alcohol use frequency (mean-centered), and their interaction, again covarying gender, age, and relationship status. The overall model was significant (F 6,432 = 9.37, p < 0.001, Multiple R 2 = 0.12). Largely consistent with the general pattern of the group results, we found no association between marijuana use and risky sex (B = −0.06, t = −0.59, p = 0.56), a significant positive association between alcohol use and risky sex; B = 0.59, t = 4.25, p < 0.001), and no significant interaction between the two (B = −0.04, t = −1.2, p = 0.23).
In addition, we examined relationships between event-level continuous measures of substance use and risky sex. First, we regressed risky sex on participants’ reported frequency of alcohol and marijuana use during sex, controlling for age, gender, and relationship status in a multiple regression. We found that marijuana use before sex, controlling for alcohol use before sex, was positively, but not significantly related to risky sex (B = 0.49, t = 1.68, p = 0.09), while alcohol use before sex, controlling for marijuana use before sex, was significantly related to risky sex (B = 0.80, t = 2.23, p = 0.03).
Protected Sex and Condom Use Intentions at Follow-Up
While the cross-sectional analyses confirm an association between substance use and risky sexual behavior, examining intentions and risk behavior 3 months after the assessment of substance use allows us to test whether higher levels of substance use put an adolescent at greater risk of subsequent risky sexual behavior. While it is not possible to randomly assign adolescents to use substances or not (which would provide the sine qua non for causal assertions) we were able to conduct analyses that allow for temporal precedence between baseline substance use and later sexual risk behavior. We examined the same relationships between substance use group at baseline and the risky sex index measure and condom use intentions at the three-month follow-up period, which goes a step beyond the original analysis in testing a directional association. As we did previously for the cross-sectional analyses, we examined these relationships using ANCOVA, with the follow-up measures as dependent variables and substance use group as the independent variable of interest; however, because the larger study involved a sexual risk reduction intervention with multiple groups (cf., [22]), we also controlled for intervention condition in these analyses, as well as the same covariates (age, gender, and relationship status) used in the cross-sectional analyses.
In a model predicting risky sexual behavior at the three-month follow-up, substance use at baseline did not predict past three-month risky sexual behavior as measured by the risky sex index. Notably, however, about half (52.2%) of participants reported that they had not had sex in the past 3 months, and thus were coded as 0 on this measure.Footnote 1 When looking only at participants who reported having sex during the three-month follow-up period (n = 118), these analyses mirrored the pattern of the cross-sectional results, though the pairwise comparisons did not meet Bonferroni-corrected levels of statistical significance. Controlling for intervention condition, gender, age, and relationship status, the overall model was significant (F 7,109 = 2.297, p = 0.03). The both group reported more risky sex than the marijuana group (t = 1.92, p = 0.058). The alcohol group reported more risky sex than the marijuana group (t = 2.08, p = 0.04). The alcohol and both groups were not significantly different from one another (t = 0.54, p = 0.58).
We observed a similar pattern when examining intentions to use condoms at follow-up as an outcome. In this model, the both group reported marginally weaker intentions to use condoms 3 months later than the marijuana group (t = 2.40, p = 0.017). The alcohol group also reported weaker intentions to use condoms 3 months later than the marijuana group, although this difference was not significant (t = 1.53, p = 0.13). The alcohol and both groups did not significantly differ in their intentions to use condoms at follow-up (t = 0.22, p = 0.82).
Given that intentions should predict later behavior, another question is whether the intentions measures for which we observed group differences at baseline are associated prospectively with behavior at follow-up. In the cross-sectional analyses, we observed differences in scenario-specific intentions for condom use between groups, and so we examined whether such intentions were correlated with behavior at follow-up. Indeed, among participants who had had sex in the past 3 months at follow-up, we found that higher scenario-specific intentions at baseline were positively correlated with condom use at follow-up (no alcohol or marijuana scenario r = 0.25, p < 0.006, alcohol scenario r = 0.26, p = 0.005, marijuana scenario r = 0.22, p = 0.02).
