
Abstract
Neuromuscular impairment associated with cerebral palsy (CP) often leads to life-long walking deficits. Our goal was to evaluate the ability of a novel untethered wearable ankle exoskeleton to reduce the severity of gait pathology from CP. In this clinical feasibility study of five individuals with CP, we used instrumented gait analysis to quantify how powered plantar-flexor assistance affected gait mechanics following multi-visit acclimation. Compared to how each participant walked normally, walking with untethered exoskeleton assistance resulted in improved ankle plantar-flexion and knee extension; residual flexion deformity across the lower-extremity improved by a clinically significant 14.4° (p = 0.022). Powered plantar-flexor assistance increased average total positive ankle power by 44% (p = 0.037), and resulted in a 30% reduction in average negative biological ankle power (p = 0.004) and a 29% reduction in average positive hip power (p = 0.009). These findings suggest that powered ankle assistance augmented, rather than simply replaced, biological function to produce a more efficient gait pattern, which was corroborated by a 19% improvement in metabolic cost of transport (p = 0.011). This study provides evidence in support of the continued investigation of ankle assistance in mobility and rehabilitation interventions for this patient population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Trauma to the brain or central nervous system during perinatal development can lead to a group of neuromuscular disorders known as cerebral palsy (CP). CP is the predominant cause of physical disability in childhood4 and often results in pathological walking patterns, including crouch gait, jump gait, and equinus gait.1,11,37 Standard therapies for these pathological gait patterns, which include passive orthoses,27 physical therapy,12 surgery,14 and muscle injections,9 have proven to be only moderately effective in reducing severity. Relative muscle strength and endurance typically decreases when body mass increases as individuals with CP grow during adolescence.2,21 The vast majority of individuals with CP have progressively reduced walking ability across their lifespans.17,31
Neuromuscular impairment from CP can lead to abnormal and inefficient gait mechanics that drastically increase the energy cost of walking.33 While the ankle plantar-flexor muscles produce a large burst of propulsive (positive) joint power during the push-off phase of unimpaired gait, individuals with CP exhibit significantly reduced positive ankle joint power during walking with and without Ankle–Foot Orthoses (AFOs).32 Additionally, most individuals with CP walk with increased hip and knee flexion combined with reduced ankle plantar-flexion, range of motion, and plantar-flexor power.28 Increasing lower-extremity extension is a primary focus of clinical gait treatment because an overly flexed posture contributes to reduced walking efficiency and typically worsens with age until ambulatory ability is lost.3
The need for additional and complimentary management techniques for gait pathology from CP has led to the development of new technologically-based treatment strategies. Treadmill-based gait training in the form of robotic perturbations22 and immersive virtual reality19 have demonstrated some promising initial findings in changing short-term function. While treadmill-based approaches are likely constrained to research facilities and clinics, wearable approaches that can be used in community settings on a daily basis provide the anticipated added benefit of increased treatment dosage and access. Repeated exposure to assistance that results in improved posture may reinforce more favorable walking patterns while also facilitating increased physical activity. Recently, wearable assistance in the form of a powered knee exoskeleton demonstrated improvement in knee kinematics while children with CP walked using the device.24 However, knee assistance did not improve ankle mechanics or lower-extremity energy transfer.25 Reduced ankle function and a reliance on more proximal muscles for forward progression likely contributes to the pathological gait patterns observed in CP,35 which suggests that wearable ankle assistance may prove beneficial for both gait rehabilitation and mobility assistance. In particular, an ankle exoskeleton may find utility for use in conjunction with standard therapies, like muscle injections and orthopedic surgery, that address spasticity and contracture. Surprisingly, the potential for powered plantar-flexor assistance to improve gait mechanics remains unknown in this patient population.
The purpose of this study was to evaluate the ability of a novel wearable ankle exoskeleton to reduce the severity of gait pathology from CP. Our primary a priori hypotheses were that powered plantar-flexor assistance would (a) increase positive total ankle joint power, (b) improve posture (i.e. reduce flexion) across the entire lower-extremity, and (c) reduce gastrocnemius muscle activity during the stance phase of walking. To test these hypotheses, we implemented custom ankle exoskeletons in a multi-visit clinical feasibility study and conducted instrumented gait analysis to analyze how assistance affected joint angles, moments, and powers, and plantar-flexor muscle activity following device acclimation. The exoskeletons were battery-powered and wireless to maximize the relevance of our findings to the future implementation of assistive devices intended for use in real-world settings.
