
Abstract
This study aims to investigate the age, period, and cohort effects on trends in activities of daily living (ADL) disability among Chinese older adults; and to explore these three temporal effects on gender and residence disparities in disability. We utilized multiple cross-sectional waves of the Chinese Longitudinal Healthy Longevity Survey data (1998–2018), including 89,511 participants aged above 65 years old. Our measurement of disability is the number of ADL items (dressing, bathing, indoor transferring, toileting, eating, and continence) participants can’t perform independently. Hierarchical age-period-cohort cross-classified random effects models were conducted to investigate age, period and cohort trends in ADL disability. Results showed that ADL disability increased with age at an increasing rate. A V-shaped cohort trend and a fluctuated period trend were identified. Females and urban residents were associated with more ADL limitations. When age increased, the gender and residence gaps in disability further increased. The cohort-based gender and residence inequalities in ADL limitations converged with successive cohorts. The period-based residence gap in ADL limitations diverged throughout the 20-year period, while the corresponding period-based change in gender disparity was not significant. These findings suggested that age, period, and cohort had different and independent effects on ADL disability among Chinese older adults. The age effect on trends in ADL is stronger compared to period and cohort effects. The gender and residence disparities in disability increased with age and decreased with successive cohorts. These patterns might help inform healthcare planning and the priorities for medical resource allocation accordingly.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In China, life expectancy at birth rapidly increased from 43.83 years in 1950 to 76.62 years in 2015 (United Nations, Department of Economic and Social Affairs, Population Division 2019). Meanwhile, the number of people aged above 65 years old increased from 49.91 million in 1982 to 190.59 million in 2020 (National Bureau of Statistics of the People's Republic of China 2021). Older people usually face higher risk of being disabled and use more medical care (Colombo et al. 2011). The increase in their number and life expectancy may affect the future sustainability of medical care systems and social support programs (Morciano et al. 2015). Hence, concern has emerged about whether this increased longevity among Chinese population will be accompanied by more disability, which may increase the demand for and costs of daily assistance, medical services and long-term care (Liang et al. 2015; Yu et al. 2016).
A better understanding of disability trends across the life course and over time is crucial to both aging population and whole society, due to disability leads to deterioration in quality of life for individuals and heavy burden for their families and long-term care system (Liang et al. 2015). Numerous studies have shown that the prevalence of age-specific disability decreased in recent years (Liang et al. 2015; Freedman et al. 2002; Feng et al. 2013); while other studies reported an increasing disability trend (Yu et al. 2016; Seeman et al. 2010) or a flat trend (Freedman et al. 2013; Sarkeala et al. 2011). However previous studies rarely adjusted for three unique effects related to disability trends, which are age, period and cohort (APC) effects. The age effect reflects biological and social processes of aging specific to individuals (Reither et al. 2009). The period effect refers to external factors that equally affect all age groups at a particular calendar time. The cohort effect reflects the different formative life experiences for successive generations (Canizares and Badley 2018; Zhang et al. 2020). As each temporal dimension distinctively contributes to the study of health, these temporal sources of variations in disability need to be distinguished. Failure to isolate APC effects would lead to bias and confounding results of disability trends (Zhang et al. 2020).
In order to examine the disability trends accurately, researchers began to estimate APC effects simultaneously, but could be improved further. An American study found that when adjusted for APC effects, a stable period trend and an increasing cohort trend in activities of daily living (ADL) disability were shown. However, unadjusted cohort trends in ADL disability showed continual declines (Lin et al. 2012). A European study covering 15 countries identified a small overall changes in disability over time periods and a U-shaped cohort trend (Beller and Epping 2021). A Hong Kong study found an increasing period trend in ADL disability from 2003 to 2012 and no significant cohort trend. The relative short cohort range (from 1904 to 1947) in this study may influence the exploration of cohort effects (Yu et al. 2016). Another study in China reported that ADL disability slowly increased from 1998 to 2014 and decreased with successive cohorts (Zhang et al. 2020). While this study used intrinsic estimator method for the APC analyses, this method may be a poor approximation to the process of social change and would produce larger bias in small samples when the underlying effects were zero than when they were not zero (Yang and Land 2009). Meanwhile it only focused on those people aged 80 years and above, which may not reflect the age effects entirely. Given these limitations in previous studies, researches using advanced methods to explore APC effects on disability trends in a longer time span are needed. While due to the identification problem induced by the exact linear dependency between APC (period = age + cohort), it is not possible to directly estimate the linear effect of any one of the APC variables holding the other two constant (Fosse and Winship 2019). Nowadays, numerous strategies to separate APC effects were developed, such as constrained generalized linear model (CGLM) (Fienberg and Mason 1979), APC model with intrinsic estimator algorithm (Yang et al. 2004), APC characteristic model (APCCM) (O'Brien 2015), hierarchical APC growth curve model (HAPC-GCM) (Lynch 2003) and hierarchical APC cross-classified random effects model (HAPC-CCREM) (Yang and Land 2006). The HAPC-CCREM was developed by Yang et al. in 2006, in which period and cohort effects are treated as level 2 variables to solve the identification problem (Yang and Land 2009). The HAPC-CCREM had been a useful tool to identify age, period, and cohort trends in health (Jiang and Wang 2018; Lin et al. 2014) and happiness (Yang 2008). However, some researchers criticized this model. For example, they thought that the estimation of this model would vary with the width of unequal intervals, since the HAPC-CCREM is a type of constrained estimator (Bell and Jones 2014, 2018). While Reither et al. (2015) have already addressed this critique and provided additional support for the use of HAPC-CCREM when analyzing data from repeated cross-sectional surveys. Thus, this study intends to investigate the disability trends among Chinese older adults using the HAPC-CCREM.
