
Abstract
Background
Adolescents involved with the criminal justice system are at particularly high-risk for the Human Immunodeficiency Virus and sexually transmitted infections.
Purpose
The purpose of this study was to longitudinally examine gender-specific models of condom use, incorporating temporal stability of intentions.
Methods
Adolescents on probation (N = 728) were recruited to complete longitudinal surveys including measures of Theory of Planned Behavior and gender-specific constructs, relationship length, and condom use.
Results
Gender-specific models of condom use behavior suggested by previous research were mostly replicated. For young women, the effect of baseline intentions on subsequent condom use behavior was stronger when intentions were either stable or increasing. For young men, more stable, increasing intentions were directly associated with more condom use. There was preliminary evidence to suggest an association between temporal stability of intentions and decreasing condom use in stable relationships.
Conclusions
Intervention efforts should be tailored by gender and aim to forestall decreasing intentions and condom use over time by addressing difficulties in maintaining condom use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Approximately 19 million new cases of sexually transmitted infections (STIs) are reported every year, with adolescents representing around half of these cases [1]. Furthermore, 13 to 29 year olds accounted for approximately 34% of new Human Immunodeficiency Virus (HIV) infections in 2006 [2]. Adolescents involved with the juvenile justice system are a subgroup at particularly high risk for HIV and STIs [3, 4], so much so that some have suggested arrest history as a marker for HIV risk [5]. Higher rates of anal intercourse, a greater number of sex partners, and lower rates of condom use have been documented among justice system-involved adolescents relative to the general adolescent population [6], all leading to high rates of unintended pregnancy and STIs [6, 7]. The aims of the current research are first to understand the psychological processes underlying condom use in this population with high levels of risky sexual behavior, by testing gender-specific models of condom use, which have at their core the Theory of Planned Behavior (TPB) as a theoretical framework. Second, we aim to incorporate stability of intentions to use condoms over time within these gender-tailored TPB-based models to extend research on how stability of intentions moderates the effect of intentions on behavior, and how this may differ by gender. These questions are important theoretically as well as practically, to inform the design of interventions with the capacity to decrease risky sexual behavior and maintain safer behavior over time in this population at very high risk of negative outcomes.
Justice System-Involved Adolescents
Previous research has shown that justice system-involved adolescents have lower levels of condom use than the general population of adolescents [5], leading to high rates of STIs. The Centers for Disease Control and Prevention (CDC) gathered data from 38 states and Puerto Rico that test young people for STI at entry into a juvenile detention center. As an example, the rate of chlamydia in that sample was 6.1% in young men and 13.8% in young women between the ages of 12 and 18 years. CDC STI surveillance data for adolescents between the ages of 15 and 19 years in the general population, in contrast, show that less than 1% of young men and only 3% of young women tested positive for chlamydia [4]. There is an abundance of research on possible mechanisms of this discrepancy in risky sexual behavior and STI incidence, including differences in personality constructs such as future orientation, optimism for the future, and self-esteem [8–10], as well as structural barriers such as poverty [11]. Another factor that compounds these risks is that justice-involved adolescents are exactly the group that may miss the benefit of standard HIV/STI and pregnancy prevention programs, which are typically delivered in school settings [12]. Truancy is a major reason for adolescents being in the juvenile justice system, and, in fact, it is so pervasive and its consequences so dire that it has been identified as a “national priority” by the Office of Juvenile Justice and Delinquency Prevention [13]. Finally, these adolescents may be more vulnerable to sexual health risks in general due to lack of stable home environments, inadequate social support, and lack of economic assets [14–17], which make interventions tailored to this population essential.
Despite increasing numbers of young women in the juvenile justice system [18], historically, work with justice system-involved adolescents has often been confined to young men [19–22]. Gender-specific predictors of safer sexual behavior are important to explore given the gendered nature of condom use in general [23], and gender-specific interventions have been suggested by numerous epidemiological reports due to increased risk for STI among young women in juvenile justice [24, 25]. The few studies that have focused on young women or gender differences in the juvenile justice population have typically emphasized relationships between gender and STI/HIV prevalence [25, 26]. More appropriate may be a consideration of how the gendered nature of heterosexual relationships might influence the structural differences in the theory-based prediction of condom use in young men versus young women in the juvenile justice system. As one example, Robertson, Stein, and Baird-Thomas [27] found structural differences in a theoretical model of condom use suggesting different key determinants of condom use for young men versus women. However, this study was limited by its cross-sectional design and is characterized by postdiction (i.e., with current beliefs “predicting” past behavior) [28, 29]. Additionally, Robertson et al. only examined differences between the genders on a set of general constructs, without a consideration of potential gender-specific antecedents. We aim to fill these gaps in the research by using a longitudinal design and testing tailored and previously validated path models of condom use that incorporate gender-specific constructs [23, 30].
The Theory of Planned Behavior and Gender
We use the TPB [31] as the basis for our gender-specific models, which has been widely validated in the context of condom use behavior [32] as well as other health-related behaviors such as physical activity [33, 34] and healthy eating [35]. The TPB includes only general predictors, as opposed to gender-specific predictors and has rarely been tested among high-risk justice system-involved populations. TPB variables of attitudes, norms, self-efficacy,Footnote 1 and intentions account for a substantial proportion of variability in condom use behavior across studies, but further work is warranted regarding potential antecedents of these constructs. Many have noted the theoretical insufficiency of social cognitive health behavior theories such as TPB in capturing contextual factors associated with health behaviors [36–38], and the gendered context of condom use is likely to be one of those situations [39]. The gender-tailored models tested here build upon a small amount of work that has introduced female- and male-specific constructs into a TPB framework as a means to capture gendered roles in the sexual script.
