
Abstract
Trace- and macro-chemical elements are crucial for cellular physiological functioning, and their alterations in biological fluids might be associated with an underlying pathological state. Hence, this study aimed to examine and summarize the published literature concerning the application of salivary ionomics for caries diagnosis. An extensive search of studies was conducted using PubMed, EMBASE, Web of Science, and Scopus, without any language and year restriction for answering the following PECO question: “In subjects (i.e., children, adolescents, or adults) with good systematic health, are there any variations in the salivary concentrations of trace- or macro-elements between caries-free (CF) individuals and caries-active (CA) subjects?” A modified version of the QUADOMICS tool was used to assess the quality of the included studies. The Review Manager Version 5.4.1. was used for data analyses. The analysis of salivary chemical elements that significantly differed between CF and CA subjects was also performed. Thirty-four studies were included, involving 2299 CA and 1669 CF subjects, having an age range from 3 to 64 years in over 16 countries. The meta-analysis revealed a statistically significant difference (p < 0.05) in the salivary levels of calcium, phosphorus, chloride, magnesium, potassium, sodium, and zinc between CA and CF subjects, suggesting higher levels of calcium, phosphorus, potassium, and sodium in CF subjects while higher levels of chloride, magnesium, and zinc in CA patients. Half of the included studies (17/34) were considered high quality, while the remaining half were considered medium quality. Only zinc and chloride ions were found to be higher significantly and consistent in CF and CA subjects, respectively. Conflicting outcomes were observed for all other salivary chemical elements including aluminum, bromine, calcium, copper, fluoride, iron, potassium, magnesium, manganese, sodium, ammonia, nitrite, nitrate, phosphorus, lead, selenium, and sulfate ions.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Dental caries is a dynamic, multifactorial, sugar-driven, and biofilm-modulated oral condition that leads to the phasic demineralization and remineralization of tooth hard tissues [1]. The equilibrium between protective and pathological determinants affects the beginning and progression of the disease [2]. This interaction between the determinants establishes the categorization of persons and groups into caries susceptible classes, permitting an increasingly tailored procedure to care [3]. Caries can develop throughout life, both in permanent and primary dentitions, and can deteriorate the tooth crown and, later in life, exposed root surfaces [4]. The prevalence of caries is considered to have hiked recently in children aged between 2 and 5 years globally, making this age group a global priority action area [1]. Caries is a preventable, however, unevenly distributed condition having significant quality-of-life and economic burdens [5]. Hence, the early diagnosis and prevention of caries is imperative considering the disease as a serious health problem that affects a large population of adults and children worldwide [6].
Salivary diagnostics has remarkable potential as an efficient approach for the early diagnosis, prognostication, and monitoring of the post-therapy status of several oral and systemic conditions [7,8,9]. Saliva is a complex body fluid containing an entire library of biomolecules including microbiota, metabolites, proteins, microRNA, mRNA, DNA, and ions [10]. The several benefits of saliva as a clinical tool over tissues and serum include: (a) association with levels in the blood; (b) greater sensitivity; (c) easy transportation and storage; (d) cost-effectiveness; (e) good cooperation with subjects; (f) smaller sample quantity; and (g) non-invasive sample collection [7]. Hence, the saliva represents a promising source to discover and validate biomarkers [11]. Although several clinical utilities of salivary diagnostics are available presently, the deficiency of definite biomarkers for caries and user-friendly, inexpensive, and portable approaches still prevent salivary diagnostics from being entirely clinically translated.
The ionome is defined as “the mineral nutrient and trace element constituents of an organism, representing the inorganic ingredient of cellular and organismal systems” [12]. Ionomics, the study of the ionome, deals with the simultaneous and quantitative measurement of the elemental composition of living organisms and alterations in this composition as a result of genetic modifications, developmental state, and physiological stimuli [12]. Some elements, known as macro-elements, are imperative for human life, and they are required in greater amounts, since they modulate vital biological processes including enzymatic catalysis, cellular signaling, and hormone production (for instance sodium, potassium, calcium, and magnesium). Other elements, called trace elements, are needed in minute amounts including iodine, selenium, iron, and zinc [13]. Over the past few years, Ionomics has been used to study human pathological and physiological states [14, 15]. The disturbance of equilibrium in these elements has been persistently correlated with human conditions including periodontitis [16], cancer [17], neurodegenerative diseases [18], diabetes mellitus [19], and caries [20].
Recently, research trends have been aimed toward the investigation of salivary ionomics regarding dental caries considering that the imbalance of macro-elements, as well as trace elements, could be associated with the process of caries development and/or progression. To the authors’ knowledge, no systematic review has been performed till today, hence the current review aimed to summarize the published literature concerning the application of salivary ionomics for caries diagnosis. Furthermore, a methodological evaluation of the included articles’ quality was conducted for assessing the risk of bias (RoB) and favoring the standardization of future studies related to the field.
Materials and methods
Study protocol and registration
The protocol of this systematic review was registered with the Open Science Framework (OSF) Registries (https://doi.org/10.17605/OSF.IO/FD27X). This systematic review was performed as per the Cochrane Handbook and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline principles [21, 22].
Focused question
The focused question was devised utilizing the principle of Population (P), Exposure (E), the appropriate Comparator or Control (C), and the Outcome of interest (O): “In subjects (i.e., children, adolescents, or adults) with good systematic health, are there any variations in the salivary concentrations of trace- or macro-elements between caries-free (CF) individuals and caries-active (CA) subjects?”.
Population (P): Systematically healthy individuals.
Exposure (E): Subjects with a confirmed diagnosis of caries.
Control/Comparison (C): Individuals without any carious lesion.
Outcome of interest (O): Variations in the salivary concentration of trace- or macro-elements between CF and CA subjects.
Inclusion and exclusion criteria
Original human research having an observational methodological design (i.e., cohort, case–control, and cross-sectional) reporting data regarding salivary chemical elements. Both retrospective and prospective investigations were included. The study was deemed eligible if it used any of the following indices for the detection of caries: (a) the Nyvad system; (b) the Ekstrand–Ricketts–Kidd system; (c) the International Caries Detection and Assessment System (ICDAS); and (d) the Decayed, Missing, Filled Teeth (DMFT)/Decayed, Missing, Filled Surfaces (DMFS) indices.
The exclusion criteria comprised: (a) articles having no control group (CF subjects); and (b) literature reviews, clinical case reports, letters to editors, animal studies, and in vitro studies.
Information sources and screening procedure
Two authors (A.A.A. and F.A.) independently conducted a thorough and independent search in four electronic databases (i.e., Google Scholar, Web of Science, Scopus, and PubMed/MEDLINE), without any language and year restriction. All searches were undertaken from the earliest date available until 31 September 2022. Moreover, a manual search was performed for screening the bibliographies of the included articles for relevant studies. Any disagreement was resolved by discussion.
