
Abstract
Purpose
The burden of health and safety related issues emanating from the modern workplace is overwhelming. Although the prevailing statistics found in the literature show that victims of workplace fatalities and injuries are higher in developing countries and transition economies, there is a very limited understanding of the causal factors that may correspond to the continuous increase in the occupational exposure of employees to various fatalities and injuries. The purpose of this study was to review the literature on occupational safety of workers with the objective of highlighting the major causal factors of workplace injuries and fatalities from a multi-regional perspective, particularly on job-contexts with highest safety and health related hazards.
Methodology
A systematic review of the literature was conducted on 73 empirical studies in the regions of Europe, Africa, the Middle East, Asia, Australia, and the Americas (the US & Canada).
Findings
The results showed that the highest number of injuries and fatalities were mostly found in the construction industry. It further emerged that most of the studies were centered in developing countries within Africa and Asia. Other results and recommendations were discussed for each region.
Value
The findings from this study have the potential to expose the regional dynamics in relation to safety in the workplace. This study also addresses the main areas of concern for stakeholders to promote organizational development and safety culture.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The extent of human engagement in various occupations has led to a rise in varying degrees of injuries and fatalities across both developed and developing nations. The migration of some industrial undertakings, in particular the manufacturing from higher-income countries to low-and-middle income countries, has intensified exposure to hazardous chemicals (Sorensen et al. 2017), and increased risks to occupational injuries and varying health impairment among workers. According to a report commissioned by the international labor organization (ILO), it is estimated that about 2.78 million deaths (Takala et al. 2017), 313 million non-fatal accident and 160 million work-related diseases occur in the workplace globally. The burden of health and safety related issues emanating from the modern workplace is overwhelming. It is estimated that about 10,000,000 occupational injuries occur annually in China (Liu et al. 2015). In the United States, thousands of death and disability cases occur due to occupational accidents annually (Christian et al. 2009). The International Labor Organization avers that most workers are at risk of various work-related injuries, fatalities, and various health challenges. For example, health issues such as pneumoconiosis, musculoskeletal disorders, and mental issues are widespread (Mrema et al. 2015).
Occupational injuries and fatalities have both social and economic costs on a nation as a whole. The economic costs of work-related injuries, fatalities, and illness have triggered a number of concerns from scholars and practitioners to the study of workplace safety (Christian et al. 2009; Friend and Kohn 2014). The majority of previous research studies have focused on accident causing mechanisms and unsafe worker behaviors (Frese and Keith 2015; Liu et al. 2016; Reason 2005; Wirth et al. 2017) in order to explain various work-related injuries and fatalities. Despite this, no clear picture has emerged to show how certain factors of unsafe worker behaviors can contribute to injuries and fatalities in a job specific context such as construction, healthcare, energy, and other domains.
Most countries and industries face a common challenge of managing safety and health of workers. This can be attributed to the fact that most work related accidents and fatalities have an immediate effect on workers which require efficient safety management practices to curb them (Fugas et al. 2012; Takala et al. 2014). As such, producing knowledge that highlights areas of concern can be a key for ensuring effective safety management practices. Many researchers have dwelt on safety climate measures as a means of modeling safety behavior of workers (Fogarty et al. 2017; Neal and Griffin 2002, 2006; Sullman et al. 2017; Zohar 2010; Zohar and Luria 2005). In addition, safety-maturity models have been utilized in high-hazard industries in an attempt to reduce certain work-related injuries and fatalities (Foster and Hoult 2013; Hudson 2007; Parker et al. 2006). Most previous studies on occupational safety and health were successful in reducing workplace incidents through systems re-engineering and organizational safety culture modifications. However, work-related injuries and fatalities continue to occur in various workplaces. This warrants a detailed examination of specific factors influencing the recurring cases of occupational injuries and fatalities.
Although previous systematic reviews have attempted to describe associated factors of workplace-related injuries and fatalities, very few studies provided a comprehensive review with focus on varied jobs in a region-specific context. For example, Manu et al. (2012) provided important guidelines for identifying accident trajectories in the construction industry. In addition, Khanzode et al. (2012) mapped out an accident causation model and series of events that may contribute to workplace accidents. However, there is a need for further review that expands insight to cover causal factors specific to different industries across regions. Thus, we are of the view that understanding the contextual factors that leads to injuries and fatalities in a specific region is very critical in the drive toward the reduction/elimination of workplace injuries and fatalities. With this in mind, the current study aims to review previous studies on injuries and fatalities in the workplace with the objective of highlighting the major factors in a region-specific manner, particularly on job-contexts with the highest safety and health related hazards. It is assumed that outcomes from this review will expose the regional dynamics in relation to safety in the workplace, as well as underscore the critical areas for concern by stakeholders. Hence, this study seeks to describe the causal factors of injuries and fatalities in the workplace from a multi-regional perspective.
Our review was guided by one research question: “What are the key factors leading to workplace injuries and fatalities in a region-specific context?” To answer this question, we used search and data extraction strategies similar to those of previous reviews (e.g., Lamontagne et al. 2007; Schultz and Edington 2007). The review of major injuries and fatalities was classified to cover regions of Europe, Africa, the Middle East, Asia, Australia, and the Americas(the US & Canada). The reason for this classification is because of differences in work conditions, technologies, local circumstances, and quality or presence of supervisions. Furthermore, categorizing injuries and fatalities factors across these regions may reveal important differences and clues to the organizational role into which the practice of certain safety policies and awareness may grow. In addition, differences in safety practices to reduce the risk of injuries and fatalities are of concern to workers and employees.
Method
We conducted a systematic review of empirical studies on factors influencing occupational injuries and fatalities among workers within the domain of occupational safety and health research. Previous studies that employed both primary (original/empirical) and secondary data (Searcy and Mentzer 2003), published in peer-reviewed journals and conference proceedings, were considered for selection. To ensure that the existing body of knowledge about factors that influence injuries and fatalities were carefully identified for further evaluation, we followed well-established frameworks for conducting review studies (Fisch and Block 2018; Moher et al. 2009).
Search strategy and data source
A comprehensive search of electronic databases was performed to identify relevant articles. For this study, we selected the following keywords for the search: “factors” OR “causes” AND “influence” AND “injuries” OR “fatalities” OR “incidents” OR “accidents” AND “workplace” OR, “employee’s safety” AND “behavior,” OR “organizational safety AND injuries” OR, “factors influencing workers’/employees’ safety,” and “safety factors in job.” These keywords were entered into prominent academic databases, including Google Scholar, Scopus, Web of Science, Elsevier, ProQuest, Emerald, and Springer. The databases were searched for citations with no starting date limitation.
Inclusion criteria
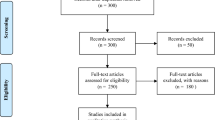
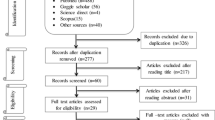
The following boundary conditions guided the search strategy and inclusion of previous studies for this review: (a) only empirical peer reviewed research on factors influencing injuries and fatalities among workers; (b) papers published in English; and (c) published papers from 1998 to 2020. Some of the papers were more central and useful than others. Our initial search led to the identification of 1500 studies. We screened these papers for potential duplicates. All titles and abstracts similar or related to the search keywords were screened and included for further evaluation. The screening of titles and abstracts yielded 300 studies that were found to meet the eligibility criteria for further evaluation. The evaluation of the studies was conducted bearing in mind the objective and the methodological paradigm adopted in this study. After the exclusion of duplicates, 250 full-text eligible articles were reviewed. Systematic review papers, meta-analysis studies, theoretical and conceptual articles, and non-peer reviewed research reports were excluded from this review. Some studies dealing with unspecified work conditions as well as not typically studied certain safety aspects were also excluded. Consequently, 73 peer reviewed empirical studies were identified and used in this review (see Fig. 1).