In a study of college women, two female-specific constructs, acceptance of sexuality and control over the sexual encounter, were implicated in women’s self-efficacy to use condoms, which in turn predicted their intentions [23]. The development of the acceptance of sexuality construct was built upon research suggesting that young women are less likely than men to believe they will have sexual intercourse, feel guiltier about doing so, and feel less responsibility for their sexuality [40–42]. The development of the control over the sexual encounter construct was built upon research suggesting that a particular barrier to women’s condom use is a lack of perceived control over what occurs during the sexual encounter [42–44], or feelings of powerlessness during sex [45, 46].
In a study of college men testing a male-specific TPB model, the male-specific construct of sexual self-control predicted greater self-efficacy and male-specific condom attitudes were positively related to general attitudes toward condom use [30]. The development of the sexual self-control construct was built upon research suggesting that men had lower perceived self-control or ability to stop sexual activity once it has been initiated with regard to condom use than did women [47]. The development of the male-specific condom attitudes construct was built upon research into specific outcome beliefs held by men, including that condoms are inconvenient to use [48, 49], are difficult to put on and keep on [50], have insufficient lubrication [50, 51], and that putting on a condom causes a loss of erection.
The prior work on gender-specific TPB models was conducted in college populations, and it is possible that the dynamics of the gendered experience of condom use are different among higher risk adolescents, both for reasons of culture, education, and opportunity as well as differences in developmental stage. Therefore, an aim of the current research is to empirically test the structure of these models in a sample of justice system-involved adolescents using a path analytic approach. Consistent with the TPB, the gender-specific constructs are positioned as antecedents of the core constructs of attitudes, norms, and self-efficacy (c.f., 52, 53) and are thus meant to increase the specificity of the model in terms of its ability to account for variability in the core TPB constructs associated with condom use intentions and behaviors among high-risk adolescent young men versus young women.
The Theory of Planned Behavior and Temporal Stability of Intentions to Use Condoms
Another weakness of the traditional TPB model is that the constructs were originally conceptualized as static, but these cognitions have actually been shown to change over time as a result of internal and external influences, and this is especially the case for intentions [54]. A growing body of research suggests that “temporal stability of intentions” [55, 56] may be one reason for the suboptimal prediction of behavior from intentions and other TPB constructs (i.e., the more stable intentions are over time, the better they predict behavior) [55]. In situations where relatively inconsistent frequency of intercourse, switching of partners and concurrent partnerships are common, as is the case with adolescent sexual behavior [57], condom use intentions are likely to be especially vulnerable to instability. Therefore, incorporating the phenomenon of temporal stability into the larger framework of the TPB is a second aim of the current research, with a focus on how this may differ for men and women. There is already some evidence that the relationship between condom use intentions and behaviors may be different for men versus women. For example, Von Haeften, Fishbein, Kaspryzk, and Montano [58] reported that, while men and women had similar intentions to use condoms, men were more successful in actually carrying out their condom use intentions. Thus, not only might there be gender-specific predictors of intentions, there may be gender-specific patterns in the stability of intentions over time that influence the intention–behavior relationship for young men versus young women.
In addition to the two primary aims of the study, we also wanted to conduct an exploratory analysis of the association between a change in relationship partner with a change in intentions to use condoms. A change in partner is one of many possible contextual factors likely to impact change in intentions to use condoms among adolescents. Indeed, recent research suggests a longitudinal effect of partner change on STI acquisition in adolescent women [59]. The effect of partner change may differ by gender, as previous research has indicated relationship pressures may act on women more than men in condom use decisions [60]. Given the nature of the use of male condoms, where a man can unilaterally make the decision to use a condom while a woman must negotiate her desires with each different partner [61], men’s condom use intentions may remain stable regardless of relationship switching while women’s intentions may be more likely to fluctuate based on partner switching.
Overview of Current Research
The current research first aimed to replicate and confirm previously validated gender-specific expanded TPB models of condom use in a sample of high-risk, justice system-involved adolescents in a path-modeling framework using a longitudinal design. By using gender-specialized measures of the antecedents of attitudes and self-efficacy, we aimed to understand the psychological processes underlying the proximal determinants of condom use and how they differed by gender (see Fig. 1). These models were drawn directly from the Bryan et al. studies [23, 30]. A second aim was to expand upon the Bryan et al. studies by incorporating temporal stability of intentions within the framework of the TPB. We expected that intentions would predict condom use more strongly for those whose intentions were more stable and increasing, and that TPB constructs of attitudes, norms, and self-efficacy might also predict stability of intentions. Finally, we conducted an exploratory analysis to examine the possibility that a change in relationship may be one contributor to the instability of intentions. We expected a change in relationship to be associated with more unstable intentions and that this effect would be moderated by gender.

