
Abstract
This chapter is a review of the occupational health and safety measures in the public sector to determine their adequacy in ensuring the wellbeing of the employees in the working environment. The goal of occupational health and safety measures is to prevent or at least minimize the chances of injuries, deaths and diseases arising from the working environment. Like many other countries, Zimbabwe is a signatory to the International Labour Organisation (ILO) Conventions on occupational health and safety. The country has developed policy, legislation and institutional frameworks on occupational health and safety at sectoral, organisational and national levels. The study adopted an exploratory qualitative design and data was gathered through the desktop to determine any gaps in terms of occupational health and safety strategies in place. The study results established that the occupational health and safety measures in the public sector are inadequate. The country lacks a comprehensive and harmonized occupational health and safety legal framework. The study recommends that the government of Zimbabwe should take adequate preventative and protective measures to ensure a safe working environment for all workers in the public sector.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Occupational health and safety
- Public sector
- Personnel health
- Occupational hazards
- Legislative framework
Introduction and Background
Workers constitute half of the world’s population and are the main contributors to the economic and social development of modern societies (ILO, 2019). Access to health and safety in the workplaces has however not matched the industrialization spur in both 1stworld and developing economies (Moyo et al., 2015). This is supported by statistics showing that more than 2 million work related deaths and about 300 million non-fatal occupational accidents occur annually around the globe (Mpofu, 2019). According to the ILO (2019), these occupational accidents and deaths result in global economic costs amounting to about 4% of the global gross domestic product (GDP). Despite these alarming statistics and the negative effects that occupational fatalities have on people’s lives Occupational Health and Safety (OHS) has not received significant attention and support when compared to other global health problems such as Malaria, tuberculosis and HIV and AIDS. In fact (Schmidth et al., 2017) argue that Occupational Health and Safety issues remain an island whose existence remains recognized but little effort is put towards supporting it. There is thus, an urgent need for policymakers to come up with adequate support, preventive, protective and control measures to redress the situation.
Despite millions of workers being at risk of various types of occupational-related diseases including pneumoconiosis, mental health and musculoskeletal disorders, there is a scarcity of information on work-related fatalities in Sub Saharan Africa on that to base OHS outcomes (Mrema et al., 2015). The region lacks coordinated systems to collect this data regularly and actively, relying on “passive notifications” from either compensation institutions or labour inspectorate whenever workplace accidents occur (Mrema et al., 2015). Published literature estimates about 18,000 workers die in work-related accidents on the continent annually, while more than 1.3 million are injured in accidents and 67,00 contract occupational illness (Mpofu, 2019). Zimbabwe is no exception to this as evidenced by the significant gaps in OHS related information (Maumbe, 2017). The magnitude of work-related accidents and illnesses arising from economic activities such (manufacturing, transport, construction, commerce and agriculture) in Zimbabwe are yet to be fully ascertained because of lack of coordinated national reporting systems for such accidents (Maumbe, 2017) In this regard diseases, accidents and deaths as a result of occupational hazards are a major concern among Zimbabwean workers.
When it comes to public sector employees, the most common causes of work-related hazards within office settings emanate from prolonged physical inactivity (Muzhazha-Nyandoro & Nyawude, 2017). It has been observes that prolonged physical inactivity especially among employees who spend most of their working hours seated can lead to numerous health problems such as cardiovascular diseases, digestive problems, obesity, and reduced lung efficiency (Brauer, 2006). Similarly, Jambwa and Chitongo (2013) argue that sedentary public sector employees are further exposed to hazardous conditions such as dust in their poorly ventilated offices, old, dilapidated office furniture, long hours of computer use, and other related hazards caused by poor working conditions that strain their bodies.
According to Brauer (2006), long hours of computer use among public sector employees are harmful to human health and can result in soreness and numbness in the arms and shoulders. In addition to this, bright light and flickering images on the computer can strain eyes. In the long run, millions of employees acquire diseases, injuries and some become permanently disabled due to these occupational hazards (Jambwa & Chitongo, 2013). Despite the tremendous negative effects on the lives of employees and their families, access to OHS in the workplace remains a challenge in Zimbabwe (Muzhazha- Nyandoro and Nyawude, 2017). Statistics reveal that the country continues to experience a sharp increase in occupational mishaps with figures rising 2443% to 133 000 employees who were injured and contracted the work-related illness in 2019 (Mhlanga, 2020). The figures indicate a widespread problem and a substantial economic burden on individuals, the government, and the society at large. Higher occupational injuries, illness and deaths are also adding to the economic crisis experienced in Zimbabwe, highlighting the need to invest in OHS (Mhlanga, 2020). Employers and in this case, the government, must forecast, assess and control a wide range of workplace-related hazards that can harm the health and safety of their employees.
Banda (2014) observes that putting in place effective occupational health and safety strategies appeal to an employee’s mental status including trust and reliability. Murral et al. (2011) highlights that implementing OHS programmes promotes organisational efficiency and reduces costs. Moreover, these measures signify the employer’s moral and ethical commitment to protect their workers from accidents and ill health when at work. In summary, the overall benefit of implementing OHS strategies include organisational efficiency, increased worker morale, reduced costs, employee retention and staff commitment to the organisation. It is against this background that the study explores health and safety perspectives in the Zimbabwean public sector and their implications on employee wellbeing. Public sector employees are critical to economic development and the provision of basic goods and services, and their wellbeing should be guaranteed at all costs. The study seeks to address the following key questions; What are the regulatory frameworks governing OHS in Zimbabwe’s public sector? That key institutions are involved in OHS in Zimbabwe? What are the current gaps and challenges to OHS in Zimbabwe’ public sector?