Discussion
Across multiple measures of risky sexual behavior and condom use intentions, both cross-sectionally and prospectively, we found that adolescents who frequently used marijuana, but not alcohol (the “marijuana group”), reported significantly less risky sexual behavior as well as greater intentions to use condoms than either adolescents who frequently used alcohol, but not marijuana (the “alcohol group”), or adolescents who frequently used both substances (the “both” group). Additionally, we consistently observed that adolescents who used both substances did not differ substantially from those who were primarily heavy alcohol users. Further, although higher frequency of alcohol use was associated with more risky sex, higher frequency of marijuana use was not. To be clear, the vast majority of adolescents in all three groups were engaging in risky sexual behavior; recall that only 36% of our sexually active participants reported using a condom at most recent intercourse. Thus our data do not suggest that marijuana use does not contribute to risky sexual behavior, as other data from our group show that the two are indeed related when marijuana users are examined relative to nonusing controls [35]. Rather, these analyses speak to matters of degree of sexual risk associated with patterns of substance use.
Our findings add to the limited and conflicting literature examining whether different associations exist between marijuana versus alcohol and sexual risk behavior. The results of our study are relatively consistent with Hingson et al. [10] and Guo et al. [11], who found stronger associations between alcohol use and risky sex than between marijuana use and risky sex in samples of non-justice involved young adults. However, our findings diverge from the more recent study by Ritchwood et al., who found significant independent/additive effects of alcohol use and marijuana use on risky sexual behavior that were relatively larger for marijuana use [14]. It is important to note that the amount of risky sexual behavior as well as substance use was considerably higher in our sample of justice-involved adolescents than in their community sample of low-SES African American youth. For example, in their sample only 13% had used marijuana more than once in the past year, while in our sample 75% were current marijuana users and the average frequency of use across the sample was between 4–5 times per month and once per week. Thus our study is perhaps better able to validly examine whether frequency of use is associated with sexual risk, as we had very high levels of each, rather than a highly skewed distribution representing a minority of young people engaging in either risk behavior with any frequency. Our findings also differ from Kingree and Betz [13], who found that justice-involved adolescents were more likely to have reported use of marijuana than alcohol before risky sex, and Kingree et al. [12] who found that greater use of marijuana, but not alcohol, was associated with risky sex. There are several possible reasons for this discrepancy. Differences in study location (Georgia vs. New Mexico), sample race/ethnicity (66% Black vs. 67% Hispanic) and time period (late 1990s vs. late 2010s) between the studies may explain the divergent pattern of our findings. It is also notable that Kingree et al. [12] included several covariates in their regression models (e.g., age, gender, race, future orientation, condom attitudes, AIDS knowledge), but did not include relationship status. These differences in covariates used in our studies or even potential suppression effects in their models could explain our differing results. Ultimately, there is simply very little research in the area of marijuana use and risky sexual behavior, so we need more data from diverse samples in order to clarify the conditions under which marijuana versus alcohol versus the co-occurring heavy use of both substances has the strongest relationship to risky sex.
Our findings should be viewed in light of some limitations. Due to the high rates of overall substance use in our sample, we could not include a group of similar adolescents who do not use either of these substances, and our heavy marijuana and heavy alcohol groups did use relatively small amounts of the other substance. Additionally, our data do not provide insight into a mechanism for why we observe these differences. In other words, why are marijuana-using adolescents less likely to engage in risky sex and more likely to report intentions to use condoms? Although we can speculate that perhaps alcohol increases sensitivity to rewarding outcomes (like sexual intercourse without a condom) in ways that marijuana might not (cf., [36]), we do not have direct evidence that this is the case and this is clearly an area that requires further study.
In addition, our data are largely cross-sectional, and although our longitudinal data supports our cross-sectional findings, we are of course unable to randomly assign adolescents to use alcohol or marijuana. Therefore, we do now know whether heavier alcohol use causes adolescents to engage in behavior that is riskier, or whether adolescents who are predisposed to heavy alcohol use are simply also more likely to take risks across behavioral domains. We were also limited in that our sample contained a large number of heavy marijuana users, and thus, there were significantly fewer adolescents in the “alcohol-only” group relative to the other two groups. Importantly, however, poly-substance use is the more typical pattern for adolescents who engage in substance use [37], so the finding that those with heavy use of both alcohol and marijuana engage in high levels of sexual risk suggests that this is a particularly high risk group and consequently an important group to target for sexual risk reduction (cf., [21]). That said, however, this group did not differ in their risk behavior from adolescents who primarily used alcohol only.