The PRISMA flow diagram for article searching and selection process
Assessment protocol
The 73 studies were carefully reviewed to identify the factors that influence injuries and fatalities among workers in different workplace settings. Two reviewers were asked to code each paper on the basis of originality, methodological soundness, the interpretation of the results, and their relevance to this review. They then met to discuss and to reach an agreement on any differences in coding. The interrater agreement (using intra-class correlation coefficient and its 95% confidence interval) between the experts was assessed. The overall quality of the 73 studies was scored from 1 to 3, low-high) based on: (1) appropriateness of the method, (2) relevance to focus of this review, and (3) whether the findings are credible and valid. We measured the weight of each study by summing scores on each of the three dimensions. The inter-rater reliability (r) for the three dimensions between the two experts ranged from 0.83 to 0.91.
Due to the heterogeneity of the 73 studies (e.g., job contexts, workplace settings, and safety measures), we agreed to code the factors identified according to countries and job contexts (e.g., healthcare, mining, manufacturing, construction, corporate, energy, and agriculture). A further synthesis of the identified job-contexts was performed to classify similar jobs into one job-domain. For example, studies based on oil and gas, petroleum drilling, and electricity generation plants were classified as energy industry. This was based on the description of Sovacool and Mukherjee (2011) who reported that the energy sector may include electricity supply, nuclear power, oil, and gas. Studies based on production of goods and services (e.g., home-based enterprises, wood-workers, artisans, welders, sprayers, mechanics, and rural transport services) on small-scale were categorized as small and medium-sized enterprises (SMEs). This was based on the International Labor Organization’s (ILO) description of such entrepreneurial undertakings, as cited in Dodoo and Al-Samarraie (2019). Further, we classified studies that dealt with banking, media houses, and administrative jobs as corporate sector. The foregoing process enabled us to identify multi-regional factors that were associated with injuries and fatalities in different workplace settings.
Results
In order to identify the key factors contributing to workplace injuries and fatalities and their relative outcomes, we categorized the findings based on the context domains and regions (see Table 1). The regional categorization includes: Europe (15%), Africa (31.5%), the Middle East (8.2%), Asia (27.4%), Australia (4%), and the Americas (the US & Canada) (13.8%). Figure 2 provides an illustration of the distribution of previous studies on factors leading to occupational injuries and fatalities across countries.

Distribution of studies on factors leading to occupational injuries and fatalities worldwide
Europe
In Europe, we reviewed previous studies in an attempt to identify causes of injuries and fatalities in the workplace from countries such as the United Kingdom, Spain, Italy, Ireland, Sweden, Netherland, Norway, and Denmark. The study found a substantial number of empirical studies in the healthcare sector and manufacturing industry, followed by construction industry, corporate sector, and the petrochemical industry. It was inferred from the previous studies that the leading contributory factors of healthcare-related injuries were mostly induced by the work environment and emotional state of workers. Factors such as violence and abuse from patients (Angland et al. 2014; Ramacciati et al. 2015) were mostly experienced by nurses, particularly those working in the triage areas, stress from high job demand and job insecurity (Bronkhorst 2015). These factors negatively influenced the emotional and mental state of workers by making them feel vulnerable. By implication, it appears that there is a need for concrete measures to address the environmental factors such as long waiting time. Andersen et al. (2019) investigated back injury risk factors among healthcare workers. The authors found that certain causal factors experienced by workers can be due to patient transfer and lack of psychosocial support. However, lack of critical assistive devices (e.g., sliding sheets, intelligent beds, walking aids, and ceiling lifts) and poor task coordination among co-workers may also contribute to workers’ back-injury cases.
Furthermore, our review of studies on the manufacturing industry revealed that factors related to safety culture can be the main causes of injuries and fatalities among workers. According to Nordlöf et al. (2015), practices such as constant tradeoffs, non-compliance with safety procedure, risky co-worker behaviors and low management commitment to safety were identified as factors that potentially led to injuries among workers. This was mostly attributed to work-related pressure such as meeting targets and deadlines. We also found that the storage of equipment and materials in unsuitable areas and prolonged work hours can potentially affect the safety and health of workers. This practice was largely blamed on the lack of adequate working space, poor monitoring/supervision, and lack of understanding the associated risks of behavior (Baldissone et al. 2019). Due to extended periods of work and non-compliance of working cycle, workers are forced to work in non-ergonomic positions that contribute to injuries and other health impairments.
Our review of previous studies on the construction industry showed the role of risk-taking behaviors and lapses with safety supervision in increasing injuries and fatalities among workers. The majority of injury and fatality cases were also found to be attributed to workers’ low perceptions of risk and its consequences. This includes aspects such as driving with obstructed visibility, unnecessary risk-taking, non-use of safety equipment, staying in danger zone, skipping a phase in the sequence of operation, and lack of communication between co-workers (Bohm and Harris 2010; Winge et al. 2019). In addition, our review showed that the lack of appropriate skills for handling machines and lapses with supervision (e.g., inability of control unsafe conditions and actions) can result in unsafe practices that potentially induced injuries among workers (Winge et al. 2019).
Within the corporate sector, most of the previous studies emphasized the role of stress, mental strain, and work pressure in increasing injuries and various health risks among workers (Carter et al. 2013). The corporate sector is often perceived as a risk-free environment in relation to direct injuries resulting from a job. However, workers in this sector experience various psychosocial conditions such as stress, musculoskeletal disorders, and other health risks, which often manifest after a long period of time. We found that work pressure and workload can force employees to work in non-ergonomic conditions. In addition, insufficient break to refresh and long working hours were found to contribute almost equally to physical, mental, and emotional exhaustion among workers. We are of the view that more attention could be placed on informing management and workers about the hazards associated with the job, its effects on their safety and health, and the need for comprehensive measures to mitigate these hazards.
In the energy industry, previous studies (Kvalheim and Dahl 2016) have attributed work pressure as the major factor that led to injuries and fatalities among workers. In the mining industry, the literature showed that factors such as non-compliance safety procedures and non-use of personal protective clothing (Sanmiquel et al. 2010) were the main unsafe practices that led to injuries among workers. In sum, the efficacy of any safety and health system should rest largely on individual workers. Therefore, sensitizing workers, especially those in the construction, manufacturing, mining, and energy on cue-recognition of hazards and empowering them to report incidents, is the way forward.
