
Abstract
Aim
Associations among screen time, dietary habits, cognition, and academic achievement with differences depending on different screen behaviors have been reported. This study aimed to analyze the associations among passive (TV viewing) and active (using other electronic devices) screen time and academic achievement and executive functions in schoolchildren and to assess whether this relationship is mediated by diet quality.
Subjects and methods
This was a cross-sectional study including 562 schoolchildren (M age = 9.58, 52,14% girls). Sociodemographic and anthropometric variables, academic achievement, executive functions, screen time, dietary habits, and cardiorespiratory fitness were assessed. ANCOVA models were conducted to test mean differences in academic achievement, executive functions, and diet by screen time categories. The PROCESS macro was used for mediation analyses.
Results
The results suggest that children who spent >3 h watching TV had lower academic achievement. Children who spent >3 h using other electronic devices had more inhibition, although differences disappeared after adjusting for confounders. Both types of screen use were associated with a lower quality of diet (p <.05).
Conclusion
Diet quality was a significant mediator between both screen time and academic achievement. Longer screen time leads to poorer food choices and this, in turn, affects academic achievement. Furthermore, this preliminary finding supports potential differences between passive and active screen use.
Clinical trial registration
MOVI-da-Fit! http://clinicaltrials.gov/ct2/show/NCT03236337. First Registered: August 1, 2017.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Screen time has been associated with several negative physical health markers, such as an increased cardiometabolic risk as well as worse cognition (the set of mental processes that contribute to perception, memory, intellect, and action) and academic achievement (AA) and in general, with poorer psychological health (Adelantado-Renau et al. 2019; Costigan et al. 2013; Page et al. 2010; Saunders and Vallance 2017; Wu et al. 2017). Despite this, the average of screen time has gradually increased in children and adolescents worldwide. On average, 53.3% of children and adolescents exceed the screen time recommendation of 2 h/day (Strasburger et al. 2013), and more than 3.6 h/day in screen-based behaviors, with TV viewing as the most prevalent use of screen time, 2.6 h/day (Thomas et al. 2020). However, the nature of these associations and mechanisms though which different types of screen behaviors are associated with cognition and AA and their interactions with dietary habits remain unexplored.
The impact of screen media on functional connectivity between cognition-related brain areas is controversial. While some empirical studies have found a reduction in brain connectivity related to screen time (Hong et al. 2013; Horowitz-Kraus and Hutton 2018; Takeuchi et al. 2015), others have reported positive or null effects (Adelantado-Renau et al. 2019), possibly because screen-related sedentary behavior does not refer to a single concept but rather encompasses several screen types whose complexity of use suggests that we are not dealing with the same behavior (Paulus et al. 2019). Some studies have reported that more passive screen use, such as watching television and video viewing, has a detrimental effect on cognition and AA (Horowitz-Kraus and Hutton 2018; Suggate and Martzog 2020), whereas others have found that more active screen use, which involves cognitively or physically engaging screen activities, may be beneficial (Sweetser et al. 2012; Walsh et al. 2020). Last, it has also been postulated that the detrimental effect of screen time on cognition and AA may be because this behavior takes time away from other activities, such as doing homework, reading books, sleeping, socializing, being physically active, or engaging in creative play (Horowitz-Kraus and Hutton 2018; Sharif et al. 2010).
Excessive screen time was associated with higher energy intake and lower fruit and vegetable consumption, which might be due to distractors and food advertisements (Cartanyà-Hueso et al. 2021; Shang et al. 2015; Wärnberg et al. 2021). In addition, unhealthy dietary patterns with low consumption of fruit, fish, and vegetables and high consumption of junk food have been associated with lower AA (Naveed et al. 2020; Vassiloudis et al. 2014), which might be due to the effect of nutrients on the brain (Naveed et al. 2020). Furthermore, two studies have examined the combined impact of diet and screen time on AA, showing that adherence to diet and screen time recommendations is associated with higher AA (Faught et al. 2017, 2019).
The aim of this study was twofold: first, to analyze the association between screen time behavior with quality of diet, executive functions, and AA; and second, to examine whether quality of diet acts as a mediator of the relationship between each screen time behavior and AA.
Material and methods
Study design and participants
The present study is a cross-sectional analysis of the baseline data of MOVI-daFit!, a cluster-randomized controlled trial (NCT03236337). This study followed the AGReMA statement for reporting mediation analyses (Lee et al. 2021) (appendix Table A.1). The study design, sampling procedures and methods have been fully described elsewhere REF (Martínez-Vizcaíno et al. 2019). Briefly, children aged 9 to 11 years (n = 559) belonging to 10 schools from Cuenca (Spain) were examined between September to October 2017, by trained researchers following standardized procedures. All schoolchildren met the following inclusion criteria: (i) not having any Spanish learning disabilities and (ii) not having any chronic disease or any mental or physical disorder.