Literature Review
Occupational Health and Safety in the Contemporary Public Sector: An Overview
Over the last two decades, working conditions in the public sector have considerably changed under political pressures to enhance efficiency and effectiveness (Schmidth et al., 2017). These changes and reforms have been implemented in accordance with the principles of New Public Management (NPM) that include contacting out, decentralization of activities and introduction of performance management drawn from the private sector (Hall, 2013). In other words, private sector practices have been transferred to the public sector. NPM also emphasises the need to adopt robust systems and checks for improved employee health and safety in the workplace. However, these NPM transformations have also affected working life, with negative consequences for working conditions including issues on OHS due to growing demands and dwindling resources (Diefenbuch, 2009).
NPM introduced contracting between separated purchaser and provider and today public sector institutions are now regarded as large businesses purchasing professional services and temporary labour (Schmidt et al., 2017). This situation has resulted in contract employment and retrenchments, that has seen a decline in workplace and worker safety representation, a critical cog in the formulation and implementation of OHS systems (Dienfenbuch, 2009). In most countries, both developing and developed, worker representation has been seen as key support for effective OHS in the public sector (Jambwa and Chitongo, 2013). Additionally, the ILO also stipulates that the employer should ensure that employees and their health and safety representatives are consulted, informed, and trained on all aspects of OHS, including emergency arrangements associated with their work (Taderera, 2012). Similarly, in Zimbabwe, legislation requires employers to consult health and safety representatives regarding OHS measures and programmes, the decrease in worker representation is thus problematic and poses threats for effective OHS promotion in organisations (Jabwa and Chitongo, 2013). As such employers should make certain the establishment and effective functioning of safety and health committees and the recognition of workers’ safety and health representatives in accordance with national laws and practices.
Moreover, in most countries, political systems are based on the principle that decisions taken by the elected politicians shall be put into practice by professional officials in public administration (Schmidt et al., 2017). As such fundamentals and overall limits on the adoption, implementation, and management of OHS provisions and the budgets for the utilisation of these services is set by politicians (Schmidt et al., 2017). Guided by the various legislative frameworks underpinning good labour practices and motivated by knowledge, market dynamics, scope and nature of the organisation, public sector organisations should thus find OHS models perceived to be best in their organisations. Ultimately, in modern-day societies, political governance plays a huge part in the implementation of OHS policies, projects, and plans. As such strong political will is necessary for effective OHS implementation across the globe.
Numerous competing theoretical models have been suggested and used in the domain of OHS research and these include Heinrich’s Domino- accident causation model, Bird’s loss causation theory and Rasmussen’s risk management framework. According to (Wang & Yan, 2019) each of these theories have their distinct approach when used for analysing accidents. However, they have a common disadvantage (Fu et al., 2016), they fail to define the accident cause and each level so that people may not prevent accidents by directly, accurately, or conveniently applying the analytical process and interpreting their results. As such an improved accident causation model was developed by Fu et al. (2016).
Improved Accident Causation Model
The Improved Accident Causation Model seeks to demonstrate the relationship between the cause and effect that the predating theories have failed to do (Wang & Yan, 2019). It postulates that all occupational accidents belonging to the organisation are mainly attributed to internal organisational causes at both individual and organisational levels (Fu et al., 2016). Furthermore, the theory indicates that accidents also result from interactions among causal factors residing at all levels of the sociotechnical system that are from the government to all individuals in the involved organisation. These causal factors can be classified as internal and external causes based on the manageable boundaries of the organisation. Wang and Yan (2019) define the internal causes as those much more changeable and controllable by the managers of the organisation to improve safety performance. These internal causes, therefore, serve as key points for accident analysis, and they include lack of safety culture, poor or non-existent safety management systems, flaws in safety awareness and lack of safety knowledge. On the other hand, external causes mainly involve factors from natural disasters, poor government supervision and substandard OHS designs that commonly contribute to accidents by influencing the internal causes (Fu et al., 2016). Figure 11.1 below depicts the Improved Accident Causation Model.

(Source Adopted from Fu et al. [2016])
Improved accident causation model
According to Fu et al. (2016), the red dotted line signifies the manageable boundary of an organisation related to the accidents that separate all the causes in socio-technical systems into internal and external ones. The blue boxes are the internal causes that are categorized into five classifications from individual faults to organisational deficiencies. The blue arrows in the diagram indicate the sequence of internal causes leading to accidents and these include defective safety management systems, flaws in individual safety knowledge, then unsafe acts and unsafe conditions that eventually lead to an accident. It should be noted the correlation between these factors is what ultimately results in occupational accidents (Wang & Yan, 2019). On the other hand, the red arrows show the order undertaken when conducting accident analysis that begins from bad outcomes to immediate causes, to flaws in an employee’s safety knowledge, safety awareness, flaws in the organisational safety management systems and finally in the weakness in safety culture (Fu et al., 2016).
The significance of this theory lies in its ability to provide a pathway for accident analysis from the individual level to the organisational level. Given the nature of the public sector, this theory enables OHS research to be conducted with individual organisations in mind as they differ in scope and mandate. It also encourages systematic research into the multiple causes of accidents in government departments, parastatals and local authorities that can lead to effective systems that abate occupational accidents among public sector employees.