Materials and Methods
Ankle Exoskeleton
A lightweight and customizable ankle exoskeleton was designed and fabricated to provide untethered bilateral ankle assistance to individuals with gait deficits from CP (Fig. 1a). A detailed description of the design, including the files necessary for reproduction, are reported in Ref. 26. In summary, high-performance DC motors powered by an onboard battery actuated a pulley aligned with each ankle joint via a Bowden cable transmission (Fig. 1b). Torque sensors were mounted in-line with the exoskeleton’s ankle joint for feedback-based motor control. The Bowden cable transmission system was utilized to place the device’s heaviest components on the participant’s torso in order to minimize the metabolic burden of adding mass to the lower body.6 An electrical control system was mounted at the waist and included the battery and a custom printed circuit board with micro-controller, motor drivers, signal conditioners, and Bluetooth module. The untethered design was used for all experiments in this study. The battery provided greater than 30 min of operation at the highest level of assistance used across all participants.

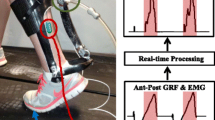
Ankle exoskeleton and experimental setup. (a) Picture of one of the participants walking with their custom untethered ankle exoskeleton, which operated completely untethered (battery powered and wireless). (b) Schematic representation of the exoskeleton transmission system for providing ankle assistance. The exoskeleton transmitted torque data via Bluetooth to a computer synchronized with the motion capture system (c) Schematic depiction of the experimental set up, which included assessment of kinematics, kinetics, muscle activity, and indirect calorimetry. (d) Schematic of ankle assistance timing across the gait cycle and tunable control parameters (rise time and magnitude). (e) Exoskeleton walking duration required by participant to acclimate to assistance across at least four visits. Participant P5 required nearly twice the amount of exoskeleton training time before acclimating to assistance. (f) The average reduction in metabolic cost across the cohort during walking with personalized ankle plantar-flexor assistance, as reported in Ref. 25.
To provide robust control of ankle plantar-flexor assistance, embedded foot sensors placed under the ball of the foot informed a simple finite state machine that distinguished plantar-flexor assist-on, assist off, and an optional dorsi-flexor assist-on states (Fig. 1d). During the plantar-flexor assist-on state, we implemented a torque profile that mimicked the timing and shape of the biological ankle moment. During the assist off state, the motors were controlled so that zero external torque was applied to the ankle by counteracting friction and motor inertia.
Participants
Five ambulatory individuals with CP (5–35 years old) completed this multi-visit study to evaluate the feasibility of untethered powered ankle assistance to improve gait mechanics (Table 1). To assess the efficacy of powered ankle assistance across a range of potential users with the purpose of aiding the design of future large-scale intervention studies, we included younger individuals, as young as 5 years old, with milder gait pathologies, as well as older individuals, with more severe gait pathologies. We sought to determine device applicability across the wide age range because early childhood intervention of gait disorders in CP is critical for preventing ambulatory decline,10 while fewer options exist for the continued management of gait impairment in older individuals.
The cohort included individuals with levels of neuro-motor impairment that spanned the ambulatory range (levels I-III) of the Gross Motor Function Classification System (GMFCS, 5-level clinical classification system of movement ability),3 and levels of spasticity, assessed via the Modified Ashworth Scale (MAS, 6-level classification of resistance to passive soft-tissue stretching),29 that spanned a range from no tone (score of 0) to considerable tone (score of 3). All participants had passive ankle plantar-flexion range of motion within normal levels. Clinical descriptions of each participant’s pathological gait pattern are presented in Table 2.
This study was approved by the Northern Arizona University Institutional Review Board under protocol #986744. Criteria for inclusion in this study included diagnosis of CP, age between 5 and 75 years old, the ability to walk on a treadmill with or without using a handrail, at least 10° of passive ankle plantar-flexion, and the ability to understand and follow simple directions. Participants were excluded from the study if they had orthopaedic surgery within the prior six months or a condition other than CP that could have impacted their safety. The first five individuals that met the inclusion/exclusion criteria were invited to participate. We obtained written consent from each adult participant. For children, we obtained their verbal assent as well as written consent from one of their parents.
Study Protocol
Each participant’s first visit consisted of the consent process, a physical evaluation conducted by a licensed physical therapist that included neuro-motor, spasticity and range-of-motion assessment, and lower-extremity measurement for device customization. Next, participants completed several training sessions during which the research team individually tuned the timing, shape, and magnitude of assistive torque for each participant with the goal of maximizing walking efficiency (Fig. 1d). Participants completed a minimum of 90 min of exoskeleton walking across a minimum of four training visits. Training and tuning persisted until the research team anticipated that each participant was acclimated to assistance and that a suitable level of assistance was established (Fig. 1e). Tuning consisted of adjusting the magnitude, on–off timing, and rise-time of assistance.
On a final data collection visit, we conducted gait analysis (Fig. 1c) while participants walked on an instrumented treadmill at their preferred speed. We compared how participants walked normally in a baseline condition that included walking in their normal shoes (shod) and with AFOs if they were prescribed by the participant’s physician (Table 1), to how participants walked with customized untethered exoskeleton assistance (exoskeleton-assisted). We also evaluated how participants walked while wearing the exoskeleton in an unassisted condition meant to isolate the effects of the exoskeleton’s mass (detailed description and data are presented in Supplementary Material). We used respiratory data collected from a portable metabolic testing system (K5, Cosmed) and Brockway’s standard equation5 to compute the metabolic cost of transport across walking conditions. We previously reported a reduction in metabolic cost of transport during walking with assistance in this cohort (Fig. 1f).26 For the present study, we focused our investigation on the exoskeleton-assisted walking trial that resulted in the greatest improvement in walking economy for each participant.