Hypothesized models of condom use. Male-specific constructs and relationships are represented by dashed lines, female-specific constructs and relationships are represented by dotted lines
Methods
Participants
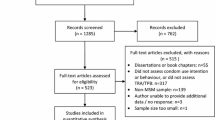
Data for these analyses were taken from a larger longitudinal study assessing substance use and sexual risk among adolescents (total baseline, n = 728) recruited from juvenile probation offices in the Denver metropolitan area. Participants answered questions about their substance use and sexual behavior every 6 months over a 2-year period, and data from the first three waves of collection are utilized here. Youth were tracked in multiple ways throughout the course of the study (e.g., obtaining contact information for someone who would always know where they are), and we stayed in close contact with participants through reminder phone calls and mailings. Using these procedures, we were able to maintain high retention rates of 90.1% (n = 656) and 85.7% (n = 624) at the 6-month and 12-month follow-ups, respectively. Of those participants who completed follow-up measures, 24% (n = 161) had not engaged in sexual intercourse in the 6 months preceding the 12-month follow-up and were not included in analyses related to condom use. At baseline, participants (485 men and 243 women) had a mean age of 15.71 years (SD = 1.05; range, 14–18). The sample was ethnically diverseFootnote 2: 40.9% were Hispanic, 24.5% were African-American, 15.7% were White, 11.6% were multi-racial, 3.4% were American-Indian/Alaskan Native, 1.1% was Asian/Pacific Islander, and the remaining 2.9% did not identify their race/ethnicity. In terms of sexual orientation, we found that 6% and 26% of women reported being sexually attracted to the same sex and both sexes, respectively. For men, 3% and 2% of men reported same- and both-sex attraction, respectively.Footnote 3 Of those participants who reported being in a relationship at baseline (n = 431), 15% described the relationship as “Casually Dating,” 39% as “Steadily Dating,” and 46% as “Seriously Committed.”
Procedures
Posters advertising the opportunity to be involved in research were placed in the waiting rooms of youth probation offices. During peak hours, research staff approached young people waiting for appointments and asked if they were interested in information about a longitudinal research study about health and risk behaviors. If interested, a brief description of the study was provided. Eligibility criteria including being (1) 14–18 years old, (2) currently on probation, (3) able to speak and read English, (4) cognitively capable of understanding the assent information, and (5) having fully informed consent of a parent or legal guardian (unless 18 years old). Written informed assent was obtained from each participant (or informed consent in the case of 18-year-old participants) and recorded verbal consent via tape-recorded phone calls was obtained from each parent/guardian for youth under the age of 18 years. Probation and juvenile justice staff had no involvement in recruitment, and the decision to participate or not had no impact on the young person’s probation status or treatment. Participants received $20 for completing the baseline assessment and $50 for each of the follow-up assessments. All procedures were reviewed and approved by the local IRB, and a federal certificate of confidentiality was obtained from NIH/NIDA. Questionnaire data were collected using Audio Computer-Assisted Self-Interviewing (ACASI) technology on individual laptop computers, with the questions also read over headphones to minimize issues with literacy in this population [44–46]. Baseline questionnaires were completed at the probation offices and follow-up questionnaires were completed at a location convenient for the adolescent (e.g., their home, a coffee shop) or over the phone by a trained research assistant if an in-person survey was impossible (e.g., the adolescent moved out of state).
Measures
Full descriptions and reliability information of measures used for analyses at baseline can be seen in Table 1. Although both genders completed scales measuring gender-specific constructs, they were distinctly developed for the appropriate gender and were not meant to be equally applicable to the opposite gender. Therefore, means and alphas for the gender-specific constructs represent that of their appropriate gendered participants only. All of these measures were answered on four-point Likert scales ranging from “Disagree a lot” to “Agree a lot,” and scale scores were calculated as a mean of the items comprising each scale.
Intentions were measured using four items at both baseline and 6-month follow-up (α = 0.82 and 0.87, respectively) and asked participants to indicate the likelihood they would buy condoms, carry condoms when they go out, talk to a partner about condoms, and use a condom every time they have sexual intercourse in the subsequent 6 months. This measure has shown high reliability and validity across various adolescent samples [8, 23, 62–64]. Response options were: “Will not happen,” “Probably won’t happen,” “Probably will happen,” and “Will definitely happen.” An index of temporal stability of intentions was calculated from baseline and 6-month follow-up answers on the four intentions questions using modified methods developed by Conner, Sheeran, and Armitage [65] to measure the absolute amount of change in between waves of longitudinal data. We have revised this measure to include the direction of change in intentions. Therefore, in our measure of Directional temporal stability, a zero score indicates no change in intentions; positive values indicate increasing intentions (with higher numbers indicating more change), and negative values indicate decreasing intentions (with lower numbers indicating more change). This variable is calculated as a single index based on the average of four distinct ways of calculating differences between baseline and follow-up: (1) the difference between the two mean scores on the scale, (2) the mean of the differences between individual items, (3) the mean of proportion of change to amount of possible change of individual items, and (4) the number of items changed, after standardization. In order to examine the interaction between baseline intentions and temporal stability within our path models, an interaction term was calculated by multiplying scores on baseline intentions and temporal stability scales. Condom use at baseline and 12-month follow-up was measured with one item: “In the past 6 months, how much of the time did you use condoms when you had sexual intercourse?” Response options were: “Never,” “Almost Never,” “Sometimes,” “Almost Always,” and “Always.”
We measured Relationship Change between baseline and 6-month follow-up by asking first if participants were currently in a relationship at baseline (yes/no).Footnote 4 For those participants at baseline who indicated that they were in a relationship (n = 431), we determined if they were in the same relationship at 6-month follow-up by coding the number of months they had been in their relationship at follow-up as greater than or equal to 6 (i.e., in same relationship; n = 166) versus below 6 (i.e., not in same relationship, n = 265).
