
Abstract
Aim
The Internet is the main source of child health information among parents of young children. The aim of this study was to evaluate how regular use of a specific child health website would influence the perceived parental self-efficacy and knowledge of Norwegian mothers with young children. We also wanted the mothers to evaluate the usefulness and user-friendliness of the study website. In addition, usage of the web site in the general population was recorded in the same period.
Subjects and methods
In this prospective survey, 99 Norwegian mothers were recruited as users of a Norwegian website (www.syktbarn.no) developed and managed by Norwegian physicians. Standardized questionnaires were used to assess background information and self-perceived parental competence before and after using the website. Forty-six mothers reported using the site regularly for 9–12 months, and after usage a questionnaire was filled out to evaluate the site’s usefulness. General usage of site was examined with Google Statistics.
Results
After usage, the mothers rated themselves with less anxiety when their child was ill (t = 2.49, p = 0.017, paired sample t-test) and with increased knowledge about childhood disease (t = −2.95, p = 0.004). More mothers claimed to know how to recognize serious disease in their child (t = −3.16, p = 0.003). More than 80 % of mothers appreciated the structure, content and usefulness of the study website. Search characteristics of the mothers were similar to those of the general population.
Conclusion
Regular usage of a child health website developed by physicians increased the self-efficacy and knowledge and reduced anxiety among Norwegian mothers of young children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Internet has become the leading source of open-access health information, and specialized websites and different types of eHealth applications have shown the potential to increase empowerment, competence and knowledge among “health-seekers” on the web (Fox 2009, 2011). Resources found on the web have been reported to have a direct effect on people’s health decisions and behavior (Allen and Rainie 2000; Wainstein et al. 2006). Young parents of today—the so-called Internet generation—are more concerned, better informed and want a more active, consumerist role than earlier generations of parents when it comes to child health (Plantin and Daneback 2009). Societal change has replaced the traditional grandmother with lots of knowledge with the Internet as the most obvious and essential source of child health information (O’Connor and Madge 2004; Rothbaum et al. 2008). Nearly all parents of young children and especially mothers with sick children use the Internet to search for child health advice and recommendations, and they want easy access to information that they can trust (Horrigan and Rainie 2002; Bernhardt and Felter 2004; Bos et al. 2008). The widespread availability of affordable broadband Internet access to an increased number of families, which reached 90 % of Norwegian households with children in 2011 (Statistics Norway 2011), has made it possible to launch instructional video clips as an integral part of Internet-based health information applications and websites.
Is health information on the Internet really helpful? In a systematic review by Fox (2009), 22 of 25 studies evaluating the beneficial value of computer-based patient education programs reported knowledge gains, a few studies reported higher patient satisfaction and seven reported no or a negative impact. The programs that included multimedia content had the highest impact. However, only three of the programs were web-based. Some programs have focused on parental management of children’s diseases, such as asthma, fever and atopic dermatitis (Homer et al. 2000; O’Neill-Murphy et al. 2001; Krishna et al. 2003; Bergmo et al. 2009). Most of these programs reported knowledge gain, and a few found additional effects on self-perceived parental competence.
We recently published a survey about the Internet habits of 99 Norwegian mothers of young children and found that the Internet is their main source for child health information (Skranes et al. 2014). During childhood sickness, most parents will search the Internet actively for useful information about what to do and when to seek medical help. Our study also showed that most mothers of young children become anxious when their child becomes sick and they feel a lack of knowledge. To our knowledge, no study has described the impact of long-term use of a specialized child health website on self-perceived parental competence. More research is also needed to investigate how consumers of web information evaluate online healthcare sites in order to gain knowledge about how to create useful and trustworthy websites.
The aim of the present study was to evaluate the impact of use of a Norwegian website about child health (www.syktbarn.no) in a representative group of Norwegian mothers with young children. We wanted to measure whether such usage would increase perceived parental competence by reducing anxiety and increasing knowledge about childhood disorders. We also wanted the mothers to evaluate the beneficial value, quality and user-friendliness of the study website. Finally, we wanted to register the usage pattern of the study website in the general public.
