
Abstract
The inverted pendulum model predicts that the major challenge for neural control of the upright posture is the inherent instability of the body due to the center of mass (COM) being above the base of support (BOS). If so, even slight elevation of the COM may substantially destabilize posture. The destabilizing effect of heavy load positioned above the COM has been demonstrated. We examined sensitivity of posture to light (1–5% of body weight) load by placing weights on the shoulders and assessing functional reach distance in the forward, right, and left directions and postural sway during quiet stance. At each load level, the quiet stance task was tested with and without vision. The 1% of body weight load significantly shortened reach distance in the forward direction. It also increased postural sway. Interestingly, additional weight did not result in further deficits. The results support high sensitivity of postural stability to COM elevation that increases the challenge for neural control of posture and that can potentially be used for early detection of declines in postural stability.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Maintaining upright posture during standing and locomotion is one of the most challenging tasks of human daily activities. Postural stability is the ability to control the center of mass in relationship to the base of support.21 Understanding how our nervous system addresses the challenges of postural stability is necessary to develop effective interventions for people with diminished postural stability.
The challenges of maintaining upright posture are represented by the inverted pendulum model that emphasizes that the body’s center of mass (COM) is above the base of support.2,26,27 Consequently, the upright posture is inherently unstable. The instability is caused by the gravitational moment applied to the COM that pulls the body downward. To maintain the upright posture, the body needs to constantly compensate for this moment. A wide range of motor control mechanisms are used to provide this compensation and stabilize the body against gravity, including reflexes and voluntary central control both in the feedforward and feedback control modes with the use of visual, proprioceptive, and vestibular information.6,11,12
The gravitational moment is proportional to the COM height, body mass, and the sine of the angle of the body deviation from the vertical. This predicts that elevation of the COM would increase the instability of the upright posture by increasing both the COM height and body mass. Indeed, a destabilizing effect of a heavy load, constituting about 10% of body weight or higher, positioned above the COM, such as a backpack, has been repeatedly demonstrated.1,3,5,9,10,15,16,18,20,28 In these studies, postural sway increased with increases in load and in the height of its placement,18,20,28 and more in older than younger adults.15 In contrast, load placed at the waist level or lower did not affect postural sway.18,28
For example, the effect of 12, 21, and 30 kg load on postural sway was assessed when load was carried in a backpack and weighted vest.18 The load was located at the upper back when carried in the backpack and it was evenly distributed at the waist level when carried in the vest. Postural sway linearly increased with load in the backpack condition. However, no significant changes in postural sway were found in the weighted vest condition. While a backpack results in an asymmetrical, posterior position of load, another study used load evenly distributed around the body.16 The load was of 10 and 20% of the body weight (BW), and it was positioned either at the height of the body COM or 15% of the body height above the body COM. Application of larger load and load positioned more superior to the body COM lead to increased postural sway. These results suggest that destabilization of posture is caused not only by increases in load but also by placement of the load above the natural body COM, which elevates the total COM.
The inherent instability of the upright posture demonstrated by the inverted pendulum model predicts high sensitivity of postural stability to COM elevation. The goal of the present study was to test this sensitivity. We elevated the COM by placing two equal weights on the top of the shoulders. Four conditions of total load constituted of the two weights were used: 0% (no load), 1, 3, and 5% of BW. We assessed the effect of the load by evaluating the functional reach distance and postural sway during quiet stance. We hypothesized that even a light, 1% of BW load placed above the natural body’s COM would destabilize the upright posture, decreasing the functional reach distance and increasing postural sway. To examine whether the effect of load is increased in the absence of visual information, the quiet stance task under the four load conditions was performed with eyes open and closed.
Materials and Methods
Sixteen right-handed participants (5 males, 11 females) ranging in age from 18 to 39 years (mean = 22, SD = 5.19 years) were recruited from the student body of Arizona State University. Participants reported no neuromuscular disorders, musculoskeletal injuries, falls occurring during the last 5 years, or any noticeable problems with postural stability. Informed consent, approved by the Institutional Review Board of Arizona State University, was obtained from all participants. Demographic information, including height and weight, was obtained. The height ranged between 1.52 and 1.85 m (mean = 1.68 m, SD = 0.08 m), weight ranged between 48 and 106 kg (mean = 68.97 kg, SD = 16.16 kg), and BMI ranged between 20.0 and 31.1 (mean = 24.4, SD = 4.6).