Substantial studies had demonstrated that disability disparities were associated with gender (Zeng et al. 2007), race (Lin et al. 2014), residence (urban/rural) (Liang et al. 2015), and socioeconomic status (SES) (Zimmer et al. 2012). However, evidence on cohort-based trends in disability disparities by these factors was limited and with mixed results (Freedman et al. 2002). An American study showed that the black–white disparity in disability decreased with successive cohorts except for ADL disparity among women (Lin et al. 2014). While a UK study reported that SES disparities in disability enlarged in later cohorts (Morciano et al. 2015). A Chinese study reported that cohort effects on gender and residence disparities in disability were not significant (Li 2015). Another Chinese study in Hong Kong reported that cohort-based trends of ADL disability were flat for both genders (Yu et al. 2016). However, most of these studies didn’t simultaneously adjusted for APC which may result in biased estimations (Yang and Land 2009); and most of them applied limited waves of longitudinal data. Indeed, a better understanding of the cohort effects on disability disparities by demographic factors and SES is necessary. In China, gender and residence (refer to urban and rural) disparities are two major sources of persistent social inequality (Li 2015). The unique economic, political, social and demographic transitions undergone in China may have distinct cohort effects on disability disparities, which may be different from that in western countries. Therefore, how gender and residence differentials in disability changed over age, period, and cohort among Chinese older people needs to be studied further.
Delineating disability trends is important in understanding individual’s health status as well as estimating the demand of medical and long-term care services. Using data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), one of the best sources of data on Chinese older people with multiple birth cohorts during the 20-year period from 1998 to 2018, this study aims to use the HAPC-CCREM to investigate age, period, and cohort effects on trends of ADL disability; and to explore these three temporal effects on gender and residence disparities in disability.
Methods
Data sources
This study used data of the 1998, 2000, 2002, 2005, 2008, 2011, 2014, and 2018 waves of CLHLS. Zeng had introduced the survey design in detail previously (Zeng and James 2002). The CLHLS is a nationwide survey conducted in a randomly selected half of the counties and cities in 22 Chinese provinces, covering approximately 85% of the total population in China (Zeng and James 2002). The CLHLS attempted to interview all the centenarians from the sampled area who voluntarily agreed to participate in the study. The CLHLS also adopted a targeted random-sample design to ensure representativeness through interviews with approximately equal numbers of male and female nonagenarians, octogenarians, and young-old (65–79 years old) living near the centenarians (Zeng et al. 2017). The response rate was 88% if those who were too sick to interview or who had migrated before the interview were considered as non-participants. If those people were excluded, the response rate was 98% (Zeng et al. 2001). According to previous assessment, the quality of the CLHLS data was high in terms of data completeness, reliability and validity (Gu 2008). Every participant provided written informed consent before the survey. The CLHLS has been approved by Research Ethics Committees of Duke University and Peking University. More details about sampling design of the CLHLS are shown in Online Resource.
Study samples
Since the CLHLS conducted over 20 years from 1998 to 2018 including older people across successive cohorts, it was suitable for the exploration of age, period, cohort effects on disability trends. There were 92,860 samples aged above 65 years old in all eight waves. Because the self-reported age after 105 years old was not reliable (Zeng et al. 2002) and most respondents at advanced ages suffered extremely high and varying levels of disability, which may lead to unstable estimates in analysis (Zimmer et al. 2012), we excluded 2202 participants aged above 105 years old. Then, 1147 participants were excluded further as they missed information on ADL. Thus, the final sample size in analyses was 89,511 (Details of the sample selection are given in Fig S1 in Online Resource).
Variables
ADL disability
Our measurement of disability is the number of ADL limitations. The CLHLS evaluated ADL using six items from the Katz’s ADL Index (Katz et al. 1963) including dressing, bathing, indoor transferring, toileting, eating, and continence for every participants in every survey. The number of ADL limitations in this study was calculated as the number of items that participants could not able to do without assistance. It ranged from zero to six, with lower value indicating better physical ability. Participants with one limitation or more were defined as ADL disabled.