Materials and methods
Study population
In this survey, a convenience sample of 99 Norwegian mothers of young children were recruited for participation in a prospective follow-up study concerning the impact of usage of a newly developed open-access website focusing on child health information for parents. The participants were partly recruited based on a modified “snowball recruitment strategy,” which acted by asking current participants to refer us to other potential participants (Browne 2005). Some mothers were recruited from a group of parents participating in an intervention study performed at the Department of Pediatrics, St. Olav University Hospital in Trondheim (Botngård et al. 2013). In addition, some mothers were recruited to the study randomly from a group of mothers asking the net doctor questions on the study website. The survey started in November 2011 and ended in November 2012. The participants actively used the study website for 6–12 months.
The intervention website: www.syktbarn.no (sick child)
During the survey period the intervention website (www.syktbarn.no) was an open-access, non-commercial Norwegian online resource especially designed for parents of young children. The website contains videos, audio clips, animations, illustrations, pictures and text materials regarding children’s illnesses but also normal development. In addition, the parents can use an interactive “symptom checker,” which will help them to decide what to do and when to seek medical advice when their child is sick. The user may also use the “ask the doctor” service. A unique feature of the website is the authentic video clips of sick children with common childhood symptoms such as rashes, fever, coughing and breathing difficulties. All the content of the website was composed and developed by Norwegian pediatricians and general physicians and later reviewed by pediatricians from university hospitals in Sweden, Finland.
Methods
At baseline, i.e., before usage of the site, the participating mothers answered standardized questionnaires concerning background demographics, their use of the Internet as a source of information in general and the health status of their child/children. To evaluate self-perceived anxiety and parental competence concerning child health and what to do when their child was sick, a questionnaire with modified elements from the Perceived Health Competence Scale (PHCS) was completed by the participating mothers at baseline and after 6–12 months of using the study website. PHCS is a domain-specific measure of the degree to which an individual feels capable of effectively managing his or her health outcomes and was developed to provide a measure of perceived competence at an intermediate level of specificity with eight items combining outcome and behavioral expectancies (Shelton Smith et al. 1995). In our study, the PHCS was modified to child health, and the respondents answered 16 statements on a five-point Likert scale based on strongly disagree/agree for classifying answers; six statements reflected self-perceived anxiety, and ten statements were knowledge-related. This modified questionnaire was pre-tested on a smaller group of mothers in a focus group, but not validated. In addition, the mothers completed a standardized form evaluating the content, user-friendliness and value of the study website. All questionnaires were available in both paper versions and online surveys. To evaluate usage of the study website in the general population, we looked at the traffic and usage patterns during the period from February 2012 to November 2012. Information about the total number of visits, new versus returning visitors, demographics, access through mobile devices, visitors’ flow and most visited pages was collected.
Statistics
The results of the survey were analyzed quantitatively and qualitatively. IBM SPSS Statistics 20 for Windows was used for statistical analyses. Descriptive statistics were used to present mothers’ Internet usage and their perceived competence when their child was sick, measured before and after having used the website for at least 9 months. For variables with a normal distribution, t-tests were performed, while the Mann-Whitney U-test was used to analyze differences in ordinal or scalar variables with a non-normal distribution. To evaluate and compare results before and after usage, paired sample t-tests were performed. Three sum scores of the individual statements about self-perceived anxiety and knowledge were calculated. Two-sided P-values ≤ 0.05 were considered statistically significant. Google Analytics (version 2011, www.google.com/analytics) was used to measure usage of the study website in the general population. Google Analytics is the most widely used free-of-charge website statistics service and aims to generate detailed statistics about the usage of a website, i.e., collection and analysis of user traffic and path movement, including specific end nodes visited. Analyses of user traffic may provide a better understanding of the key issues of a web-based application, such as how it may reflect the user’s needs and its supposed impact on user adoption and behavior change.
Ethics
The Regional Committee for Medical Research Ethics approved the study protocol (project no. 2009.2203), and written informed consent was obtained from the participants.
Results
Demographic factors
Some clinical characteristics of the study participants are listed in Table 1. The mean age of participating mothers was 33.1 years (SD 5.9 years), with a mean reported age for their children of 1.6 years (SD 1.6 years). With regard to education, 46 % of mothers had finished university college (“høyskole”), and 33 % had a university degree. Thirty-two percent were single-child families, 43 % had two children, and 25 % of families included three or more children. Nineteen percent of mothers had at least one child with a chronic disorder, most often allergy or asthma (Table 1).