Overview of Analysis
For descriptive analysis, t tests were run on general TPB variables to look for differences by gender, using a Bonferroni correction to adjust for the number of comparisons (α = 0.005). Next, path models were estimated to test the gender-specific models of intentions in Fig. 1, with baseline intentions predicting condom use at the 12-month follow-up. Twelve-month condom use was used as the outcome variable following suggestions from previous research to measure intentional stability prior to behavior in longitudinal studies [65]. Drawing upon previous research concerning the different experiences of condom use between the genders [23, 27, 30], we expected the gender-specific constructs to be important only to the gender for which they were designed, and thus estimated confirmatory models consistent with the literature, as opposed to including all constructs in all models. Finally, regression analyses were conducted to explore the effect of relationship change on temporal stability, as one potential contributor to the instability of intentions. We expected relationship change from baseline to 6-month to be associated with temporal stability of intentions from baseline to 6-month, and we explored whether these analyses were moderated by gender.
Results
Condom use was low, with only 31% of participants at 12-month follow-up reporting “Always” using a condom in the previous 6 months, while 14% reported “Never” using a condom. Results indicated a number of gender differences (see Table 2). Specifically, young men reported significantly more frequent condom use at baseline and at 12-month follow-up, less positive attitudes toward condom use, and more positive intentions to use condoms at baseline and follow-up. Surprisingly, young men and women did not differ in temporal stability of intention. The mean of the overall sample differed significantly from zero (M = −0.23, t = -5.82, p < 0.0001), indicating that, on average, participants’ intentions were decreasing over time. One might wonder whether involvement in the juvenile justice system would restrict access to condoms in some way, and this did not appear to be the case. While 73% of participants were still on probation at the 6-month follow-up and 54% at the 12-month follow-up, there were no differences in condom use at 12-month follow-up by probation status, both separated and collapsed by gender.
The model for young women is presented in Fig. 2. Most hypothesized paths in the model were significant, and the model exhibited adequate fit to the data, χ 2 (22, N = 242) = 59.77, p < 0.0001, Comparative Fit Index (CFI) = 0.95, Root Mean Square Error of Approximation (RMSEA) = 0.08, 90% confidence interval (0.06, 0.11), Standardized Root Mean Square Residual (SRMR) = 0.10. Model variables accounted for 19% of the variance in intentions, and 27% of the variance in condom use. As can be seen in Fig. 2, the basic framework of the TPB was confirmed, with more positive condom attitudes, higher self-efficacy, and more positive perceived norms (marginally) all associated with greater intentions to use condoms. The gender-specific construct of control over the sexual encounter, but not acceptance of sexuality, was positively associated with condom use self-efficacy. Not self-efficacy, attitudes, or norms were associated with temporal stability of intentions. Controlling for baseline condom use, condom use at 12 months was predicted by baseline intentions as hypothesized, and although there was no main effect of directional temporal stability of intentions on condom use, temporal stability moderated the effect of baseline intentions on condom use. In other words, the effect of intentions on behavior depended on how stable those intentions were over time. Figure 3 demonstrates the impact of intentions on condom use across three categories on temporal stability: decreasing intentions, stable intentions, and increasing intentions. Specifically, the effect of intentions on condom use was stronger for young women with increasing intentions (directional temporal stability = 1; β = 1.12, p < 0.0001) than non-changing (directional temporal stability = 0; β = 0.88, p < 0.0001) and decreasing intentions (directional temporal stability =−1; β = 0.64, p < 0.001).

Estimated model of 12-month condom use for women, controlling for baseline condom use; + p < 0.10, *p < 0.05, **p < 0.01, ***p < 0.001

Condom use by baseline intentions, temporal stability of intentions, and gender
For young men (see Fig. 4), most hypothesized paths were significant, and the model exhibited adequate fit to the data, χ 2 (18, N = 458) = 133.12, p < 0.0001, CFI = 0.94, RMSEA = 0.12, 90% confidence interval (0.10, 0.14), SRMR = 0.13. The model accounted for 33% of the variance in intentions and 25% of the variance in condom use. The TPB structure was mostly confirmed, with attitudes, norms, and self-efficacy predicting intentions. Male-specific condom attitudes were associated with condom attitudes and sexual self-control with self-efficacy as predicted. Unlike the young women’s model, however, self-efficacy was negatively related to temporal stability of intentions, such that participants with higher self-efficacy reported less stable and decreasing intentions. Attitudes were positively associated with temporal stability, as expected, with more positive attitudes associated with increasing intentions. Controlling for baseline condom use, intentions and directional temporal stability were positively associated with 12-month condom use, with higher intentions at baseline and increasing intentions predicting more condom use. There was no interaction between baseline intentions and directional stability (see Fig. 3, bottom panel).

Estimated model of 12-month condom use for men, controlling for baseline condom use; *p < 0.05, **p < 0.01, ***p < 0.001
Finally, we explored whether changes in relationship may be contributing to the effect of non-stable, decreasing intentions on condom use. As expected, we found a negative association such that being in the same relationship was associated with more unstable and decreasing intentions (M =−0.47) as compared with being in a different relationship or no relationship at 6 months (M =−0.20; F(1, 368) = 7.24, p < 0.01; Cohen’s d = 0.28). Counter to expectations, this effect did not differ by gender.
Discussion
By using gender-specialized antecedents of attitudes and self-efficacy, we aimed to understand the psychological processes underlying condom use within a TPB framework and how they differ structurally by gender. Young men had higher rates of condom use and higher intentions to use condoms than did young women. On the other hand, young women had more positive attitudes towards condoms. Control over the sexual encounter was associated with self-efficacy to use condoms for young women, as expected. Also, as expected, sexual self-control and male-specific attitudes were associated with self-efficacy and attitudes for men, respectively. While attitudes, norms, and self-efficacy were all significant predictors of intentions for young men, only attitudes and self-efficacy met the criteria for significant predictors in young women. This perhaps suggests that norms are a less important determinant of intentions for young women.