Four conditions of load were used: 0% (no load), 1, 3, and 5% of the BW. A light, customized vest with small pockets to hold the weights across the top of the shoulders was worn by the participants. Small, pre-weighed packets of lead pellets were used as weights. The weights calculated to constitute a percentage of BW and rounded to the nearest 100 g were divided into halves and placed in the pockets of the vest. The vest was adjusted to the body of each participant. The pockets containing weights were firmly secured with Velcro strips to prevent displacement of the weights during the testing session.
Participants performed two tasks: functional reach and quiet stance. During performance of both tasks, participants were barefoot, wearing thin socks. Functional reach is commonly used to assess postural stability for different clinical populations, including frail elderly patients and Parkinson’s disease patients.19,23 Distance of functional reach was assessed in the forward and two lateral (right and left) directions using procedures of Weiner and colleagues.25 During the forward reach, participants were asked to stand straight with the right side of the body adjacent to but not touching a wall. The right arm was stretched forward horizontally, parallel to the wall, with the hand positioned in a closed fist. During the lateral reaches, participants were asked to stand with the back turned to the wall, with either the right or left arm stretched horizontally, along the wall. Participants were instructed to reach as far as possible in each direction, maintaining the arm in the horizontal position and keeping both feet flat and in place on the floor. The position of the third metacarpal head was marked on a measuring grid affixed to the wall before the initiation of each reach and again when the maximal reach distance was achieved. The horizontal distance between the two marks was measured and recorded. In each direction, two trials of functional reach were performed in each of the four load conditions randomized across subjects. If there was more than a 2 cm difference between the two trials, a third trial was performed. Mean maximal reach distance was calculated for the two trials with the closest measured values and was subsequently used for analysis. The data were recorded manually on a score sheet for each participant.
During the quiet stance task, participants were instructed to stand still on a force platform (HUMAC Balance Board, CSMi, Inc., Stoughton, MA). The feet were positioned according to the HUMAC Balance Board instructions, approximately at shoulder width apart. For each subject, the feet position was marked on the top of the force platform to standardize measurements. Participants kept the arms folded across the chest. They were instructed to keep the head straight and focus their gaze on a visual marker affixed at eye level to the wall 2 m in front of them. When eyes were closed, participants were instructed to maintain the same position of the head as when the eyes were open. To assess postural sway, time-varying series of the center of pressure (COP) position were recorded in the mediolateral (X axis) and anterior–posterior (Y axis) directions at a sampling rate of 100 Hz. The data were filtered using a low-pass dual-pass Butterworth filter with a cut-off frequency of 10 Hz. Within each load condition, postural sway was evaluated under two conditions of visual feedback, with eyes open (EO) and eyes closed (EC), for a total of eight conditions. Two trials of 30 s duration were performed in each condition. This amount of data was deemed sufficient taking into account that 30–60 s of data were used for postural analysis in many studies.4,7,17,22 At least 15 s rest intervals between trials were provided for each load level. After four trials performed at each load level, participants stepped down from the platform and walked freely for two min. Participants were instructed to request longer rest periods if needed. The order of the load and visual conditions was randomized across subjects.
Capturing the movement of the COP is often used to measure postural stability. Although various COP metrics have been used, including amplitude of movement, velocity, acceleration, and jerk,24 amplitude and velocity of the COP are used most frequently as they have shown strong discriminative capabilities.7,13,17 We therefore assessed postural sway by computing four characteristics: sway area represented by the area of an ellipse inclusive of 95% of the COP data points,14 COP velocity, and sway variability separately along the mediolateral and anterior–posterior direction represented by SD of the corresponding COP coordinate. The obtained values of each characteristic were averaged between the two trials for each condition and participant.