Keywords, MeSH terms, and other free terms regarding the “dental caries” and “ionomics” were utilized with Boolean operators (AND, OR) to combine searches. The search methodology included suitable alterations in the keywords and followed the syntax rules of the individual search engine. Supplementary Table 1 depicts the different combinations of terms/keywords used for the literature search. A reference management software (EndNote X6; Thomson Reuter) was used to import the obtained studies, which were consequently screened for removing the duplicates. Authors of the included articles were contacted in case of any clarification or missing data.
Study selection
Independent and thorough screening of the titles and abstracts was conducted by two authors (A.A.A. and F.A.). The full texts of the potentially eligible articles were downloaded for independent evaluation by the same authors. After analyzing the full text, the reason to exclude the articles was noted. In case of disagreement, a third investigator (M.K.A.) was consulted.
Data extraction and data items
After formulating a data collection form, a pilot study was conducted to test the data extraction. The critical data from the included articles were collected by two authors (A.A.A. and F.A.). Data extraction consisted of the following items: (1) pre-sampling methods, i.e., restriction and timing; (2) saliva collection method, i.e., saliva type, amount, and sampling time; (3) pre-analytical methods, i.e., sample storage, sample preparation, and detection method; (4) sample size; including case and control groups; (5) age range of the subjects; (6) caries index used; and (7) salivary concentration of the mineral(s) examined in CA and CF subjects. In the case of a study that compared the CF and CA subjects with and without any particular medical condition (i.e., diabetes mellitus), only the data of the systematically healthy subjects were gathered.
Quality assessment and risk of bias in the included studies
The quality assessment and the RoB in the included studies were performed independently by two authors (A.A.A. and F.A.) as part of the data extraction procedure utilizing a modified version of the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies and the QUADOMICS tool [11, 23]. This tool, formulated to assess quality issues regarding omics investigations, contains thirteen items particularly addressed to assess the research question, study cohort, exposure, outcomes, and statistics. Each item was assigned either 1 or 0 point, and subsequently, articles were rated on the basis of their total score. The interpretation of the final scores was as follow: 0–3 = very low quality; 4–6 = low quality; 7–10 = medium quality; and ≥ 11 = high quality.
Data synthesis strategy
The Review Manager (Version 5.4.1, The Cochrane Collaboration, 2020) was used to conduct the meta-analysis. For each study, the standardized mean difference (SMD) and 95% confidence interval (CI) were recorded to show the variations in salivary concentrations of different ions between CA and CF subjects. To assess the pooled SMD significance, the Z test was employed; and a p < 0.05 was considered statistically significant. For assessing the heterogeneity, the I2 statistic and Cochrane Q test were applied. The investigation of publication bias was carried out through a funnel plot utilizing the Egger’s and Begg’s tests.
The salivary concentration of chemical element(s) was originally reported as median (minimum–maximum), median (interquartile range [IQR]), or mean ± standard deviation (SD). The authors attempted to convert the salivary concentration of individual chemical elements to mean ± SD utilizing the same unit of measurement (mg/L) for allowing comparisons. When data were recorded as median (minimum–maximum) or median (IQR), the respective mean and SD were recorded as per the procedure described by Hozo and colleagues [24]. Moreover, we have presented an analysis of salivary chemical elements that significantly differed between CF and CA subjects.
Results
Screening process outcomes
Figure 1 shows the PRISMA flowchart of the article selection procedure. After searching all four electronic search engines complemented with manual searching and removing duplicate studies, 971 studies were found. After evaluating titles and abstracts together with full texts, 59 studies were evaluated for eligibility. Then, 25 studies were excluded due to the following reasons: (a) studies which had different aims than the present study (n = 10) [25,26,27,28,29,30,31,32,33,34]; (b) studies which used the biological sample fluid other than saliva (i.e., blood) (n = 09) [35,36,37,38,39,40,41,42,43]; (c) studies which failed to mention any caries detection method (n = 03) [44,45,46]; (d) studies which did not contain any control group (n = 02) [47, 48]; and (3) study published in Chinese language (n = 01) [49]. Finally, 34 studies were included in the present systematic review [20, 50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82].

Flow chart of literature search and selection criteria adapted from the PRISMA
General characteristics of the included studies
Table 1 depicts the general characteristics of the included studies. Ten studies were conducted in India [50, 52, 53, 62, 63, 65, 73, 74, 76, 77], followed by Brazil (n = 3) [20, 61, 79], Iran (n = 3) [59, 75, 81], Iraq (n = 3) [54, 64, 66], China (n = 2) [57, 60], Israel (n = 2) [72, 78], the USA (n = 2) [58, 82], while Colombia [68], Denmark [55], Finland [70], Italy [51], Japan [71], Kosovo [56], Romania [80], Turkey [69], and Ukraine [67] contributed to one study each. A total of 3968 subjects (range: 28 [78]–527 [71]) were recruited in the included studies, out of which 2299 were CA and 1669 were CF, having an age range from 3 [20, 52, 53, 75, 81] to 64 [65] years for the participants of both study groups. Four studies compared the concentration of different salivary chemical elements between CF and CA subjects with and without conditions including dental erosion [55], periodontitis [63], diabetes mellitus [65], and familial dysautonomia [78].
Table 2 summarizes the pre-sampling, saliva collection, and pre-analytical methods. around 44% (15/34) of the included studies did not mention details about pre-sampling methods, while only 44% (15/34) studies reported saliva collection timings. Non-stimulated saliva was collected as the sample biological medium in around 59% (20/34) of the studies, followed by stimulated saliva (21%; 7/34), mixed saliva (18%; 6/33), while 1 study failed to report the type of saliva collected [53]. The amount of saliva collected among the included studies ranged between 50 uL and 20 mL, while nearly 1/3rd of the included studies (11/34) did not report the amount of saliva collected. Around half of the included studies (53%; 18/34) performed saliva collection procedure between 08:00 a.m. and 12:00 p.m., one study collected saliva between 01:00 and 03:00 p.m., while the other half of the included studies did not report time of saliva collection. Around 56% (19/34) of the studies reported sample preparation methods, and a wide range of variation was noticed regarding sample storage temperature, i.e., 4 ℃, − 18 ℃ − 20 ℃, − 80 ℃. The identification approaches were primarily based on the salivary chemical element being investigated. Atomic absorption spectrophotometry was the most utilized detection method and was employed for the identification of several salivary chemical elements including calcium, chloride, copper, iron, potassium, magnesium, manganese, sodium, lead, phosphate, and zinc. All the included studies performed targeted analysis (i.e., identified particular salivary chemical elements), while no study conducted untargeted analysis (maximizing discovery of salivary chemical element[s] using a broad-spectrum analysis).
Across the 34 included studies, the analysis of 19 different salivary chemical elements was performed including aluminum, bromine, calcium, chloride, copper, fluoride, iron, potassium, magnesium, manganese, sodium, ammonia, nitrite, nitrate, phosphorus, lead, selenium, sulfate, and zinc. The most frequently analyzed elements was calcium (n = 19), followed by phosphorus (n = 16), copper (n = 8), potassium (n = 8), fluoride (n = 7), iron (n = 7), sodium (n = 7), zinc (n = 6), and chloride (n = 6) (Table 3). Interestingly, the diagnostic accuracy of these elements was not measured in any included study.