Methodology
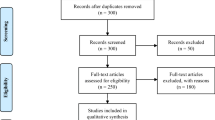
This study was qualitative. The researchers employed secondary data collection methods. Secondary methods involve documentary review were journal articles, academic books, newspapers and research articles were examined to gain insights into the issues relating to the Health and safety perspectives in the Zimbabwe public sector. Bailey (1994) argues that documentary search entails the analysis of documents that contain information regarding the subject matter to be studied. The definition above recommends the researchers determine the relevance of the sources that they utilise based on their significance to the research. Similarly, Dey, 2005 observes that criteria for choosing documents used in a study must reflect the issues on that the researchers are seeking evidence. The researchers gathered data regarding the Health and Safety perspectives in the Zimbabwe public sector from documents that include both published and unpublished works. The main advantage of using this instrument was that the data was readily available. Since the research relied on secondary data, the researchers acknowledged sources used to avoid plagiarism. Manual thematic and Matrix analysis on Microsoft word was then used to analyse data.
Results and Discussion
Occupational Health and Safety Management in Zimbabwe
Regulatory Frameworks Governing Occupational Health and Safety in Zimbabwe
At an international level, occupational health and safety regulations are modelled around the ILO Conventions 155 and 161 that guide the promotion of occupational health and safety systematically (Mazhazha-Nyandoro & Nyaude, 2017). The ILO guidelines facilitate the formation, implementation, and evaluation of OHS interventions and regulations at sectoral, organisational, and national levels in all member countries (ILO, 2001). In addition, the ILO-OHS Framework (2001) outlines the legislation and standards, that apply to organisations and prescribes the procedures for hazardous and risk assessment.
Zimbabwe as a signatory to the above-mentioned ILO conventions came up with laws surrounding health and safety at the workplace. At a general level, occupational and health safety laws that apply to all employers and employees across sectors are the Labour Act, Chapter 28.01 and NSSA (Accident Prevention) (Workers Compensation scheme) Notice No. 68 of 1990 (Mywage.org/Zimbabwe: online). These laws emphasise creating awareness and promoting health and safety in the workplaces, providing rehabilitation services, and enforcing health and safety legislation and providing financial benefits to families of workers who have been killed or injured or who have acquired occupational illness (Jerie, 2012). These frameworks are discussed below.
Accident Prevention and Workers’ Compensation (Statutory Instrument 68 of 1990)
According to Mpofu (2019), Statutory Instrument 68 of 1990 is quite detailed in presenting a platform for the management of OHS issues in places of employment across all sectors. The key issues highlighted in this Act include the roles of employers and employees in implementing OHS policies and safeguarding their OHS rights in workplaces. It also provides for the right to compensation for employees that suffer injuries and illness acquired during their course of service. Statutory Instrument 68 of 1990 goes further to stipulate the grounds on that compensation will not be granted to employees. The reasons include, death occurring more than a year after an accident at work unless it is verified to have directly originated from the injury and deliberate negligence and misconduct (Moyo et al., 2015). Scheduled occupational illnesses arising from various workplace hazards are also listed and serious occupational accidents are defined as those resulting in permanent disablement of more than 30% (Government of Zimbabwe, 2010).
Additionally, the Statutory Instrument highlights that employers should notify all workers of any risks arising from the use of new technologies and their imminent dangers. Furthermore, the employer must take an instantaneous action to discontinue any operations or activities that poses danger to the safety and health of employees and evacuate them as appropriate. This Statutory Instrument also prescribes that is the responsibility of NSSA to compensate injured workers in the event of occupational hazards, paid from the financial contributions from both the employer and employees collected over the employment period. However, the literature reviewed brought to light a number of challenges that affect the effectiveness of this Statutory Instrument in Zimbabwe, and these include lack of proper enforcement mechanisms and capacity challenges (inadequate financial, human and technological resources (Moyo et al., 2015, Mazhazha-Nyandoro & Nyaunde, 2017).
Based on the research reviews it was apparent that the enforcement mechanisms provided for by SI 68 of 1990 (punishment of a level five fine or a jail sentence not exceeding six months) imposed on defaulters, raises doubt as to whether the employers and workers will live up to their responsibilities. In other words, these penalties are not sufficient motivation for employers and employees to comply with OHS regulations put in place by the government. The study also found out that the contributions currently paid to NSSA are not enough adequate to cover medical bills and the welfare of injured employees and their families in the event of permanent disability. The small percentage of each employee’s contribution (1.38% of each employee’s insurable earning) and the current prevailing economic environment in the country has largely contributed to this situation. For instance, for a public employee earning 30 000 ZWL their contribution would only be $ 414 ZWL. It was also observes that the Factory Inspectorate and OHS services department at NSSA is currently understaffed and has limited transportation capacity. To this effect, the department is forced to take limited action on reported accidents. In most cases, priority is given to very serious cases or those in easy to reach areas within the proximity of the inspectorate.
Public Service State Service (Disability Benefits) Act [Chapter 16:05]
According to this scheme workers who became permanently disabled from injuries sustained at workplaces of at least 30% are entitled to compensation that is paid as a pension (Government of Zimbabwe, 2010). The scheme further stipulates that workers who suffer permanent disabilities below 30% receive a hefty once-off payment commensurate with the severity of their condition (Government of Zimbabwe, 2010). In analysis, public servants in Zimbabwe hardly benefit from this scheme in the event of occupation hazards. Although the tenants of the scheme are good, the processes of benefiting from the scheme are highly bureaucratic and cumbersome such that few workers have benefited from the scheme since its inception.