There is recent and emerging empirical work from the clinical cognitive neuroscience literature that suggests alcohol and marijuana have different consequences for brain development and functioning in adolescence [38,39,40,41]. In terms of the acute effects of each substance on cognition, motivation, and behavior, there is also evidence that the two substances differ. Lane et al. [36] provide an excellent review of the similarities and differences in alcohol and marijuana in terms of molecular mechanisms of action, and demonstrated experimentally that in a risky decision making ask, both drugs increased the selection of the more risky option. Importantly, though, they did so via different biases; while alcohol intoxication increased sensitivity to gains and losses, marijuana intoxication affected learning/memory processes associated with the expected payoffs of risky versus non-risky options. As another example of dissociation of the acute effects of these substances, De Sousa Fernandes Perna et al. [42] showed that while alcohol intoxication increased aggression in response to an aggression prime, marijuana intoxication decreased aggression in response to the same prime. Outside the laboratory, there is increasing evidence that the effects of these substances on real-world behavior also differ. For example, while marijuana use has acute effects on cognition that impair driving, this risk is vastly lower than the risk of alcohol use for being in a fatal automobile crash (e.g., [43]). These related lines of evidence converge to suggest that there is ample reason to believe that the effects of alcohol versus marijuana on sexual decision-making could differ, and that these differences could be the result of either the effects of marijuana versus alcohol directly on brain structure and function over time or the result of effects on risky decision-making acutely. Rigorous experimental work on the acute effects of alcohol versus marijuana on sexual decision-making in adolescents is near-impossible, and thus studies like ours that attempt to understand the nature of the associations of these variables as they occur in the real world are critical.
It is perhaps only through the continued study of these associations in different sub-populations of adolescents, and the quantitative synthesis of such studies, that we may eventually have some clarity on the overlap versus dissociation of the influences of alcohol and marijuana use on sexual behaviors that place adolescents at risk. With regard to the effects of marijuana in particular, we are really only at the tip of the iceberg in terms of our understanding, and more research is critically needed [44]. That said, our data suggest that when designing interventions to reduce substance use in the context of risky sexual behavior, it might be especially effective to preferentially target efforts toward reducing harm associated with alcohol use, both in the context of marijuana use and alone.
Notes
In a logistic regression controlling for intervention condition and the same covariates, baseline substance use group did not predict whether or not participants reported having had sex in the past 3 months.
References
Centers for Disease Control (CDC). HIV among youth. 2016. http://www.cdc.gov/hiv/group/age/youth/index.html.
Teplin L, Mericle A, McClelland G, Abram K. HIV and AIDS risk behaviors in juvenile detainees: implications for public health policy. Am J Public Health. 2003;93(6):906–12.
Armour J, Hammond S. Minority youth in the juvenile justice system: disproportionate minority contact. Washington, DC: National Conference of State Legislators; 2009.
Ritchwood TD, Ford H, DeCoster J, Lochman JE, Sutton M. Risky sexual behavior and substance use among adolescents: a meta-analysis. Child Youth Serv Rev. 2015;52:74–88.
Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schulenberg JE. Monitoring the future national survey results on drug use: 1975–2014: overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, The University of Michigan; 2015.
Hopfer C. Implications of marijuana legalization for adolescent substance use. Subst Abus. 2014;35(4):331–5.
Montanaro E, Ewing SWF, Bryan AD. What works? An empirical perspective on how to retain youth in longitudinal HIV and substance risk reduction studies. Subst Abus. 2014;36(4):493–9.
Teplin LA, Abram K, McClelland G, Mericle A, Dulcan M, Washburn D. Psychiatric disorders of youth in detention. Washington, DC: Office of Juvenile Justice and Delinquency Prevention Juvenile Justice Bulletin; 2006.
Teplin LA, Abram KM, Washburn JJ, Welty LJ, Hershfield JA, Dulcan MK. Northwestern juvenile project: overview. Washington, DC: US Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention; 2013.
Hingson R, Strunin L, Berlin B, Heeren T. Beliefs about AIDS, use of alcohol and drugs, and unprotected sex among Massachusetts adolescents. Am J Public Health. 1990;80(3):295–9.