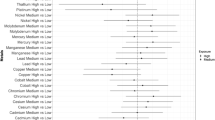
Changes in salivary elemental profiles in caries and healthy subjects
According to Fig. 2, a consistent and significantly higher trend was revealed by zinc and chloride in CF and CA subjects in 4 varying studies each, respectively. The salivary concentrations of zinc ranged between 0.0586 ± 0.0122 mg/L and 123.3 ± 17.9 mg/L in CF and between 0.049 ± 0.017 mg/L and 1.7 ± 0.7 mg/L in CA subjects, whereas the salivary levels of chloride ranged between 193.7 ± 98.2 mg/L and 1126 ± 222.5 mg/L in CF and 263.5 ± 142.4 mg/L and 1181.5 ± 222.5 mg/L in CA subjects.

Analysis of significantly increased salivary chemical elements in caries-free and caries-active subjects
Controversial outcomes were observed for all other salivary chemical elements. For salivary calcium, phosphorus, and copper, 11/13, 5/7, and 3/5 reports revealed significantly higher trends in CF individuals, respectively, whereas inverse tendency (i.e., higher salivary levels in CA patients) was observed in the remaining studies. The salivary concentrations of calcium, phosphorus, and copper ranged between 2.342 ± 0.698 mg/L and 357.7 ± 43.82 mg/L, 4.197 ± 0.468 mg/L and 738 ± 252 mg/L, and 0.0038 ± 0.0041 mg/L and 0.53 ± 0.15 mg/L in CF individuals, respectively, whereas their salivary levels in CA subjects ranged between 4.828 ± 0.660 mg/L and 267.5 ± 19.63 mg/L, 2.795 ± 0.641 mg/L and 673.2 ± 91.8 mg/L, and 0.002 ± 0.0027 mg/L and 0.35 ± 0.10 mg/L, respectively. For salivary iron, fluoride, sodium, and potassium, 5/7, 3/5, 3/4, and 2/3 reports demonstrated significantly higher trends in CA patients, respectively, whereas inverse tendency (i.e., higher salivary levels in CF subjects) was noticed in the remaining studies. The salivary levels of iron, fluoride, sodium, and potassium ranged between 0.0034 ± 0.0079 mg/L and 5.84 ± 3.21 mg/L, 0.011 ± 0.010 mg/L and 30 ± 20 mg/L, 79.36 ± 38.88 mg/L and 3420 ± 1620 mg/L, and 94.6 ± 48.3 mg/L and 1070 ± 205 mg/L in CF individuals, respectively, whereas their salivary levels in CA subjects ranged between 0.0058 ± 0.0012 mg/L and 8.61 ± 1.10 mg/L, 0.0042 ± 0.0023 mg/L and 0.27 ± 0.01 mg/L, 106.24 ± 68.25 mg/L and 2520 ± 1620 mg/L, and 123.7 ± 39.2 mg/L and 8000 ± 170 mg/L, respectively. Conflicting outcomes were observed regarding magnesium, whose salivary concentrations were greater in CF subjects according to one study, while another report revealed the higher salivary levels of magnesium in CA patients. Salivary levels of magnesium ranged between 3.15 ± 2.40 mg/L and 21.6 ± 12.6 mg/L in CF subjects, and between 3.86 ± 2.12 mg/L and 21.6 ± 12.6 mg/L in CA subjects. Since the analysis of other ions, including manganese, lead, ammonium, sulfate, bromide, nitrite, and nitrate, was performed in one study each, hence, their comparison was not possible. However, the salivary concentration of manganese, lead, ammonium, sulfate, and bromide ions, was revealed to be higher in CA patients than in CF subjects, while the salivary levels of nitrate and nitrate ions were found to be greater in CF subjects than CA patients.
Quality assessment
Table 4 depicts the outcomes of the methodological quality evaluation utilizing the QUADOMICS method. Only 6 studies (18%) were considered high quality, while the remaining 28 studies (82%) were graded as high quality. The least reported items in the included studies were: (a) intermediate/uninterpretable test outcomes reported (0%); (b) measurement and adjustment of potential confounding factors (12%); (c) sample size calculation (24%); (d) description of methods and timing of biological specimen collection related to clinical factors (53%); and (e) sample handling and pre-analytical methods (56%).
Synthesis of results
Figure 3 depicts the salivary concentration of calcium in CF and CA subjects. For salivary calcium levels, outcomes demonstrated an SMD of − 0.34% (95% CI − 0.44, − 0.24; p < 0.00001), indicating a statistically significant difference between CF and CA subjects (i.e., higher salivary levels of calcium in CF subjects). Moreover, a great amount of heterogeneity was observed (calcium: I2 = 95%; p < 0.00001).

Forrest plot of salivary levels of calcium in caries-free and caries-active subjects
Figure 4 depicts the salivary concentration of phosphorus in CF and CA subjects. For salivary phosphorus levels, outcomes demonstrated an SMD of − 0.29% (95% CI − 0.40, − 0.18; p < 0.00001), indicating a statistically significant difference between CF and CA subjects (i.e., higher salivary levels of phosphorus in CF subjects). Moreover, a great amount of heterogeneity was observed (phosphorus: I2 = 90%; p < 0.00001).

Forrest plot of salivary levels of phosphorus in caries-free and caries-active subjects
Figure 5 depicts the salivary concentration of chloride, magnesium, and manganese in CF and CA subjects. For salivary chloride (Fig. 5A) and magnesium (Fig. 5B) levels, outcomes demonstrated an SMD of 0.49% (95% CI 0.36, 0.61; p < 0.00001) and 0.20% (95% CI 0.01, 0.38; p < 0.03), respectively, suggesting a statistically significant difference between CF and CA subjects (i.e., higher salivary levels of chloride and magnesium in CA patients). Moreover, a great amount of heterogeneity was observed regarding the salivary levels of chloride (chloride: I2 = 95%; p < 0.001), while no statistically significant heterogeneity was observed for salivary levels of magnesium (magnesium: I2 = 59%; p < 0.06). However, for salivary levels of manganese (Fig. 5C), outcomes revealed an SMD of 0.06% (95% CI − 0.10, 0.22; p = 0.47), indicating that the salivary concentration of chloride and magnesium did not differ statistically between CF and CA subjects. Moreover, a great amount of heterogeneity was observed (manganese: I2 = 90%; p < 0.001).

Forrest plot of salivary levels of A chloride; B magnesium; and C manganese in caries-free and caries-active subjects
Figure 6 depicts the salivary concentration of potassium, sodium, and zinc in CF and CA subjects. For salivary potassium (Fig. 6A) and sodium (Fig. 6B) levels, outcomes demonstrated an SMD of 0.26% (95% CI 0.14, 0.38; p < 0.0001) and 0.27% (95% CI 0.15, 0.39; p < 0.001), respectively, suggesting a statistically significant difference between CF and CA subjects (i.e., higher salivary levels of potassium and sodium in CF subjects). Moreover, a great amount of heterogeneity was observed (potassium: I2 = 96%; p < 0.00001 and sodium: I2 = 89%; p < 0.00001). For salivary zinc (Fig. 6C) levels, outcomes demonstrated an SMD of − 0.26% (95% CI − 0.42, − 0.09; p < 0.002), suggesting a statistically significant difference between CF and CA subjects (i.e., higher salivary levels of zinc in CA patients). Moreover, a great amount of heterogeneity was observed (zinc: I2 = 92%; p < 0.00001).