Our findings largely replicate the gender-specific models suggested by previous research in college students [33, 34]. This represents the first study of which we are aware to examine gender-specific theoretically based models in a longitudinal study with high-risk adolescents and further underscores the potential need for tailoring interventions by gender in future work. In contrast with work in college students, acceptance of sexuality was not associated with young women’s condom self-efficacy. It should be noted that both the acceptance of sexuality and control over the sexual encounter scales’ reliabilities were somewhat low, a limitation of the current research. Therefore, it is plausible that acceptance of sexuality remains an important construct of interest in high-risk young women, but we may not have the appropriate instrument to measure it in this population. Given the theoretical importance of these constructs, a combination of qualitative and quantitative research might be helpful to develop better measures of acceptance of sexuality and control over the sexual for adolescent young women in future research.
Temporal stability in past research [56, 65] has typically examined only an absolute change in level of intentions, disregarding whether or not that change is in the increasing or decreasing direction. The current research expands upon prior temporal stability work to explore how the direction of the instability influences behavior. In general, condom use intentions decreased over time in this sample, although the effects of these changes in intentions seem to have differed by gender. For young women, and consistent with prior research, the effect of baseline intentions on subsequent condom use behavior was strongest when intentions were increasing [56]. For young men, however, temporal stability had only a main effect on condom use, such that increasing intentions were associated with more condom use.
This study is the first of which we are aware to incorporate temporal stability of intentions into the larger TPB framework, allowing us to examine TBP constructs as predictors of intention stability. None of the theoretical constructs significantly predicted stability for young women, but there was a positive effect of attitudes and a negative effect of self-efficacy on stability for young men. The negative effect on self-efficacy was surprising, and we speculate that perhaps very high levels of self-efficacy may have engendered overconfidence and a resulting lack of self-regulatory vigilance, although this relationship needs to be replicated before any strong assertions are made as to its cause. Regardless, the basic TPB framework has not traditionally taken temporal stability into account. We have shown that researchers interested in studying the TPB structure may need to be cognizant of how condom use intentions may change over time, particularly in adolescence, a developmental stage characterized by relatively unstable and sporadic romantic and sexual behaviors.
Some limitations of the current study should be noted. First, condom use was measured with a single item, which is a limitation despite the fact that this item has high face validity and is well understood by participants with limited reading abilities. Second, our conclusions are limited to those participants who reported having had sex at least once between 6- and 12-month assessments. The inter-assessment period of 6 months is clearly a factor in assessing the temporal stability of intentions, as participants’ estimate of their behavior over the preceding 6 months is likely to be influenced by recall errors [66]. In terms of study generalizability, we have documented that there were n = 387 adolescents who indicated initial interest in the study but who did not participate for a variety of reasons (18.9% ineligible, 3.4% entered detention or treatment after providing assent, 28.4% for whom we were unable to obtain parental consent, and 49.4% who lost interest or repeatedly no-showed). We have no information to compare enrolled participants to those lost before first assessment, but, our sample is comparable in terms of key demographic (e.g., ethnicity) and behavioral (e.g., sexual history) variables to other samples of justice-involved adolescents [63], providing some evidence that our sample is typical of the broader population. As with all studies of sexual behavior, we are limited by the self-report nature of the data. Finally, our study focused on intra-individual social cognitive constructs as predictors of condom use behavior and did not take into account important structural factors, family characteristics, peer and social network characteristics, or partner attributes.
Despite the limitations, we believe our findings have the potential to influence both future research efforts and intervention development for this high-risk population. Further research is warranted to examine why adolescents’ intentions may decrease over time in order to forestall these changes via intervention efforts. Changing partnerships may be one mechanism of decreasing intentions, as we have shown, but research also indicates that day-to-day changes in intentions may be linked to depletion of self-control and mood [67]. Other mechanisms to explain decreasing intentions may include changing motivations for sex (e.g., transitioning from having sex for pleasure to having sex for procreation) [68] or changes in perceived risk [69]. Finally, research suggests that condoms have symbolic meanings in relationships in terms of indicating less fidelity, closeness, commitment, and love [70, 71]. Thus, ceasing condom use may convey a qualitative change in the relationship in degree of commitment, love, and being “serious.” Recent research with adolescents that found a longitudinal link between partner change and STI acquisition also indicated that relationship characteristics of relationship quality, closeness of partner to family, and friends, and length of relationship were negatively associated with subsequent partner change [59]. In future research, qualitative methodology could be used to examine what it means to be in a serious versus casual relationship for this population and what causes this change, and prospective diary methodologies could be used to determine how changes in relationship qualities, changes in relationships, and changes in intentions to use condoms converge to increase STI incidence.
The differing pattern of results for young men and women in this sample of justice system-involved adolescents further underscores the need to be highly cognizant of gender-specific content and potentially the need for tailored interventions. A randomized controlled trial comparing gender-tailored to non-tailored interventions would be the next step for future research in this area. Although our tailored models did not account for additional variability in predicting condom use, we have shown medium-sized effects in predicting more proximal constructs that have been shown to relate to behavior and be amenable to change through intervention. By incorporating the gender-specific constructs into the models, we have accounted for variability in self-efficacy (10% for women and 15% for men) and attitudes (17% for men) that would not be accounted for by the traditional TPB. Incorporating these antecedents in intervention materials could include highlighting ways to maintain control of oneself in the “heat of the moment” in order to enact one’s intentions for young men, thereby increasing their self-efficacy. In addition, teaching male-specific strategies that serve to improve condom attitudes would be important. For example, intervention content could highlight ways to enhance sensitivity for men (e.g., various ways of using lubrication with condoms, preventing loss of erection by waiting until the penis is fully erect before applying the condom). On the other hand, bolstering young women’s perceptions that they have control over the sexual encounter has the potential to increase self-efficacy and intentions [62]. It is important for young women to understand that, while their male partners might not bring up condom use, they overwhelmingly agree to use them when their female partners raise the topic. Finally, for both genders, the inclusion of strategies to forestall the increasing difficulties in maintaining condom use in established relationships is essential.