The Public Health Control of Tobacco Statutory Instrument 264 of 2002 and the Labour Relations HIV and AIDS S.I 202 of 1998
At the secondary level, there is the Public health control of Tobacco (Statutory Instrument (S.I) 264 of 2002) that protects workers from acquiring illness due to public smoking. This instrument bans smoking in enclosed public places including places of work. Although the Act exists, its applicability in the Zimbabwean public sector remains a big challenge. The concept of public places is rather difficult to interpret and enforce thus workers feel it is their right to smoke while at work. Due to the lack of proper infrastructure, the protection and health of workers are highly compromised. Most public service offices are highly congested and lack proper ventilation thereby exposing workers to risks of getting ill while at work.
Labour Relations HIV and AIDS S.I 202 of 1998 is another framework that safeguards the health and safety of employees in Zimbabwe’s public sector. Among other issues, this legislation spells out the provision of protective clothing and other safety devices to prevent the spread of HIV and AIDS in workplaces (Taderera, 2012). In a bid to promote mental health among workers infected by the disease it prohibits discrimination on the grounds of HIV and AIDS status, including respecting the confidentiality of the employee’s HIV status and prohibiting compulsory testing for HIV as a requirement of employment (Taderera, 2012). In line with this framework, the study findings revealed that all public institutions acknowledge that the fight against HIV and AIDS calls for a multi-sectoral approach where all public employees are involved both in their individual and official capacities.
The public Sector also developed the HIV Workplace policy that directed public service departments on forming HIV and AIDS workplace structures to support those infected and affected and promoting educating others on contracting HIV. To ensure the success of this policy, findings reveal that all public institutions have put in place HIV and AIDS focal individuals who have undertaken training in mainstreaming HIV and AIDS issues in organisational strategic plans and developmental programmes. The policy framework also spells out HIV/AIDS as an occupational issue and defines those who contracted the virus while conducting their direct duties to be compensated by the government.
Although the policy is good, its application and interpretation by user departments have been very weak. Due to limited fiscal space, the government has not been able to seriously follow up HIV cases as an occupational health issue rather these have been left with human resources departments to manage workforce mobility. Therefore, the commitment of the employer to protect and assist the public sector workforce against HIV/AIDS has been a rhetoric theme that lacked systematic interpretation and implementation. Most government departments reveal they do not have HIV/AIDs workplace committees and the absence of workers’ committees in the public servants set up presents difficulties for those who could have benefited as there is no formal structure to handle health safety concerns from employees.
The Factories and Workers Act Chapter 14:08
The Factories and Worker Act Chapter 14:08 is also used to promote OHS in Zimbabwe (Banda, 2014). This Act addresses the need to establish accident registers at workplaces and ensure that all accidents that result in absence of more than three days are reported to the inspector for accountability purposes (Muzhazha-Nyandoro & Nyawude, 2017). It also requires that medical personnel attending to employees suffering from lead, mercury poisoning or anthrax as a result of occupational exposures make a formal report to the inspector (Mpofu, 2019). The implementation of the Act within the public sector departments resides within human resources practitioners and indeed exists. The study established there are registers maintained at workplaces especially within the health occupations where all health personnel must maintain incident reports on a daily, weekly, and monthly basis. However, the interval of reporting has been affected by negative attitudes and a lack of appreciation of the importance of maintaining such a record.
Furthermore, it was established that the country has a weak system for the comparative analysis and production of annual occupational health statistics (Masekameni et al., 2020). Although the government of Zimbabwe through NSSA has adopted an OHS database management system for collecting, classifying and analysing accident data it is not effectively used due to technical and financial constraints. Correspondingly, attributable to the dearth of staff in the public domain and lack of appreciation of the importance of maintaining OHS records, data entry is not carried out uniformly throughout the public sector. In the end, this could mean that the data cannot be used to report and analyse data using international classification systems (Masekameni et al., 2020) accurately and truthfully.
Public Health (COVID-19) Prevention, Containment and Treatment Regulations (Statutory Instrument 77 of 2020)
Following the emergence of the Corona Virus in 2019 (COVID-19) and the subsequent declaration by the World Health Organisation of the virus as a global catastrophe, the pandemic has been threatening the health and livelihoods of employees around the world. In response to the pandemic, a state of disaster was declared by the president of Zimbabwe on the 20th of March 2020 and soon after this the SI 77 of 2020 was gazetted to limit and prohibit commercial activities in both the public and private sectors, and outline measures to prevent, contain and treat those affected by the disease. (Muzvidziwa-Chilunjika et al. 2020) argue that the capacity of the public sector to deliver basic services has been comprised by the pandemic in the following ways:
-
Exacerbated absenteeism due to sickness, deaths and attending to sick relatives or funerals
-
Increased stress at the workplace due to inadequate Personal Protective Equipment PPE, leading to lower productivity.
-
The brain drain of qualified and experienced employees (especially in the health sector) due to their mass exodus in pursuit of greener pastures in European countries who were hit hard by the pandemic
In relation to OHS, the legislation outlines that employer should test their employees and adhere to the Covid-19 prevention protocols at their workplaces. The statutory instrument also stipulates that employers should provide PPE, sanitisers and maintain workplace hygiene practices including the provision of clean water sources for washing hands in public places. The study found out that public institutions such as state universities, parastatals including ZETDC and some local authorities gave out PPE (masks) and sanitisers to their staff. However, it was observes that these provisions were not adequate, and their distribution was not constant due to financial constraints. It was disturbing to argue that the working conditions of public healthcare workers, who were the most critical instrument in the fight against the pandemic were at times dire. This is supported by a series of health worker strikes that were instigated in part due to a lack of adequate PPE between August and September 2020. A situation that hampered the efficient delivery of health services to the public at a time they need them the most.