Change in perceived competence and anxiety after usage of the study website
Table 2 shows changes in the self-perceived parental competence, degree of care and empowerment after usage of the study website among a subsample of 46 mothers who had used the program three times or more during the study period. Significant changes were seen for answers on 4 of the 16 statements in the questionnaire and for 2 of the 3 sum scores. For the statement “I become very anxious when my child is ill,” significantly lower scores (more disagreement with the statement) were seen after usage than before (t = 2.49, p = 0.017). For the statements “I do not have control,” “I know how to test for serious disease in a child,” and “I know how to test for neck stiffness,” higher scores (more agreement) were reported after usage than before (t = −2.32, p = 0.025; t = −3.16, p = 0.003; t = −4.24, p = 0.000, respectively). No change was found for the self-perceived anxiety sum score (t = 0.04, p = 0.972), while the two sum scores for knowledge increased after usage of the study web site (t = −2.08, p = 0.041 and t = −2.95, p = 0.004) (Table 2).
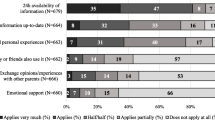
Evaluation of the website by the participating mothers
The results of the evaluation of the website are presented in Table 3. Sixty-two mothers (63 %) responded to the evaluation form, and for the content and usefulness of the site, 90 % or more of the mothers agreed on the following statements: “The site gave a good explanation for my child’s symptoms,” “After using the site, I know if the child’s illness is severe,” “The site gave me useful information about childhood disorders,” “I trust the information/advice that I get from the site,” “The site seems trustworthy and professional in design,” “The site gives simple and easy understandable advice,” “I think it’s easy to follow the advice given,” and “I think the site has a large utility value.” Ninety-one percent of mothers disagreed with the statement “I don’t know how to follow the advice from the site.” With regard to the site structure, 90 % or more of the participants agreed on the following: “I think the content is simple and easy-to-follow,” “The site is easy to navigate,” “The video clips increase learning outcome,” and “I quickly find the material that I am searching for.” All users denied that the site was too technical for them to use.
Free text answers: favorite aspects of the site and reasons for use
When the mothers were asked what they liked best about the website, the responders focused on both the structure and content of the site (Table 4). Nearly all responded that the site was easy to use and gave clear answers to their questions. Major content benefits were the multimedia material (video clips, sound files and photos), indicated by 76 % of responses, and the ask-the-doctor service, reported by 72 % of the responders. A third of the mothers also said that it was important that the site was developed and managed by physicians and therefore had professional and trustworthy content. About a quarter of the mothers emphasized the symptom-checker service was useful (Table 4). When asked for the most common medical reasons for using the website, the most frequently reported answers were: upper and lower airway infections (46 %), acute gastroenteritis (12 %), rashes (12 %), fever (7 %) and asthma/allergy in 6 % of responders (Table 5).
Free text answers: suggestions for improvement
Approximately a fourth of the responders had suggestions for improving the site, which mainly included additional content about allergies, different types of rashes and psychomotor development in older children. Two responders suggested that the site structure site should be improved.
General usage of the study web site
From 12 February to 12 November 2012 (9 months), the study website had a total of 229,111 visits, varying from 23,000 visits per month during the initial months after opening the site to 35,000 visits during the later months. Most visits occurred on Mondays and Sundays (about 1,300 per day) and the least on Fridays and Saturdays (about 900 per day). About three of four visits were new visitors, while the remaining 25 % were made by returning visitors (n = 57,000); the latter number increased during the last 3 months of registration. Of the returning visitors, about half of them had visited the site twice, and the rest had visited three or more times. Visitors to the site came from 128 countries, with 62 % of users coming from Norway, 33 % from Sweden and about 1 % from the USA. Across the entire time period, mobile usage of the site comprised 43 % of visits, increasing to 48 % for the last 2 months. Regarding mobile device information, an iPhone was used by 45 %, iPad by 31 % and Samsung Galaxy by about 9 % of users. When looking at visitors’ flow, about 1/3 started on the site’s home page, while 15 % entered the exanthema/rashes section first. The large majority of users (92 %) accessed the website through the Google search engine, and the mean number of pages viewed by each visitor was 2.7 pages. The most popular topics of the website were: exanthema/rashes (11 %), the symptom checker (9 %) and the opening home page (3 %).