MOVI-daFIT! was approved by the Clinical Research Ethics Committee of the Virgen de la Luz Hospital in cuenca (REG: 2016/PI021) and by the Board of Governors of each school. Parents were invited to an informative meeting and provided written consent. Children were asked to provide verbal consent prior to the completion of each test.
Variables and measurements
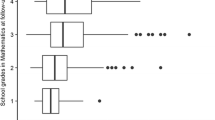
Academic achievement was assessed by the final grades in language and mathematics from the previous year (2016/17; 3rd and 4th grades). These scores could range from 1 (minimum) to 10 (maximum).
Executive functions were measured using the NIH Toolbox administered by an iPad app (Weintraub et al. 2013).
Inhibition was measured with the Flanker task (Zelazo et al. 2013). Participants were asked to indicate the left–right orientation of a central stimulus while inhibiting attention to the potentially incongruent stimuli surrounding it. In some trials, the orientation of the flanking stimuli was congruent with the orientation of the central stimulus, and in other trials, the orientation was incongruent. The version included four practice trials, and if passed, a 20-trial block was presented. A final score was calculated incorporating both accuracy and reaction time.
Cognitive flexibility was assessed using the Dimensional Change Card Sort Test (Zelazo et al. 2013). Participants were presented two target cards and asked to sort a series of bivalent test cards, first according to “shape” and then according to “color.” A four-trial practice was presented; if they passed, participants were presented with a 30-trial block. A final score was calculated incorporating accuracy and reaction time.
Working memory was assessed with the List Sorting Working Memory Test (Tulsky et al. 2013). Participants were required to repeat the names of a set of items that were visually and audibly presented. Then, participants were required to name the presented items while ordering them from smallest to largest. In each trial, the number of items increased by one. In the first part of the test, all items belonged to the same category, and in the second part, items from two categories were presented together, and children had to name items by category and size. Final scores were based upon a sum of the total correct trials across the two lists.
Screen time was measured by using a questionnaire completed by parents, in which they were asked about the number of hours of leisure time that the child spent viewing TV or using other electronic devices (computers, tablets, smartphones, or videogames) during the weekdays and weekend. The averages (in terms of frequency per week and hours per week) were then divided by seven to calculate the average of h/day of screen time. These data were categorized, based on previous recommendations (Tremblay et al. 2011), as adequate (<2 h/day), high (2-3 h/day), and very high (>3 h/day) when exceeding recommendations.
Diet quality was estimated using the Children’s Eating Habits Questionnaire (CEHQ), completed by parents (Lanfer et al. 2011), whose food frequency section allowed parents to report the frequency of their child’s consumption of 15 food items in a typical week during the preceding 4 weeks. Response options were: “Never,” “Less than once a week”, “Once a week,” “2–4 times a week,” “5–6 times a week,” “1 time per day,” and “2 or more times per day.” A health dietary quality index (HDQI) was calculated from the CEHQ as a measure of the extent to which children’s dietary intake follows nutritional guidelines (Arvidsson et al. 2017). Briefly, healthy dietary recommendations include limiting the intake of refined sugars, reducing fat intake, especially saturated fat, choosing whole grains, when possible, consuming 400–500 g of fruits and vegetables per day and fish 2–3 times per week. The items with high scores (higher scores indicates greater frequency of consumption) were the following: consumption of fruit, vegetables, milk, cheese or other dairy products, cereals, bread, and fish. Otherwise, the items with lower scores (a lower score indicates lower consumption frequency) were the following: sweets, sugary soft drinks, light soft drinks, and chips. Each component has a minimum score of 0 and a maximum score of 7, where the highest score indicates the highest possible quality of the diet.
Height was measured with a Seca® 222, and weight was measured with Seca® 661 scales (Seca, Birmingham, UK) with the children in lightweight clothing and barefoot. Body mass index (BMI) was calculated as weight divided by the square height in meters (kg/m2).
Cardiorespiratory fitness was measured using the 20-m shuttle run test. Participants were encouraged to run back and forth between two lines 20 m apart, following a sound signal that increased by 0.5 km/h each minute. Participants failed the test when they did not reach the lines before the signal sounded twice. Maximal oxygen intake (VO2 max) was calculated by applying the Léger formula (Léger et al. 1988).
Socioeconomic status was assessed by using a validated questionnaire (Domingo-Salvany et al. 2000), completed by both parents, about education level and occupation. Mother’s education was used as a covariate, as several authors have pointed out that it is one of the main determinants of AA (Chen 2004). Maternal education level was the maximum level of education achieved by the mother and was categorized as follows: (1) no studies; (2) primary studies; (3) high school studies; and (4) university studies.