Although the government embarked on OHS inspections to carry to monitor the adherence of COVID-19 protocols at workplaces, information provided by NSSA in its report on Convention no 170 of the ILO indicated that it remains a challenge to refer cases of incompliance detected during inspections to courts due to limited understanding of Judicial system on OHS issues. Coupled with lenient penalties imposed on those who fail to follow the OHS laws, enforcement of compliance remains problematic in Zimbabwe (ILO, 2020).
Key Institutions Involved in Occupational Health and Safety in Zimbabwe’s Public Sector
Ministry of Public Service, Labour and Social Welfare
The Ministry of Public Service, Labour and Social Welfare is the arm of government that works in partnership with the ILO in promoting good OHS governance in Zimbabwe (Taderera, 2012). This is achieved through its Labour administration and employment services department whose statutory responsibility is to protect all workers by promoting fair labour practices and making the utmost possible contribution to the socio-economic wellbeing of the nation (NSSA, 2012). The Ministry is also responsible for crafting and implementing national policies, plans and projects on OHS through NSSA. The study established that the Ministry of Public Service Labour and Social welfare has a department that represents employees on any form of labour practices likely to affect their welfare, health and safety. The function is decentralized to provincial and district levels across the country to assist workers in accessing information and advise them of their rights. The quality of knowledge disseminated from the respective Ministry offices and the accessibility of the functions by workers remains a debate. However, to a lesser extent, public sector workers in Zimbabwe have a representative body that is designed to assist solve occupational issues in cases of disagreements within the service period.
In relation to the protection of public servants’ OHS rights, a study by (Masekameni et al., 2020) indicated the need by the government to take measures to ensure that workers are fully protected from undue consequences especially on those who remove themselves from a work situation that they have reasonable justification to believe presents an imminent danger to their health and life. Furthermore (Masekameni et al., 2020) emphasised the need to avail information on legal frameworks adopted when such cases occur.
National Social Security Authority (NSSA)
NSSA is a statutory corporate body established in terms of the NASSA Act (Chapter 17:04) tasked by the government to provide social security. Its mission is to provide sustainable social security and promote OHS to all its members through responsive schemes and services. The body has four departments that are, OHS promotions and training, research and development, Factory inspectorate and OHS services. This institution also works hand in hand with the Zimbabwe Occupational Health and Safety Council (ZOHSC) that is a tripartite organisation that comprises the government, employers, and labour unions.
Through its OHS services department, the body raises awareness, promote health and safety in workplaces and compensate victims of occupational accidents through its two schemes (Pension and other benefits scheme and Accident Prevention and Workers’ compensation scheme. The schemes meet all the expenses related to workplace illness and injuries such as drugs, hospital bills, transport, artificial limbs (crutches, hearing aids and dentures) and other apparatus used by people who have been physically disabled (NSSA, 2012). However, the study discovered that the National Social Security Schemes governed under NSSA have been marred by misappropriation of contributors’ funds and in the past years has been on public domain for failing to offer meaningful assistance to workers in the event of eventualities while at work. Furthermore, despite the contributions made by the employees within the public sector, the assistance rendered by NSSA in the event of accidents is rather not known. It was also observes that the public service workforce covered by under scheme is very small, currently, the employees in the civil service are not covered at all. It is thus critical that the country develop strategies targeted at workers in the public sector as they are not immune to numerous workplace health and safety hazards.
The Zimbabwe Occupational Health and Safety Council (ZOHSC)
This council is a tripartite organisation of government, employers, and trade unions. The council was established to facilitate the interaction of these three main actors to come up with OHS plans, projects and programmes that can transform the labour industry, individual organisations and employees (Taderera, 2012). Moreover, the council provides a linkage between the government and individual organisations for systematic evaluation and review of OHS policies, plans and projects emanating from the micro and macro levels (Taderera, 2012). The study established that the council has been very instrumental in the promotion of OHS in Zimbabwe through its research and the advice it renders to the minister of Public Service, Labour and Social Welfare on policy matters. In some cases, the ZOHSC also supervises the occupational health and safety activities of NSSA on behalf of the minister. The council, however, has limited capacity to carry out more groundbreaking research in OHS. This limited capacity can be addressed by collaborative work, where Tertiary institutions in the country support the council in carrying out this research.
Challenges of Implementing Standard Occupational Health and Safety Practices in Zimbabwe’s Public Sector
The study discovered several challenges that public institutions in Zimbabwe are encountering in their attempt to implement standard occupational health and safety practices. These challenges include;
A Substantial Underestimation of Occupational Illness
The underestimation of occupational illness and disease-related fatalities is possibly one of the most serious challenges impeding the implementation of standard occupational health and safety practices in Zimbabwe’s public sector. In 2020 NSSA recorded only 4574 injuries and 47 fatalities a sharp contrast to 133 000 injuries recorded by the Zimbabwe National Statistic Agency (Mhlanga, 2020). The lack of adequate surveillance systems at NSSA has led to much of the data on the disease impact of occupational risk to be drawn from ad hoc surveys that report incorrect figures. These figures present a false picture that results in a cycle of neglect as many cases go unnoticed.