Africa
In this region, we reviewed previous studies from countries such as Ethiopia, Morocco, Ghana, Togo, Nigeria, Kenya, Uganda, Tanzania, Zimbabwe, and South Africa. A substantial number of empirical studies was linked to the mining industry, followed by the healthcare sector, construction, manufacturing, SME’s, and corporate sector. Previous studies on the mining industry showed that miners’ exposure to harmful chemicals, dust, and inadequate ventilation were conditions that potentially led to several health issues, particularly respiratory disorders (Ayaaba et al. 2017). Other factors such as non-use of protective clothing, long working hours, work pressure (Boniface et al. 2013; Chimamise et al. 2013; Long et al. 2015), and lack of knowledge about risks associated with the use of harmful chemicals–particularly among artisanal and small and medium scale miners (Armah et al. 2016)–were also found to play a role in increasing injuries and accidents among miners. However, in other previous studies excessive noise levels in the mines (Chadambuka et al. 2013) was associated with injuries and accidents that occur in the mining sector. In addition, Ajith and Ghosh (2019) found that job stress and dissatisfaction, drug usage, poor management and supervision, and poor work conditions were common triggers of accidents, injuries, and fatalities among small-scale miners.
Studies on the healthcare sector have also focused on causal factors of injuries and risk of infection among healthcare workers (Aynalem Tesfay and Dejenie Habtewold 2014; Giurgiu et al. 2016; Nsubuga and Jaakkola 2005; Yassi et al. 2014). Some of the main factors were related to needle stick injuries, non-use of gloves or breakage of gloves which are believed to increase the risk of HIV infections. Some work-related injuries were attributed to high job demands associated with healthcare provision in the sub-region. This may be due to insufficient medical facilities and resource constraints on the supply side against the high demand for medical care in most countries in Africa. Furthermore, a limited level of knowledge about occupational safety and health risks among staff (e.g., nurses) may be another factor worth investigating. For this reason, more studies are still needed to reveal the various factors that results in unsafe behavior, injuries, and fatalities among healthcare workers to direct future research and policy development.
Our review of the literature on the construction industry in Africa showed that mechanical hazards, unsafe work environment, long working hours, insufficient break regimes, lack of safety awareness, and negligence by management were among the factors that led to injuries and fatalities among workers (Irumba 2014; Kheni et al. 2010; Nyende-Byakika 2016). This may lead to the assumption that most of the triggers of occupational hazards are induced by the work environment and lack of management. In addition, Amissah et al. (2019) identified individual related factors such as alcoholism, smoking, and aging as prominent factors associated with injuries and fatalities among construction workers. This study is of the view that future research must focus on the role of regulatory bodies so that employers in the construction industry would be duty-bound to ensure the safety and health of their workers. Meanwhile, studies on the manufacturing industry in Africa also sought to examine the causal factors of work-related injuries (Aderaw et al. 2011; Kifle et al. 2014). Factors such as non-use of personal protective clothing, exposure to excessive noise, fumes, dusts, and long working hours were identified as conditions that induced work-related accidents, injuries, and fatalities.
As for SMEs, this study identified that long working hours, over confidence, negligence, non-adherence to regulations (Jones et al. 2016; Olvera et al. 2016; Uzondu et al. 2019), low or non-use of personal protective clothing, exposure to hazardous chemicals, poor hygiene, and poor working environments (Atombo et al. 2017; Kwame et al. 2014; Loewenson 1998; Monney et al. 2014; Ohajinwa et al. 2017) were the main causes of injuries and fatalities among workers. The findings showed a limited evidence regarding the effectiveness of health and work procedures in reducing work-related risks. This may be due to the low level of education among SME workers. In addition, SMEs consist of a higher level of occupational injury cases than large-scale companies (Faris 2017; Nakata et al. 2006).
In the corporate sector, the study found that the sedentary lifestyle of employees coupled with less physical activities may contribute to workers’ health (Aidoo et al. 2015). Our review showed that the majority of employees spend long periods of time in the workplace. Such practice can potentially lead to health-related issues such as cholesterol buildup, high-blood pressure, and obesity. Research on safety and health in this sector has been scarce but the finding calls for attention in this job domain.
Middle East
In the Middle East region, our review revealed some factors related to injuries and fatalities in countries such as Iran, Turkey, and Israel. Studies were mostly found in the energy industry, followed by the healthcare sector, manufacturing and construction industry. The identified factors were mostly related to ergonomic hazards, inappropriate or non-usage of personal protective clothing, negligence, and lack of safety awareness, which led to injuries of varying degrees and fatalities (Nouri et al. 2008; Ünsar and Süt 2015). In addition, the review showed that organizational issues related to poor direct safety management (e.g., poor safety monitoring, condescending safety supervision and bullying, and low tolerance of other co-workers), work overload, poor ambience, inadequate skills and training, and insufficient pay were the main influencers of unsafe worker behaviors (Harsini et al. 2020). It is assumed that these factors may create an unsafe psychological work environment that results in influencing workers’ sense of belonging and acceptance, low morale, and emotional exhaustion.
The literature on the construction industry in this region revealed that injuries and fatalities were mostly due to workers’ non-compliance of proper work procedures. For example, using machines for irregular purposes, over speeding, and non-usage of safety equipment (Mohammadfam et al. 2017) were identified as causes of injuries among workers. With respect to the healthcare sector, the study found that the conditions that led to worker injuries were due to the general lack of knowledge in managing patients and ineffective security measures (Çelebioğlu et al. 2010) in the health facilities. With regard to the manufacturing industry, injury-causing situations were mostly linked to the drivers’ fatigue or inattention. Our review showed the importance of social influences on consequent behaviors of workers. In particular, it showed that negative risky relationships from co-workers influenced workers’ unsafe behavior (Peretz and Luria 2017), thus leading to injuries and fatalities.
Asia
In Asia, we found a number of factors related to injuries and fatalities from countries such as China, Thailand, Hong Kong, India, Taiwan, Singapore, and Malaysia. Most previous studies in this region were performed in the construction industry, followed by mining, healthcare, manufacturing, agriculture, energy, and the corporate sectors. In the construction industry, most studies were concerned about investigating aspects related to non-usage of personal-protective clothing, over confident attitude to risks, influence of unsafe co-worker attitude, and unsafe work environment (e.g., poor lighting and limited space) (Aksorn and Hadikusumo 2007; Choudhry 2014; Hon et al. 2010; Huang et al. 2016; Low et al. 2018). Other organizational factors that we identified were stress due to work overload and inadequate supervision, lack of experience and training, and insufficient pay (Gao et al. 2018). Another noteworthy finding relates to the negative impact of workplace ostracism, psychological detachment, and emotional exhaustion on workers’ safety performance (Chen and Li 2020). This finding not only emphasizes the importance of psychological safety on workers’ behavior, it also contributes to the overall health and well-being of workers. The findings in this region reiterate the factors identified in Africa. This can be attributed to the fact that most countries in Asia and Africa are striving toward economic development status and undertaking a number of built environment projects. These have led to lapses in the management of the safety and health of their workers.