Discussion
Increased parental competence after usage
The mothers reported less anxiety after using the website in our study. Most parents become anxious when their child gets sick (Parkinson et al. 1999) and may feel helpless about what to do and how to provide support to their sick child (Kai 1996). Parental anxiety may be transmitted to the child and worsen coping skills (Kain et al. 1996). However, studies report that highly educated parents are less anxious and have greater empowerment that those with lower levels of education (Scrimin et al. 2009), which may explain why the mothers in our study feel more secure after usage. The mothers also reported more disagreement with the statement “I always measure the temperature for fever” after using the website. This may indicate less anxiety about fevers and more knowledge about the advantages of running a fever during a childhood infection. Similar findings were reported in two studies measuring the effects on parental anxiety about fever after the use of parental education programs on fever (Impicciatore et al. 1997; O’Neill-Murphy et al. 2001). The study website emphasizes the beneficial effects of fever and that a child in general good health does not need fever-reducing medicine. After usage of the study website, the mothers claimed to have more competence when their child was sick and more knowledge about severe childhood diseases.
More mothers knew how to test for neck stiffness in case of infectious meningitis. Two of the major challenges that parents are faced with when their child gets sick are to separate mild from severe disease and to decide when to contact the doctor. Studies have shown that parents want sufficient information about the child’s symptoms and illness so that they can know how to handle and assess the severity of an illness with regard to when to seek medical advice (Kai 1996). Early detection of symptoms and signs leading to diagnosis and early treatment is critical for a successful recovery and to reduce morbidity, complications and death from severe acute illnesses such as meningitis and septicemia in children. Educating parents on how to observe and detect such signs is therefore of utmost importance, and a professional website with authentic videos and a doctor’s voice, like the study website offers, may be a useful resource.
Evaluation of the study website
Based on their self-reports, the mothers were very satisfied with the study website regarding both the content and structure of the site. They especially appreciated the multimedia content, but also the user-friendliness of the site. They thought the language used was easy to comprehend, and none claimed that the site was too technical to handle. One challenge for young parents is to evaluate the quality of the websites that they enter after an Internet search, i.e., to what degree to trust the credibility of the content (Roberts and Copeland 2001). In a systemic review of 79 studies investigating the quality of health-related web-based information, the authors reported that 70 % of the studies concluded that quality was a problem for the websites investigated (Eysenbach et al. 2002). In a recent report, Knapp et al. (2011) found that only half of the Internet users in the survey reported that they were able to tell high- from low-quality online resources. Many parents therefore express a wish for guidance by doctors and easier access to websites that they know they can trust (Tuffrey and Finlay 2002; Wainstein et al. 2006; Khoo et al. 2008). In our study, many of the mothers reported that they depended on the site’s content because it was developed by medical doctors. This is in agreement with other studies showing that the most trusted sources of health information are physicians and nurses (Bernhardt and Felter 2004; Hesse et al. 2005). Mothers of young children consider organizational websites run by not-for-profit entities and websites run by universities, hospitals and medical centers as examples of sites where they can find reliable content, although many complain that information on such sites tends to be too academic and difficult to understand (Bernhardt and Felter 2004). This may partly explain why such websites have had limited success in reaching the general public (Kind et al. 2004). In addition, such sites tend to focus on disease-specific information, while parents of sick children need symptom-based information, which is more difficult to find on the web (Tuffrey and Finlay 2002).
Previous studies have shown that low literacy may hinder the active use of the Internet for gathering health information and limit the beneficial effects on knowledge gain and empowerment (Ronsman and Rootman 2004). However, one of the major advantages of today’s widely distributed broadband Internet service is the possibility of presenting multimedia content with easy real-time streaming of video clips and sound files. A website that presents videos of real symptoms and childhood illnesses, sound files and animations together with video interviews of doctors explaining medical issues may be more accessible for viewers with low literacy. In our study, these elements, together with language simplicity, were emphasized as some of the major advantages of the health information given on the website. We speculate that multimedia-based eHealth applications may be a valuable tool in reducing the effects of low literacy on child health management in parental groups.