Guo J, Chung I-J, Hill KG, Hawkins JD, Catalano RF, Abbott RD. Developmental relationships between adolescent substance use and risky sexual behavior in young adulthood. J Adolesc Health. 2002;31(4):354–62.
Kingree J, Braithwaite R, Woodring T. Unprotected sex as a function of alcohol and marijuana use among adolescent detainees. J Adolesc Health. 2000;27:179–85.
Kingree J, Betz H. Risky sexual behavior in relation to marijuana and alcohol use among African-American, male adolescent detainees and their female partners. Drug Alcohol Depend. 2003;72(2):197–203.
Ritchwood TD, DeCoster J, Metzger IW, Bolland JM, Danielson CK. Does it really matter which drug you choose? An examination of the influence of type of drug on type of risky sexual behavior. Addict Behav. 2016;60:97–102.
Simons JS, Maisto SA, Wray TB. Sexual risk taking among young adult dual alcohol and marijuana users. Addict Behav. 2010;35(5):533–6.
Archive The National Juvenile Court Data. Juvenile court statistics 2009. Pittsburgh: National Center for Juvenile Justice; 2009.
Bryan A, Rocheleau CA, Robbins RN, Hutchinson KE. Condom use among high-risk adolescents: testing the influence of alcohol use on the relationship of cognitive correlates of behavior. Health Psychol. 2017;24(2):133–42. doi:10.1037/0278-6133.24.2.133.
Bryan AD, Schmiege SJ, Magnan RE. Marijuana use and risky sexual behavior among high-risk adolescents: trajectories, risk factors, and event-level relationships. Dev Psychol. 2012;48(5):1429–42.
Schmiege SJ, Bryan AD. Heterogeneity in the impact of marijuana use and alcohol use on risky sexual behavior among justice-involved youth: a regression mixture modeling approach. AIDS Behav. 2016;20(4):821–32.
Rosengard C, Stein LAR, Barnett NP, Monti PM, Golembeske C, Lebeau-Craven R. Co-occurring sexual risk and substance use behaviors among incarcerated adolescents. J Correct Health Care. 2006;12(4):279–87. doi:10.1177/1078345806296169.
Skeem JL, Scott E, Mulvey EP. Justice policy reform for high-risk juveniles: using science to achieve large-scale crime reduction. Annu Rev Clin Psychol. 2014;10:709–39.
Callahan TJ, Montanaro E, Magnan RE, Bryan AD. Project MARS: design of a multi-behavior intervention trial for justice-involved youth. Transl Behav Med. 2013;3(1):122–30.
Williams ML, Freeman RC, Bowen AM, Zhao Z, Elwood WN, Gordon C, et al. A comparison of the reliability of self-reported drug use and sexual behaviors using computer-assisted versus face-to-face interviewing. AIDS Educ Prev. 2000;12(3):199–213.
Schmiege SJ, Broaddus MR, Levin M, Bryan AD. Randomized trial of group interventions to reduce HIV/STD risk and change theoretical mediators among detained adolescents. J Consult Clin Psychol. 2009;77(1):38.
Sobell LC, Sobell MB. Timeline follow-back. In: Measuring alcohol consumption. New York: Springer; 1992. p. 41–72.
Bryan A, Fisher JD, Fisher WA. Tests of the mediational role of preparatory safer sexual behavior in the context of the theory of planned behavior. Health Psychol. 2002;21(1):71–80.
Bryan A, Aiken LS, West SG. HIV/STD risk among incarcerated adolescents: optimism about the future and self-esteem as predictors of condom use self-efficacy. J Appl Soc Psychol. 2004;34(5):912–36.
Rubin R. US prisons missing opportunities to tackle HIV in inmates. Lancet. 2016;388(10049):1041–2.
Bryan AD, Aiken LS, West SG. Young women’s condom use: the influence of acceptance of sexuality, control over the sexual encounter, and perceived susceptibility to common STDs. Health Psychol. 1997;16(5):468–79. doi:10.1037/0278-6133.16.5.468.
Bryan A, Schindeldecker MS, Aiken LS. Sexual self-control and male condom-use outcome beliefs: predicting heterosexual men’s condom-use intentions and behavior. J Appl Soc Psychol. 2001;31(9):1911–38. doi:10.1111/j.1559-1816.2001.tb00210.x.