Age, period, and cohort
Participants’ age divided by ten was grand mean centered for ease of interpretation of the intercept values (Yang and Land 2009). Period indicated the year in which the survey conducted, which included 1998, 2000, 2002, 2005, 2008, 2011, 2014, and 2018. Cohort was the year participants were born in. Participants who were born before 1900 or after 1940 were grouped separately to ensure a sufficient number of participants (Lin et al. 2012; Yu et al. 2016). We subsequently grouped other birth cohorts into five-year bands.
Covariates
Gender (male = 0; female = 1) and current residence (urban = 0; rural = 1) are key stratification factors. We also adjusted for participants’ demographic characteristics and SES, which were demonstrated their associations with ADL disability in previous studies (Zimmer et al. 2012; Zeng et al. 2007). Demographic characteristics included birthplace, marital status, and co-residence. Birthplace was dichotomized as urban and rural. Marital status was defined as married, separated (including divorced and separated), widowed and never married. Co-residence was defined as alone and living with others (including household members and living in a nursing home). SES included education and job. Education was defined as illiterate who hadn’t received any education and literate. The CLHLS collected participants’ job information through the following question ‘What was your main occupation before age 60?’ Considering most people were farmers at that time and positive effects from agricultural occupation on ADL ability according to previous studies (Zeng et al. 2007), we classified job into three categories: farmers, professional & governmental personnel (including professional and technical personnel and governmental, institutional or managerial personnel) and others (including industrial worker; commercial or service worker; military personnel and others).
Statistical methods
First, we summarized the basic characteristics of study samples in all and eight waves using means ± standard deviation or frequency (percentages). Then, we applied hierarchical age-period-cohort models to simultaneously estimate the age, period, and cohort trends of ADL disability for repeated cross-sectional data.
The HAPC model could address classical APC identification problem in two ways (Yang and Land 2009). First, we grouped individuals born in a five-year range into a single cohort to break the linear dependence among the APC dimensions. Second, the nonlinear transformations approach suggested applying a parametric nonlinear transformation, such as polynomials to at least of one of APC dimensions to break their linear relationships (Yang 2008). According to this strategy and previous findings of curvilinear age effects on health (Yang and Land 2009; Li 2015), this study proposed models of ADL limitations as a quadratic function of age.
We then fit HAPC-CCREM to examine APC effects on ADL disability. In each regression model, ADL disability (the number of ADL limitations) was regressed on age in linear and squared terms, and covariates (birthplace, marital status, co-residence, education and job) as needed. The coefficients of period, cohort, gender and residence were allowed to have random effects, which have been increasingly used in social sciences (Yang 2008). This design made it possible to explore the period-based and cohort-based trends of gender and residence disparities in ADL disability. In total, the model took the following form:
Level-1 Model:
where \({\mathrm{ADL}}_{ijk}\) stands for the number of ADL limitations for respondent i (for i = 1, 2, …, \({n}_{jk}\)) within period j (for j = 1, 2, …, 7) and cohort k (for k = 1, 2, …, 10); A and A2 denote age and age-squared, respectively; S denotes gender; R denotes residence; \({X}_{p}\) denotes the vector of other individual-level variables, including age by gender, age by residence to test how do gender and residence inequalities in ADL disability vary with age and control variables (birthplace, marital status, co-residence, education and job) that were known to be strongly associated with ADL disability. \({\beta }_{0jk}\) is the intercept indicating the cell mean for the reference group at mean age surveyed in period j and belonging to cohort k; \({\beta }_{1}\) and \({\beta }_{2}\) denote the fixed coefficients for age; \({\beta }_{3jk}\) and \({\beta }_{4jk}\) denote the random coefficients for gender and residence, respectively; \({\beta }_{p}\) denotes fixed coefficients for covariates; P is the maximum number of covariates included; \({e}_{ijk}\) is the random individual effect or cell residual, which is assumed normally distributed with mean 0 and a within-cell variance \({\sigma }^{2}\). Age divided by 10 is grand mean centered for ease of interpretation of the intercept values.
Level-2 Model:
The level-2 models test whether gender and residence disparities in ADL limitations varied by period or cohort through the specifications of random variance components for the random intercept and coefficients. \({\beta }_{0jk}\) denotes random intercept, which specifies that the overall mean varies from period to period and from cohort to cohort. \({\gamma }_{0}\) is the expected mean at the zero values of all level-1 variables averaged over all periods and cohorts; \({u}_{0j}\) is the overall period effect regarding residual random coefficients of period j averaged over all cohorts with variance \({\sigma }_{u0}\); \({v}_{0k}\) is the overall cohort effect in terms of residual random coefficients of cohort k averaged over all periods with variance \({\sigma }_{v0}\). \({\gamma }_{3}\) and \({\gamma }_{4}\) are the level-2 fixed effects coefficients that represent the fixed effects of gender and residence, respectively. In order to test whether gender and residence stratifications of ADL limitations varied by period or cohort, we specify that coefficients have period effects (\({u}_{3j}\) and \({u}_{4j}\)), and cohort effects (\({v}_{3k}\) and \({v}_{4k}\)), whose corresponding random variance components are \({\sigma }_{u3}\), \({\sigma }_{u4}\) and \({\sigma }_{v3}\), \({\sigma }_{v4}\). These random variance components of period and cohort since the intercept and coefficients are assumed to have multivariate normal distributions (Yang 2008).