Forrest plot of salivary levels of A potassium; B sodium; and C zinc in caries-free and caries-active subjects
Figure 7 depicts the salivary concentration of fluoride in CF and CA subjects. For salivary fluoride levels, outcomes demonstrated an SMD of − 0.94% (95% CI − 2.11, 0.23; p = 0.12), indicating a statistically non-significant difference between CF and CA subjects. Moreover, a great amount of heterogeneity was observed (calcium: I2 = 98%; p < 0.00001).

Forrest plot of salivary levels of fluoride in caries-free and caries-active subjects
Publication bias
The funnel plots demonstrated no significant publication bias, since no significant asymmetry was identified (Supplementary File).
Discussion
The effect of salivary chemical elements on caries prevalence is a controversial subject. However, sufficient evidence has been gathered for suggesting that it is a topic that justifies an expanding and continuing research effort [83]. This systematic review is one of its kind to assess the profile of trace- and macro-elements in the saliva of CF and CA individuals. In the present review, findings for 19 different elements were reported from 34 included studies.
Findings of particular elements
The majority of the included studies revealed that the salivary levels of calcium were significantly higher in CF subjects than in CA patients. This finding is in agreement with the studies conducted by Shaw et al. [84], Tulunoglu et al. [69], Tayab et al. [85], Singh et al. [86], and Preethi et al. [87]. High salivary calcium levels may result in remineralization of incipient caries reducing the rate of caries. The saliva acts as a reservoir supersaturated with phosphate and calcium that generates an environment favoring remineralization over demineralization. However, two studies reported higher salivary calcium levels in CA patients in comparison with CF subjects, which agreed with the findings revealed by a study performed by Borella et al. [51]. According to Borella et al. [51], higher salivary levels of calcium were related to the increased caries severity. The positive association between caries and higher calcium salivary levels might be attributed to that the principle salivary inorganic ingredients, i.e., hydrogen, phosphate, and calcium ions, along with fluoride, have an imperative role regarding the solubility of tooth minerals. Any reduction in salivary pH will result in undersaturation of saliva to hydroxyapatite causing its degradation into their ionic ingredients for increasing the gradient level. Hence, inorganic phosphate and calcium ions are diffused into saliva from the tooth [51].
The salivary levels of phosphorus were found to be significantly higher in CF subjects as compared to CA patients in most of the included studies. This finding is consistent with the outcomes of the studies conducted by Singh et al. [86], and Shaw et al. [84]. This outcome might be suggestive of the protective function of phosphorus against caries. The negative association of salivary phosphorus with caries might be owing to its cariostatic action via its buffering capacity in saliva [88] and its capability of maintaining the saturation of saliva with phosphate ions [89]. Phosphate might interfere with the attachment of plaque bacteria and enamel pellicle to the enamel surface, together with inhibiting bacterial growth [90].
The present review found that the salivary levels of iron were significantly higher in CA subjects than CF individuals in the majority of the included studies. Iron is an indispensable trace element for bacterial metabolic functions and can mediate the microbial community of the host via affecting processes including caries [91]. The absorption of iron via bacteria preferentially utilizes Fe2+ and Fe3+ ions which are present in low concentrations on mucosal surfaces because of the attachment of iron to salivary glycoproteins, including transferrin and lactoferrin or intracellularly, related to ferritin or heme compounds, producing an effective host defense mechanism against bacterial growth. On the contrary, microorganisms have formed specialized mechanisms for sequestering iron from host proteins, generating iron-chelating molecules known as siderophores [92]. These compounds change iron solubility in the extracellular medium and aid its absorption into the bacteria. This mechanism permits the survival of bacteria even in iron-deficient conditions [91]. Two of the included studies reported a higher level of salivary iron in CF subjects as compared to CA patients. Caries is related to increased inflammatory response and a consequent reduction in hemoglobin concentrations [93]. As such, the synthesis of cytokines is reduced, which ultimately inhibits erythropoiesis [94].
The fluoride levels in saliva differ as per the concentration and amount of fluoride ingested, either by topical or systemic route [64]. Salivary fluoride levels were found to be significantly higher in CA patients than CF subjects in most of the included studies, indicating that saliva is not the only determinant of caries development. Contrarily, a study conducted by Zero [95] reported that a higher level of salivary fluoride was statistically associated with a lower risk of caries, suggesting that further research is required to assess the association of salivary fluoride levels with caries.
In the present review, the levels of salivary zinc and copper were found to be significantly higher in CF subjects as compared to CA patients in almost all included studies. It is well-established how zinc and copper functions are closely associated, being vital ingredients of antioxidant enzymes, such as copper–zinc superoxide dismutase [96]. Furthermore, salivary histatins are made up of copper and are relevant antimicrobial enzymes in the oral cavity [97]. Hence, higher levels of salivary copper may suggest that either histatins and/or copper–zinc superoxide dismutase are not functioning properly.
The salivary levels of several inorganic elements, such as sodium, potassium, magnesium, and chloride, were revealed to be significantly higher in CA patients than in CF subjects in the majority of the included studies. The acid-induced enamel demineralization can enhance a more considerable mobilization of saliva electrolytes owing to the increased mineral dissolution and the release of inorganic elements (sodium, calcium, potassium, magnesium, and chloride) [98]. On the contrary, saliva is also recognized as a buffering pool that may shift the dynamic equilibrium between remineralization and demineralization to modulate caries activity [99]. Moreover, an antibacterial function of sodium is also recognized, potentially indicating its high level in saliva as a defense mechanism [100].
The salivary levels of other ions, such as nitrate, nitrite, bromide, and ammonium, in CA and CF subjects were assessed in only one of the included studies. The findings revealed that the nitrate and nitrite ions were higher in the saliva of CF subjects, while higher levels of salivary bromide and ammonium ions were found in CA subjects. In the oral cavity, nitrate is primarily transported to the salivary glands via the action of nitrate reductase, then it is rapidly reduced to nitrite. These salts are quickly acidified upon their encounter with certain bacteria, including Streptococcus mutans, Actinomyces, and Lactobacillus, which are associated with caries [101]. Bromide ion has vital functions in the activation of α-amylase and synthesis of collagen-IV in saliva [102]. Ammonia, generated by arginine-rich protein, plays a crucial part to maintain a neutral pH in the oral cavity [103].