Walking trials during data collection lasted for 5 min, and were separated by a 5-min, or longer, seated rest break. Set condition sequences were randomized across participants (Supplementary Table 1). A safety tether was attached to a gait belt secured around each participant’s torso. One participant rated GMFCS III and compromised balance held an instrumented handle connected to an over-head support cable to ensure they could complete each 5-min walking trial without interruption. Since the cable only resisted tension, a single in-line loadcell allowed us to quantify similarity of weight-bearing across conditions; the handle supported 6.9 ± 1.6% of their body-weight during the baseline trial and 6.2 ± 1.6% during the exoskeleton-assisted trial (Supplementary Fig. 1).
Evaluation of Gait Mechanics and Muscle Activity
We recorded biomechanics data during the final minute of each trial. We used a wireless electromyography (EMG) measurement system (Trigno, Delsys) to record muscle activity at 1926 Hz from each lateral gastrocnemius. The gastrocnemius was selected instead of the soleus to allow placement of the wireless EMG electrode above the exoskeleton attachment and/or a participant’s AFO, which blocked the soleus. The 5 year-old participant’s limbs were unable to accommodate an electrode because of their AFOs and very small limb size. A ten-camera motion capture system (Vicon) with a custom marker set25 was used to record motion at 120 Hz: four markers were placed on each foot; clusters, each with four markers, were placed on each shank and thigh; individual markers were placed on the medial and lateral aspects of the ankle and knee joints; four markers were placed on the pelvis and three on the torso. Marker clusters, which likely increase the repeatability of kinematic measurements vs standard single-marker-only models (e.g. Vicon’s plug-in gait),18 were used to minimize application time and maximize 3D segment tracking accuracy. Ground reaction force data were recorded at 980 Hz from the instrumented treadmill. Exoskeleton data, synchronized with the motion capture system using a trigger signal, were recorded at 100 Hz. EMG, motion capture marker, ground reaction force, and exoskeleton data sampling frequencies were selected to meet standard recommendations for accurately capturing muscle activity, kinematics and kinetics of human locomotion.36
Data Analysis
We used musculoskeletal modeling software (OpenSim15) to compute lower-extremity joint angles and moments by scaling a musculoskeletal model to the anthropometrics of each participant, and then conducting inverse kinematics and inverse dynamics. Inertial properties of each custom exoskeleton component were added to the appropriate segment of each scaled model. Mechanical joint power was calculated as the product of joint angular velocity and joint moment; power was defined as positive when torque and angular velocity acted in the same direction.36 Exoskeleton mechanical joint power was calculated as the product of ankle angular velocity and applied torque. We calculated positive and negative mean joint power during stance by integrating the positive or negative portions of the joint power time series data and dividing by the duration; net mean power was calculated by integrating across both positive and negative portions.8 Positive power represents mechanical energy generation, while negative power represents energy absorption. During the exoskeleton-assisted trials, the biological contribution to the total (biological + exoskeleton) joint moment and power was found by subtracting the contribution from the exoskeleton from the total joint moment and power computed from inverse dynamics.
EMG data were band-pass-filtered between 15 and 380 Hz, rectified, and low-pass-filtered at 7 Hz to create a linear envelope.25 To mitigate the potential influence of background noise present within the EMG frequency range, and to isolate changes in muscle activity during walking relative to inactivity, the minimum muscle activity during seated rest was subtracted from the processed EMG data. These data were subsequently normalized to the peak value of the mean baseline activity pattern. Experimental biomechanics and exoskeleton data were synchronized and processed using MATLAB (2017b, MathWorks). Biomechanics data were normalized to percent gait cycle and averaged. A minimum of five representative gait cycles per limb were averaged together per participant.
We focused our clinical evaluation on lower-extremity kinematics, kinetics, and neuromuscular control, due to the importance of these measures in evaluating CP gait rehabilitation.13,14,37 Our primary outcome measures included peak mid-stance lower-extremity extension, total positive ankle joint power, and gastrocnemius muscle activity. Peak mid-stance lower-extremity extension, computed as the sum of peak hip extension, peak knee extension, and peak ankle plantar-flexion, was selected as a primary outcome measure due to the clinical importance of interventions aimed at improving dynamic posture in this patient population. To inform future larger-scale clinical intervention studies, we also analyzed several secondary outcome measures, including all remaining lower-extremity peak joint angles; mean joint moments; and mean positive, negative, and net joint powers.