Statistical analysis
To examine the normal distribution of continuous variables, graphical (normal probability plots) and statistical (Kolmogorov–Smirnov test) methods were. All continuous variables fit well within a normal distribution. Exploration of outlier values was performed. After that, data were winsorized using the 1st and 99th percentiles of the distribution of variables. The chi-squared test (categorical variables) or Student’s t test (continuous variables) was used to analyze the descriptive characteristics of the study sample by meeting the screen time guidelines categories (American Academy of Pediatrics 2021).
Bivariate Pearson correlation coefficients were used to examine the associations between variables. ANCOVA models were used to test mean differences in AA, executive functions, and diet components as dependent variables by screen media use categories (TV viewing/other electronic devices) (<2 h/day, 2-3 h/day, and >3 h/day). The results are shown unadjusted in model 0 and controlling for sex, age, BMI, cardiorespiratory fitness (VO2 max) and maternal education in model 1. Pairwise post hoc hypotheses were tested using the Bonferroni correction for multiple comparisons.
To determine whether diet quality acts as a mediator in the relationship between screen media use (TV viewing/other electronic devices) and AA (in language and mathematics) we performed mediation analyses following Baron and Kenny (1986) criteria. Those authors establish four criteria that should be met to consider a mediation analysis: (1) a change in levels of the exposure variable affects changes in the outcome; (2) a change in exposure variable affects the changes in mediator; (3) there is a significant relationship between mediator and the outcome; (4) when the previous paths are controlled, a previously significant relation between the exposure and outcome is no longer significant. When any of these conditions is not met, the mediation analysis stops (Baron and Kenny 1986). In this sense, executive functions were not included in the mediation analysis since the independent variable and the mediator were not associated with executive functions, so the first and third Baron and Kenny’s criteria were not met. For these analyses, we used PROCESS SPSS macro version 3.1, selecting Model 4 and 5.000 bias-corrected bootstrap samples (Hayes 2013).
Path “a” represents regression coefficients of diet quality on screen media use; coefficient “c” (total effect), the regression of AA on screen media use; and coefficient “b,” the regression of AA on diet quality. Path “c” (direct effect) represents the regression coefficient of AA on screen media use after controlling for the mediating variable. Based on a previous literature review to identify the most important confounders, mediation models were controlled using sex, age, BMI, cardiorespiratory fitness (VO2max), maternal education level, and executive function as covariates, as these are variables that have been shown in previous studies to be associated with the study variables (Shi et al. 2022; Wu et al. 2022). To test the statistical significance, the bootstrap confidence interval method was used. Indirect effects were considered significant when the confidence interval (95%) was not zero.
The statistical significance was set at p <.05. Statistical analyses were performed using IBM SPSS Statistics v.24 0 (IBM Corp., Armonk, NY, USA).
Results
Descriptive characteristics are presented in Table 1. Children who did not meet the screen time recommendations had higher BMI, lower cardiorespiratory fitness, lower quality of diet, and higher consumption of junk food, such as sweets, soft drinks and beverages, chips, and fries, (p < .001). Regarding AA mean differences almost reach statistical significance (p = .071) and (p = .076) in language and mathematics, respectively; and non-significant differences were found in executive functions variables.
Table 2 shows correlation coefficients among study variables. TV viewing was negatively associated with AA in language (r = -.177; p <.001) and mathematics (r = –.181; p <.001) and with HDQI (r = –.183; p <.001). No associations were reported between TV viewing and executive functions. Screen time in other electronic devices was negatively associated with HDQI (r = –.240; p <.001). A direct and significant association was found between screen time in other electronic devices and inhibition (r = .093; p <.05). However, no significant associations were reported with AA in language, mathematics, or other executive functions.
Table 3 (model 0) shows that those children who spent >3 h/day viewing TV had significantly lower scores on language and mathematics (p <.001), worse diet profiles (ate fewer fruits and more sweets and drank more soft drinks (p <.001)) and scored lower on the HDQI (p <.001). No differences in mean academic grades were found by categories of “mean time using electronic devices,” but those children who spent >3 h using these devices had better inhibition levels (p <.021) and worse HDQI (p <.001) than their peers belonging to the lowest category (<2 h). These differences, except for inhibition, were maintained after controlling for sex, age, BMI, cardiorespiratory fitness, and maternal education level (model 1).