Our review showed that poor lighting levels, ventilation and humid levels were the causal conditions that led to injuries among miners (Cui et al. 2013). Liu et al. (2019) and Fu et al. (2020) in separate writings attributed injuries and fatalities to habitual violations (e.g., improper operations of gas comprehensive prevention systems, illegal operations of miners, and inadequate safety knowledge), and lack of safety culture (e.g., strong regulation and effective control, poor leadership, lapses in planning and workflow). According to Bhattacharjee et al. (2020), failures at the organizational level and poor decision making at the individual level were the main factors of workplace incidents in the mining industry. For example, at the organizational level, it was found that the lack of resources to detect or deal with fire outburst, management priority on production over safety, and the lack of emergency response plan contributed to fatal mining accidents. At the individual level, aspects related to failure at risks and hazards assessment, ignoring safety threats and alerts were the major unsafe factors. These reflect deficiencies in the overall safety management systems. It raises concerns about workers capacity to fully detect potential hazards and the agency to voice out emergent risks. For example, Chen et al. (2019) in their study showed that poor psychological states (e.g., mental fatigue, medication, and alcohol effects) can potentially influence workers’ unsafe behavior.
Previous studies in the healthcare sector reported a significant correlation between non-compliance of glove usage and poor hand hygiene (Ji et al. 2005) with the spread of infections among workers and patients. Salahuddin et al. (2020) found unsafe behavior of healthcare practitioners to be associated with health information systems. For example, issues of carelessness in terms of mistakes in data entry was found to result in clinical errors. In addition, workarounds were found to influence delay in data entry, which poses a risk of losing critical information on patients and could lead to medication errors. Our review also showed that non-compliance to proper procedure of logging in and off the system, the habit of copy and paste were potential unsafe behaviors of practitioners that could lead to errors and outdated information. Although, these factors may not impose any direct negative effect on the healthcare workers, it may still put the lives of patients in danger.
Moreover, previous studies on the manufacturing sector have reported stress, over-confidence, lack of training, and poor supervision as the conditions that contribute to injuries and fatalities among workers (Verma and Chaudhari 2017). Within the energy sector, we found that organizational factors such as structural deficiencies, pressure to meet deadlines, disregard for climatic changes, and worker factors such as negligence were the main causes of work-related accidents and fatalities (Cheng et al. 2013). This is probably because of workers’ low risk perception. Studies on agriculture have tended to investigate aspects related to health impairment, wrong handling of equipment, and falls risk as the main work-related injuries (Zheng et al. 2014). Additionally, lack of sleep or interrupted sleep was found to be associated with certain work-related injuries (Zhu et al. 2014). On the corporate sector, stress, role ambiguity, verbal abuse, long hours of work, and high job demand (Neelamegam and Asrafi 2010) were identified as conditions that led to injuries and health risks among workers.
Australia
In Australia, our review showed that factors associated with workplace injuries and fatalities were mostly found in the healthcare sector. Previous studies have reported that the potential triggers of unsafe behavior were due to emotional, mental, and physical exhaustion (Donovan et al. 2020; Fogarty and Mckeon 2006). The majority of healthcare workers (especially graduate nurses) tend to experience information overload, leading to mental exhaustion of the individuals involved. In addition, the literature showed that certain emotional distresses (e.g., loneliness) can be critical influencers of injuries in the workplace. We also found that demands of shift work and sleep deprivation, tiredness, and fatigue were among the frequent factors influencing the health of healthcare workers. From our review, it is inferred that although these factors may not be similar for all workers, they are still detrimental to the overall health and well-being of healthcare workers.
In the mining sector, we found that factors related to injuries and fatalities were mostly due to lapses in operational leadership support such as training, ergonomic factors (e.g., technological design of equipment), ambience, physical and mental state of workers (Patterson and Shappell 2010). We show that findings relating to the mining industry are similar to the commonly experienced limitations in other regions.
The Americas (the US & Canada)
In the US & Canada, previous studies in the construction industry have examined aspects related to organizational pressures, schedule delays (Han et al. 2014), and certain working habits and ethics such as smoking, use of drugs, drinking, multiple work engagements, and long working hours (Dong et al. 2015) as the main factors that could lead to work-related injuries. However, most of these behaviors are caused by individual workers and other psychological factors. Comparatively with regions such as Europe, Africa, Asia, and the Middle East, it could be inferred that environmental induced hazards are fewer in the US & Canada. It is believed that future research on unsafe behavior must deeply examine the influence of relevant organizational and group factors on the safety behaviors of workers. Furthermore, within the healthcare sector, previous studies mostly investigated how verbal and physical abuse in the workplace can result in injuries (Wolf et al. 2014) and negative psychological outcomes among workers (McCaughey et al. 2015). For example, Merryweather et al. (2018) found that a number of slips, trips, and falls experienced by healthcare workers–especially those who provide homecare services–were due to patients weights, combative patients, and hazards within the home and neighborhood environment.
Additionally, a substantial number of studies on agriculture were also found in this region. Factors such as health impairment, contact with chemicals, long hours of work (Lewis et al. 1998), work pressure, and poor work environment (Arcury et al. 2012; Seo 2005) were the key causes of injuries and fatalities among workers. In the context of SMEs, emotional stress (McGonagle and Kath 2010), low safety knowledge, and poor working conditions were found to trigger work-related injuries and various health risks (Gutberlet et al. 2013).
Final remarks
In order to identify the key contextual issues as pertains to the causal factors of injuries and fatalities in the workplace, we categorized the findings into a multi-regional context. We also clustered the findings into job contexts in their respective regions, namely: construction, healthcare, manufacturing, mining, energy, agriculture, corporate, and SMEs. This was for the purpose of providing more insight into the factors associated with workplace injuries and fatalities. The findings from this review can be useful for identifying region-specific incident trajectories based on their socio-economic development pathways. Our review showed that most of the studies were centered in developing countries (mostly African and Asian countries).
The study found that work-related injuries and fatalities were as a result of the following factors:
-
In Europe, sensation seeking behaviors and non-compliance with safety procedures were found to contribute to injuries and fatalities among workers. It was evident that issues related to emotional and physical exhaustion among workers, particularly those in the healthcare sector, are worthy of attention from researchers, management, and the policy environment.
-
In Africa, injuries and fatalities were mostly caused by work environment, organization, and individual factors. Common environmental factors that were frequently highlighted are: falling rocks, suffocation, explosion, exposure to harmful chemicals, and exposure to excessive noise. Organizational factors in this region were mostly related to the lack of employer interest in the safety and health of their workers, long working hours, management pressure, and non-compliance with safety standards. We also found that certain individual factors were mostly associated with workers’ non-use of protective clothing, exhaustion, and lack of knowledge about risk associated with mercury use. These were evident in the construction, mining, manufacturing, and the SME’s sectors. The findings also indicated that the majority of injury and fatality-causing circumstances were mostly found in the mining sector.
-
In the Middle East, our review showed that the major factors that are responsible for injuries and fatalities among workers were due to various work environment risks and hazards. Also, organizational factors such as management pressure and condescending safety supervision styles were found to contribute to injury risk behavior. Another factor that was identified in this region was the effect of negative relationships and friendships on workers’ unsafe behaviors. It highlights the influence of co-workers for shaping safety performance in organizations. Therefore, workers easily violate safety procedures when they observe other colleagues engage in the same practices.
-
In Asia, similar to the case of Africa, the major causes of injuries and fatalities in the workplace were due to work environmental, organizational, and individual factors. For example, it was found that workers’ limited knowledge about safety and health practices, intentional violation of recommended safety practices, over confidence, poor work environment, lack of management commitment to safety, long working hours and job insecurity, risky behaviors of co-workers, and non-use of personal protective equipment were causal factors. Interestingly, however, the findings showed a similar trend of factors of injuries and fatalities to those in the Middle East. Another aspect worth noting is the issue of negative social influence on workers’ risky behavior and the lack of psychological safety.