The effect of load on the functional reach distance in each direction was examined with the use of a one-way ANOVA with repeated measures. A 2-way 4 × 2 (load, vision) ANOVA with repeated measures was applied to each postural sway characteristic. The significance level was set at 0.05. When a significant load effect was revealed, post hoc multiple comparisons were conducted using the Bonferroni test which adjusted the observed significance level.
Results
Functional Reach
The means for forward, right lateral, and left lateral reach distances in each load condition are shown in Fig. 1. Since reach distance depends on subject’s height, all functional reach data were normalized to the height of each subject. The one-way ANOVA revealed that increases in load caused significant decreases in reach distance in the forward [F(3, 45) = 15.82, p < .001] and left [F(3, 45) = 5.38, p = .003] directions. The effect of load on reach distance in the right direction was not significant (p > 0.1). Post hoc testing revealed that in the forward direction, reach distance was significantly higher in the no-load (0%) condition as compared to each loaded condition; however, there were no significant differences among the three loaded conditions. In the left direction, the only significant difference was between the 0 and 3% load conditions (p < 0.05).

The effect of load on the non-normalized maximal distance of functional reach in the forward and two lateral directions. The reach distance in the forward and left directions increased with application of load of 1 and 3% of BW, respectively, but it did not differ among the three loaded conditions. Here and in Fig. 2, the vertical bars show SE.
Postural Sway
The four sway characteristics are shown in Fig. 2. The load effect was significant for all outcome variables [sway area: F(3, 13) = 5.74, p < 0.005; lateral COP SD: F(3, 13) = 8.42, p < 0.001; anterior–posterior COP SD: F(3, 13) = 3.63, p < 0.05; and COP velocity: F(3, 13) = 4.76, p < 0.01]. Post hoc testing revealed that all characteristics except for the anterior–posterior COP SD significantly increased with load as compared to the no-load condition. Namely, sway area significantly increased with load in the 1% load condition. The lateral COP SD significantly increased under all three loaded conditions as compared to the no-load condition. The COP velocity significantly increased with load in the 1 and 5% load conditions. No significant differences were found among the three loaded conditions for any of the four characteristics.

The effect of load on the four characteristics of postural sway. All characteristics increased when a 1% of BW load was applied but further increases in load did not provide a significant effect in the majority of cases. All characteristics except for lateral COP SD were also significantly increased without visual feedback.
Removal of vision significantly increased sway area [F(1, 15) = 6.54, p < 0.05], COP velocity [F(1, 15) = 47.93, p < 0.001], and anterior–posterior COP SD [F(1, 15) = 9.19, p < 0.01] but not lateral COP SD. No significant interactions between vision and load were found.
Discussion
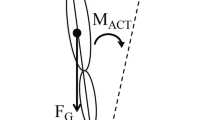
Previous research demonstrated that elevation of the total COM through placement of heavy load (about 10% of BW and higher) above the natural body COM destabilizes the upright posture.1,5,9,10,16,18,20 Our results show that the elevation of the COM using even as light of a load as 1% of BW also causes posture destabilization. The 1% of BW load influenced both functional reach distance and postural sway. The distance of the forward reach was shorter in the three loaded conditions as compared to the no-load condition. The shortening of the reach distance with load was likely caused by the need to keep the COP within the BOS. Indeed, the functional reach task requires subjects to move the COP close to the BOS boundary, as shown schematically in Fig. 3. The load caused a forward shift of the COM (shown in the figure as LCOM), requiring subjects to decrease the reach distance in order to keep the COP within the BOS. Thus, the shortening of the reach distance supports the elevation of the COM with load positioned on the shoulders and suggests that this elevation significantly influences postural control even with a 1% of BW load. This interpretation also accounts for the limited effect of further increases in load on forward reach distance. This is evident from the formula for the calculation of the height HLCOM at which the LCOM is located:
where H COM is the height of the COM without load, H SH is the height of the shoulders, m B is the body mass, and m L is the load mass. Since mL is present in both the numerator and denominator, HLCOM is influenced by HSH more than by mL. When load was increased, mL increased but H SH (as well as H COM) remained the same, explaining the lack of significant decreases in reach distance for loads beyond 1% of BW.

Schematic presentation of the COM and COP without load and with load (LCOM and LCOP, respectively) during forward reach.