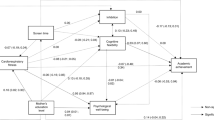
Figure 1 shows the mediation analyses assessing whether the association between screen time behaviors and AA was mediated by HDQI. In the first regression step (path a), both types of screen time were negatively associated with HDQI (p <.001), indicating that higher amounts of time spent in screen time activities were associated with lower HDQI. The HDQI (path b) was positively associated with achievement in language and mathematics (p <.001) in all the mediation models, indicating that higher HDQI was associated with better AA in both language and mathematics. Thus, the significant paths were the following: TV viewing was associated with HDQI with AA in language [IE = –0.025; 95% CI (–0.036; –0.014)]; TV viewing was also associated with HDQI, and HDQI with AA in mathematics [IE = –0.025; 95% CI (–0.037; –0.015)]. Regarding screen time in other electronic devices, it was also associated with HDQI, and HDQI with AA in language [IE = –0.033; 95% CI (–0.047; –0.020)]; and screen time in other electronic devices was associated with HDQI, and HDQI with AA in mathematics [IE = –0.035; 95% CI (–0.049; –0.022)]. In Fig. 1a and b, TV viewing showed a negative and significant total effect (path c), which was attenuated while introducing HDQI into the model (path c’), indicating a partial mediation (p <.001). Regarding time spent in other electronic devices, the mediated effect (a x b), X on Y through M, was significant; in language path c, it was significant and when the mediator was entered in the model the significance disappeared (c’) indicating a full mediation; however, no direct or total effects were significant between other electronic devices and mathematics, indicating indirect-only mediation (Zhao et al. 2010), see Fig. 1c and d.

Mediation between screen time (TV and other electronic devices) and academic achievement through health dietary quality index (HDQI), controlling for gender, age, body mass index, cardiorespiratory fitness, maternal education, and executive function. Note. Path a, association between independent variable and mediators; path b, association between mediator and dependent variables; path c, total effect between independent and dependent variables; path c’, direct effect of independent variable on dependent variable. EDs = other electronic devices; IE indirect effect (95% confidence interval); PM percentage of mediation. *p < 0.05 **p < 0.001
Discussion
This study analyzed the associations of two screen-related behaviors (TV viewing and time spent using other electronic devices) with diet, cognition, and AA and examined whether diet quality mediates the relationship between these screen behaviors and AA. Our analyses confirm that both types of screen-related behaviors have detrimental effects on dietary habits, so that children who spend more time watching TV or with other electronic devices have lower quality of diet. Moreover, diet quality mediated the association between TV viewing and other electronic devices with AA (academic grades in mathematics and language); however, between screen time on electronic devices with AA in mathematics only an indirect association through diet quality was observed.
Studies analyzing the relationship between screen time and AA show mixed results (Adelantado-Renau et al. 2019; Walsh et al. 2020; García-Hermoso and Marina 2017; Syväoja et al. 2018). In our study, passive screen time (TV viewing) was associated with lower AA in mathematics and language, such that children who spent >3 h watching TV had a lower AA. Several mechanisms could explain the detrimental effect of TV viewing on AA: the time-displacement hypothesis (Kostyrka-Allchorne et al. 2017) proposes that TV viewing replaces activities such as socializing, homework, physical activity, or sleeping; or the passivity hypothesis (Shin 2004). Moreover, TV viewing has been shown to decrease attention and cognition (Horowitz-Kraus and Hutton 2018; Nathanson et al. 2014; Takeuchi et al. 2015; Walsh et al. 2020) and to increase behavioral problems and unhealthy habits (Kostyrka-Allchorne et al. 2017; Shin 2004). Last, a study found that TV viewing affected the gray matter volume of the frontopolar cortex and that this was associated with impaired verbal abilities (Takeuchi et al. 2015).
In contrast, our data in the mediation analysis support that the time spent using other display devices was associated with lower AA in language but not directly associated with AA in mathematics. Additionally, we have also shown a direct and significant association between screen time in other electronic devices and inhibition (r = .093; p <.05). According to a previous study (Walsh et al. 2020), children who spend >3 h/day using other electronic devices scored higher in the inhibition dimension of executive functions. In our study, this effect disappeared with further adjustments. A recent study showed that videogaming and active screen uses that challenge executive functions may benefit top-down cognitive processes (Diamond and Lee 2011) and may induce brain plasticity tied to cognitive functions (Kühn et al. 2014), which are related to AA (Chaddock et al. 2011). Similarly, another study suggested that video game playing is linked with structural alterations indicative of maturation and specialization in brain areas tied to executive functions (Paulus et al. 2019). Finally, some research has suggested that children’s metabolic and physiological responses to active screen uses are different from the time spent watching TV (Wang and Perry 2006), such that energy expenditure during video game play is significantly higher than that expended during TV viewing (Sweetser et al. 2012). Additionally, some video games actively promote increased physical activity (Graves et al. 2008). This positive effect of some screen use on executive functions could mitigate the association between screen time using other electronic devices and academic performance in mathematics, as performance in this subject is strongly related to executive functions (Bull and Lee 2014).
Regarding executive functions, previous studies have found significant inverse effects of screen time on executive functions and AA (Adelantado-Renau et al. 2019; Horowitz-Kraus and Hutton 2018; Takeuchi et al. 2015). However, in our study, no significant differences were observed in the mean of executive functions by categories of screen time. These results may suggest two facts: one, that the negative relationship between screen use and academic performance would occur because children use more electronic devices, thus reducing their study time, which translates into poorer academic performance, and not because the use of electronic devices has a direct negative influence on their cognitive performance. And second, that the relationship between screen time and cognition may not be direct or occur more in the long term. Additionally, these null results highlight the importance of considering screen time as a complex variable, so it is important to consider what use is being made of the screen, what apps are being used, if they are cognitive demandant or not, among others. In this line, some specific screen time activities might be associated with improvements in executive function, such as educational games or exergames (Choi et al. 2020; Özçetin et al. 2019; López et al. 2021). Thus, more research is needed to discern the effect on specific cognitive domains of different types of screen time behavior.