Additionally, the study found out that several occupational illnesses that public workers are exposed to have been largely underestimated in formal reporting systems. These include respiratory diseases in office workers exposed to dust, communicable diseases in laboratory and health personnel, back and eye problems in office workers who spend most of their time sitting in front of computers. Without correct systematic indicative information, occupational health outcomes in the public sector will not get the attention they deserve. In fact (Mhlanga, 2020) observes that underestimating occupational health risks means they will never be considered as key factors in production decisions, when in fact they are key in determining the productivity of the public sector. Raising awareness of the costs of poor OHS conditions at the national and organisational level is, therefore, key to ensuring the prioritization of OHS issues. Awareness campaigns will act as eye-openers on the benefits that public organisations can reap from investing in the prevention of occupational fatalities and illness.
Lack of a Comprehensive and Harmonized Occupational Health and Safety Framework
The research established that the country lacks a comprehensive and harmonized OHS legal framework that covers all workplaces. It was observed that most public sector employees are not covered by OH or social legislation and they do not have access to occupational health services. Moreover, findings revealed that there is no state intervention in OHS disputes, and it remains a challenge to refer cases of incompliance to courts of law due to an inadequate understanding of judicial systems on OHS issues. There is thus needed to work on implementing coherent legal frameworks that prioritize and protect public sector employees as they are key in national development.
Inadequate Occupational Health Safety Budgeting and Staff
Findings indicated that most public institutions do not have adequate OHS budgets. In parastatals such as ZETDC for instance OHS budgets are crafted and authorized by the Human Resources Department in consultation with the Health Officer at the organisation’s headquarters. This arrangement leaves health officers in different branches with little autonomy to decide on OHS issues that may require urgent attention to that funds may need additional authorization.
The study also found out that public organisations fail to adequately allocate the human capital required to effectively implement OHS strategies needed to realize a safe work environment for their employees. For instance, at Mbare Polyclinic this study observes that one of the challenges that they were facing in the execution of their duties along with other health officers in various local clinics was inadequate staff leading to a high workload. Amongst these responsibilities include budgeting for OHS activities, initiating health and safety-related training and development, attending to the requirements of workers who would have been involved in workplace accidents, maintaining a health insurance register for all employees, and carrying out inspections on the upholding of OHS standards at the various local clinics. The government together with individual public sector organisations need to avail adequate resources required to successfully implement OHS systems to realize positive outcomes.
Weak Organisational Culture
As indicated by the Improved Accident Causation Model organisational culture is a critical factor in the success of OHS implementation. However, the findings revealed that most public sector organisations have weak OHS culture. The study established that the actualization of safety at the individual level is affecting the drive to run operations under safe most mode in most public organisations. The findings point to the fact that most public sector employees mainly care about their health and safety than those of their counterparts. As a result of this, they are generally reluctant to embrace OHS policies and safety culture as a collective. It is of paramount importance that public employees be taught that the creation of a safe and healthy working environment inclusive for all is key for development cooperation aimed at poverty reduction.
Conclusions and Recommendations
The study concluded that Zimbabwe lacks a comprehensive and harmonized occupational health and safety legal framework. Access to health and safety in the workplaces has however not matched the industrialization spur in both 1stworld and developing economies. When it comes to public sector employees the most common causes of work-related hazards within office settings emanate from prolonged physical inactivity. It has been observes that prolonged physical inactivity especially among employees who spend most of their working hours seated can lead to numerous health problems such as cardiovascular diseases, digestive problems, obesity, and reduced lung efficiency.
The public sector subscribes to the International Labour Organisation OHS conventions, NSSA Statutory Instrument 68/90 and several other statutes that concern the safety of the worker amongst them the Factories and Workers Act [Chapter 151:08] and the Occupational Health and Safety Act. These form the regulatory basis on that the public sector implements its OHS system. Further to these regulatory frameworks are the policy and institutional frameworks that act as blueprints to the operationalization of the OHS. Institutional frameworks include the Ministry of Public Service, Labour and Social welfare, National Social Security Authority, Zimbabwe Occupational Health and Safety Council (ZOHSC), Ministry of Health and Child Care (MOHCC).
One of the important pillars of a universal OSH strategy includes the adoption and implementation of a national preventative OSH protocol. New technologies, globalisation and continuous demographic shifts have produced far-reaching changes in the world of work and new challenges for the safety and health of workers (Lavicoli, 2016). According to Zwetsloot et al. (2017), the zero-accident vision is a promising approach developed in industry, but not so much addressed by the safety science research community. Policymakers in the public sector should establish policies that are easy to adopt and take account of occupational safety and health strategies. The conditions that give rise to injuries must be reflected in regulatory standards, that must be communicated to workplace parties, and enforcement strategies must be implemented to identify and address non-compliance (MA, 2016).
Occupational safety strategies should be premised on understanding a safe work environment to ensure the strategies address the right causes. Leaders need to construct a safety culture that will not collapse under the pressure of quick fixes but a culture of excellence (Saujani, 2016). A strong safety culture allows managers to make practical regulations that emphasise a harmonious relationship between humans and nature and strengthen miners’ awareness of mine safety (Chu et al., 2016). The strength of a company’s safety performance lies within the strength of its safety culture (Ali & Shariff, 2016). Ivensky (2016) concurred with Ali and Shariff (2016) and added if culture is to yield sustainable results; it must be integrated wholly and firmly within core line management instruments and the fundamental tasks of human resources management.