The “ask the doctor” service was among the most popular elements of the study website. This is in agreement with a Swedish study in which the participants, mostly women, appreciated such a service because it was convenient and flexible and they could reflect on the written answer given by the net doctor (Umefjord et al. 2006).
General usage of the study web site
The study website received most visitors on Sunday and Monday and the least on Friday and Saturday. This finding was consistent throughout the whole registration period. We do not know whether this is typical for most websites with child health information content, but we speculate that this may be due to a larger tolerance among parents of childhood sickness at the start of the weekend, hoping that the child will be healthy again when the weekend is over. Common infections in children are a huge burden on parents’ work absences and on children’s time lost from kindergarten and school (McConnochie et al. 2009). The increased number of visits to the study website on Sunday and Monday may be due to the fact that many parents then have to decide whether to be absent from work the following day because of a sick child or whether the child is healthy enough to go to kindergarten or school. Typical topics that were searched for using Google were: rashes, coughing, fever and signs of severe disease. Similar topics also raised great interest among the mothers in the study. Since sick children present with symptoms, not with diagnoses, health websites should focus more on symptom-based information than fact sheets about different diseases (Khoo et al. 2008). About 25 % of visitors had used the study website several times, which may indicate the usefulness of site. It is interesting that about half of the visitors entered the site via mobile devices such as an iPhone and iPad. To our knowledge such large usage of mobile devices for health information has not been reported before, with the Pew Research Center reporting mobile access to the Internet for 39 % of the adult US population in 2010 as a comparison (Smith 2010). We therefore speculate that the use of mobile devices for self-care health information and empowerment will be the main future trend in eHealth development toward stronger needs-led and consumer-oriented healthcare (Bos et al. 2008).
Limitations of study
There are some limitations of this study that may influence the generalization of the results to mothers of young children more generally. The mothers participating in this study were mostly recruited from urban areas, and most of them were well educated. This may have created a selection bias, since studies have shown that socioeconomic factors such as education, income and housing location influence Internet habits and the degree to which an individual’s increased knowledge and skills actually create changes in empowerment and health-promoting behavior and practice (Heymann et al. 2005). However, within the total study group there was no correlation between Internet use and education (Skranes et al. 2014). In addition, studies have reported that searching for health information seems more independent of socioeconomic factors than general Internet usage (Plantin and Daneback 2009), especially with the digital divide narrowing over time because of the increased use of mobile devices and broadband access to a more diverse population (Fox 2011; Knapp et al. 2011). Also, when comparing the usage of the study website in the general population to the pattern reported by our study participants, we found several similarities that strengthen the generalizability of our results. Both groups entered the study site mainly via search engines and searched for symptom-based information. In fact, “rashes and coughing” was the most popular topic in both groups.
The strength of the study was that all interviews were done by the same investigator and that the study had a prospective design, reducing the chance of recall bias. Only 46 of the 99 recruited mothers had used the site more than twice during the study period and thereby had their answers on the modified PHCS after usage registered, which may have created a selection bias. However, when comparing demographic factors for those who answered and non-responders, we did not find any differences in maternal age, number of children or educational level (data not shown). A high attrition rate is common in web-based intervention studies (Wangberg et al. 2008; Christensen et al. 2009; van der Zanden et al. 2012), and in our study some mothers reported lack of use of the site simply because their children had been healthy during the whole study period. During the intervention period, the participating mothers may have received support from several other sources as well, including the maternity health clinic, childbirth education, social networks and other parenting websites. Therefore, we cannot be sure that the improvement in parental competence and reduced anxiety reported in the study period is only due to website usage; however, the mothers claimed a beneficial effect of using the site when their child was sick. Another weakness is the lack of validation of the modified PHCS questionnaire.