Therefore, in the level-1 model, we could test whether gender and residence gaps in ADL limitations varied with age by including interaction terms of age with gender or residence. The level-2 model could test whether these differentials varied by period or cohort. Based on the combination of two-level models, we conducted seven models to assess the APC effects on ADL limitations and the change of gender and residence disparities in ADL limitations with APC. Model 1 was a two-level model with a fixed effect for age and random effects for period and cohort to explore the net APC effects on ADL limitations. Model 2 added the key independent variables, gender and residence to explore their influence on ADL limitations. Model 3 added the interactions between age and gender or residence to explore how gender and residence gaps in ADL limitations varied with age. Model 4 adjusted covariates based on Model 3. Then, Model 5 added random effects of coefficient of gender to explore how gender disparities in ADL limitations varied by period and cohort. Similarly, Model 6 added random effects of coefficient of residence to explore how residence disparities in ADL limitations varied by period and cohort. Model 7 combined Model 4–6 to conduct a full model. Analyses were conducted using SAS PROC MIXED (Yang and Land 2009). Bayesian Information Criterion (BIC) was used to compare models concerning the goodness of fit, the smaller BIC value indicating the better model fit (Raferty 1986).
Results
Basic characteristics of samples
Table 1 showed the basic characteristics of samples in all and every survey. There were 89,511 samples in total with an average age of 87.5. There were more females and rural residents in all and most surveys. Most of respondents were born in a rural area, illiterate, working as farmers, living with others and widowed. In total, the average ADL limitations of samples was 0.77 and ranged from 0.62 to 1.05 among eight surveys.
Age-period-cohort trends and differentials in ADL limitations
Table 2 presented estimates of fixed effects of all individual-level covariates and random-effect variance components. From Model 1 in Table 2 and Fig. 1, we identified that net of random period and cohort effects, the effect of age was curvilinear, indicating that ADL limitations increased at an increasing rate as one moved through the life course. Level-2 results suggested that ADL limitations varied in a smaller magnitude by period and cohort, relative to the age effect. The period effect was nearly flat from 1998 to 2008, followed by an upward trend. The cohort effect was V-shaped, indicating the earlier and later cohort had relative more ADL limitations at average compared to middle cohorts. Model 2 indicated that males and rural residents had significantly fewer ADL limitations relative to females and urban residents, when age, period and cohort effects were considered.

Overall age, period, and cohort effects on ADL limitations
Age variations in gender and residence disparities in ADL limitations
Model 3 indicated that the gender and residence disparities in ADL limitations varied significantly with age. When age increased, the gender gap and residence gap further increased. Model 4 revealed that birthplace, education, marital status, job and living condition had significant influences on ADL limitations. Those respondents who were born in rural area, literate, married, living alone and farmers had fewer ADL limitations.
Comparing Model 3 with Model 4, the age, gender and residence effects remained highly significant but decreased a little in size. All the interaction effects remained significant when confounding variables were considered. The interaction effects of gender with age shrank in size, while the interaction effects of residence with age enlarged. The smaller BIC statistic indicated a better model fit for Model 4 than any of the previous models. While this finding was not surprising in light of previous studies of social correlates of ADL disability. It also suggested two findings: one is that the individual-level effects still hold when level-2 heterogeneity, reflecting the period and cohort effects, were taken into account; another one is that net of age and other individual-level covariate, there are significant variations which can be attributed to period-specific factors.
Time trends of gender and residence disparities in ADL limitations
Model 5 and 6 displayed that gender and residence disparities in ADL limitations varied significantly with cohort net of age, period, and other factors. The corresponding period change in residence disparities was significant, while in gender disparities was not significant. From Fig. 2, we found that the gaps in ADL limitations between genders decreased across cohorts, which was largely because of the decreasing ADL limitations for females and relatively stable trends for males among successive cohorts.

Predicted cohort variations in gender disparity in ADL limitations
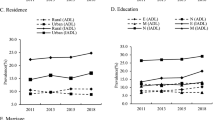
Figure 3a demonstrated that residence gaps also decreased across cohorts. Rural residents experienced an upward trend in ADL limitations and urban residents experienced a relatively stable trend. Figure 3b demonstrates that the urban and rural gap was much more pronounced throughout the 20-year period. From 1998 to 2005, rural residents experienced a downward trend in ADL limitations and urban residents experienced some fluctuations. Then from 2005 to 2018, both urban and rural residents showed similar fluctuations and a larger residence gap in more recent years.