-
In Australia, our review showed that the most common factors associated with injuries in the workplace were due to emotional, cognitive, and physical exhaustion experienced by workers, particularly in the healthcare sector. Although these factors do not cause injuries directly, they still may impact negatively on the health and well-being of workers.
-
In the US & Canada, the study found that major causes of injuries and fatalities were due to stress emanating from work pressure, drug abuse, and other psychological factors. We further found violence and aggression from patients (mostly among healthcare workers). Other environmental factors such as work pressure, job insecurity, and work overload were found to significantly contribute to the psychological and emotional disorders of workers.
Recommendations
From the above discussion, it could be inferred that the majority of the factors related to injuries and fatalities in the workplace were mostly similar, especially in regions such as Africa, Asia, and the Middle East. In addition, countries in these regions are classified as transitioning economies; therefore, they are prone to similar economic conditions, and as a result most employers pay less attention to the safety and health conditions of their employees. In these three regions, the factors that contributed to workers’ injuries and fatalities were mostly due to poor work environment, which is also an indication of weak enforcement of safety regulations. For example, in Africa, it is recommended that state actors should take special interest in the safety and health of the working population and strengthen occupational safety and health institutions to oversee the implementation of safety regulations. Reference could be made to the US’s and UK’s safety and health administrative bodies in order to effectively guide the implementation of indigenous institutions that will monitor and control safety issues in the workplace. We further suggest that employers in the region of Africa should look at more workable scenarios for increasing workers’ safety knowledge and safety performance. This includes improving the work environment to reduce hazards, as well as examining how certain behavioral and emotional factors of workers can contribute to their non-compliance of safety procedures. We also recommend that future researchers should pay more attention to explore how changes in workers’ commitment can be the reason for them to follow specific safety standards or vice versa.
In the Middle East, the study recommends that state actors may consider promoting safety awareness in the region. Also, employers may consider strengthening safety training to increase safety awareness among workers, reduce workplace hazards, and take interest to understand the role of psychosocial factors in changing workers safety-oriented behavior. It is believed that this will enable employers to better understand the behavior of workers and allow them to come up with suitable solutions to address various safety-related concerns at the workplace. The study suggests that future research may examine ways to promote safety awareness and behavior among workers. Practitioners should also show commitment to safety training, as well as ensuring a sound balance between production and safety (Kvalheim and Dahl 2016).
In the case of Asia, this study recommends that employers should deepen safety training as well as devote resources to ensure the reduction of hazards at the workplace. Another noteworthy factor was the issue of unsafe psychological conditions that lead workers to experience insecurity in the workplace. Thus, it is anticipated that future studies should be dedicated to exploring how regulatory bodies can effectively monitor and ensure that employers comply with safety and health regulations. In addition, future studies should also consider exploring how organizations could promote psychological safety in the workplace.
As for Australia, the US & Canada, and Europe, it is recommended that decision makers should focus their attention on the various emotional trauma and psychological issues emanating from the workplace, mainly through continuous safety campaigns on stress management. Employers should devote more effort to reduce job pressure on workers by regulating working hours and reducing workload. In addition, employers should take keen interest in issues, such as violence and aggression at the workplace, and introduce proper security measures to protect workers.
The regional dynamics highlighted in this study are an indication that different approaches are required in the drive toward minimizing or eradicating work-related injuries and fatalities. Despite these findings, we are of the view that the state of knowledge about injury and fatality-causing conditions at the workplace remains the subject of some debate. We recommend that future research should concentrate on other factors such as theory development, measurement of the relationships between culture, demographic variables, and occupational stress or workplace injuries and fatalities, and psychological safety. In addition, we propose for a shift in the methodological approach from the purely quantitative based nature to include qualitative research methodologies. This can offer an in-depth understanding of issues that go beyond the “safety iceberg” and explore the underlying factors that promote or hinder safety in the workplace.
References
Aderaw Z, Engdaw D, Tadesse T (2011) Determinants of occupational injury: a case control study among textile factory workers in Amhara regional state, Ethiopia. J Trop Med 2011:657275. https://doi.org/10.1155/2011/657275
Aidoo H, Essuman A, Aidoo P, Yawson AO, Yawson AE (2015) Health of the corporate worker: health risk assessment among staff of a corporate organization in Ghana. J Occup Med Toxicol 10:30. https://doi.org/10.1186/s12995-015-0072-7
Ajith MM, Ghosh AK (2019) Comparison of parameters for likelihood and severities of injuries in artisanal and small-scale mining (ASM). Safety Sci 118:212–220. https://doi.org/10.1016/j.ssci2019.04.010
Aksorn T, Hadikusumo B (2007) The unsafe acts and the decision-to-err factors of Thai construction workers. J Const Developing Countries 12:1–25
Amissah J, Badu E, Agyei-Baffour P, Nakua EK, Mensah I (2019) Predisposing factors influencing occupational injury among frontline building construction workers in Ghana. BMC Res Notes 12:728. https://doi.org/10.1186/s13104-019-4744-8
Andersen LL, Vinstrup J, Villadsen E, Jay K, Jakobsen MD (2019) Physical and psychosocial work environmental risk factors for back injury among healthcare workers: prospective cohort study. N J Environ Res Pub Health 16:4528. https://doi.org/10.3390/ijerph16224528
Angland S, Dowling M, Casey D (2014) Nurses’ perceptions of the factors which cause violence and aggression in the emergency department: a qualitative study. N Emeg Nursing 22:134–139. https://doi.org/10.1016/j.ienj.2013.09.005