Our findings highlight the mediating role of diet quality on the associations between screen time and AA. Both types of screen time were associated with higher consumption of sweets, chips, and soft drinks, lower consumption of fruit and fish, and lower dietary quality. Similarly, a previous review found a significant relationship between screen time and all adverse dietary outcomes (Shqair et al. 2019). One of the most compelling arguments for the link between electronic media use and food consumption is commercial advertising. Fast food is heavily promoted in media, and children’s exposure to TV shapes their preferences toward advertised foods (Emond et al. 2021) to the detriment of typical, self-regulation of food intake (Braude and Stevenson 2014).
Similarly, previous studies found associations between dietary intake and AA, especially breakfast, global dietary quality patterns and negative associations with junk food consumption (Burrows et al. 2017) and that low consumption of fish, fruits, and high-fat fast foods were linked with poor cognition and AA (Vassiloudis et al. 2014; Naveed et al. 2020). Among the hypothetical mechanisms of influence of diet on AA, the effect of diet on physical growth and other health conditions (Naveed et al. 2020) are mechanisms associated with neurodevelopmental processes that occur during childhood (Prado and Dewey 2014).
Strengths and limitations
The strengths of this study include the large sample size; the consideration of different dimensions of screen time behaviour; and that it is the first study to analyse in a combined model the effect of two different types of screen use, the quality of the diet, and its impact on AA, controlling for the most significant covariates reported in the literature. However, some limitations must be considered. First, due to the study’s design, we were unable to ascertain causal relationships among study variables or directionality. However, the temporality in the direction of the diagrams proposed in our study is consistently endorsed by the availability of theoretical knowledge and previous studies. Therefore, further longitudinal, and experimental studies are recommended to confirm this hypothesis. Second, although the assessment of screen time differentiated TV viewing from other electronic devices (tablets, computers, or smartphones), we did not gather information about the different uses of screens, such as video gaming, social networks, or academics. Moreover, other sedentary behaviors that may positively influence AA, such as reading or drawing, were not considered. Third, because screen time and diet are self-reported measurements, our analyses are not free of potential biases such as social desirability bias and recall bias that threaten the accuracy of our data. Finally, some authors have suggested that the effect of diet on AA may have direct and indirect paths, as well as synergistic effects with other behaviors such as physical activity or sleep.
Conclusions
These results suggest that children who spent >3 h per day on screen time make poorer food choices, which, in turn, are associated with worse AA. Our results confirm the pivotal role of diet quality in the relationship between screen time and AA, differentiating between TV time and time using other electronic devices. Moreover, our data suggest that both screen-related behaviors are associated with an unhealthy diet and therefore support the implementation of public health interventions aimed at preventing these negative influences. Further studies with longitudinal and experimental designs, considering several types of screen time, are recommended.
Data availability
[Dataset] Visier-Alfonso, María Eugenia (2021). Screen, Mendeley Data, V1, https://doi.org/10.17632/8bshtfjw97.1.
References
Adelantado-Renau M, Moliner-Urdiales D, Cavero-Redondo I, Beltran-Valls MR, Martínez-Vizcaíno V, Álvarez-Bueno C (2019) Association between screen media use and academic performance among children and adolescents: a systematic review and meta-analysis. JAMA Pediatr 173:1058–1067. https://doi.org/10.1001/jamapediatrics.2019.3176
American Academy of Pediatrics (2021) Media and children [Retrieved from] https://www.aap.org/en/patient-care/media-and-children/. Accessed 23 May 2023
Arvidsson L, Eiben G, Hunsberger M et al (2017) Bidirectional associations between psychosocial well-being and adherence to healthy dietary guidelines in European children: prospective findings from the IDEFICS study. BMC Public Health 17:926. https://doi.org/10.1186/s12889-017-4920-5
Baron RM, Kenny DA (1896) The moderator–mediator variable distinction in social psychologicalresearch: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol 51(6):1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