Statistical Analysis
We used paired two-tailed t tests to determine how our biomechanical measures were affected by walking with exoskeleton assistance compared to baseline. We checked that the data in each comparison were normally distributed using the Kolmogorov–Smirnov test with small-sample Lillifors correction.20 Wilcoxon signed-rank tests were used to evaluate statistical significance for distributions that failed normality. The statistical tests used for each comparison are noted in the text. We used the Holm–Bonferroni approach to sequentially adjust the statistical significance level from α < 0.05 to α < 0.0167 when evaluating our a priori hypotheses; the Holm–Bonferroni-adjusted p values, denoted with an “*”, are reported throughout. We evaluated our secondary outcome measures with a fixed significance level of α < 0.05. The effects of exoskeleton assistance on joint mechanics and muscle activity were evaluated across all limbs to account for inter-limb asymmetry exhibited by the participants. Mean ± standard error (SE) are presented in the text and figures for group level comparisons.
Results
Exoskeleton Performance
The ankle exoskeleton provided 0.24 ± 0.02 Nm kg−1 of peak torque and 0.47 ± 0.27 W kg−1 of peak positive joint power to the participants during walking with assistance. The exoskeleton generated 0.080 ± 0.013 W kg−1 of average (positive) joint power and absorbed 0.029 ± 0.004 W kg−1 of average (negative) joint power during the stance phase (Fig. 2). Peak assistance from the exoskeleton amounted to 21% of the peak biological ankle moment and 33% of the peak biological positive ankle power during baseline walking.

Exoskeleton torque and power during walking. Experimentally-measured exoskeleton torque (a) and mechanical joint power (b) applied to each participant’s right limb across the gait cycle (blue). The specified (desired) torque is indicted by the orange lines. Shading depicts ± 1.0 standard deviation. Differences between the desired and measured torque occurred during intervals in the gait cycle when the high ankle angular velocity exceeded the speed rating of the motor and gearbox; the effect of this undesired response was assessed to be minimal. The large standard deviation for the torque and power output for P3 was a result of this participant’s variable gait pattern, which elicited variable onset of assistance. The bar plot on the right presents the mean stance phase exoskeleton torque and power across all limbs. Error bars depict standard error. Brackets indicates significance.
Effects of Assistance on Gait Kinematics
Exoskeleton assistance improved lower-extremity posture during walking. We found that walking under the exoskeleton-assisted condition increased peak stance-phase lower-extremity extension by 14.4° ± 4° (paired t test, adjusted p = 0.022, Fig. 3a) compared to baseline. Peak ankle plantar-flexion increased by 5 ± 12° (paired t test, p = 0.032, Fig. 4a) and peak knee extension in mid-stance increased by 5° ± 8° (paired t test, p = 0.037, Fig. 5a) during exoskeleton-assisted walking compared to baseline; peak hip extension was not significantly different (paired t test, p = 0.187, Fig. 6a).

Effects of assistance on primary outcome measures. Group average peak lower-extremity extension (a), mean total positive ankle power (b), and mean gastrocnemius muscle activity (c) during baseline walking (gray) and exoskeleton-assisted walking (blue). Total ankle power during baseline walking is composed entirely of the biological contribution, while total ankle power during exo-assisted walking is the sum of the exoskeleton and biological contributions. Error bars depict ± 1.0 standard error. p values reflect Holm–Bonferroni multiple-comparisons adjustment; all differences were statistically significant. The “typical range” extension and power data are from unimpaired healthy-weight children.23

Effects of assistance on ankle mechanics. Ankle angles (a), moments (b), and powers (c), for each participant’s right limb across the gait cycle during baseline walking (gray) and exoskeleton-assisted walking (red); the total (biological + exoskeleton) moment and power during exoskeleton-assisted walking is depicted in blue. Shading depicts ± 1.0 standard deviation. The bar plots on the right present peak plantar-flexion angle (top), mean stance-phase ankle moment (middle), and average stance-phase positive, negative, and net ankle power (bottom) across all limbs for each walking condition. Error bars depict standard error. Brackets indicates significance. * indicates Holm–Bonferroni adjusted p value. The “typical” ankle angle is the average pattern from unimpaired healthy-weight children.22

Effects of assistance on knee mechanics. Knee angles (a), moments (b), and powers (c), for each participant’s right limb across the gait cycle during baseline walking (gray) and exoskeleton-assisted walking (red). Shading depicts ± 1.0 standard deviation. The bar plots on the right present peak mid-stance knee extension (top), mean stance-phase knee moment (middle), and average stance-phase positive, negative, and net knee power (bottom) across all limbs for each walking condition. Error bars depict standard error. Brackets indicates significance. The “typical” knee angle is the average pattern from unimpaired healthy-weight children.22

Effects of assistance on hip mechanics. Hip angles (a), moments (b), and powers (c), for each participant’s right limb across the gait cycle during baseline walking (gray) and exoskeleton-assisted walking (red). Shading depicts ± 1.0 standard deviation. The bar plots on the right present peak mid-stance hip extension (top), mean stance-phase hip moment (middle), and average stance-phase positive, negative, and net hip power (bottom) across all limbs for each walking condition. Error bars depict standard error. Brackets indicates significance. The “typical” hip angle is the average pattern from unimpaired healthy-weight children.22
Effects of Assistance on Gait Kinetics
Walking with ankle plantar-flexor assistance affected ankle mechanics. The total ankle moment (biological + exoskeleton) during assisted walking was not significantly different from the biological moment during baseline walking (paired t test, p = 0.077, Fig. 4b). The mean biological ankle moment during exoskeleton-assisted walking decreased by 27.5 ± 8.7% (paired t test, p = 0.001) compared to the biological moment during baseline walking (Fig. 4c). Compared to baseline walking, average positive total ankle power increased by 43.6 ± 7.4% (paired t test, adjusted p = 0.037, Fig. 3b) and decreased average negative total ankle power by 17.5 ± 3.9% (paired t test, p = 0.024) during assisted walking; the average net total ankle power increased by 0.12 ± 0.08 W kg−1 (paired t test, p < 0.001). While average positive biological ankle power was not significantly different across conditions, participants reduced their average negative biological ankle power by 30.3 ± 5.3% (paired t test, p = 0.004) during assisted walking compared to baseline; average net biological ankle power increased by 0.07 ± 0.6 W kg−1 (paired t test, p = 0.003).