Broaddus MR, Schmiege SJ, Bryan AD. An expanded model of the temporal stability of condom use intentions: gender-specific predictors among high-risk adolescents. Ann Behav Med. 2011;42(1):99–110. doi:10.1007/s12160-011-9266-0.
Robertson AA, Stein JA, Baird-Thomas C. Gender differences in the prediction of condom use among incarcerated juvenile offenders: testing the information-motivation-behavior skills (IMB) model. J Adolesc Health. 2006;38(1):18–25.
Schmiege SJ, Levin ME, Bryan AD. Regression mixture models of alcohol use and risky sexual behavior among criminally-involved adolescents. Prev Sci. 2009;10(4):335–44.
Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2013. Atlanta: US Department of Health and Human Services; 2014. http://www.cdc.gov/std/stats13/surv2013-print.pdf.
Schmiege SJ, Bryan AD. Heterogeneity in the relationship of substance use to risky sexual behavior among justice-involved youth: a regression mixture modeling approach. AIDS Behav. 2015;20(4):821–32.
Lane SD, Yechiam E, Busemeyer JR. Application of a computational decision model to examine acute drug effects on human risk taking. Exp Clin Psychopharmacol. 2006;14(2):254–64.
Moss HB, Chen CM, Yi H. Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug Alcohol Depend. Elsevier. 2014;136:51–62.
Jacobus J, Squeglia LM, Bava S, Tapert SF. White matter characterization of adolescent binge drinking with and without co-occurring marijuana use: a 3-year investigation. Psychiatry Res Neuroimaging. 2013;214(3):374–81.
Jacobus J, McQueeny T, Bava S, Schweinsburg BC, Frank LR, Yang TT, et al. White matter integrity in adolescents with histories of marijuana use and binge drinking. Neurotoxicol Teratol. 2009;31(6):349–55.
Jacobus J, Squeglia LM, Sorg SF, Nguyen-Louie TT, Tapert SF. Cortical thickness and neurocognition in adolescent marijuana and alcohol users following 28 days of monitored abstinence. J Stud Alcohol Drugs. 2014;75(5):729–43.
Schweinsburg AD, Schweinsburg BC, Nagel BJ, Eyler LT, Tapert SF. Neural correlates of verbal learning in adolescent alcohol and marijuana users. Addiction. 2011;106(3):564–73.
De Sousa Fernandes Perna EB, Theunissen EL, Kuypers KPC, Toennes SW, Ramaekers JG. Subjective aggression during alcohol and cannabis intoxication before and after aggression exposure. Psychopharmacology. 2016;233(18):3331–40.
Romano E, Torres-Saavedra P, Voas RB, Lacey JH. Drugs and alcohol: their relative crash risk. J Stud Alcohol Drugs. 2014;75(1):56–64.
McCormick M, Abrams, DI, Alegria M, Checkley W, Collins RL, Cooper Z, Du Plessis AJ, Feldstein Ewing SW, Hennessy S, Hutchison K, Kaminski NE, Patel S, Piomelli D, Sidney S, Wallace RB, Williams JW. Committee on the Health Effects of Marijuana: an evidence review and research agenda. The health effects of cannabis and cannabinoids: the current state of evidence and recommendations for research. A Report of the National Academies of Sciences, Engineering, & Medicine. Washington, DC: The National Academies Press; 2017.
Saunders J, Aasland O, Babor T. Development of the alcohol use disorders identification test (AUDIT). WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction. 1993;88(6):791–804.
Stephens R, Roffman R, Curtin L. Comparison of extended versus brief treatments for marijuana use. J Consult Clin Psychol. 2000;68(5):898–908.
Acknowledgements
This research was funded by a grant from NIH/NIAAA (Grant Number 2R01AA013844) to Angela Bryan. We would like to thank Jairo Ramos for his help with the Spanish translation of our abstract.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Arielle Gillman, Elizabeth Yeater, Sarah Feldstein Ewing, Alberta Kong, and Angela Bryan declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Gillman, A.S., Yeater, E.A., Feldstein Ewing, S.W. et al. Risky Sex in High-Risk Adolescents: Associations with Alcohol Use, Marijuana Use, and Co-Occurring Use. AIDS Behav 22, 1352–1362 (2018). https://doi.org/10.1007/s10461-017-1900-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-017-1900-9