Critical analysis of methodological issues
Salivary concentrations of macro- and trace elements have been conventionally assessed utilizing varying approaches, including gamma-ray spectrometry, thermal neutron activation analysis, potentiometry, inductively coupled plasma optical emission spectrometry, and atomic absorption spectrometry. Particularly, the most frequently utilized method in ionomics is inductively coupled plasma mass spectrometry, since it permits accurate and rapid routine multi-element identification with enhanced sensitivity for biological samples [104]. Recognizing the high heterogeneity of outcomes for individual element concentration, the application of varying detection approaches might be a critical factor.
Standardizing the sampling methods, according to collection timing, home oral hygiene, and dietary restrictions, is of utmost significance [23]. If the desired analyte is primarily secreted by a particular gland, gathering saliva from that specific gland’s glands would be the most appropriate sampling approach. However, it is important for the user, whether a clinician or researcher, to note that this collection method is invasive and requires specialized devices. Sampling whole saliva is a more convenient and rapid method compared to collecting glandular saliva. Despite the lower concentration of analytes in whole saliva, enhancing its performance in analysis can be achieved through pre-concentration techniques. Choosing between collecting stimulated and unstimulated saliva is crucial due to the impact of exogenous and endogenous factors, as well as salivary parameters, such as pH and flow rate, on the composition of saliva. For instance, unstimulated saliva is less influenced by flow rate and pH, but typically yields smaller sample volumes compared to stimulated saliva collection. Nevertheless, stimulated samples tend to be more diluted, so the decision between collecting stimulated or unstimulated saliva depends primarily on the specific analyte being targeted. Therefore, due to the various factors that can impact salivary secretion and composition, it is imperative to establish a precise standard for saliva collection to obtain reliable and comparable data. The selection of the sampling device also relies on the specific analyte being considered. The scientific literature indicates variations in the performance of commercial devices in terms of recovering the targeted analyte. For instance, the cotton swab used in Salivette® exhibits a notable interaction with biological molecules. As there is no established standard, it is essential to take into account the interplay between collection methods, saliva types, and devices, emphasizing the need for careful consideration beforehand [105]. Moreover, seasonal and circadian changes are of primary significance while the interpretation of the results from ions and metabolites in saliva [106]. Finally, differences in sample sizes and racial background may also be associated with a high variability [107].
The saliva/dental plaque interface
After consuming sugar, a cariogenic challenge initiates a series of diverse processes at four interconnected yet physically distinct locations. As a result, multiple events occur simultaneously and interact with each other in various locations: within the saliva, at the interface between saliva and plaque, within the plaque itself, and within the enamel [108]. Collins and Dawes [109] demonstrated that the remaining amount of fluid in the oral cavity, if distributed evenly across its inner surface, would create a film of approximately 100 um thickness. Research conducted by Lecomte and Dawes [110] and independently by Weatherell et al. [111] suggests that the interaction between the salivary film and the bulk saliva is highly dependent on the specific location.
The bulk saliva is supersaturated with phosphate and calcium ions, which might constantly precipitate on the surface of the tooth in the absent of any control [112]. Neyraud and Dransfield [113] found that bulk saliva consisted of around 1 mM ionized calcium and around 5 mM total calcium. In low-salivary flow subjects, total calcium in parotid saliva reduced with flow rate and pH; however, in high-salivary flow subjects, calcium increased with pH and was not associated with salivary flow rate [114]. Nevertheless, both total and ionized calcium increased with flow rate of parotid saliva [115]. Therefore, it seems that the wide range of values reported for calcium ions in saliva is owing to the differences in the location of saliva collection, the salivary gland, the degree, the type of stimulation, and the probable contribution of salivary flow rate, which might be associated with the size of the gland [116].
Conclusion and future perspectives
Although ionomics is a rapidly growing field, however, our comprehension of the association between the salivary concentration of different elements and caries risk is still limited. In this review, the authors have critically analyzed the published literature regarding ionomics as a new approach for improving the early diagnosis, prevention, treatment, and prognosis of caries. Substantial reduction and assimilation of big data resulting from high-throughput approaches are greatly required for successfully translating biochemical profiles into clinical utility. When considerable variations in salivary trace- and macro-elements among subjects will become clear, a micro-fluidic chair-side test might be formulated for the early diagnosis and/or assessing the clinical advancement of the therapy. Owing to great concerns to develop portable, non-invasive, and accurate diagnostic methods for population-based approaches and individual utility, the outcomes from the current review suggest a dire need for identifying and quantifying trace- and macro-salivary chemical elements for caries by providing methods of diagnostic accuracy.
In conclusion, only zinc and chloride ions were found to be significantly and consistently higher in CF and CA subjects, respectively. Conflicting outcomes were observed for all other salivary chemical elements including aluminum, bromine, calcium, copper, fluoride, iron, potassium, magnesium, manganese, sodium, ammonia, nitrite, nitrate, phosphorus, lead, selenium, and sulfate ions.
Data availability
The data used to support the findings are all included in the article.
References
Ahmad P, Hussain A, Carrasco-Labra A, Siqueira WL. Salivary proteins as dental caries biomarkers: a systematic review. Caries Res. 2022. https://doi.org/10.1159/000526942.
Moussa DG, Ahmad P, Mansour TA, Siqueira WL. Current state and challenges of the global outcomes of dental caries research in the meta-omics era. Front Cell Infect Microbiol. 2022;12:682.
Arshad AI, Ahmad P, Dummer PM, Alam MK, Asif JA, Mahmood Z, Abd Rahman N, Mamat N. Citation classics on dental caries: a systematic review. Eur J Dent. 2020;14(01):128–43.
Pitts N, Zero D. White paper on dental caries prevention and management. FDI World Dent Fed. 2016. https://doi.org/10.1007/978-3-319-30552-3_1.
Frencken JE, Sharma P, Stenhouse L, Green D, Laverty D, Dietrich T. Global epidemiology of dental caries and severe periodontitis–a comprehensive review. J Clin Periodontol. 2017;44:S94–105.
Cummins D. Dental caries: a disease which remains a public health concern in the 21st century–the exploration of a breakthrough technology for caries prevention. J Clin Dent. 2013;24:A1–14.
Malathi N, Mythili S, Vasanthi HR. Salivary diagnostics: a brief review. ISRN Dent. 2014;2014:158786.
Giannobile WV, Beikler T, Kinney JS, Ramseier CA, Morelli T, Wong DT. Saliva as a diagnostic tool for periodontal disease: current state and future directions. Periodontol. 2000;2009(50):52–64.
Asa’ad F, Fiore M, Alfieri A, Pigatto PDM, Franchi C, Berti E, Maiorana C, Damiani G. Saliva as a future field in psoriasis research. BioMed Res Int. 2018;2018:7290913.
Buduneli N. Environmental factors and periodontal microbiome. Periodontol. 2000;2021(85):112–25.
Baima G, Iaderosa G, Citterio F, Grossi S, Romano F, Berta GN, Buduneli N, Aimetti M. Salivary metabolomics for the diagnosis of periodontal diseases: a systematic review with methodological quality assessment. Metabolomics. 2021;17:1–21.
Salt DE, Baxter I, Lahner B. Ionomics and the study of the plant ionome. Annu Rev Plant Biol. 2008;59:709–33.