The effect of load on reach distance in the lateral directions was smaller than that in the forward direction. A possible reason for this is that the COP may not approach the lateral BOS boundaries during maximal reach due to biomechanical constraints of the body that do not allow bending laterally far enough when the feet are at the shoulder width apart. This interpretation is supported by the substantially shorter reach distance in the two lateral directions with respect to that of the forward direction (see Fig. 1). The slightly higher effect of load in the left compared with right direction may be related to the dominance of the right arm. However, we cannot test this hypothesis because arm dominance of the participants was not recorded in this study.
With regard to postural sway, the effect of load on all four characteristics was similar, demonstrating a significant destabilization of posture with the 1% of BW load. This finding is consistent with the predictions of the inverted pendulum model, in that elevation of the COM through the placement of weights on the shoulders destabilizes upright posture. Further increases in load did not cause any substantial changes as compared to the 1% load level. In contrast to the height of LCOM that mainly depends on H SH and not on m L, the moment that rotates the body downward is proportional to both H SH and m L, and therefore, the inverted pendulum model predicts further destabilization of posture with increases in load. Thus, biomechanical considerations do not account for the finding that postural destabilization caused by 1% of BW load did not increase when heavier loads were applied. This finding, however, can be accounted for with behavioral considerations. It is possible that participants allowed the slight destabilization caused by the 1% of BW load because they were able to keep this level of destabilization under control and coping with it would require unnecessary effort. When heavier loads were applied, participants may have actively prevented further increases in postural sway characteristics as these increases would otherwise threaten stability. The findings of the previous studies that much heavier load (10% of BW and heavier) increase postural sway proportionally with increases in load18,20 suggest that starting from some level of load, young adults have difficulty to prevent further increases in postural sway, and their postural stability declines.
This study has a number of limitations. First, including of load levels higher that 5% of BW would allow to better span the results obtained here for light loads and the results obtained in the previous studies for heavy loads. Second, even though the inverted pendulum model of the upright posture that limits body motion to ankle rotation is functional, COM elevation may increase amplitudes of knee and hip rotations and change coordination among the joint motions, which was not examined here. Finally, the influence of individual anthropometric differences and gender on the destabilization caused by light load should be further investigated. For example, participant height may impact postural outcomes including functional reach, which prompted the normalization to height in the current report. Additional use of measurements of the arm length and other body parameters, including those from Eq. (1), may reveal individual differences in the effect of elevated COM on postural stability.
Despite these limitations, it can be summarized that our results demonstrate that a light, 1% of BW load placed on the shoulders causes relatively small, but significant destabilization of the upright posture in young, healthy adults. This finding suggests high sensitivity of postural stability to elevation of the COM, as predicted by the inverted pendulum model. The high sensitivity to COM elevation supports the inverted-pendulum mechanical properties of the body as the major challenge for neural control of standing and locomotion.6,8,11,12 It also generates prospects of the use of COM elevation with a light load for early detection of stability declines and development of effective interventions.
References
Al-Khabbaz, Y. S. S. M., T. Shimada, and M. Hasegawa. The effect of backpack heaviness on trunk-lower extremity muscle activities and trunk posture. Gait & Posture. 28:297–302, 2008.
Cavagna, G. A., H. Thys, and A. Zamboni. The sources of external work in level walking and running. J. Physiol. 262:639–657, 1976.
Chow, D., M. Kwok, J. Cheng, M. Lao, A. Holmes, A. Au-Yang, F. Y. Yao, and M. S. Wong. The effect of backpack weight on the standing posture and balance of schoolgirls with adolescent idiopathic scoliosis and normal controls. Gait & Posture. 24:172–181, 2006.
Hassan, B. S., S. Mockett, and M. Doherty. Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects. Ann Rheum Dis. 60:612–618, 2001.
Heller, M. F., J. H. Challis, and N. A. Sharkey. Changes in postural sway as a consequence of wearing a military backpack. Gait & Posture. 30:115–117, 2009.
Horak, F. B. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing 35(Supplement 2):ii7–ii11, 2006.