Predicted cohort and period trends in residence disparity in ADL limitations
Discussion
Using eight waves of the CLHLS data from 1998 to 2018, we applied the HAPC-CCREM to explore trends of ADL disability among Chinese older adults. Our findings indicated that the number of ADL limitations increased with age at an increasing rate. We also found a V-shaped cohort trend and a fluctuated period trend. Females and urban residents were associated with more ADL limitations. When age increased, the gender and residence gaps in disability further increased. The cohort-based gender and residence inequalities in ADL limitations converged with successive cohorts. The period-based residence gap in ADL limitations diverged throughout the 20-year period, while the corresponding period-based change in gender disparity was not significant.
A V-shaped trend was found among successive cohorts, indicating the earlier and later cohort had more ADL limitations at average compared to middle cohorts, which was consistent with previous studies (Beller and Epping 2021; Lin et al. 2014). Beller and colleagues used data from 15 European countries found that when adjusted for APC effects simultaneously, a general cross-country U-shaped birth cohort effect was shown for overall disability (Beller and Epping 2021). According to previous researches, there were two opposing processes, compression of morbidity and expansion of morbidity, influenced health of older people (Zeng et al. 2017). Compression of morbidity is that the later cohorts might benefit from progress in advanced disease treatment, declining disability effects of some chronic diseases, and improved standards of living. These benefits of success imply that the later cohorts could reach older ages with better health and functional capacity in daily living. While expansion of morbidity is that improvements in medical conditions and living standards in recent years may increase the survival rate of individuals in relatively poor health status, which might increase overall ADL disabilities (Zeng et al. 2017). Participants in earlier cohorts who could survive to advanced age suffering possible hardships in early life stage were likely to be more robust. Those weaker individuals in earlier cohorts almost died before the advanced age (Zeng et al. 2007), only those healthier were still alive. Thus, process of compression of morbidity might be dominate from the earliest cohort to middle cohort, leading to a downward cohort trend among them. While older adults in middle cohort to latest cohort were relatively young, the selective survival effect may be weaker (Yu et al. 2016). Thus, process of expansion of morbidity might be dominate from the middle cohort to latest cohort, leading to an upward cohort trend among them.
The period effects on ADL limitations were minor and fluctuated, which is consistent with the findings from previous studies (Lin et al. 2012; Martin et al. 2011; Beller and Epping 2021). An American study reported ADL disability remained stable across time when adjusted for age, cohort, and other sociodemographic variables (Lin et al. 2012). ADL disability referred to the culmination of the disablement process, which typically represented severer limitations than that of instrumental activities of daily living (IADL) or physical functioning (Zimmer et al. 2012). Thus, the period change on ADL disability may not be obvious and sensitive. Further observation of period-based trend on ADL disability in a longer period is needed.
We identified that males had significantly fewer ADL limitations than did females, which was in line with the previous studies (Zimmer et al. 2012; Crimmins et al. 2011, 2019; Zeng and James 2002). According to previous findings, females have lower grip strength measures, slower gait speed and worse balance compared with males (Ahrenfeldt et al. 2019; Wheaton and Crimmins 2016). Thus, the general weakness of women’s physique compared with men might influence the gender gap in ADL. In addition, this gap between genders is more marked with increasing age, thus confirming findings from other studies (Oksuzyan et al. 2010; Scheel-Hincke et al. 2020; Serrano-Alarcón and Perelman 2017). A widening of the gender difference in ADL with increasing age may be consistent with the survival effect, which could leave the healthiest men in the sample (Austad and Fischer 2016). Meanwhile, cumulative disadvantage theory believed that effects of risk factors would accumulate over the life course, thus increasing heterogeneity in later life (Ferraro and Kelley-Moore 2003). Those individuals experienced disadvantages in early life would face a cascade of additional risks to health and well-being throughout their lives (O'Rand and Hamil-Luker 2005). Due to the preference for sons in old Chinese society (Zhang et al. 2008), a majority of females experienced relatively tough early lives than males, reflecting in their lower possibilities to get adequate food, education and medical service during sickness (Zeng et al. 2007). Thus, very careful attention should be given to females to prevent or postpone the onset of disability and to ensure they obtain adequate care.
In line with other studies (Li 2015; Zeng and James 2002), we found that urban residents were more disabled than rural residents were and this disparity diverged with increasing age. There was a household registration system (Hukou), which divided population into agricultural and nonagricultural area with different economic, social and healthcare systems in China (Chen et al. 2010). The living standards and access to health care in rural area were much worse than urban area for a long time (Li 2015). There are some potential explanations for residence disparity. First, most of rural residents did agricultural work, which could help them to maintain their capacity for daily living. Almost urban residents did non-manual work before they were retired. They may not engage in as much physical activity as rural residents did (Zeng and James 2002). Second, there are more facilities available to assist older adults in urban area than in rural area. Therefore, rural residents have to perform daily activities by themselves, which could help them to maintain their physical capacity for a longer time (Zeng and James 2002).