Chellan P, Sadler PJ. The elements of life and medicines. Phil Trans R Soc A. 2015;373:20140182.
Sun L, Yu Y, Huang T, An P, Yu D, Yu Z, Li H, Sheng H, Cai L, Xue J. Associations between ionomic profile and metabolic abnormalities in human population. PLoS One. 2012;7: e38845.
Hansen AF, Simić A, Åsvold BO, Romundstad PR, Midthjell K, Syversen T, Flaten TP. Trace elements in early phase type 2 diabetes mellitus—a population-based study. The HUNT study in Norway. J Trace Elem Med Biol. 2017;40:46–53.
Baima G, Iaderosa G, Corana M, Romano F, Citterio F, Giacomino A, Berta GN, Aimetti M. Macro and trace elements signature of periodontitis in saliva: a systematic review with quality assessment of ionomics studies. J Periodont Res. 2022;57:30–40.
Callejon-Leblic B, Gómez-Ariza JL, Pereira-Vega A, Garcia-Barrera T. Metal dyshomeostasis based biomarkers of lung cancer using human biofluids. Metallomics. 2018;10:1444–51.
Stefano F, Cinzia N, Marco P, Marco G, Rita G, Augusto F, Rosita G. Hair microelement profile as a prognostic tool in Parkinson’s disease. Toxics. 2016;4:27.
Peruzzu A, Solinas G, Asara Y, Forte G, Bocca B, Tolu F, Malaguarnera L, Montella A, Madeddu R. Association of trace elements with lipid profiles and glycaemic control in patients with type 1 diabetes mellitus in northern Sardinia, Italy: an observational study. Chemosphere. 2015;132:101–7.
Poletto AC, Singi P, Barri RM, Casanova AA, Garbelini CCD, da Silva CC, Venancio EJ. Relationship of levels of trace elements in saliva and dental caries in preschool children using total reflection X-ray fluorescence technique (TXRF). J Trace Elem Med Biol. 2021;63: 126663.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10:1–11.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Baima G, Corana M, Iaderosa G, Romano F, Citterio F, Meoni G, Tenori L, Aimetti M. Metabolomics of gingival crevicular fluid to identify biomarkers for periodontitis: a systematic review with meta-analysis. J Periodont Res. 2021;56:633–45.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:1–10.
Watanabe K, Tanaka T, Shigemi T, Saeki K, Fujita Y, Morikawa K, Nakashima H, Takahashi S, Watanabe S, Maki K. Al and Fe levels in mixed saliva of children related to elution behavior from teeth and restorations. J Trace Elem Med Biol. 2011;25:143–8.
Anand S, Masih U, Yeluri R. Comparative quantitative assessments of salivary ion activity product for hydroxyapatite and buffering capacity in children with different caries experience. J Clin Pediatr Dent. 2016;40:480–5.
Karshan M. Do calcium and phosphorus in saliva differ significantly in caries-free and active-caries groups? J Dent Res. 1942;21:83–6.
Sharma A, Subramaniam P. Association of salivary zinc levels to dental caries and body mass index. A comparative study. J Clin Pediatr Dent. 2021;45:265–8.
Dogra S, Bhayya D, Arora R, Singh D, Thakur D. Evaluation of physio-chemical properties of saliva and comparison of its relation with dental caries. J Indian Soc Pedod Prev Dent. 2013;31:221–4.
Oktysyuk Y, Rozhko M, Bazalytska O. Correction of mineral methabolism of saliva in children affected by dental caries. Farmatsija. 2017;64:40–5.
Klitynska OV, Stishkovskyy AV, Hasiuk NV, Avetikov DS, Ivaskevych VZ. Statistical analysis of the impact of clusters on caries prevalence and intensity in children aged 6–7 with different somatic health statuses. Wiad Lek. 2020;73:434–40.
Sejdini M, Berisha N, Citaku E. Determination and influence of saliva calcium and magnesium in children with different intensity of caries. J Int Dent Med Res. 2018;11:51–6.
Mungia R, Cano SM, Johnson DA, Dang H, Brown JP. Interaction of age and specific saliva component output on caries. Aging Clin Exp Res. 2008;20:503–8.
Costa EM, Azevedo JAPd, Martins RFM, Rodrigues VP, Alves CMC, Ribeiro CCC, Thomaz EBAF. Salivary iron (Fe) ion levels, serum markers of anemia and caries activity in pregnant women. Rev Bras de Ginecol e Obstet. 2017;39:94–101.
Subhadharsini S. Serum zinc level in dental caries patients. Int J Pharm Sci Rev Res. 2015;35:19–20.
Shaoul R, Gaitini L, Kharouba J, Darawshi G, Maor I, Somri M. The association of childhood iron deficiency anaemia with severe dental caries. Acta Paediatr. 2012;101:e76–9.
Jayakumar A, Gurunathan D. Estimation of ferritin levels in children with and without early childhood caries-A case–control study. J Adv Pharm Educ Res. 2017;7:15–7.
Flink H, Tegelberg Å, Sörensen S. Hyposalivation and iron stores among individuals with and without active dental caries. Acta Odontol Scand. 2000;58:265–71.
Koppal PI, Sakri MR, Akkareddy B, Hinduja DM, Gangolli RA, Patil BC. Iron deficiency in young children: a risk marker for early childhood caries. Int J Clin Pediatr Dent. 2013;6:1–6.
Flink H, Tegelberg Å, Thörn M, Lagerlöf F. Effect of oral iron supplementation on unstimulated salivary flow rate: a randomized, double-blind, placebo-controlled trial. J Oral Pathol Med. 2006;35:540–7.
Shamsaddin H, Jahanimoghadam F, Poureslami H, Haghdoost AA. The association between growth factors and blood factors with early childhood caries. J Oral Health Oral Epidemiol. 2017;6:196–202.
Schroth RJ, Levi J, Kliewer E, Friel J, Moffatt ME. Association between iron status, iron deficiency anaemia, and severe early childhood caries: a case–control study. BMC Pediatr. 2013;13:1–7.
Shannon IL. Parotid fluid flow rate, parotid fluid, and serum inorganic phosphate concentrations as related to dental caries status in man. J Dent Res. 1964;43:1029–38.
Dawes C, Jenkins G. Some inorganic constituents of dental plaque and their relationship to early calculus formation and caries. Arch Oral Biol. 1962;7:161–72.
Karshan M. Factors in saliva correlated with dental caries. J Dent Res. 1939;18:395–407.
Becks H, Wainwright W, Young D. Further studies of the calcium and phosphorus content of resting and activated saliva of caries-free and caries-active individuals. J Dent Res. 1943;22:139–46.
Shannon IL, Feller R. Parotid saliva flow rate, calcium, phosphorus, and magnesium concentrations in relation to dental caries experience in children. Pediatr Dent. 1979;1:16–20.
Zipkin I, Bullock F, Mantel N. The relation of salivary sodium, potassium, solids and ash concentration to dental caries experience in children, 5 to 6 and 12 to 14 years of age. J Dent Res. 1957;36:525–31.