Improving workplace safety and health is key to organisational development and sustainability. Training may offer some potential in helping support learning, behaviour change and is consistent with feedback and development approaches used in the public sector training is an integral part of risk management for risk identification and communication between all the stakeholders including management, technical and safety personnel, Walker (2014), argued that lack of knowledge and training is a major cause of occupational accidents especially in the public sector. Educational safety programmes are therefore required to increase peoples’ knowledge by giving them a background on theories, principles and techniques for improving their future problem-solving abilities (Line&Albechrtsen, 2016).
There ought to be an independent budgetary allocation for the OHS activities outside of the Human Resources Department. The work specialisation of the proposed department of OHS requires an independent budgetary allocation that would enable for OHS specific financial planning. Such an establishment will ensure that there is an independent financial function in which the Director of OHS resides over defending OHS spending. This will also ensure that there is reduced bureaucratic tape in the attainment of approval to spend on other non-budget planned expenditures such as emergency cases. Therefore, there is a need for an independent budgetary allocation towards OHS to the OHS Department.
References
Ali, S., & Shariff, A.M.2016. An integrated conceptual framework for proactive improvement of safety culture. International Review of Management and Marketing, 6(4), 120–124.
Alli, B. O. (2001). Fundamental principles of occupational health and safety. Available at: https://www.ilo.org/wcmsp5/groups/public/@dgreports/@dcomm/@publ/documents/publication/wcms_093550.pdf
Amponsah-Tawiah, K., & Dartey-Baah, K. (2011). Occupational health and safety: Key issues and concerns in Ghana. International Journal of Business and Social Science, 2(14),119–125. https://www.researchgate.net/publication/280557400_Occupational_Health_and_Safety_Key_Issues_and_Concerns_in_Ghana
Anger, W. K., Elliot, D. L., Bodner, T., Olson, R., Rohlman, D. S., Truxillo, D. M., Montgomery, D. (2015). Effectiveness of total worker health interventions.Journal of Occupational Health Psychology, 20, 226–325.
Arab trade Union Confedaration. (2020). Occupational Health and Safety at work during the COVID-19 Pandemic. Arab trade Union Confedaration
Bailey, K. D. (1994). Methods of social research. The Free Press.
Banda, B. (2014). Assessment of OHS systems and practice in Zimbabwe. NSSA Journal, 14(8).
Brauer, T. (2006). Safety and health for engineers (2nd ed.). Wiley.
Chu, C., Jain, R., Muradian, N., & Zhang, G. (2016). Statistical analysis of coal mining safety in China with reference to the impact of technology. Journal of the Southern African Institute of Mining and Metallurgy, 116(1), 73–78.
Cooper, D. (2015). Effective safety leadership: Understanding types & styles that improve safety performance. Professional Safety, 60(2), 49. Retrieved from https://www.onepetro.org/
Dey, I. (2005). Qualitative data analysis. Routledge, Taylor and Francis Group.
Diefenbuch. (2009). New public management in public sector organisations. The dark sides of managerialistic enlightment. Public Administration, 87(4), 892–909.
Dube, S., & Danescu, D. (2011). Supplemental guidance: Public sector definition. Available at: https://global.theiia.org/standardsguidance/Public%20Documents/Public%20Sector%20Definition.pdf
Factories and Works Act. Chapter 14.08 149 Revised 1996. Government of Zimbabwe Printers.
Fu, G., Fan Y.,Tong, R., & Gong, Y. (2016). A universal methodolody for the causation analysis of accidents (4th ed.). Journal of Accident Prevention, 2(3), 7–12.
Government of Zimbabwe. (2010). Ministry of public service, labour and social welfare. www.pslsw.gov.zw
Government of Zimbabwe. (2014). Zimbabwe National occupational safety and health policy, Harare, Government Printers.
Government of Zimbabwe. Labour Act 28:01. Government Publications.
Health and Safety Laws. Available at: file:///C:/Users/thispc/Downloads/Health%20and%20Safety%20Laws%20for%20Employees%20at%20Work%20in%20Zimbabwe%20-%20Mywage.org_Zimbabwe.html.
Hall, (2013). New Public Management in Sweden: The risky balance between bureaucracy and politics in (Schmidt et al. 2017).
ILO. (2010). Guidelines on Occupational Health and Management Systems (ILO-OSH 2001). Safe work, ILO Geneva.
ILO. (2019). World day for safety and health at work. https://www.ilo.org/safework/events/safeday/lang--en/index.htm
Ivensky, V. (2016). Safety expectations: Finding a common denominator. Professional Safety, 61(7), 38–43. Retrieved from https://www.onepetro.org.
Jambwa and Chitongo. (2013). Challenges of implementing Occuptional Health and safety measures in Marondera Municipality department of works in (Muzhazha- Nyandoro and Nyaunde 2017).
Jerie, S. (2012). OHS problems among workers in the Wood industry in Mutare, Zimbabwe. Journal of Emerging Trends in Economic and Management Sciences, 3(3), 278–289.
Kim, Y., Park, J., & Park, M. (2016). Creating a culture of prevention in occupational safety and health practice. Safety and Health at Work., 7(2), 89–96.
Lavicoli, S. 2016. The new EU occupational safety and health strategic framework: 2014–2020, objectives and challenges. Occupational Medicine, 66(3). 180–182.
Line, M. B., & Albrechtsen, E. (2016). Examining the suitability of industrial safety management approaches for information security incident management. Information & Computer Security, 24(1), 20–37.
MA, Q. M. (2016). Systematic review of qualitative literature on occupational health and safety legislation and regulatory enforcement planning and implementation. Scandinavian Journal of Work, Environment & Health, 42(1), 3.