Arcury TA, O’Hara H, Grzywacz JG, Isom S, Chen H, Quandt SA (2012) Work safety climate, musculoskeletal discomfort, working while injured, and depression among migrant farmworkers in North Carolina. Am J Pub Health 102:S272–S278. https://doi.org/10.2105/AJPH.2011.300597
Armah FA, Boamah SA, Quansah R, Obiri S, Luginaah I (2016) Unsafe occupational health behaviors: understanding mercury-related environmental health risks to artisanal gold miners in Ghana. Front Environ Sci 4:29. https://doi.org/10.3389/fenvs.2016.00029
Atombo C, Wu C, Tettehfio EO, Nyamuame GY, Agbo AA (2017) Safety and health perceptions in work-related transport activities in Ghanaian industries. Saf Health Work 8:175–182. https://doi.org/10.1016/j.shaw.2016.10.002
Ayaaba E, Li Y, Yuan J, Ni C (2017) Occupational respiratory diseases of miners from two gold mines in Ghana. N J Environ Res Pub Health 14:337. https://doi.org/10.3390/ijerph14030337
Aynalem Tesfay F, Dejenie Habtewold T (2014) Assessment of prevalence and determinants of occupational exposure to HIV infection among healthcare workers in selected health institutions in Debre Berhan town, north Shoa zone, Amhara region, Ethiopia, 2014. AIDS Res Treatment 2014:731848. https://doi.org/10.1155/2014/731848
Baldissone G, Comberti L, Bosca S, Murè S (2019) The analysis and management of unsafe acts and unsafe conditions: data collection and analysis. Safety Sci 119:240–251. https://doi.org/10.1016/j.ssci.2018.10.006
Bhattacharjee R, Dash A, Paul P (2020) A root cause failure analysis of coal dust explosion disaster–gaps and lessons learnt. Engin Failure Analy 111:104229. https://doi.org/10.1016/j.engfailanal.2019.104229
Bohm J, Harris D (2010) Risk perception and risk-taking behavior of construction site dumper drivers. N J Occup Safety Ergono 16:55–67. https://doi.org/10.1080/10803548.2010.11076829
Boniface R, Museru L, Munthali V, Lett R (2013) Occupational injuries and fatalities in a tanzanite mine: need to improve workers safety in Tanzania. Pan Afr med J 16:120. https://doi.org/10.11604/pamj.2013.16.120.3420
Bronkhorst B (2015) Behaving safely under pressure: the effects of job demands, resources, and safety climate on employee physical and psychosocial safety behavior. J Saf Res 55:63–72. https://doi.org/10.1016/j.jsr.2015.09.002
Carter B, Danford A, Howcroft D, Richardson H, Smith A, Taylor P (2013) ‘Stressed out of my box’: employee experience of lean working and occupational ill-health in clerical work in the UK public sector work. Employ Soc 27:747–767. https://doi.org/10.1177/0950017012469064
Çelebioğlu A, Akpinar RB, Küçükoğlu S, Engin R (2010) Violence experienced by Turkish nursing students in clinical settings: their emotions and behaviors. Nurse Educ Today 30:687–691. https://doi.org/10.1016/j.nedt.2010.01.006
Chadambuka A, Mususa F, Muteti S (2013) Prevalence of noise induced hearing loss among employees at a mining industry in Zimbabwe. Afr Health Sci 13:899–906. https://doi.org/10.4314/ahs.v13i4.6
Chen Y, Li S (2020) Relationship between workplace ostracism and unsafe behaviors: the mediating effect of psychological detachment and emotional exhaustion. Psychol Reports 123:488–516. https://doi.org/10.1177/0033294118813892
Chen Z, Qiao G, Zeng J (2019) Study on the relationship between worker states and unsafe behaviours in coal mine accidents based on a Bayesian networks model. Sustainability 11:5021. https://doi.org/10.3390/su11185021
Cheng C-W, Yao H-Q, Wu T-C (2013) Applying data mining techniques to analyze the causes of major occupational accidents in the petrochemical industry. J Loss Prev Process Ind 26:1269–1278. https://doi.org/10.1016/j.jlp.2013.07.002
Chimamise C, Gombe NT, Tshimanga M, Chadambuka A, Shambira G, Chimusoro A (2013) Factors associated with severe occupational injuries at mining company in Zimbabwe, 2010: a cross-sectional study. Pan Afr Med J 14:5. https://doi.org/10.11604/pamj.2013.14/5/full/
Choudhry RM (2014) Behavior-based safety on construction sites: a case study. Accid Analy Prev 70:14–23
Christian MS, Bradley JC, Wallace JC, Burke MJ (2009) Workplace safety: a meta-analysis of the roles of person and situation factors. Am Psychol Assoc 94:1103–1127. https://doi.org/10.1037/a0016172
Cui L, Fan D, Fu G, Zhu CJ (2013) An integrative model of organizational safety behavior. J Saf Res 45:37–46. https://doi.org/10.1016/j.jsr.2013.01.001
Dodoo JE, Al-Samarraie H (2019) Factors leading to unsafe behavior in the twenty first century workplace: a review. Manag Rev Quart 69:391–414. https://doi.org/10.1007/s11301-019-00157-6
Dong XS, Wang X, Largay JA (2015) Occupational and non-occupational factors associated with work-related injuries among construction workers in the USA. N J Occup Environ Health 21:142–150. https://doi.org/10.1179/2049396714Y.0000000107
Donovan H, Welch A, Williamson M (2020) Reported levels of exhaustion by the graduate nurse midwife and their perceived potential for unsafe practice: a phenomenological study of Australian double degree nurse midwives. Workplace Health Safety XX:1–7. https://doi.org/10.1177/2165079920938000
Faris K (2017) Survey of occupational safety and sanitary conditions in small scale enterprises in Jimma southwestern Ethiopia. Ethiopia J Health Dev (EJHD) 12:183–190
Fisch C, Block J (2018) Six tips for your (systematic) literature review in business and management research. Manag Rev Quart 68:103–106. https://doi.org/10.1007/s11301-108-0142-x
Fogarty GJ, Mckeon CM (2006) Patient safety during medication administration: the influence of organizational and individual variables on unsafe work practices and medication errors. Ergono 49:444–456. https://doi.org/10.1080/00140130600568410
Fogarty GJ, Murphy PJ, Perera HN (2017) Safety climate in defence explosive ordnance: survey development and model testing. Safety Sci 93:62–69. https://doi.org/10.1016/j.ssci.2016.11.010
Foster P, Hoult S (2013) The safety journey: using a safety maturity model for safety planning and assurance in the UK coal mining industry. Minerals 3:59–72. https://doi.org/10.3390/min3010059
Frese M, Keith N (2015) Action errors, error management, and learning in organizations. Annu Rev Psych 66:661–687. https://doi.org/10.1146/annurev-psych-010814-015205
Friend MA, Kohn JP (2014) Fundamentals of occupational safety and health (7th edn). Bernan, Landam
Fu G, Xie X, Jia Q, Tong W, Ge Y (2020) Accidents analysis and prevention of coal and gas outburst: understanding human errors in accidents. Proc Safety Environ Protect 134:1–23. https://doi.org/10.1016/j.psep.2019.11.026
Fugas CS, Silva SA, Meliá JL (2012) Another look at safety climate and safety behavior: deepening the cognitive and social mediator mechanisms. Accid Analy & Prev 45:468–477. https://doi.org/10.1016/j.aap.2011.08.013
Gao S, Low SP, Howe HJA (2018) Systemic lapses as the main causes of accidents in the Singapore construction industry. Civil Engin Environ Syst 35:81–98. https://doi.org/10.1080/10286608.2018.1518437