Hiraishi N, Tanaka M, Takagi Y. The relationship between inorganic ion composition of saliva and dental caries prevalence in children. Kokubyo Gakkai Zasshi. 1999;66:249–53.
Duggal M, Chawla H, Curzon M. A study of the relationship between trace elements in saliva and dental caries in children. Arch Oral Biol. 1991;36:881–4.
Borella P, Fantuzzi G, Aggazzotti G. Trace elements in saliva and dental caries in young adults. Sci Total Environ. 1994;153:219–24.
Sekhri P, Sandhu M, Sachdev V, Chopra R. Estimation of trace elements in mixed saliva of caries free and caries active children. J Clin Pediatr Dent. 2018;42:135–9.
Kotian N, Gurunathan D. Estimation of salivary ferritin in children with childhood caries–a cross sectional study. Braz Dent Sci. 2021;24:1–6.
Hussein AS, Salih BA, Al-Nasir MG. The association of salivary calcium, inorganic phosphorus, zinc and copper in children and early childhood caries: a case-control study. J Oral Dent Res. 2017;4:110–9.
Bardow A, Lykkeaa J, Qvist V, Ekstrand K, Twetman S, Fiehn N-E. Saliva composition in three selected groups with normal stimulated salivary flow rates, but yet major differences in caries experience and dental erosion. Acta Odontol Scand. 2014;72:466–73.
Sejdini M, Meqa K, Berisha N, Çitaku E, Aliu N, Krasniqi S, Salihu S. The effect of Ca and Mg concentrations and quantity and their correlation with caries intensity in school-age children. Int J Dent. 2018;2018:2759040.
Zhang Y, Huang S, Jia S, Sun Z, Li S, Li F, Zhang L, Lu J, Tan K, Teng F. The predictive power of saliva electrolytes exceeds that of saliva microbiomes in diagnosing early childhood caries. J Oral Microbiol. 2021;13:1921486.
Shannon IL. Salivary sodium, potassium, and chloride levels in subjects classified as to dental caries experience. J Dent Res. 1958;37:401–6.
Mollaasadollah F, Bakhshi M, Namdari M, Papi Z, Shabestari SB. Relationship of chemical composition of saliva, body mass index, and nutrition with permanent first molar caries in 6–12 years old. Open Access Maced J Med Sci. 2020;8:42–7.
Zhou J, Jiang N, Wang Z, Li L, Zhang J, Ma R, Nie H, Li Z. Influences of pH and iron concentration on the salivary microbiome in individual humans with and without caries. Appl Environ Microbiol. 2017;83:e02412-e2416.
de Oliveira Buche B, Gusso B, Torres MF, Dalledone M, de Paiva Bertoli FM, de Souza JF, Pizzatto E, Brancher JA. Association between decrease in salivary iron levels and caries experience in children. Rev Odonto Cienc. 2017;32:94–8.
Pandey P, Reddy NV, Rao VAP, Saxena A, Chaudhary C. Estimation of salivary flow rate, pH, buffer capacity, calcium, total protein content and total antioxidant capacity in relation to dental caries severity, age and gender. Contemp Clin Dent. 2015;6:S65–71.
Rajesh K, Zareena SH, Kumar MA. Assessment of salivary calcium, phosphate, magnesium, pH, and flow rate in healthy subjects, periodontitis, and dental caries. Contemp Clin Dent. 2015;6:461–5.
Abbas MJ, Al-Hadithi HK, Mahmood MA-K, Hussein HM. Comparison of some salivary characteristics in iraqi children with early childhood caries (Ecc) and children without early childhood caries. Clin Cosmet Investig Dent. 2020;12:541–50.
Uk A, Hegde U, Ayas M. Role of salivary electrolytes in prevalence of dental caries among diabetic and non-diabetic adults. J Clin Diagnostic Res. 2018;12:5–8.
Kadoum NA, Salih BA. Selected salivary constituents, physical properties and nutritional status in relation to dental caries among 4–5 year’ s old children (comparative study). J Baghdad Coll Dent. 2014;26:150–6.
Bilyschuk L, Keniuk A, Goncharuk-Khomyn M, Yavuz I. Association between saliva quantity and content parameters with caries Intensity levels: a cross-sectional study among subcarpathian children. Pesqui Bras Odontopediatr Clín Integr. 2020;19: e5048.
Angarita-Díaz MP, Simon-Soro A, Forero D, Balcázar F, Sarmiento L, Romero E, Mira A. Evaluation of possible biomarkers for caries risk in children 6 to 12 years of age. J Oral Microbiol. 2021;13:1956219.
Tulunoglu Ö, Demirtas S, Tulunoglu I. Total antioxidant levels of saliva in children related to caries, age, and gender. Int J Paediatr Dent. 2006;16:186–91.
Turtola L. Salivary fluoride and calcium concentrations, and their relationship to the secretion of saliva and caries experience. Eur J Oral Sci. 1977;85:535–41.
Watanabe K, Tanaka T, Shigemi T, Hayashida Y, Maki K. Mn and Cu concentrations in mixed saliva of elementary school children in relation to sex, age, and dental caries. J Trace Elem Med Biol. 2009;23:93–9.
Gedalia I, Yardeni J, Gershon I. Dental caries rate and fluoride content of dental calculus and saliva. J Am Dent Assoc. 1963;66:525–8.
Rajkumaar J, Mathew MG. Association of severe early childhood caries with salivary ferritin. J Family Med Prim Care. 2020;9:3991–3.
Zahir S, Sarkar S. Study of trace elements in mixed saliva of caries free and caries active children. J Indian Soc Pedod Prev Dent. 2006;24:27–9.
Shahrabi M, Nikfarjam J, Alikhani A, Akhoundi N, Ashtiani M, Seraj B. A comparison of salivary calcium, phosphate, and alkaline phosphatase in children with severe, moderate caries, and caries free in Tehran’s kindergartens. J Indian Soc Pedod Prev Dent. 2008;26:74–7.
Vijayaprasad K, Ravichandra K, Vasa A, Suzan S. Relation of salivary calcium, phosphorus and alkaline phosphatase with the incidence of dental caries in children. J Indian Soc Pedod Prev Dent. 2010;28:156–61.
Kaur A, Kwatra K, Kamboj P. Evaluation of non-microbial salivary caries activity parameters and salivary biochemical indicators in predicting dental caries. J Indian Soc Pedod Prev Dent. 2012;30:212–7.
Mass E, Gadoth N, Harell D, Wolff A. Can salivary composition and high flow rate explain the low caries rate in children with familial dysautonomia? Pediatr Dent. 2002;24:581–6.
de Oliveira BB. Estimation of the salivary iron in children with dental caries: a pilot study. Iran J Public Health. 2016;45:1083–4.
Oancea R, Bonte D, Podariu AC, Rosianu RS, Tampa M, Matei C. Evaluation of salivary biochemical parameters in caries free and caries active children. Rev Chim. 2014;65:1200–4.
Bagherian A, Asadikaram G. Comparison of some salivary characteristics between children with and without early childhood caries. Indian J Dent Res. 2012;23:628–32.