Braude L, Stevenson RJ (2014) Watching television while eating increases energy intake. Examining the mechanisms in female participants. Appetite 76:9–16. https://doi.org/10.1016/j.appet.2014.01.005
Bull R, Lee K (2014) Executive functioning and mathematics achievement. Child Dev Perspect 8:36–41. https://doi.org/10.1111/cdep.12059
Burrows T, Goldman S, Pursey K, Lim R (2017) Is there an association between dietary intake and academic achievement: a systematic review. J Hum Nutr Diet 30:117–140. https://doi.org/10.1111/jhn.12407
Cartanyà-Hueso À, González-Marrón A, Lidón-Moyano C, Garcia-Palomo E, Martín-Sánchez JC, Martínez-Sánchez JM (2021) Association between leisure screen time and junk food intake in a nationwide representative sample of spanish children (1-14 Years): a cross-sectional study. Healthcare (Basel) 9:228. https://doi.org/10.3390/healthcare9020228
Chaddock L, Hillman CH, Buck SM, Cohen NJ (2011) Aerobic fitness and executive control of relational memory in preadolescent children. Med Sci Sports Exerc 43:344–349. https://doi.org/10.1249/MSS.0b013e3181e9af48
Chen E (2004) Why socioeconomic status affects the health of children: a psychosocial perspective. Curr Dir Psychol Sci 13:112–115. https://doi.org/10.1111/j.0963-7214.2004.00286.x
Choi E, Shin SH, Ryu JK, Jung KI, Kim SY, Park MH (2020) Commercial video games and cognitive functions: Video game genres and modulating factors of cognitive enhancement. Behav Brain Funct 16. https://doi.org/10.1186/s12993-020-0165-z
Costigan SA, Barnett L, Plotnikoff RC, Lubans DR (2013) The health indicators associated with screen-based sedentary behavior among adolescent girls: a systematic review. J Adolesc Health 52:382–392. https://doi.org/10.1016/j.jadohealth.2012.07.018
Diamond A, Lee K (2011) Interventions shown to aid executive function development in children 4 to 12 years old. Science 333(6045):959–964. https://doi.org/10.1126/science.1204529
Domingo-Salvany A, Regidor E, Alonso J et al (2000) Una propuesta de medida de la clase social. Aten Prim 25:350–363. https://doi.org/10.1016/S0212-6567(00)78518-0
Emond JA, Utter H, Eschholz A, Chang V, Gottlieb MA, Sargent JD (2021) Promotion of meal premiums in child-directed tv advertising for children’s fast-food meals. Pediatrics 147. https://doi.org/10.1542/peds.2020-042994
Faught EL, Ekwaru JP, Gleddie D, Storey KE, Asbridge M, Veugelers PJ (2017) The combined impact of diet, physical activity, sleep and screen time on academic achievement: a prospective study of elementary school students in Nova Scotia. Canada Int J Behav Nutr Phys Act 14:29. https://doi.org/10.1186/s12966-017-0476-0
Faught EL, Qian W, Carson VL, Storey KE, Faulkner G, Veugelers PJ, Leatherdale ST (2019) The longitudinal impact of diet, physical activity, sleep, and screen time on Canadian adolescents’ academic achievement: an analysis from the COMPASS study. Prev Med 125:24–31. https://doi.org/10.1016/j.ypmed.2019.05.007
García-Hermoso A, Marina R (2017) Relationship of weight status, physical activity and screen time with academic achievement in adolescents. Obes Res Clin Pract 11:44–50. https://doi.org/10.1016/j.orcp.2015.07.006
Graves LEF, Ridgers ND, Stratton G (2008) The contribution of upper limb and total body movement to adolescents’ energy expenditure whilst playing Nintendo Wii. Eur J Appl Physiol 104:617. https://doi.org/10.1007/s00421-008-0813-8
Hayes AF (2013) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach The Guilford Press, New York. https://onlinelibrary.wiley.com/doi/abs/10.1111/jedm.12050. Accessed 23 May 2023
Hong SB, Zalesky A, Cocchi L et al (2013) Decreased functional brain connectivity in adolescents with internet addiction. PloS one 8:e57831. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0057831. Accessed 23 May 2023
Horowitz-Kraus T, Hutton JS (2018) Brain connectivity in children is increased by the time they spend reading books and decreased by the length of exposure to screen-based media. Acta Paediatr 107:685–693. https://doi.org/10.1111/apa.14176
Kostyrka-Allchorne K, Cooper NR, Simpson A (2017) The relationship between television exposure and children’s cognition and behaviour: a systematic review. Deve Rev 44:19–58. https://doi.org/10.1016/j.dr.2016.12.002
Kühn S, Gleich T, Lorenz RC, Lindenberger U, Gallinat J (2014) Playing Super Mario induces structural brain plasticity: gray matter changes resulting from training with a commercial video game. Mol Psychiat 19:265–271. https://doi.org/10.1038/mp.2013.120
Lanfer A, Hebestreit A, Ahrens W et al (2011) Reproducibility of food consumption frequencies derived from the Children’s Eating Habits Questionnaire used in the IDEFICS study. Int J Obes 35:61–68. https://doi.org/10.1038/ijo.2011.36