Giurgiu DI et al (2016) Wellbeing and occupational risk perception among health care workers: a multicenter study in Morocco and France. J Occup Med Toxicology 11:20. https://doi.org/10.1186/s12995-016-0110-0
Gutberlet J, Baeder AM, Pontuschka NN, Felipone S, Dos Santos TL (2013) Participatory research revealing the work and occupational health hazards of cooperative recyclers in Brazil. N J Environ Res and Pub Health 10:4607–4627. https://doi.org/10.3390/ijerph10104607
Han S, Saba F, Lee S, Mohamed Y, Peña-Mora F (2014) Toward an understanding of the impact of production pressure on safety performance in construction operations. Accid Analy Prev 68:106–116. https://doi.org/10.1016/j.aap.2013.10.007
Harsini AZ, Ghofranipour F, Sanaeinasab H, Shokravi FA, Bohle P, Matthews LR (2020) Factors associated with unsafe work behaviours in an Iranian petrochemical company: perspectives of workers, supervisors, and safety managers. BMC Public Health 20:1–13. https://doi.org/10.1186/s12889-020-09286-0
Hon CK, Chan AP, Wong FK (2010) An analysis for the causes of accidents of repair, maintenance, alteration and addition works in Hong Kong. Safety Sci 48:894–901. https://doi.org/10.1016/j.ssci.2010.03.013
Huang Y, Wang X, Ding R, Xia N (2016) Risk perception, risk propensity, and unsafe behavior: an empirical study of workers in Chinese construction industry. In: Industrial Engineering and Engineering Management (IEEM), 2016 IEEE International Conference, pp 1121–1125
Hudson P (2007) Implementing a safety culture in a major multi-national. Safety Sci 45:697–722. https://doi.org/10.1016/j.ssci.2007.04.005
Irumba R (2014) Spatial analysis of construction accidents in Kampala, Uganda. Safety Sci 64:109–120. https://doi.org/10.1016/j.ssci.2013.11.024
Ji G, Yin H, Chen Y (2005) Prevalence of and risk factors for non-compliance with glove utilization and hand hygiene among obstetrics and gynaecology workers in rural China. J Hosp Infection 59:235–241. https://doi.org/10.1016/j.jhin.2004.09.027
Jones SL, Walsh JT, Appiah-Opoku S (2016) Rural transport health and safety in sub-Saharan Africa: online survey snapshot of expert opinion. Develop S Africa 33:677–702. https://doi.org/10.1080/0376835X.2016.1203763
Khanzode VV, Maiti J, Ray PK (2012) Occupational injury and accident research: a comprehensive review. Safety Sci 50:1355–1367. https://doi.org/10.1016/j.ssci.2011.12.015
Kheni NA, Gibb AG, Dainty AR (2010) Health and safety management within small-and medium-sized enterprises (SMEs) in developing countries: study of contextual influences. J Const Engin Manag 136:1104–1115
Kifle M, Engdaw D, Alemu K, Sharma HR, Amsalu S, Feleke A, Worku W (2014) Work related injuries and associated risk factors among iron and steel industries workers in Addis Ababa, Ethiopia. Safety Sci 63:211–216. https://doi.org/10.1016/j.ssci.2013.11.020
Kvalheim SA, Dahl Ø (2016) Safety compliance and safety climate: a repeated cross-sectional study in the oil and gas industry. J Saf Res 59:33–41. https://doi.org/10.1016/j.jsr.2016.10.006
Kwame O-B, Kusi E, Lawer E (2014) Occupational hazards and safety practices: a concern among small scale sawmilling industries in tamale Metropolis, Ghana international. J Scient Tech Res 3:234–236
Lamontagne AD, Keegel T, Louie AM, Ostry A, Landsbergis PA (2007) A systematic review of the job-stress intervention evaluation literature, 1990–2005. N J Occup Environ Health 13:268–280. https://doi.org/10.1179/oeh.2007.13.3.268
Lewis MQ, Sprince NL, Burmeister LF, Whitten PS, Torner JC, Zwerling C (1998) Work-related injuries among Iowa farm operators: an analysis of the Iowa farm family health and Hazard surveillance project. Am J Indust Med 33:510–517. https://doi.org/10.1002/(SICI)1097-0274(199805)33:5,510::AID-AJIM11.3.0.CO;2-0
Liu Q, Meng X, Hassall M, Li X (2016) Accident-causing mechanism in coal mines based on hazards and polarized management. Safety Sci 85:276–281. https://doi.org/10.1016/j.ssci.2016.01.012
Liu R, Cheng W, Yu Y, Xu Q, Jiang A, Lv T (2019) An impacting factors analysis of miners' unsafe acts based on HFACS-CM and SEM. Proc Safety Environ Protection 122:221–231. https://doi.org/10.1016/j.psep.2018.12.007
Liu X, Huang G, Huang H, Wang S, Xiao Y, Chen W (2015) Safety climate, safety behavior, and worker injuries in the Chinese manufacturing industry. Safety Sci 78:173–178. https://doi.org/10.1016/j.ssci.2015.04.023
Loewenson RH (1998) Health impact of occupational risks in the informal sector in Zimbabwe. N J Occup Environ Health 4:264–274. https://doi.org/10.1179/oeh.1998.4.4.264
Long RN, Sun K, Neitzel RL (2015) Injury risk factors in a small-scale gold mining community in Ghana’s upper east region. N J Environ Res Pub Health 12:8744–8761. https://doi.org/10.3390/ijerph120808744
Low BKL, Man SS, Chan AHS (2018) The risk-taking propensity of construction workers—an application of quasi-expert interview. N J Environ Res Pub Health 15:2250. https://doi.org/10.3390/ijerph15102250
Manu PA, Ankrah NA, Proverbs DG, Suresh S (2012) Investigating the multi-causal and complex nature of the accident causal influence of construction project features. Accid Analy Prev 48:126–133. https://doi.org/10.1016/j.aap.2011.05.008
McCaughey D, Turner N, Kim J, DelliFraine J, McGhan GE (2015) Examining workplace hazard perceptions & employee outcomes in the long-term care industry. Safety Sci 78:190–197. https://doi.org/10.1016/j.ssci.2015.04.013
McGonagle AK, Kath LM (2010) Work-safety tension, perceived risk, and worker injuries: a meso-mediational model. J Saf Res 41:475–479. https://doi.org/10.1016/j.jsr.2010.09.002
Merryweather AS, Thiese MS, Kapellusch JM, Garg A, Fix DJ, Hegmann KT (2018) Occupational factors related to slips, trips and falls among home healthcare workers. Safety Sci 107:155–160. https://doi.org/10.1016/j.ssci.2017.07.002
Mohammadfam I, Ghasemi F, Kalatpour O, Moghimbeigi A (2017) Constructing a Bayesian network model for improving safety behavior of employees at workplaces. Appl Ergono 58:35–47. https://doi.org/10.1016/j.apergo.2016.05.006
Moher D, Liberati A, Tetzlaff J, Altman DG, Group atP (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals Internal Med 151:264–269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
Monney I, Bismark D-A, Isaac O-M, Kuffour RA (2014) Practices among vehicle repair artisans in an urban area in Ghana. J Environ Occup Sci 3:147–153. https://doi.org/10.5455/jeos.20140528072614
Mrema EJ, Ngowi AV, Mamuya SH (2015) Status of occupational health and safety and related challenges in expanding economy of Tanzania. Annals Glob Health 81:538–547. https://doi.org/10.1016/j.aogh.2015.08.021
Nakata A et al (2006) The prevalence and correlates of occupational injuries in small-scale manufacturing enterprises. J Occup Health 48:366–376. https://doi.org/10.1539/joh.48.366
Neal A, Griffin MA (2002) Safety climate and safety behaviour. Aus J Manag 27:67–75. https://doi.org/10.1177/031289620202701S08
Neal A, Griffin MA (2006) A study of the lagged relationships among safety climate, safety motivation, safety behavior, and accidents at the individual and group levels. J Appl Psycho 91:946–953. https://doi.org/10.1037/0021-9010.91.4.946