Howcroft, J., E. D. Lemaire, J. Kofman, and W. E. McIlroy. Elderly fall risk prediction using static posturography. PLoS ONE 12:e0172398, 2017.
Kuo, A. D., and J. M. Donelan. Dynamic principles of gait and their clinical implications. Phys Ther. 90:157–174, 2010.
Ledin, T., and L. M. Odkvist. Effects of increased inertial load in dynamic and randomized perturbed posturography. Acta Otolaryngol. 113:249–252, 1993.
Li, X., and A. S. Aruin. The effect of short-term changes in the body mass on anticipatory postural adjustments. Exp. Brain Res. 181:333–346, 2007.
Maki, B. E., and W. E. McIlroy. Postural control in the older adults. Gait Balance Disord. 12:635–658, 1996.
Massion, J. Postural control system. Curr. Opin. Neurobiol. 4:877–887, 1994.
Piirtola, M., and P. Era. Force platform measurements as predictors of falls among older people – a review. Gerontology. 52:1–16, 2006.
Prieto, T. E., J. B. Myklebust, R. G. Hoffmann, E. G. Lovett, and B. M. Myklebust. Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans. Biomed. Eng. 43:956–966, 1996.
Punakallio, A., S. Lusa, and R. Luukkonen. Protective equipment affects balance abilities differently in younger and older firefighters. Aviat. Space Environ. Med. 74:1151e1156, 2003.
Qu, X., and M. A. Nussbaum. Effects of external loads on balance control during upright stance. Gait Posture. 29:23e30, 2009.
Raymakers, J. A., M. M. Samson, and H. J. J. Verhaar. The assessment of body sway and the choice of the stability parameter(s). Gait Posture. 21:48–58, 2005.
Rugelj, D., and F. Sevšek. The effect of load mass and its placement on postural sway. Appl. Ergon. 42:860–866, 2011.
Schenkman, M., T. M. Cutson, M. Kuchibhatla, J. Chandler, and C. Pieper. Reliability of impairment and physical performance measures for persons with Parkinson’s disease. Phys Ther. 77:19–27, 1997.
Schiffman, J. M., C. K. Bensel, L. Hasselquist, K. N. Gregorczyk, and L. Piscitelle. Effects of carried weight on random motion and traditional measures of postural sway. Appl. Ergon. 37:607e614, 2006.
Shumway-Cook, A., and M. H. Woollacott. Motor control: Translating research into clinical practice. Philadelphia: Lippincott Williams & Wilkins, 2017.
The Canton Ticino study, A. Merlo, D. Zemp, E. Zanda, S. Rocchi, F. Meroni, M. Tettamanti, A. Recchia, U. Lucca, and P. Quadri. Postural stability and history of falls in cognitively able older adults. Gait Posture. 36:662–666, 2012.
Thomas, J. I., and J. V. Lane. A pilot study to explore the predictive validity of 4 measures of falls risk in frail elderly patients. Arch. Phys. Med. Rehabil. 86:1636–1640, 2005.
Visser, J. E., M. G. Carpenter, H. van der Kooij, and B. R. Bloem. The clinical utility of posturography. Clin. Neurophysiol. 119:2424–2436, 2008.
Weiner, D. K., P. W. Duncan, J. Chandler, and S. A. Studenski. Functional reach: a marker of physical frailty. J. Am. Geriatr. Soc. 40:203–207, 1992.
Winter, D. A. Human balance and posture control during standing and walking. Gait Posture. 3:193–214, 1995.
Winter, D. A., A. E. Patla, F. Prince, M. Ishac, and K. Gielo-Percza. Stiffness control of balance in quiet standing. J Neurophysiol. 80:1211–1221, 1998.
Zultowski, I., and A. S. Aruin. Carrying loads and postural sway in standing: The effect of load placement and magnitude. Work. 30:359–368, 2008.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Sean S. Kohles oversaw the review of this article.
Rights and permissions
About this article

Cite this article
Dounskaia, N., Peterson, D. & Bruhns, R.P. Destabilization of the Upright Posture Through Elevation of the Center of Mass. Ann Biomed Eng 46, 318–323 (2018). https://doi.org/10.1007/s10439-017-1957-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-017-1957-7