Lee H, Cashin AG, Lamb SE et al (2021) A guideline for reporting mediation analyses of randomized trials and observational studies: the AGReMA statement. JAMA 326:1045–1056. https://doi.org/10.1001/jama.2021.14075
Léger LA, Mercier D, Gadoury C, Lambert J (1988) The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci 6(2):93–101. https://doi.org/10.1080/02640418808729800
López SL, Ruiz A, de la Torre MDL, Martínez EJM (2021) Improving cognition in school children and adolescents through exergames. A systematic review and practical guide. S Afr J Educ 41. https://www.ajol.info/index.php/saje/article/view/205732. Accessed 23 May 2023
Martínez-Vizcaíno V, Álvarez-Bueno C, Cavero-Redondo I et al (2019) MOVI-daFIT! Intervention: rationale and design of a cluster randomized controlled trial testing the effects on improving adiposity, cognition, and subclinical atherosclerosis by increasing cardiorespiratory fitness in children. Medicine (Baltimore) 98(9):e14737
Nathanson AI, Aladé F, Sharp ML, Rasmussen EE, Christy K (2014) The relation between television exposure and executive function among preschoolers. Dev Psychol 50:1497–1506. https://doi.org/10.1037/a0035714
Naveed S, Lakka T, Haapala EA (2020) An overview on the associations between health behaviors and brain health in children and adolescents with special reference to diet quality. Int J Environ Res Public Health 17. https://doi.org/10.3390/ijerph17030953
Özçetin M, Gümüştaş F, Çağ Y, Gökbay İZ, Özmel A (2019) The relationships between video game experience and cognitive abilities in adolescents. Neuropsychiatri Dis Treat 15:1171–1180. https://doi.org/10.2147/NDT.S206271
Page AS, Cooper AR, Griew P, Jago R (2010) Children’s screen viewing is related to psychological difficulties irrespective of physical activity. Pediatrics 126:e1011–e1017. https://doi.org/10.1542/peds.2010-1154
Paulus MP, Squeglia LM, Bagot K et al (2019) Screen media activity and brain structure in youth: Evidence for diverse structural correlation networks from the ABCD study. NeuroImage 185:140–153. https://doi.org/10.1016/j.neuroimage.2018.10.040
Prado EL, Dewey KG (2014) Nutrition and brain development in early life. Nutr Rev 72:267–284. https://doi.org/10.1111/nure.12102
Saunders TJ, Vallance JK (2017) Screen time and health indicators among children and youth: current evidence, limitations and future directions. Appl Health Econ Health Policy 15:323–331. https://doi.org/10.1007/s40258-016-0289-3
Shang L, Wang J, O’Loughlin J, Tremblay A, Mathieu MÈ, Henderson M, Gray-Donald K (2015) Screen time is associated with dietary intake in overweight Canadian children. Prev Med Rep 2:265–269. https://doi.org/10.1016/j.pmedr.2015.04.003
Sharif I, Wills TA, Sargent JD (2010) Effect of visual media use on school performance: a prospective study. J Adolesc Health 46:52–61. https://doi.org/10.1016/j.jadohealth.2009.05.012
Shi Y, Yu H, Di S, Ma C (2022) Body mass index and academic achievement among chinese secondary school students: the mediating effect of inhibitory control and the moderating effect of social support. Front Psychol 13:835171. https://doi.org/10.3389/fpsyg.2022.835171
Shin N (2004) Exploring pathways from television viewing to academic achievement in school age children. J Genet Psychol 165:367–382. https://doi.org/10.3200/GNTP.165.4.367-382
Shqair AQ, Pauli LA, Costa VPP, Cenci M, Goettems ML (2019) Screen time, dietary patterns and intake of potentially cariogenic food in children: A systematic review. J Dent 86:17–26. https://doi.org/10.1016/j.jdent.2019.06.004
Strasburger VC, Hogan MJ, Mulligan DA et al (2013) Children, adolescents, and the media. Pediatrics 132:958–961. https://doi.org/10.1542/peds.2013-2656
Suggate SP, Martzog P (2020) Screen-time influences children’s mental imagery performance. Dev Sci 23:e12978. https://doi.org/10.1111/desc.12978
Sweetser P, Johnson D, Ozdowska A, Wyeth P (2012) Active versus passive screen time for young children. Australas J Early Child 37:94–98. https://doi.org/10.1177/183693911203700413
Syväoja HJ, Kankaanpää A, Kallio J et al (2018) The relation of physical activity, sedentary behaviors, and academic achievement is mediated by fitness and bedtime. J Phys Act Health 15:135–143. https://doi.org/10.1123/jpah.2017-0135
Takeuchi H, Taki Y, Hashizume H et al (2015) The impact of television viewing on brain structures: cross-sectional and longitudinal analyses. Cereb Cortex 25:1188–1197. https://doi.org/10.1093/cercor/bht315