Masekameni, M. D., Moyo, D., Khoza, N., & Chamdimba, C. (2020). Accessing Occupational Health and Safety in the SADC Region. International Journal of Environmental Research of Public Health., 17, 6767. https://doi.org/10.3390/ijerph17186767
Maumbe, J.T. (2017). An analysis of the occupational health systems in the public sector. The case of Zimbabwe Electrical Transmission and Distribution Company. Available at: https://ir.uz.ac.zw/handle/10646/3986
Mazhazha-Nyandoro, Z. F., & Nyaude, D. (2017). An Evaluation of Occupational Health and Safety (OHS) and Employee well-being in the Public Sector in Zimbabwe: A case study of the Salary Service Bureau. International Journal of Research in Business Management 5(1), 41–54 Available at: https://www.academia.edu/31225970/AN_EVALUATION_OF_OCCUPATIONAL_HEALTH_AND_SAFETY_OHS_AND_EMPLOYEE_WELL_BEING
Mrema, E., Ngowi, A. V., & Mamuya, S. H. D. (2015). Status of occupational health safety and related challenges in expanding economy of Tanzania. Annals of Global Health, 81(4), 538–547.
Ministry of Health and Child Care Zimbabwe. 2012. Health promotion, trends and current status. Ministry of Health and Child Care Zimbabwe. From http://www.mohcw.gov.zw/index.php/health-promotion, August 2021.
Mhlanga, P. (2020). Sharp rise in Zim’s occupational injuries, diseases. Business Times. Available at https://businesstimes.coz.zw/sharp-rise-in-zims-occuptional-injuries-diseases/
Moyo, D., Zungu, M., Kgalamono, S., & Mwila, C. D. (2015). Review of occupational health and safety organisation in expanding economies: The case of Southern Africa. Annals of Global Health, 8(4), 495–502.
Mpofu, L. (2019). Assessment of occupational safety and health management system OHSAS 18001 on safety performance at How mine. Available at http://hdl.hamdle.net/111408/3037.
Muchiri, F. K. (2003). Occupational health and development in Africa, Challenges and the way forward. African Newsletter on Occupational Health and Safety, 1
Müezzinoğlu, A. (2015). Role of occupational physician in mining accidents. Turkish Thoracic Journal, 16(1), 21–24.
Murral, J., Davies, S. T., & Rees, D. (2011). Lung diseases in South African mining industry: Research and policy implementation. Journal of Public Health Policy, 32(1), 565–599.
Muzvidziwa-Chilunjika, S. R. T., Mutizwa, B., & Chilunjika, A. (2020). Unpacking the Impact of the COVID-19 pandemic in Zimbabwe’s Public Sector. Journal of Humanities and Social Sciences, 2(1), 93–104. National Social Security Authority 2012. Occupational health safety. Available at http://www.nssa.org.zw/pages/ohs.htm. Accessed in August 2021.
NSSA. (2012). Work safety is a must. https://www.nssa.org.safety-is-a-must/zw/uncategorised
Occupational Health Hazards. Available at: https://www.jliedu.com/blog/occupational-health-hazards/
Qian, Q., & Lin, P. 2016. Safety risk management of underground engineering in China: Progress, challenges and strategies. Journal of Rock Mechanics and Geotechnical Engineering. 8(4), 423–442.
Schmidth, L., Sjestrom J., and Antosson A., 2017. Understanding the challenges facing OHS in the Swedish public sector. Nordic Journal of Working Life Studies, 7(3).
Saujani, M. (2016). World-class safety culture: Applying the five pillars of safety. Professional Safety, 61(2), 37. Retrieved from www.asse.org
Saunders, M., Lewis, P., & Thornhill, A. (2003). Research methods for business students (3rd ed.). Pearson Education.
Statutory Instrument 68 of 1990. Act 12/189. NSSA Accident Prevention and workers compensation scheme Notice 1990. Government of Zimbabwe Printers.
Taderera, H. (2012). Occupational health safety management systems: Institutional Regulatory frameworks in Zimbabwe. International Journal of Human Resources Studies, 2(4).
Walker, S. (2014). Training: The foundation for safety. Engineering and Mining Journal, 32.
Wang, J., & Yan, M. (2019). Application of an improved model for model accident analysis. A case study. International of Environmental Research and Public Health, 162756, 1–12.
World Health Organisation. (2009). Occupational Health. The global Occupational Health network Newsletter. Available at http//www.who.int/occuptationalhealth/net/gohnet15pdf?ua=1.
ZOHSC. (1997). Comprehensive analysis of health and safety management in Zimbabwe. Mimeo Report Harare.
Zwetsloot, G. I., Kines, P., Wybo, J.-L., Ruotsala, R., Drupsteen, L., & Bezemer, R. A. (2017). Zero accident vision based strategies in organisations: Innovative perspectives. Safety Science, 91, 260–268.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Mapuvire, D.H., Chilunjika, S.R.T., Mutasa, F. (2022). The Health and Safety Perspectives in the Zimbabwe Public Sector. In: Chiware, M., Nkala, B., Chirisa, I. (eds) Transformational Human Resources Management in Zimbabwe. Springer, Singapore. https://doi.org/10.1007/978-981-19-4629-5_11
Download citation
DOI: https://doi.org/10.1007/978-981-19-4629-5_11
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-4628-8
Online ISBN: 978-981-19-4629-5
eBook Packages: Business and ManagementBusiness and Management (R0)