Knee joint moments and powers were not significantly different between walking conditions (Figs. 5b and 5c). Compared to baseline, stance-phase average hip flexor moments increased by 0.10 ± 0.04 Nm kg−1 (paired t test, p = 0.018) during exoskeleton-assisted walking (Fig. 6b). Average positive and net hip power decreased by 29.2 ± 6.0% (paired t test, p = 0.009) and 63.2 ± 15.0% (paired t test, p = 0.009), respectively, during assisted vs. baseline walking (Fig. 6c).
Effects of Assistance on Muscle Activity
Ankle assistance altered stance-phase muscle activity. Mean stance-phase gastrocnemius activity decreased by an average of 26 ± 6% (paired t test, adjusted p = 0.004) during walking with exoskeleton assistance (Figs. 3c and 7).

Effects of assistance on muscle activity. Gastrocnemius electromyography for each participant’s right limb across the gait cycle during baseline walking (gray) and exoskeleton-assisted walking (red). Shading depicts ± 1.0 standard deviation. The bar plot on the right presents mean stance-phase gastrocnemius activity across all limbs for each walking condition. Error bar depict standard error. Electromyography data were not available for participant P3 because placement of the wireless electrode was prevented by prescribed AFOs that extended to just below the knee. Brackets indicates significance. * indicates Holm–Bonferroni adjusted p value.
Isolating the Effects of the Exoskeleton’s Mass on Outcome Measures
During the unassisted exoskeleton condition, the motor controller was effective in producing minimal torque output across the gait cycle; the average amount of residual exoskeleton torque applied to the ankle joint was less than 1.65% of the biological ankle moment (Supplementary Fig. 2). During walking while wearing the exoskeleton as it operated under zero-torque mode, participants exhibited a 22% increase in negative ankle power (paired t test, p = 0.048), a 125% decrease in net ankle power (paired t test, p = 0.005), a 109% (paired t test, p = 0.005) increase in mean knee extensor moment, and a 29% increase in average positive knee power (paired t test, p = 0.035) compared to baseline walking (Supplementary Table 2). No statistically significant differences were observed in peak stance-phase extension across individual joints during walking in this unassisted condition.
Discussion
The primary goal of this study was to evaluate the capacity for powered ankle plantar-flexor assistance to reduce the severity of clinical gait pathology in CP. The findings support our hypotheses that powered ankle assistance would increase propulsive ankle joint power, improve lower-extremity posture, and reduce plantar-flexor muscle activity during walking in children and young adults with neurological gait deficits. Powered assistance was well-tolerated, and improvements were observed following a relatively short number of acclimation visits. We used exoskeletons that were battery-powered and wireless to maximize the relevance of our findings to the future implementation of assistive devices intended for use in real-world settings. While individual responses to exoskeleton assistance were variable, as expected in this heterogeneous patient population, several statistically significant trends were observed across the cohort.
Our study participants exhibited approximately 20° of excessive peak joint flexion across the hip, knee, and ankle joints during the stance phase. Walking with untethered exoskeleton assistance improved peak lower-extremity extension by around 14°, resulting in a mid-stance posture much closer to that of unimpaired gait. While still acknowledging other potential contributing factors to flexed posture from CP, including altered muscle stiffness, our findings reaffirm prior conclusions that reduced ankle power may be a primary contributor to the flexed gait pattern exhibited by individuals with CP,30 and that assistance to a particular lower-extremity joint has the potential to improve posture up the kinematic chain.25 CP can affect gait mechanics in all three planes of motion. Future analyses should expand upon this initial sagittal plane investigation, particularly because improved sagittal plane kinematics resulting from powered ankle assistance may alleviate abnormal frontal and transverse plane compensations.