Conclusions and clinical implications
Regular use of a website about child health developed by experienced physicians enhanced perceived parental competence, reduced anxiety and increased knowledge among Norwegian mothers of young children. Websites combining high-quality trustworthy medical content and with a high degree of user-friendliness may be valuable tools for self-education and increased empowerment of parents of sick children. The traditional health services should contribute to and appreciate the development of eHealth applications that have the potential to improve public health and self-care, thereby tempering the problem of waiting lists and rising healthcare costs (McConnochie et al. 2005; van der Zanden et al. 2012). Physicians should keep themselves updated on available high-quality child health websites and recommend them to parents, while encouraging families to avoid inappropriate websites (Bernhardt and Felter 2004).
References
Allen K, Rainie L (2000) Parents online. Pew Internet & American Life Project. http://www.pewinternet.org/reports/oldmedia/Files/Reports/pdfs/PIP_Parents_Reports.pdf. Accessed 20 October
Bergmo TS, Wangberg SC, Schopf TR, Solvoll T (2009) Web-based consultations for parents of children with atopic dermatitis: results of a randomized controlled trial. Acta Paediatr 98:316–320
Bernhardt JM, Felter EM (2004) Online pediatric information seeking among mothers of young children: results from a qualitative study using focus groups. J Med Internet Res 6:e7
Bos L, Carroll D, Marsh A (2008) The impatient patient. Stud Health Technol Inform 137:1–13
Botngård A, Skranes LP, Skranes J, Døllner H (2013) Multimedia based health information to parents in a pediatric acute ward: a randomized controlled trial. Patient Educ Couns 93:389–393
Browne K (2005) Snowball sampling: using social networks to research non-heterosexual women. Int J Soc Res Methodol 8:47–60
Christensen H, Griffiths KM, Farrer L (2009) Adherence in Internet interventions for anxiety and depression. J Med Internet Res 11:e13
Eysenbach G, Powell J, Kuss O, Sa ER (2002) Empirical studies assessing the quality of health information for consumers on the world wide web: a systematic review. JAMA 20:2691–2700
Fox MP (2009) A systematic review of the literature reporting on studies that examined the impact of interactive, computer-based patient education programs. Patient Educ Couns 77:6–13
Fox S (2011) The social life of health information. Pew Internet & American Life Project. http://www.pewinternet.org/files/old-media/Files/Reports/2011/PIP_Social_Life_of_Health_Info.pdf. Accessed 20 October 2013
Hesse BW, Nelson DE, Kreps GL, Croyle RT, Arora NK, Rimer BK, Viswanath K (2005) Trust and sources of health information: the impact of the Internet and its implications for health care providers: findings from the first Health Information National Trends Survey. Arch Intern Med 165:2618–2624
Heymann J, Hertzman C, Barer M, Evans R (2005) Healthier societies: from analysis to action. Oxford University Press, Oxford
Homer C, Susskind O, Alpert HR, Ms O, Schneider L, Rappaport LA, Rubin DH (2000) An evaluation of an innovative multimedia educational software program for asthma management: report of a randomized, controlled trial. Pediatrics 106:210–215
Horrigan J, Rainie L (2002) The Broadband Difference: How online behavior changes with high-speed Internet connections. Pew Internet & American Life Project. http://www.pewinternet.org/pdfs/PIP_Political_Info_Report.pdf. Accessed 21 October 2013
Impicciatore P, Pandolfini C, Casella N, Bonati M (1997) Reliability of health information for the public on the World Wide Web: systematic survey of advice on managing fever in children at home. BMJ 314:1875–1879
Kai J (1996) Parents’ difficulties and information needs in coping with acute illness in preschool children: a qualitative study. BMJ 313:987–990
Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV (1996) Preoperative anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med 150:1238–1245
Khoo K, Bolt P, Babl FE, Jury S, Goldman RD (2008) Health information seeking by parents in the Internet age. J Paediatr Child Health 44:419–423
Kind T, Wheeler KL, Robinson B, Cabana MD (2004) Do the leading children’s hospitals have quality web sites? A description of children’s hospital web sites. J Med Internet Res 6:e20