Dodds MW, Johnson DA, Mobley CC, Hattaway KM. Parotid saliva protein profiles in caries-free and caries-active adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 1997;83:244–51.
Losee FL, Ludwig TG. Trace elements and caries. J Dent Res. 1970;49:1229–35.
Shaw L, Murray J, Burchell C, Best J. Calcium and phosphorus content of plaque and saliva in relation to dental caries. Caries Res. 1983;17:543–8.
Tayab T, Rai K, Kumari A. Evaluating the physicochemical properties and inorganic elements of saliva in caries-free and caries-active children. An in vivo study. Eur J Paediatr Dent. 2012;13:107–12.
Singh S, Sharma A, Sood P, Sood A, Zaidi I, Sinha A. Saliva as a prediction tool for dental caries: an in vivo study. J Oral Biol Craniofac Res. 2015;5:59–64.
Preethi B, Dodawad APR. Evaluation of flow rate, pH, buffering capacity, calcium total protein, total antioxident levels of saliva in caries free and caries active children-an invivo study. Indian J Clin Biochem. 2010;25:425–8.
Englander HR, Shklair IL, Fosdick LS. The effects of saliva on the pH and lactate concentration in dental plaques: I. Caries-rampant individuals. J Dent Res. 1959;38:848–53.
Edgar M, Higham SM. Saliva and the control of plaque pH. Br Dent J. 1996;10:81–94.
Dawes C. Factors influencing salivary flow rate and composition. Br Dent J. 1996;3:32–49.
Wang R, Kaplan A, Guo L, Shi W, Zhou X, Lux R, He X. The influence of iron availability on human salivary microbial community composition. Microbial Ecol. 2012;64:152–61.
Rolerson E, Swick A, Newlon L, Palmer C, Pan Y, Keeshan B, Spatafora G. The SloR/Dlg metalloregulator modulates Streptococcus mutans virulence gene expression. J Bacteriol. 2006;188:5033–44.
Schroth RJ, Pierce A, Rodd C, Mittermuller BA, Moffatt ME. Improvement in iron and iron-related nutritional status following pediatric dental surgery to treat severe early childhood caries. Pediatr Dent. 2022;44:58–66.
Miguel J, Bowen W, Pearson S. Effects of frequency of exposure to iron-sucrose on the incidence of dental caries in desalivated rats. Caries Res. 1997;31:238–43.
Zero DT. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health. 2006;6:S9.
Thomas B, Ramesh A, Suresh S, Prasad BR. A comparative evaluation of antioxidant enzymes and selenium in the serum of periodontitis patients with diabetes mellitus type 2. Contemp Clin Dent. 2013;4:176–80.
Melino S, Santone C, Di Nardo P, Sarkar B. Histatins: Salivary peptides with copper (II)-and zinc (II)-binding motifs: perspectives for biomedical applications. FEBS J. 2014;281:657–72.
LeGeros R. Calcium phosphates in enamel, dentin and bone. Monogr Oral Sci. 1991;15:1–201.
de Sousa ET, Lima-Holanda AT, Nobre-dos-Santos M. Changes in the salivary electrolytic dynamic after sucrose exposure in children with early childhood caries. Sci Rep. 2020;10:1–8.
Natarajan K, Gayathri R, Vishnu P. Analysis of electrolytes in saliva of periodontitis and healthy individuals. Int J Pharm Sci Rev Res. 2016;41:12–4.
Duncan C, Dougall H, Johnston P, Green S, Brogan R, Leifert C, Smith L, Golden M, Benjamin N. Chemical generation of nitric oxide in the mouth from the enterosalivary circulation of dietary nitrate. Nat Med. 1995;1:546–51.
Novo DLR, Mello JE, Rondan FS, Henn AS, Mello PA, Mesko MF. Bromine and iodine determination in human saliva: challenges in the development of an accurate method. Talanta. 2019;191:415–21.
Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of saliva and dental plaque in the dynamic process of demineralization and remineralization (part 1). J Clin Pediatr Dent. 2004;28:47–52.
Donati GL, Amais RS, Williams CB. Recent advances in inductively coupled plasma optical emission spectrometry. J Anal At Spectrom. 2017;32:1283–96.
Bellagambi FG, Lomonaco T, Salvo P, Vivaldi F, Hangouët M, Ghimenti S, Biagini D, Di Francesco F, Fuoco R, Errachid A. Saliva sampling: Methods and devices. An overview. Trac-Trends Anal Chem. 2020;124: 115781.
Romano F, Meoni G, Manavella V, Baima G, Mariani GM, Cacciatore S, Tenori L, Aimetti M. Effect of non-surgical periodontal therapy on salivary metabolic fingerprint of generalized chronic periodontitis using nuclear magnetic resonance spectroscopy. Arch Oral Biol. 2019;97:208–14.
Tahmasebi H, Asgari S, Hall A, Higgins V, Chowdhury A, Thompson R, Bohn MK, Macri J, Adeli K. Influence of ethnicity on biochemical markers of health and disease in the CALIPER cohort of healthy children and adolescents. Clin Chem Lab Med. 2020;58:605–17.
Dibdin GH. Plaque fluid and diffusion: study of the cariogenic challenge by computer modeling. J Dent Res. 1990;69:1324–31.
Collins LM, Dawes C. The surface area of the adult human mouth and thickness of the salivary film covering the teeth and oral mucosa. J Dent Res. 1987;66:1300–2.
Lecomte P, Dawes C. The influence of salivary flow rate on diffusion of potassium chloride from artificial plaque at different sites in the mouth. J Dent Res. 1987;66:1614–8.
Weatherell JA, Strong M, Robinson C, Ralph JP. Fluoride distribution in the mouth after fluoride rinsing. Caries Res. 1986;20:111–9.
Zhang F, Cheng Z, Ding C, Li J. Functional biomedical materials derived from proteins in the acquired salivary pellicle. J Mater Chem B. 2021;9:6507–20.
Neyraud E, Dransfield E. Relating ionisation of calcium chloride in saliva to bitterness perception. Physiol Behav. 2004;81:505–10.
Norris MB, Noble AC, Pangborn RM. Human saliva and taste responses to acids varying in anions, titratable acidity, and pH. Physiol Behav. 1984;32:237–44.
Lagerlöf F, Ekstrand J. The effect of flow rate on the ionized calcium concentration of human parotid saliva. Caries Res. 1982;16:123–8.
Robertson WG, Marshall RW, Bowers GN. Ionized calcium in body fluids. Crit Rev Clin Lab Sci. 1981;15:85–125.
Funding
None.
Author information
Authors and Affiliations
Contributions
AAA, FA, and MKA: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, visualization.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants or animals.
Informed consent
For this type of study, informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Alqahtani, A.A., Alhalabi, F. & Alam, M.K. Salivary elemental signature of dental caries: a systematic review and meta-analysis of ionomics studies. Odontology 112, 27–50 (2024). https://doi.org/10.1007/s10266-023-00839-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-023-00839-4