Across all participants, powered ankle assistance resulted in the greatest kinematic improvement for the individual with the most flexed baseline walking pattern of the cohort (P2, moderate crouch gait). This finding suggests that powered ankle assistance may be beneficial, even increasingly so, for greater levels of impairment.
Moreover, mild-to-moderate ankle muscle spasticity, which was present in this cohort, did not appear to inhibit the ability of the ankle exoskeleton to elicit improved gait mechanics. However, a much larger sample size is needed to establish the relationships between spasticity and clinical outcomes during exoskeleton assisted walling. Future studies should investigate the potential for powered ankle assistance to treat more diverse presentations of CP, including more severe gait pathology and spasticity levels.
Powered ankle assistance appears to augment underlying biological function and results in a measurably more efficient walking pattern in this patient population. Not only did external assistance increase total average positive and net ankle joint power, but it also reduced average negative biological ankle power, meaning less energy was dissipated. Further, ankle assistance resulted in reduced positive hip joint power requirements. This suggests that ankle assistance reduced the inefficient requirement of muscles crossing the hip joint for forward progression of the body’s center of mass.35 Together, these finding suggests that ankle assistance resulted in a more efficient transfer of energy across the lower-extremity.
Powered ankle assistance may be more beneficial than powered knee assistance in children with gait deficits from CP. In a prior study of children and adolescents with CP that focused on treating crouch gait, we found that powered stance-phase knee extension assistance increased both average positive and negative hip power while also increasing average negative ankle power.25 Those prior findings indicate that knee assistance may actually produce a less biomechanically efficient gait pattern by increasing total (positive and negative) energy transfer. Indeed, in that same study, activity of the plantar-flexor, hip flexor, and hip extensor muscles increased during walking with knee assistance. In contrast, our present analysis showed that powered ankle assistance produced a more biomechanically efficient gait pattern across the lower-extremity, corroborated by assessment of energy expenditure via indirect calorimetry.
We observed a reduction in gastrocnemius activity as participants walked using the exoskeleton, which is another likely contributor to the improvement in energy cost as our participants walked with assistance. This reduction in muscle activity demonstrates neuromuscular modulation in a patient population that is similar to unimpaired individuals walking with powered ankle assistance.34 The changes in gastrocnemius muscle activity may not represent improved neuromuscular function. In theory, there may be some concern for assistive devices that result in reduced muscle activity because, all things equal, reduced muscle activity may lead to muscle atrophy over time. This is an important concern that highlights a potential undesirable consequence of powered assistance. Powered devices such as the one used in this study may be particularly useful because they can provide both assistance and resistance. As a result, they could be used to combine mobility assistance with specific intervals of resistive gait training intended to improve muscle strength or motor control, which is a promising area of research.7,16,22 A holistic approach utilizing wearable assistance and rehabilitation-focused interventions19,22 may be most beneficial.
Eliciting benefits from powered assistance requires overcoming the burden of adding the exoskeleton’s mass to the body. Wearing the exoskeleton while it operated under zero-torque mode proved detrimental to gait mechanics, particularly at the ankle, which undoubtedly contributed to the 19.7% increase in the metabolic cost of transport compared to baseline. Therefore, the improvements in gait mechanics during walking with the active exoskeleton were a result of powered assistance rather than simply wearing the device. Moreover, powered assistance had to overcome the detrimental effects of the device’s passive properties. While a primary design goal of our exoskeleton was to minimize adding mass to the body, further reductions in mass and the influence other passive effects (e.g. cable stiffness) would likely elicit even greater improvements in outcomes.
The small number of participants that complete the protocol is an aspect of this feasibility study that warrants consideration. The sample size, which was similar to other prominent multi-visit repeated-measures studies (e.g. n = 622), was selected due to the time consuming nature of fabricating the custom exoskeletons and having participants complete the training visits. We note that the cohort in this study was purposefully diverse (ages ranging from 5 to 30, mild to moderate gait severity) and sufficient in establishing statistically significant differences in our primary outcome measures with multiple comparisons correction. Our findings of significant differences reported for our secondary outcomes should be interpreted with caution given the fixed significance level. Future studies should expand on this work by investigating the effects of powered ankle assistance across a wider range of individuals, particularly those with more severe gait deficits. The potential for participant fatigue to influence gait mechanics acts as a confounding factor for repeated measures studies such as this one. We sought to minimize these potential effects by randomizing condition order across participants. Another limitation of this study was that muscle activity assessment was isolated to the gastrocnemius. Moreover, muscle strength was not measured, which may have aided our conclusions regarding appropriate device settings and implementation. Future studies should expand the number of muscles analyzed and incorporate EMG and strength measurement of the ankle, knee and hip extensors because we observed changes in joint mechanics across the entire lower-extremity.