Conclusions
Young people involved in the juvenile justice system incur tremendous morbidity and mortality due to high rates of sexual risk behavior, and their involvement in the justice system often prevents them from being exposed to HIV/STI risk-reduction interventions delivered in schools. Understanding the social–cognitive as well as interpersonal determinants of safe sexual behavior and then translating those theoretical and empirical findings to the development of interventions that are appropriate to the justice-context continues to be an important and significant area of research with the goal of improving the health of these highly vulnerable young people.
Notes
The traditional conceptualization of the TPB includes the construct “perceived behavioral control.” Perceived behavioral control refers to the degree to which one believes that they can effectively perform the behavior and is considered by many [52] largely synonymous with self-efficacy; therefore, we have used the term “self-efficacy” throughout the paper to refer to this construct.
Given the ethnic diversity of the sample, we explored whether there were racial/ethnic differences in study outcomes. These analyses indicated no mean differences in study constructs between whites and nonwhites, or between Hispanics as compared with other nonwhites after a Bonferroni correction. We also examined the effect of race/ethnicity in the path analysis framework using a cross-groups analysis for each of gender-specific models and did not find significant overall differences (for women: Δχ 2 (df = 12) = 12.62, ns; for men: Δχ 2 (df = 12) = 10.63, ns).
We re-estimated the male- and female-specific models excluding participants who did not report heterosexual attraction, and the results were unchanged. Thus, we included all participants in analyses.
Change in Relationship Type was also measured. Participants described their relationship as “Casually dating,” “Steadily dating,” or “Seriously committed” at both time points. Change was calculated with a difference score. Positive numbers indicated increasing seriousness and negative numbers indicated decreasing seriousness. This construct was not associated with temporal stability and therefore not presented.
References
Weinstock H, Berman S, Cates W. Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspectives on Sexual and Reproductive Health. 2004; 36: 6–10.
Hall HI, Song R, Rhodes P, Prejean J, et al. Estimation of HIV incidence in the United States. JAMA. 2008; 300: 520–529.
Romero EG, Teplin LA, McClelland GM, Abram KM, et al. A longitudinal study of the prevalence, development, and persistence of HIV/sexually transmitted infection risk behaviors in delinquent youth: Implications for health care in the community. Pediatrics. 2007; 119: 1126–41.
Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, 2008. Atlanta, GA: U.S. Department of Health and Human Services; November 2009. Available at http://www.cdc.gov/std/stats08/adol.htm, accessed 10/14/2010.
Tolou-Shams M. Brown LK. Gordon G. Fernandez I. Project SHIELD Study Group. Arrest history as an indicator of adolescent/young adult substance use and HIV risk. Drug & Alcohol Dependence. 2007; 88: 87–90.
Teplin LA, Mericle AA, McClelland GM, Abram KA. HIV and AIDS risk in juvenile detainees: Implications for public health policy. American Journal of Public Health. 2003; 93: 906–12.
Crosby R, Salazar LF, DiClemente RJ, Yarber WL. Health risk factors among detained adolescent females. American Journal of Preventive Medicine. 2004, 27: 404–410.
Bryan AD, Aiken LS, West SG. HIV/STD risk among incarcerated adolescents: Optimism about the future and self esteem as predictors of condom use self-efficacy. Journal of Applied Social Psychology. 2004; 34: 912–936.
Robbins RN, Bryan A. Relationships between future orientation, impulsive sensation seeking, and risk behavior among adjudicated adolescents. Journal of Adolescent Research. 2004; 19: 428–45.
Schmiege SJ, Feldstein-Ewing SW, Hendershot, CS, Bryan AD. Positive outlook as a moderator of the effectiveness of an HIV/STI intervention with adolescents in detention. Health Education Research. In press.
Girard GA. Poverty and inequity in adolescent health care. Adolescent Medicine. 2009; 20: 887–99.
Kirby D. The impact of schools and school programs upon adolescent sexual behavior. Journal of Sex Research. 2002; 39: 27–33.
Henry KL, Huizinga DH. School-related risk and protective factors associated with truancy among urban youth placed at risk. Journal of Primary Prevention. 2007; 28: 505–19.
Hay C, Fortson EN, Hollist DR, Altheimer I, Schaible LM. The impact of community disadvantage on the relationship between the family and juvenile crime. Journal of Research in Crime and Delinquency. 2006; 43: 326–356.
Ge X, Donnellan MB, Wenk E. The development of persistent criminal offending in males. Criminal Justice and Behavior. 2001; 28: 731–755.
Brady SS. Dolcini MM. Harper GW. Pollack LM. Supportive friendships moderate the association between stressful life events and sexual risk taking among African American adolescents. Health Psychology. 2009; 28: 238–48.
Ssewamala, FM, Han C-K, Neilands TB, Ismayilova L, Sperber E. Effect of economic assets on sexual risk-taking intentions among orphaned adolescents in Uganda. American Journal of Public Health. 2010; 100: 483–488.
American Bar Association and the National Bar Association. Justice by Gender: The Lack of appropriate prevention, diversion, and treatment alternatives for girls in the justice system. Available at www.abanet.org/crimjust/juvjus/girls.html. Accessibility verified May 24, 2010.