We found that gender and residence disparities in ADL limitations varied significantly with cohorts. When confounding factors were adjusted, these stratifying effects were not statistically significant. Meanwhile, the gender and residence gaps were larger in the earlier cohorts than in the later cohorts. The reduced gender gap may largely due to the decreasing ADL limitations for females among successive cohorts. The improvement in ADL ability for females in later cohorts may partly due to the increasing schooling rate (Liang et al. 2015). Previous studies also demonstrated that the increase in educational achievements might contribute to favorable ADL trends in late life (Lin et al. 2014; Freedman et al. 2002). Due to increasing disabilities among rural residents in later cohorts, the residence gaps converged. One potential explanation may be that in earlier cohorts, there were more rural residents did agricultural jobs, which may help them maintain their capacity for daily living (Zeng and James 2002). The proportion of farmers reduced in later cohorts, thus their advantages in ADL abilities may have diminished somewhat. Another potential explanation was related to the selective survival effect. Due to large gaps of living conditions between urban and rural area in earlier cohorts, rural residents who endured such hardship in life and survived tend to be healthier than urban residents (Zeng and James 2002; Zimmer et al. 2012). With the rapid development and improvement of rural economic and social conditions, the gaps of overall living conditions between urban and rural area were gradually narrowing in later cohorts, thus the effect of death selection may be reduced as well. More rural residents in relatively poor health status were saved by improved medical conditions, which might increase overall ADL disabilities in rural area (Zeng et al. 2017).
This study had some limitations. First, ADL disability was a self-reported indicator rather than more objective tests of function status. While, for the CLHLS, the results of ADL and other objective health measures show good internal consistency and construct validity (Gu 2008). In future work, other objective indicators of functional status such as grip strength or the chair stand test could be used to obtain a more complete picture of APC trends in health (Beller et al. 2019). Second, due to the data limitation, the earliest and latest birth cohorts did not capture a full age distribution, which may bias the estimates for cohort trends. Thus, nationally surveillance of health changes could be proceeded. Third, in this study we focused on basic effects of APC and individual variables. Effects from macroeconomic and medical variables on ADL disability should be further explored.
Conclusion
In conclusion, we found that ADL disability increased with age at an increasing rate among Chinese older adults. The gender and residence inequalities in disability enlarged with age, while reduced with cohorts. These findings of dynamics of disability could help forecast future disability trends and care services needed and hence, to inform healthcare planning and the priorities for resource allocation (Yu et al. 2016).
Data availability
The dataset of CLHLS could be obtained upon application on the website (https://sites.duke.edu/centerforaging/programs/chinese-longitudinal-healthy-longevity-survey-clhls/).
Code availability
Analyses were conducted using SAS PROC MIXED.
References
Ahrenfeldt LJ, Scheel-Hincke LL, Kjærgaard S et al (2019) Gender differences in cognitive function and grip strength: a cross-national comparison of four European regions. Eur J Public Health 29:667–674. https://doi.org/10.1093/eurpub/cky266
Austad SN, Fischer KE (2016) Gender differences in lifespan. Cell Metab 23:1022–1033. https://doi.org/10.1016/j.cmet.2016.05.019
Bell A, Jones K (2014) Don’t birth cohorts matter? A commentary and simulation exercise on Reither, Hauser, and Yang’s (2009) age–period–cohort study of obesity. Soc Sci Med 101:176–180. https://doi.org/10.1016/j.socscimed.2013.09.004
Bell A, Jones K (2018) The hierarchical age–period–cohort model: why does it find the results that it finds? Qual Quant 52:783–799. https://doi.org/10.1007/s11135-017-0488-5
Beller J, Epping J (2021) Disability trends in Europe by age-period-cohort analysis: Increasing disability in younger cohorts. Disabil Health J 14:100948–100948. https://doi.org/10.1016/j.dhjo.2020.100948
Beller J, Miething A, Regidor E et al (2019) Trends in grip strength: age, period, and cohort effects on grip strength in older adults from Germany, Sweden, and Spain. SSM - Popul Health 9:100456. https://doi.org/10.1016/j.ssmph.2019.100456
Canizares M, Badley EM (2018) Generational differences in patterns of physical activities over time in the Canadian population: an age-period-cohort analysis. BMC Public Health. https://doi.org/10.1186/s12889-018-5189-z