In summary, this clinical feasibility study provides evidence that light-weight untethered ankle exoskeleton assistance can result in improved gait kinematics and kinetics in children and young adults with CP. Improvements were observed across a wide range of participant characteristics. We found that the biomechanical changes underlying the 19% improvement in metabolic cost of transport included improvement in posture, more efficient energy transfer across the lower-extremity, and a reduction in muscle activity. Our findings suggest that exoskeleton assistance enhanced, rather than simply replaced, biological function. This study adds to rationale for the continued investigation of powered plantar-flexor assistance to reinforce more-favorable walking patterns in future intervention studies in children and young adults with neurological disorders. Additional research is needed to fully determine the potential clinical benefit of powered ankle assistance for individuals with CP.
References
Armand, S., G. Decoulon, and A. Bonnefoy-Mazure. Gait analysis in children with cerebral palsy. EFORT open Rev. 1:448–460, 2016.
Bell, K. J., S. Ounpuu, P. A. DeLuca, and M. J. Romness. Natural progression of gait in children with cerebral palsy. J. Pediatr. Orthop. 22:677–682, 2002.
Bjornson, K. F., B. Belza, D. Kartin, R. Logsdon, and J. F. McLaughlin. Ambulatory physical activity performance in youth with cerebral palsy and youth who are developing typically. Phys. Ther. 87:248–257, 2007.
Boyle, C. A., S. Boulet, L. A. Schieve, R. A. Cohen, S. J. Blumberg, M. Yeargin-Allsopp, S. Visser, and M. D. Kogan. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics 127:1034–1042, 2011.
Brockway, J. M. Derivation of forulae used to calculate energy expenditure in man. Hum. Nutr. Clin. Nutr. 41C:463–471, 1987.
Browning, R. C., J. R. Modica, R. Kram, and A. Goswami. The effects of adding mass to the legs on the energetics and biomechanics of walking. Med. Sci. Sports Exerc. 39:515–525, 2007.
Burdea, G. C., D. Cioi, A. Kale, W. E. Janes, S. A. Ross, and J. R. Engsberg. Robotics and gaming to improve ankle strength, motor control, and function in children with cerebral palsy: a case study series. IEEE Trans. Neural Syst. Rehabil. Eng. 21:165–173, 2013.
Collins, S. H., M. B. Wiggin, and G. S. Sawicki. Reducing the energy cost of human walking using an unpowered exoskeleton. Nature 522:212–215, 2015.
Corry, I. S., A. P. Cosgrove, C. M. Duffy, T. C. Taylor, and H. K. Graham. Botulinum toxin A in hamstring spasticity. Gait Posture 10:206–210, 1999.
Damiano, D. L. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys. Ther. 86:1534–1540, 2006.
Damiano, D. L., K. E. Alter, and H. Chambers. New clinical and research trends in lower extremity management for ambulatory children with cerebral palsy. Phys. Med. Rehabil. Clin. N Am. 20:469–491, 2009.
Damiano, D. L., A. S. Arnold, K. M. Steele, and S. L. Delp. Can strength training predictably improve gait kinematics? A pilot study on the effects of hip and knee extensor strengthening on lower-extremity alignment in cerebral palsy. Phys. Ther. 90:269–279, 2010.
Damiano, D. L., L. A. Prosser, L. A. Curatalo, and K. E. Alter. Muscle plasticity and ankle control after repetitive use of a functional electrical stimulation device for foot drop in cerebral palsy. Neurorehabil. Neural Repair 27:200–207, 2013.
De Mattos, C., K. Patrick Do, R. Pierce, J. Feng, M. Aiona, and M. Sussman. Comparison of hamstring transfer with hamstring lengthening in ambulatory children with cerebral palsy: further follow-up. J. Child. Orthop. 8:513–520, 2014.
Delp, S. L., F. C. Anderson, A. S. Arnold, P. Loan, A. Habib, C. T. John, E. Guendelman, and D. G. Thelen. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 54:1940–1950, 2007.
Dodd, K. J., N. F. Taylor, and D. L. Damiano. A systematic review of the effectiveness of strength-training programs for people with cerebral palsy. Arch. Phys. Med. Rehabil. 83:1157–1164, 2002.
Dreher, T., D. Vegvari, S. I. Wolf, A. Geisbüsch, S. Gantz, W. Wenz, and F. Braatz. Development of knee function after hamstring lengthening as a part of multilevel surgery in children with spastic diplegia: A long-term outcome study. J. Bone Jt. Surg. Ser. A 94:121–130, 2012.
Duffell, L. D., N. Hope, and A. H. McGregor. Comparison of kinematic and kinetic parameters calculated using a cluster-based model and Vicon’s plug-in gait. Proc. Inst. Mech. Eng. Part H J Eng. Med. 228:206–210, 2014.
Gagliardi, C., A. C. Turconi, E. Biffi, C. Maghini, A. Marelli, A. Cesareo, E. Diella, and D. Panzeri. Immersive virtual reality to improve walking abilities in cerebral palsy: a pilot study. Ann. Biomed. Eng. 2018. https://doi.org/10.1007/s10439-018-2039-1.