Neelamegam R, Asrafi S (2010) Work stress among employees of Dindigul district central cooperative bank, Tamil Nadu: a study IUP. J Manag Res 9:57–69
Nordlöf H, Wiitavaara B, Winblad U, Wijk K, Westerling R (2015) Safety culture and reasons for risk-taking at a large steel-manufacturing company: investigating the worker perspective. Safety Sci 73:126–135. https://doi.org/10.1016/j.ssci.2014.11.020
Nouri J, Azadeh A, Fam IM (2008) The evaluation of safety behaviors in a gas treatment company in Iran. J Loss Prev Process Ind 21:319–325. https://doi.org/10.1016/j.jlp.2007.11.006
Nsubuga FM, Jaakkola MS (2005) Needle stick injuries among nurses in sub-Saharan. Af Trop Med N Health 10:773–781. https://doi.org/10.1111/j.1365-3156.2005.01453.x
Nyende-Byakika S (2016) Occupational safety and health issues on road construction sites in sub-Saharan Africa: a case study from Uganda. Afr J Sci, Tech, Innov Dev 8:256–263. https://doi.org/10.1080/20421338.2016.1156838
Ohajinwa CM, van Bodegom PM, Vijver MG, Olumide AO, Osibanjo O, Peijnenburg WJ (2017) Prevalence and injury patterns among electronic waste workers in the informal sector in Nigeria. Injury Prev 24:185–192. https://doi.org/10.1136/injuryprev-2016-042265
Olvera LD, Guézéré A, Plat D, Pochet P (2016) Earning a living, but at what price? Being a motorcycle taxi driver in a sub-Saharan African city. J Transp Geogr 55:165–174. https://doi.org/10.1016/j.jtrangeo.2015.11.010
Parker D, Lawrie M, Hudson P (2006) A framework for understanding the development of organisational safety culture. Safety Sci 44:551–562. https://doi.org/10.1016/j.ssci.2005.10.004
Patterson JM, Shappell SA (2010) Operator error and system deficiencies: analysis of 508 mining incidents and accidents from Queensland, Australia using HFACS. Accid Analy Prev 42:1379–1385. https://doi.org/10.1016/j.aap.2010.02.018
Peretz RA, Luria G (2017) Drivers’ social-work relationships as antecedents of unsafe driving: a social network perspective. Accid Analy Prev 106:348–357. https://doi.org/10.1016/j.aap.2017.07.005
Ramacciati N, Ceccagnoli A, Addey B (2015) Violence against nurses in the triage area: an Italian qualitative study. N Emerg Nurs 23:274–280. https://doi.org/10.1016/j.ienj.2015.02.004
Reason J (2005) Safety in the operating theatre–part 2: human error and organisational failure. Qual Safety Health Care 14:56–60. https://doi.org/10.1016/S0953-7112(05)80010-9
Salahuddin L, Ismail Z, Hashim UR, Ismail NH, Raja Ikram RR, Abdul Rahim F, Hassan NH (2020) Healthcare practitioner behaviours that influence unsafe use of hospital information systems. Health Inform J 26:420–434. https://doi.org/10.1177/1460458219833090
Sanmiquel L, Freijo M, Edo J, Rossell JM (2010) Analysis of work related accidents in the Spanish mining sector from 1982-2006. J Saf Res 41:1–7. https://doi.org/10.1016/j.jsr.2009.09.008
Schultz AB, Edington DW (2007) Employee health and presenteeism: a systematic review. J Occup Rehab 17:547–579. https://doi.org/10.1007/s10926-007-9096-x
Searcy DL, Mentzer JT (2003) A framework for conducting and evaluating research. J Account Lit 22:130–167
Seo D-C (2005) An explicative model of unsafe work behavior. Safety Sci 43:187–211. https://doi.org/10.1016/j.ssci.2005.05.001
Sorensen G, Nagler EM, Pawar P, Gupta PC, Pednekar MS, Wagner GR (2017) Lost in translation: the challenge of adapting integrated approaches for worker health and safety for low-and middle-income countries. PLoS One 12:e0182607
Sovacool BK, Mukherjee I (2011) Conceptualizing and measuring energy security: a synthesized approach. Energy 36:5343–5355. https://doi.org/10.1016/j.energy.2011.06.043
Sullman MJ, Stephens AN, Pajo K (2017) Transport company safety climate—the impact on truck driver behavior and crash involvement. Traffic Inj Prev 18:306–311. https://doi.org/10.1080/15389588.2016.1199865
Takala J, Hämäläinen P, Nenonen N, Takahashi K, Chimed-Ochir O, Rantanen J (2017) Comparative analysis of the burden of injury and illness at work in selected countries and regions. Cent Eur J Occup Environ Med 23:6–31
Takala J et al (2014) Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hygiene 11:326–337
Ünsar AS, Süt N (2015) Occupational accidents in the energy sector: analysis of occupational accidents that occurred in thermal and hydroelectric centrals between 2002 and 2010 in Turkey. Procedia-Social and Behav Sci 181:388–397. https://doi.org/10.1016/j.sbspro.2015.04.901
Uzondu C, Jamson S, Lai F (2019) Investigating unsafe behaviours in traffic conflict situations: an observational study in Nigeria. J Traffic Transp Engin (English edition) 6:482–492. https://doi.org/10.1016/j.jtte.2018.06.002
Verma S, Chaudhari S (2017) Safety of Workers in Indian Mines: study, analysis, and prediction. Safety Health Work 8:267–275. https://doi.org/10.1016/j.shaw.2017.01.001
Winge S, Albrechtsen E, Mostue BA (2019) Causal factors and connections in construction accidents. Safety Sci 112:130–141. https://doi.org/10.1016/j.ssci.2018.10.015
Wirth R, Foerster A, Rendel H, Kunde W, Pfister R (2017) Rule-violations sensitise towards negative and authority-related stimuli. Cognition Emotion 32:480–493. https://doi.org/10.1080/02699931.2017.1316706
Wolf LA, Delao AM, Perhats C (2014) Nothing changes, nobody cares: understanding the experience of emergency nurses physically or verbally assaulted while providing care. J Emerg Nursing 40:305–310. https://doi.org/10.1016/j.jen.2013.11.006
Yassi A et al (2014) Considerations for preparing a randomized population health intervention trial: lessons from a south African–Canadian partnership to improve the health of health workers. Glob Health Action 7:23594. https://doi.org/10.3402/gha.v7.23594
Zheng L et al (2014) Nonfatal work-related injuries among agricultural machinery operators in northern China: a cross-sectional study. Injury 45:599–604. https://doi.org/10.1016/j.injury.2013.07.004
Zhu H et al (2014) Sleep-related factors and work-related injuries among farmers in Heilongjiang Province, People’s republic of China. N J Environ Res Public Health 11:9446–9459. https://doi.org/10.3390/ijerph110909446
Zohar D (2010) Thirty years of safety climate research: reflections and future directions. Accid Analy Prev 42:1517–1522. https://doi.org/10.1016/j.aap.2009.12.019
Zohar D, Luria G (2005) A multilevel model of safety climate: cross-level relationships between organization and group-level climates. J Appl Psycho 90:616–628. https://doi.org/10.1037/0021-9010.90.4.616
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No funding was received for conducting this study.
Ethical approval
Ethical approval is not required for this review.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dodoo, J.E., Al-Samarraie, H. A systematic review of factors leading to occupational injuries and fatalities. J Public Health (Berl.) 31, 99–113 (2023). https://doi.org/10.1007/s10389-020-01427-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-020-01427-4