Elkington KS, Teplin LA, Mericle AA, Welty LJ, et al. HIV/sexually transmitted infection risk behaviors in delinquent youth with psychiatric disorders: A longitudinal study. Journal of the American Academy of Child & Adolescent Psychiatry. 2008; 47: 901–11.
DiClemente RJ. Predictors of HIV-preventive sexual behavior in a high-risk adolescent population: The influence of perceived peer norms and sexual communication on incarcerated adolescents’ consistent use of condoms. Journal of Adolescent Health. 1991; 12: 385–390.
Magura S, Shapiro JL, Kang SY. Condom use among criminally-involved adolescents. AIDS Care. 1994; 6: 595–603.
Oh MK, Cloud GA, Wallace LS, Reynolds J, Sturdevant M, Feinstein RA. Sexual behavior and sexually transmitted diseases among male adolescents in detention. Sexually Transmitted Diseases. 1994; 21: 127–32.
Bryan AD, Aiken LS, West SG. Young women’s condom use: The impact of perceived susceptibility, acceptance of sexuality and control over the sexual encounter. Health Psychology. 1997; 16: 468–479.
Aalsma MC, Tong Y, Wiehe SE, et al. The impact of delinquency on young adult sexual risk behaviors and sexually transmitted infections. Journal of Adolescent Health. 2010, 46: 17–24.
Robertson AA, Thomas CB, St. Lawrence JS, Pack R. Predictors of infection with Chlamydia or Gonorrhea in incarcerated adolescents. Sexually Transmitted Diseases. 2005; 32: 115–122.
Morrison-Beedy D, Carey MP, Aronowitz T, Mkandawire L, Dyne J. An HIV risk-reduction intervention in an adolescent correctional facility: Lessons learned. Applied Nursing Research. 2002; 15: 97–101.
Robertson AA, Stein JA, Baird-Thomas C. Gender differences in the prediction of condom use among incarcerated juvenile offenders: Testing the Information-Motivation-Behavior Skills (IMB) model. Journal of Adolescent Health. 2006; 38: 18–25.
Albarracin D, Fishbein M, Middlestadt S. Generalizing behavioral findings across times, samples, and measures: A study of condom use. Journal of Applied Social Psychology. 1998; 28: 657–674.
Bryan AD, Schmiege SJ, Broaddus MR. Mediational analysis in HIV/AIDS research: Estimating multivariate path analytic models in a structural equation modeling framework. AIDS & Behavior. 2007; 11: 365–383.
Bryan AD, Schindeldecker MS, Aiken LS. Sexual self-control and male condom-use outcome beliefs: Predicting heterosexual men’s condom use intentions and behavior. Journal of Applied Social Psychology. 2001; 33, 2565–2586.
Ajzen I. The theory of planned behavior. Organization Behavior & Human Decision Processes. 1991; 50: 179–211.
Albarracín D, Johnson BT, Fishbein M, Muellerleile PA. Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychological Bulletin. 2001; 127: 142–161.
Armitage CJ. Can the Theory of Planned Behavior Predict the Maintenance of Physical Activity? Health Psychology. 2005, 24: 235–245.
Norman P, Conner M. The theory of planned behavior and exercise: Evidence for the mediating and moderating roles of planning on intention-behavior relationships. Journal of Sport & Exercise Psychology. 2005, 27: 488–504.
Conner M, Norman P, Bell R The theory of planned behavior and healthy eating. Health Psychology. 2002, 21: 194–201.
Buffardi AL, Thomas KK, Holmes KK, et al. Moving upstream: Ecosocial and psychosocial correlates of sexually transmitted infections among young adults in the United States. American Journal of Public Health. 2008, 98: 1128–1136.
Barta WD, Tennen H: Lifestyle factors in HIV transmission: A functional contextualist perspective. Hauppauge, NY: Nova Biomedical Books; US, 2008.
Burke NJ, Joseph G, Pasick RJ, Barker JC. Theorizing social context: Rethinking behavioral theory. Health Education & Behavior. 2009, 36: 55S–70S.
Hutchinson M, Jemmott LS, Wood EB, et al. Culture-specific factors contributing to HIV risk among Jamaican adolescents. JANAC: Journal of the Association of Nurses in AIDS Care. 2007, 18: 35–47.
Gerrard M. Sex, sex guilt, and contraceptive use. Journal of Personality and Social Psychology. 1987; 42: 153–158
Breakwell GM, Millward LJ, Fife-Schaw C. Commitment to “safer” sex as a predictor of condom use among 16–20-year-olds. Journal of Applied Social Psychology. 1994, 24: 189–217.
Harlow LL, Quina K, Morokoff PJ, Rose JS, Grimley DM. HIV risk in women: A multifaceted model. Journal of Applied Biobehavioral Research. 1993; 1: 3–38.
De Bro SC, Campbell SM, Peplau LA. Influencing a partner to use a condom: A college student perspective. Psychology of Women Quarterly. 1994; 18: 165–182.
Wyatt GE, Riederle MH. Reconceptualizing issues that affect women’s sexual decision-making and sexual functioning. Psychology of Women Quarterly. 1994; 18: 611–25.
Amaro H. Love, sex, and power: Considering women’s realities in HIV prevention. American Psychologist. 1995, 50: 437–447.
Ickovics JR, Rodin J. Women and AIDS in the United States: Epidemiology, natural history, and mediating mechanisms. Health Psychology. 1992; 11: 1–16.