Ghasemi, A., and S. Zahediasl. Normality tests for statistical analysis: a guide for non-statisticians. Int. J. Endocrinol. Metab. 10:486–489, 2012.
Johnson, D. C., D. L. Damiano, and M. F. Abel. The evolution of gait in childhood and adolescent cerebral palsy. J. Pediatr. Orthop. 17:392–396, 1997.
Kang, J., D. Martelli, V. Vashista, I. Martinez-Hernandez, H. Kim, and S. K. Agrawal. Robot-driven downward pelvic pull to improve crouch gait in children with cerebral palsy. Sci. Robot. 2:eaan2634, 2017.
Lerner, Z. F., W. J. Board, and R. C. Browning. Pediatric obesity and walking duration increase medial tibiofemoral compartment contact forces. J. Orthop. Res. 34:97–105, 2016.
Lerner, Z. F., D. L. Damiano, and T. C. Bulea. A lower-extremity exoskeleton improves knee extension in children with crouch gait from cerebral palsy. Sci. Transl. Med. 9:1–11, 2017.
Lerner, Z. F., D. L. Damiano, and T. C. Bulea. The effects of exoskeleton assisted knee extension on lower-extremity gait kinematics, kinetics, and muscle activity in children with cerebral palsy. Sci. Rep. 7:13512, 2017.
Lerner, Z. F., G. M. Gasparri, M. O. Bair, J. L. Lawson, J. Luque, T. A. Harvey, and A. T. Lerner. An untethered ankle exoskeleton improves walking economy in a pilot study of individuals with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2018. https://doi.org/10.1109/tnsre.2018.2870756.
Maltais, D., O. Bar-Or, V. Galea, and M. Pierrynowski. Use of orthoses lowers the O(2) cost of walking in children with spastic cerebral palsy. Med. Sci. Sports Exerc. 33:320–325, 2001.
McNee, A. E., A. P. Shortland, L. C. Eve, R. O. Robinson, and M. Gough. Lower limb extensor moments in children with spastic diplegic cerebral palsy. Gait Posture 20:171–176, 2004.
Mutlu, A., A. Livanelioglu, and M. K. Gunel. Reliability of Ashworth and Modified Ashworth Scales in children with spastic cerebral palsy. BMC Musculoskelet. Disord. 9:44, 2008.
Olney, S. J., H. E. MacPhail, D. M. Hedden, and W. F. Boyce. Work and power in hemiplegic cerebral palsy gait. Phys. Ther. 70:431–438, 1990.
Rethlefsen, S. A., S. Yasmeh, T. A. Wren, and R. M. Kay. Repeat hamstring lengthening for crouch gait in children with cerebral palsy. J. Pediatr. Orthop. 33:501–504, 2013.
Romkes, J., and R. Brunner. Comparison of a dynamic and a hinged ankle-foot orthosis by gait analysis in patients with hemiplegic cerebral palsy. Gait Posture 15:18–24, 2002.
Rose, J., J. G. Gamble, A. Burgos, J. Medeiros, and W. L. Haskell. Energy expenditure index of walking for normal children and for children with cerebral palsy. Dev. Med. Child Neurol. 32:333–340, 1990.
Sawicki, G. S., and D. P. Ferris. Mechanics and energetics of level walking with powered ankle exoskeletons. J. Exp. Biol. 211:1402–1413, 2008.
Steele, K. M., A. Seth, J. L. Hicks, M. S. Schwartz, and S. L. Delp. Muscle contributions to support and progression during single-limb stance in crouch gait. J. Biomech. 43:2099–2105, 2010.
Winter, D. A. Biomechanics and Motor Control of Human Movement. New York: Wiley, 1990.
Wren, T. A., S. Rethlefsen, and R. M. Kay. Prevalence of specific gait abnormalities in children with cerebral palsy: influence of cerebral palsy subtype, age, and previous surgery. J. Pediatr. Orthop. 25:79–83, 2005.
Acknowledgments
We thank Gian Maria Gasparri, Jason Luque, and Andrea Lerner for their critical assistance with this study. This study was supported in part by NIH Grant No. 1R03HD094583-01 and Arizona Department of Health Serves Grant No. ADHS18-198864.
Conflict of Interest
Z.F.L. is a named inventor on Provisional U.S. Patent Application No. 62/644,163, “Ankle Exoskeleton System and Method for Assisted Mobility and Rehabilitation” covering the exoskeleton used in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Joel Stitzel oversaw the review of this article.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lerner, Z.F., Harvey, T.A. & Lawson, J.L. A Battery-Powered Ankle Exoskeleton Improves Gait Mechanics in a Feasibility Study of Individuals with Cerebral Palsy. Ann Biomed Eng 47, 1345–1356 (2019). https://doi.org/10.1007/s10439-019-02237-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-019-02237-w