Knapp C, Madden V, Wang H, Sloyer P, Shenkman E (2011) Internet use and eHealth literacy of low-income parents whose children have special health care needs. J Med Internet Res 13:e75
Krishna S, Francisco BD, Balas EA, König P, Graff GR, Madsen RW (2003) Internet-enabled interactive multimedia asthma education program: a randomized trial. Pediatrics 111:503–510
McConnochie KM, Wood NE, Kitzman HJ, Herendeen NE, Roy J, Roghmann KJ (2005) Telemedicine reduces absence resulting from illness in urban child care: evaluation of an innovation. Pediatrics 115:1273–1282
McConnochie KM, Wood NE, Herendeen NE, Ng PK, Noyes K, Wang H, Roghmann KJ (2009) Acute illness care patterns change with use of telemedicine. Pediatrics 123:989–995
O’Connor H, Madge C (2004) My mum’s thirty years out of date: the role of the Internet in the transition to motherhood. Commun Work Fam 3:351–369
O’Neill-Murphy K, Liebman M, Barnsteiner JH (2001) Fever education: does it reduce parent fever anxiety? Pediatr Emerg Care 17:47–51
Parkinson GW, Gordon KE, Camfield CS, Fitzpatrick EA (1999) Anxiety in parents of young febrile children in a pediatric emergency department: why is it elevated? Clin Pediatr (Phila) 38:219–226
Plantin L, Daneback K (2009) Parenthood, information and support on the Internet. A literature review of research on parents and professionals online. BMC Fam Pract 10:34
Roberts JM, Copeland KL (2001) Clinical websites are currently dangerous to health. Int J Med Inform 62:181–187
Ronsman B, Rootman I (2004) Literacy: one of the most important determinants of health today. In: Raphael D (ed) Social determinants of health: Canadian perspectives, 1st edn. Canadian Scholars Press, Toronto, pp 155–170
Rothbaum F, Martland N, Jannsen JB (2008) Parents’ reliance on the Web to find information about children and families: socio-economic differences in use, skills and satisfaction. J Appl Dev Psychol 29:118–128
Scrimin S, Haynes M, Altoe G, Bornstein MH, Axia G (2009) Anxiety and stress in mothers and fathers in the 24 h after their child’s surgery. Child Care Health Dev 35:227–233
Shelton Smith M, Wallston KA, Smith CA (1995) The development and validation of the perceived health competence scale. Health Educ Res 10:51–64
Skranes LP, Løhaugen GCC, Botngård A, Skranes J (2014) Internet use among mothers of young children in Norway—a survey of Internet habits and perceived parental competence when caring for a sick child. J Publ Health 22:423–431
Smith A (2010) Mobile Access 2010. Pew Internet & American Life Project. http://www.pewinternet.org/2010/07/07/mobile-access-2010/. Accessed 22 October 2013
Statistics Norway (2011) Online report—the information society 2011. http://www.ssb.no/a/english/aarbok/tab/tab-441.html. Accessed 3 January 2014
Tuffrey C, Finlay F (2002) Use of the Internet by parents of paediatric outpatients. Arch Dis Child 87:534–536
Umefjord G, Hamberg K, Malker H, Petersson G (2006) The use of an Internet-based ask the doctor service involving family physicians: evaluation by a web survey. Fam Pract 23:159–166
van der Zanden R, Kramer J, Gerrits R, Cuijpers P (2012) Effectiveness of an online group course for depression in adolescents and young adults: a randomized trial. J Med Internet Res 14:e86
Wainstein BK, Sterling-Levis K, Baker SA, Taitz J, Brydon M (2006) Use of the Internet by parents of paediatric patients. J Paediatr Child Health 42:528–532
Wangberg SC, Bergmo TS, Johansen JAK (2008) Adherence in Internet-based interventions. Pat Pref Adher 2:57–65
Acknowledgments
The authors would like to thank the mothers who participated in the study. We thank research assistant Karen Kam Sripada, Medical Faculty, NTNU, Trondheim, Norway, for editing the language of the manuscript. The study was funded by The Research Council of Norway (Business PhD program), the Norwegian University of Science and Technology and the Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology.
Conflicts of interest
Two of the authors (LPS and JS) are the founders of the study website. This website is non-commercial (i.e., no advertising) with membership access for the general public. Otherwise, the authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Skranes, L.P., Løhaugen, G.C.C. & Skranes, J. A child health information website developed by physicians: the impact of use on perceived parental anxiety and competence of Norwegian mothers. J Public Health 23, 77–85 (2015). https://doi.org/10.1007/s10389-015-0659-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-015-0659-6