Sacco WP, Rickman RL, Thompson K, Levine B, Reed DL. Gender differences in AIDS-relevant condom attitudes and condom use. AIDS Education and Prevention. 1993; 5: 311–26.
Fisher WA. Predicting contraceptive behavior among university men: The roles of emotions and behavioral intentions. Journal of Applied Social Psychology. 1984; 14: 104–123.
Stewart DL, DeForge BR, Hartmann P, Kaminski M, Pecukonis E. Attitudes toward condom use and AIDS among patients from an urban family practice center. Journal of the National Medical Association. 1991; 83: 772–6.
Grady WR, Klepinger DH, Billy JO, Tanfer D. Condom characteristics: The perceptions and preferences of men in the United States. Family Planning Perspectives. 1993; 25: 67–73.
Keller ML. Why don’t young adults protect themselves against sexual transmission of HIV? Possible answers to a complex questions. AIDS Education and Prevention. 1993; 5: 220–223.
Ajzen I, Madden TJ. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology. 1986; 22: 453–474.
Hennessy M, Bleakley A, Fishbein M, et al.: Differentiating between precursor and control variables when analyzing Reasoned Action Theories. AIDS and Behavior. 2009, 14: 225–236.
Sheeran P, Abraham C. Mediator of moderators: Temporal stability of intention and the intention-behavior relation. Personality & Social Psychology Bulletin. 2003; 29: 205–15.
Conner M, Sandberg T, McMillan B, & Higgins A. Role of anticipated regret, intentions and intention stability in adolescent smoking initiation. British Journal of Health Psychology. 2006; 11: 85–101.
Godin G, Gagnon H, Lambert L, Conner M. Determinants of condom use among a random sample of single heterosexual adults. British Journal of Health Psychology. 2005; 16: 85–100.
Fortenberry J, Tu W, Harezlak J, Katz BP, Orr DP. Condom use as a function of time in new and established adolescent sexual relationships. American Journal of Public Health. 2002; 92: 211–213.
Von Haeften I, Fishbein M, Kaspryzk D, Montano D. Acting on one’s intentions: Variations in condom use intentions and behaviours as a function of type of partner, gender, ethnicity and risk. Psychology, Health & Medicine. 2000; 5: 163–171.
Ott MA, Katschke A, Tu W, Fortenberry JD. Longitudinal associations among relationship factors, partner change, and Sexually Transmitted Infection acquisition in adolescent women. Sexually Transmitted Diseases. 2010; 37: epub ahead of print.
Pulerwitz J, Amaro H, DeJong W, Gortmaker SL, Rudd R. Relationship power, condom use and HIV risk among women in the USA. AIDS Care. 2002; 14: 789–800.
Broaddus MR, Morris H, Bryan AD. ‘It’s not what you said, it’s how you said it:’ Perceptions of condom proposors by gender and strategy. Sex Roles: A Journal of Research. 2010; 62: 603–14.
Bryan AD, Aiken LS, West SG. Increasing condom use: Evaluation of a theory-based intervention to prevent sexually transmitted diseases in young women. Health Psychology. 1996; 15: 371–382.
Bryan AD, Rocheleau CA, Robbins RN, Hutchison KE. Condom use among high-risk adolescents: Testing the influence of alcohol use on the relationship of cognitive correlates of behavior. Health Psychology. 2005; 24: 133–142.
Schmiege SJ, Broaddus MR, Levin M, Bryan AD. Theoretically-based mechanisms of an alcohol-related sexual risk reduction intervention among incarcerated adolescents. Journal of Counseling and Consulting Psychology. 2009; 77: 38–50.
Conner M, Sheeran P, Norman P, Armitage CJ. Temporal stability as a moderator of relationships in the Theory of Planned Behavior. British Journal of Social Psychology. 2000; 39: 469–493.
Graham CA, Catania JA, Brand R, Duong T, Canchola JA. Recalling sexual behavior: A methodological analysis of memory recall bias via interview using the diary as the gold standard. Journal of Sex Research. 2003; 40: 325–332.
Kiene SM, Tennen H, & Armeli S. Today I’ll use a condom, but who knows about tomorrow: A daily process study of variability in predictors of condom use. Health Psychology. 2008; 27: 463–472.
Hill CA, Preston LK. Individual differences in the experience of sexual motivation: Theory and measurement of dispositional sexual motives. The Journal of Sex Research. 1996; 33: 27–45.
Knauper B, Kornik R, Atkinson K, Guberman C, Aydin C. Motivation influences in the underestimation of cumulative risk. Personality & Social Psychology Bulletin. 2005, 31: 1511–1523.
Conley TD, Rabinowitz JL. Scripts, close relationships, and symbolic meanings of contraceptives. Personal Relationships. 2004, 11: 539–558.
Bauman LJ, Berman R. Adolescent relationships and condom use: Trust, love, and commitment. AIDS & Behavior. 2005, 9: 211–222.
Acknowledgments
This study was funded by the National Institute on Drug Abuse, RO1 DA019139-01. Preparation of this manuscript was supported, in part, by center grant P30-MH52776 from the National Institute of Mental Health and by NRSA postdoctoral training grant T32-MH19985. The authors wish to sincerely thank the adolescents who participated in this research as well as the staff at the probation offices where we recruited.
Conflicts of Interest
None
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Broaddus, M.R., Schmiege, S.J. & Bryan, A.D. An Expanded Model of the Temporal Stability of Condom Use Intentions: Gender-Specific Predictors among High-Risk Adolescents. ann. behav. med. 42, 99–110 (2011). https://doi.org/10.1007/s12160-011-9266-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-011-9266-0