Chen F, Yang Y, Liu G (2010) Social change and socioeconomic disparities in health over the life course in China: a cohort analysis. Am Sociol Rev 75:126–150. https://doi.org/10.1177/0003122409359165
Colombo F, Llena-Nozal A, Mercier J et al (2011) Help wanted? Providing and paying for long-term care. OECD Publishing, Paris
Crimmins EM, Kim JK, Solé-Auró A (2011) Gender differences in health: results from SHARE, ELSA and HRS. Eur J Public Health 21:81–91. https://doi.org/10.1093/eurpub/ckq022
Crimmins EM, Shim H, Zhang YS et al (2019) Differences between men and women in mortality and the health dimensions of the morbidity process. Clin Chem 65:135–145. https://doi.org/10.1373/clinchem.2018.288332
Feng Q, Zhen Z, Gu D et al (2013) Trends in ADL and IADL disability in community-dwelling older adults in Shanghai, China, 1998–2008. J Gerontol B-Psychol 68:476–485. https://doi.org/10.1093/geronb/gbt012
Ferraro KF, Kelley-Moore JA (2003) Cumulative disadvantage and health: long-term consequences of obesity? Am Sociol Rev 68:707–729. https://doi.org/10.2307/1519759
Fienberg SE, Mason WM (1979) Identification and estimation of age-period-cohort models in the analysis of discrete archival data. Sociol Methodol 10:1–67. https://doi.org/10.2307/270764
Fosse E, Winship C (2019) Analyzing age-period-cohort data: a review and critique. Annu Rev Sociol 45:467–492. https://doi.org/10.1146/annurev-soc-073018-022616
Freedman VA, Martin LG, Schoeni RF (2002) Recent trends in disability and functioning among older adults in the United States: a systematic review. JAMA 288:3137–3146. https://doi.org/10.1001/jama.288.24.3137
Freedman VA, Spillman BC, Andreski PM et al (2013) Trends in late-life activity limitations in the United States: an update from five national surveys. Demography 50:661–671. https://doi.org/10.1007/s13524-012-0167-z
Gu D (2008) General data quality assessment of the CLHLS. In: Zeng Y, Poston D, Vlosky D, Gu D (eds) Healthy longevity in China: demographic, socioeconomic and psychological dimensions. Springer, Dordrecht, pp 39–60
Jiang J, Wang P (2018) Health status in a transitional society: urban-rural disparities from a dynamic perspective in China. Popul Health Metr 16:22–22. https://doi.org/10.1186/s12963-018-0179-z
Katz S, Ford A, Moskowitz R et al (1963) Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 185:914
Li T (2015) The new methodologies of elderly health studies. China Population Publishing House, Beijing
Liang Y, Song A, Du S et al (2015) Trends in disability in activities of daily living among Chinese older adults, 1997–2006: the China Health and Nutrition Survey. J Gerontol A-Biol 70:739–745. https://doi.org/10.1093/gerona/glu204
Lin S, Beck AN, Finch BK et al (2012) Trends in US older adult disability: exploring age, period, and cohort effects. Am J Public Health 102:2157–2163. https://doi.org/10.2105/AJPH.2011.300602
Lin S, Beck AN, Finch BK (2014) Black-white disparity in disability among U.S. older adults: age, period, and cohort trends. J Gerontol B-Psychol 69:784–797. https://doi.org/10.1093/geronb/gbu010
Lynch SM (2003) Cohort and life-course patterns in the relationship between education and health: a hierarchical approach. Demography 40:309. https://doi.org/10.2307/3180803
Martin LG, Zimmer Z, Hurng BS (2011) Trends in late-life disability in Taiwan, 1989–2007: the roles of education, environment, and technology. Popul Stud (camb) 65:289–304. https://doi.org/10.1080/00324728.2011.604730
Morciano M, Hancock RM, Pudney SE (2015) Birth-cohort trends in older-age functional disability and their relationship with socio-economic status: evidence from a pooling of repeated cross-sectional population-based studies for the UK. Soc Sci Med 136:1–9. https://doi.org/10.1016/j.socscimed.2015.04.035
National Bureau of Statistics of the People's Republic of China (2021) China's National Population Census. http://data.stats.gov.cn/easyquery.htm?cn=C01. Accessed 7 Sept 2021
O’Brien R (2015) Age-period-cohort models: approaches and analyses with aggregate data. CRC Press, Boca Raton
Oksuzyan A, Crimmins E, Saito Y et al (2010) Cross-national comparison of gender differences in health and mortality in Denmark, Japan and the US. Eur J Epidemiol 25:471–480. https://doi.org/10.1007/s10654-010-9460-6
O’Rand AM, Hamil-Luker J (2005) Processes of cumulative adversity: childhood disadvantage and increased risk of heart attack across the life course. J Gerontol B-Psychol 60:117
Raferty A (1986) Choosing models for cross-classifications. Am Sociol Rev 51:145–146
Reither EN, Hauser RM, Yang Y (2009) Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States. Soc Sci Med 69:1439–1448. https://doi.org/10.1016/j.socscimed.2009.08.040
Reither EN, Land KC, Jeon SY et al (2015) Clarifying hierarchical age–period–cohort models: a rejoinder to Bell and Jones. Soc Sci Med 145:125–128. https://doi.org/10.1016/j.socscimed.2015.07.013