Thomas G, Bennie JA, De Cocker K, Castro O, Biddle SJH (2020) A descriptive epidemiology of screen-based devices by children and adolescents: a scoping review of 130 Surveillance Studies Since. Child Indic Res 13:935–950. https://doi.org/10.1007/s12187-019-09663-1
Tremblay MS, LeBlanc AG, Janssen I, Kho ME, Hicks A, Murumets K, Colley RC, Duggan M (2011) Canadian sedentary behaviour guidelines for children and youth. Appl Physiol Nutr Metab 36:59–64. https://doi.org/10.1139/H11-012
Tulsky DS, Carlozzi N, Chevalier N, Espy K, Beaumont J, Mungas D (2013) NIH Toolbox cognitive function battery (NIHTB-CFB): measuring working memory. Monogr Soc Res Child Dev 78:70–87. https://doi.org/10.1111/mono.12035
Vassiloudis I, Yiannakouris N, Panagiotakos DB, Apostolopoulos K, Costarelli V (2014) Academic performance in relation to adherence to the Mediterranean diet and energy balance behaviors in Greek primary schoolchildren. J Nutr Educ Behav 46:164–170. https://doi.org/10.1016/j.jneb.2013.11.001
Walsh JJ, Barnes JD, Tremblay MS, Chaput JP (2020) Associations between duration and type of electronic screen use and cognition in US children Comput. Hum Behav 108:106312. https://doi.org/10.1016/j.chb.2020.106312
Wang X, Perry AC (2006) Metabolic and physiologic responses to video game play in 7- to 10-year-old boys. Arch Pediatr Adolesc Med 160:411. https://doi.org/10.1001/archpedi.160.4.411
Wärnberg J, Pérez-Farinós N, Benavente-Marín JC et al (2021) Screen time and parents’ education level are associated with poor adherence to the mediterranean diet in Spanish children and adolescents: the PASOS study. J Clin Med 10:795. https://doi.org/10.3390/jcm10040795
Weintraub S, Bauer PJ, Zelazo PD, Wallner-Allen K, Dikmen SS, Heaton et al (2013) I. NIH Toolbox cognition battery (cb): introduction and pediatric data: NIH Toolbox cognition battery (CB). Monogr Soc Res Child Dev 78(4):1–15. https://doi.org/10.1111/mono.12031
Wu XY, Han LH, Zhang JH, Luo S, Hu JW, Sun K (2017) The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLOS ONE 12:e0187668. https://doi.org/10.1371/journal.pone.0187668
Wu Y, Amirfakhraei A, Ebrahimzadeh F, Jahangiry L, Abbasalizad-Farhangi M (2022) Screen time and body mass index among children and adolescents: a systematic review and meta-analysis. Front Pediatr 10:822108. https://doi.org/10.3389/fped.2022.822108
Zelazo PD, Anderson JE, Richler J, Wallner-Allen K, Beaumont JL, Weintraub S (2013) II. NIH Toolbox Cognition Battery (CB): Measuring executive function and attention: NIH Toolbox cognition battery (CB). Monogr Soc Res Child Dev 78:16–33. https://doi.org/10.1111/mono.12032
Zhao X, Lynch JG, Chen Q (2010) Reconsidering Baron and Kenny: myths and truths about mediation analysis. J consum res 37:197–206. https://doi.org/10.1086/651257
Funding
This work was supported by the Ministry of Economy and Competitiveness-Carlos III Health Institute and FEDER funds [grant number FIS PI19/01919]; the Research Network on Preventative Activities and Health Promotion [grant number RD12/0005/0009].
The study sponsor had no role in the study design, data collection, analysis, or interpretation.
The authors have no financial relationships relevant to this article to disclosure.
Author information
Authors and Affiliations
Contributions
Conceptualization: Vicente Martínez-Vizcaíno; Methodology: Mairena Sánchez-López, Celia Álvarez-Bueno; Formal Analysis and investigation: María Eugenia Visier-Alfonso; Miriam Garrido-Miguel; Writing-original draft preparation: María Eugenia Visier-Alfonso; Writing - review and editing: Miriam Garrido-Miguel, Celia Álvarez-Bueno, Montserrat Hernández-Luengo; Funding acquisition: Mairena Sánchez-López, Vicente Martínez-Vizcaíno; Resources: Mairena Sánchez-López; Supervision: Vicente Martínez-Vizcaíno
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The present study was approved by the Clinical Research Ethics Committee of the Virgen de la Luz Hospital in Cuenca (REG: 2016/PI021) and by the Board of Governors of each school.
Consent to participate
Parents were invited to an informative meeting and provided written consent. Children were asked to provide verbal consent prior to the completion of each test. All participants were informed and consented to participate in the study; additionally, they were informed and consented to having their data published anonymously.
Conflicts of interest
The authors have indicated they have no potential conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 180 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Visier-Alfonso, M.E., Garrido-Miguel, M., Álvarez-Bueno, C. et al. Influence of screen time on diet quality and academic achievement: a mediation analysis. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-02125-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-02125-7