Sarkeala T, Nummi T, Vuorisalmi M et al (2011) Disability trends among nonagenarians in 2001–2007: vitality 90+ Study. Eur J Ageing 8:87–94. https://doi.org/10.1007/s10433-011-0188-2
Scheel-Hincke LL, Möller S, Lindahl-Jacobsen R et al (2020) Cross-national comparison of gender differences in ADL and IADL in Europe: findings from SHARE. Eur J Ageing 17:69–79. https://doi.org/10.1007/s10433-019-00524-y
Seeman TE, Merkin SS, Crimmins EM et al (2010) Disability trends among older Americans: National Health and Nutrition Examination Surveys, 1988–1994 and 1999–2004. Am J Public Health 100:100–107. https://doi.org/10.2105/AJPH.2008.157388
Serrano-Alarcón M, Perelman J (2017) Ageing under unequal circumstances: a cross-sectional analysis of the gender and socioeconomic patterning of functional limitations among the Southern European elderly. Int J Equity Health 16:175–175. https://doi.org/10.1186/s12939-017-0673-0
United Nations, Department of Economic and Social Affairs, Population Division (2019) World Population Prospects 2019. https://population.un.org/wpp/DataQuery/. Accessed 10 May 2020
Wheaton FV, Crimmins EM (2016) Female disability disadvantage: a global perspective on gender differences in physical function and disability. Ageing Soc 36:1136–1156. https://doi.org/10.1017/S0144686X15000227
Yang Y (2008) Social inequalities in happiness in the United States, 1972 to 2004: an age-period-cohort analysis. Am Sociol Rev 73:204–226. https://doi.org/10.1177/000312240807300202
Yang Y, Land KC (2006) A mixed models approach to the age-period-cohort analysis of repeated cross-section surveys, with an application to data on trends in verbal test scores. Sociol Methodol 36:75–97. https://doi.org/10.1111/j.1467-9531.2006.00175.x
Yang Y, Land K (2009) Age-period-cohort analysis: new models, methods, and empirical applications. CRC Press, Boca Raton
Yang Y, Fu WJ, Land KC (2004) A methodological comparison of age-period-cohort models: the intrinsic estimator and conventional generalized linear models. Sociol Methodol 34:75–110. https://doi.org/10.1111/j.0081-1750.2004.00148.x
Yu R, Wong M, Chang B et al (2016) Trends in activities of daily living disability in a large sample of community-dwelling Chinese older adults in Hong Kong: an age-period-cohort analysis. BMJ Open 6:e013259–e013259. https://doi.org/10.1136/bmjopen-2016-013259
Zeng Y, James W (2002) Functional capacity and self-evaluation of health and life of oldest old in China. J Soc Issues 58:733–748. https://doi.org/10.1111/1540-4560.00287
Zeng Y, James W, Xiao Z et al (2001) The healthy longevity survey and the active life expectancy of the oldest old in China. Population: an English Select 13:95–116
Zeng Y, James WV, Xiao Z et al (2002) Sociodemographic and health profiles of the oldest old in China. Popul Dev Rev 28:251–273. https://doi.org/10.1111/j.1728-4457.2002.00251.x
Zeng Y, Gu D, Land KC (2007) The association of childhood socioeconomic conditions with healthy longevity at the oldest-old ages in China. Demography 44:497–518. https://doi.org/10.1353/dem.2007.0033
Zeng Y, Feng Q, Therese H et al (2017) Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet 389:1619–1629. https://doi.org/10.1016/S0140-6736(17)30548-2
Zhang Z, Gu D, Hayward MD (2008) Early life influences on cognitive impairment among oldest old Chinese. J Gerontol B-Psychol 63:S25–S33. https://doi.org/10.1093/geronb/63.1.S25
Zhang P, Lv Y, Li Z et al (2020) Age, period, and cohort effects on activities of daily living, physical performance, and cognitive functioning impairment among the oldest-old in China. J Gerontol A-Biol 75:1214–1221. https://doi.org/10.1093/gerona/glz196
Zimmer Z, Martin LG, Nagin DS et al (2012) Modeling disability trajectories and mortality of the oldest-old in China. Demography 49:291–314. https://doi.org/10.1007/s13524-011-0075-7
Funding
This study was funded by the National Natural Science Foundation of China (Grant Number 71490732).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation and analysis were performed by XH, SG, XZ, XS, and YG. The first draft of the manuscript was written by XH. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The CLHLS has been approved by Research Ethics Committees of Duke University and Peking University.
Consent to participate
Every participant provided written informed consent before the survey.
Consent for publication
Not applicable.
Additional information
Responsible editor: Marja J. Aartsen
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hu, X., Gu, S., Zhen, X. et al. Trends in activities of daily living disability among Chinese older adults from 1998 to 2018: an age-period-cohort analysis. Eur J Ageing 19, 1167–1179 (2022). https://doi.org/10.1007/s10433-022-00690-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10433-022-00690-6