
Abstract
Background
Patients with chronic kidney disease (CKD) have a higher risk of atherosclerotic cardiovascular disease (ASCVD). Dyslipidemia has been established as a risk factor for ASCVD. In the present study, we aimed to determine the prevalence of dyslipidemia at each stage of CKD.
Methods
We conducted a cross-sectional study among 4476 patients registered in the Fukuoka Kidney Disease Registry Study, a Japanese prospective cohort study in patients with non-dialysis-dependent CKD. Outcomes were the prevalence of hyper-low-density lipoprotein (LDL) cholesterolemia, hyper-non-high-density lipoprotein (non-HDL) cholesterolemia, hypertriglyceridemia, and hypo-high-density lipoprotein (hypo-HDL) cholesterolemia at each stage of CKD. We analyzed the relationships between CKD stage and the prevalence of dyslipidemia using logistic regression models.
Results
Patients in the advanced stages of CKD were more likely to have hypertriglyceridemia [OR 2.16 (95% CI 1.03–4.56), OR 2.24 (95% CI 1.04–4.84), OR 2.62 (95% CI 1.19–5.78), and OR 2.47 (95% CI 1.04–5.88) for CKD stages G3a, G3b, G4, and G5, respectively] and hypo-HDL-cholesterolemia [OR 2.66 (95% CI 1.21–5.82), OR 3.10 (95% CI 1.38–6.95), OR 2.86 (95% CI 1.25–6.53), and OR 3.30 (95% CI 1.35–8.10) for CKD stages G3a, G3b, G4, and G5, respectively] as compared with patients in CKD stage G1. The prevalence of hyper-LDL-cholesterolemia and hyper-non-HDL-cholesterolemia was not related to CKD stage.
Conclusion
Patients with advanced CKD stages are more likely to have hypertriglyceridemia and hypo-HDL-cholesterolemia than those in early stages. This type of lipid profile may represent a risk factor for ASCVD in patients with CKD.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Patients with chronic kidney disease (CKD) are predisposed to cardiovascular diseases, including coronary artery disease, stroke, peripheral artery disease, and congestive heart failure [1, 2]. Dyslipidemia plays an important role in the development of atherosclerotic cardiovascular disease (ASCVD), and previous studies have shown that patients with CKD often also have dyslipidemia [3,4,5]. Impaired lipoprotein metabolism, especially higher levels of triglyceride and lower levels of high-density lipoprotein (HDL) cholesterol have been observed in predialysis patients with CKD and dialysis patients [6,7,8,9]. Moreover, patients with CKD often have associated malnutrition and inflammation [10]; however, there was no study have evaluated the characteristics of dyslipidemia in CKD after adjusting for potentially confounding factors, such as age, nutritional status, and inflammation.
The population-based Atherosclerosis Risk in Communities (ARIC) Study revealed that high serum concentrations of cholesterol and triglyceride in patients with CKD are associated with a high risk of coronary heart disease [11]. Several randomized controlled trials of statins have been performed in patients with CKD to determine their efficacy for the prevention of ASCVD. Sub-analyses of randomized trials conducted in predialysis patients with CKD have revealed that statin treatment significantly reduces the incidence of ASCVD [12, 13]. Recently, the Chronic Renal Insufficiency Cohort (CRIC) study showed that very low-density lipoprotein-cholesterol (VLDL-C) and apolipoprotein B (Apo-B) levels, but not low-density lipoprotein-cholesterol (LDL-C), are positively associated with the risk of ASCVD [14]. This result differed from findings of the ARIC study. The reason could be that the use of statins has become the standard means of preventing cardiovascular disease (CVD); therefore, the lipid profiles of patients with CKD may have changed in recent years. Consideration of the lipid profile in patients with CKD under current therapy may be useful to refine strategies for the prevention of CVD.
In the present study, we aimed to investigate the relationship between CKD stage and dyslipidemia, including hyper-LDL-cholesterolemia, hyper-non-high-density lipoprotein (HDL)-cholesterolemia, hypertriglyceridemia, and hypo-HDL-cholesterolemia after adjustment for potentially confounding factors in patients with CKD undergoing current therapy.
Methods
Study design and population
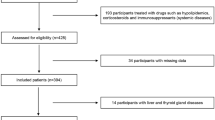
The Fukuoka Kidney Disease Registry (FKR) Study was a prospective, multicenter cohort study of non-dialysis-dependent outpatients with CKD [15]. The inclusion criteria were age ≥ 16 years and conformance with the Kidney Disease: Improving Global Outcomes (KDIGO) criteria for CKD [16]. The study sample consisted of 4,476 outpatients who were being managed by nephrologists in 12 hospitals in Fukuoka Prefecture of Japan [15]. Patient enrollment took place between January 2013 and March 2017, and all patients were scheduled to be followed up for at least 5 years. Of the 4,476 patients, 111 were excluded because of a lack of baseline data; therefore, data from 4365 patients were analyzed in the present study. The study was approved by the Clinical Research Ethics Committee of the Institutional Review Board of Kyushu University (approval number 469-04) and the ethics committees of all participating institutions; the study was registered in the University Hospital Medical Information Network clinical trials registry (UMIN000007988) and was conducted in accordance with the principles of the Declaration of Helsinki and its amendments.
Clinical parameters
Baseline demographic and clinical data were recorded at the time of enrollment. We obtained age, sex, height, body weight, blood pressure, and heart rate for all the participants. Clinical biochemical parameters [urinary protein and creatinine; hemoglobin concentration; and serum albumin, LDL-C, HDL-C, triglyceride, and C-reactive protein (CRP) concentrations] were determined by measurement in a central laboratory. Information regarding each participant’s health, the presence of diabetes, their history of CVD, and any treatments were collected from the patient medical records using a structured data format by clinical research coordinators in our research network. Body mass index (BMI) was calculated as body weight (kg) divided by height (m) squared. Patients were not required to fast when blood samples were collected.
Classification of CKD
CKD was defined and classified according to the patient’s estimated glomerular filtration rate (eGFR) using the KDIGO guidelines [16,17,18]. eGFR was calculated in patients age < 18 years using the Schwartz formula and in patients age ≥ 18 years using the following formula: eGFR (mL/min/1.73 m2) = 194 × Cr−1.094 × age−0.287 (× 0.739 for women) [18]. CKD was categorized as stages G1–G5, according to the KDIGO guidelines.
Definition of dyslipidemia
Dyslipidemia was defined according to Japan Atherosclerosis Society guidelines [19]. Non-HDL-C was calculated by subtracting HDL-C from total cholesterol. Hyper-LDL-cholesterolemia, hyper-non-HDL-cholesterolemia, and hypertriglyceridemia were defined as concentrations of LDL-C ≥ 140 mg/dL, non-HDL-C ≥ 170 mg/dL, and triglyceride ≥ 150 mg/dL, or use of lipid-lowering drugs, respectively. Hypo-HDL-cholesterolemia was defined as a concentration of HDL-C < 40 mg/dL. Dyslipidemia was diagnosed when a patient had hyper-LDL-cholesterolemia, hypertriglyceridemia, or hypo-HDL-cholesterolemia, or was taking medication for dyslipidemia.
Classification of proteinuria
Proteinuria was classified according to the KDIGO 2012 clinical practice guideline [20]. Proteinuria was evaluated by urinary protein/creatinine ratio (UpUCr). UpUCr was calculated by dividing the urinary protein values by the urinary creatinine concentrations. Proteinuria was categorized as < 0.15, 0.15–0.50, and ≥ 0.50 g/gCr.
Statistical analyses
Data are presented as mean ± standard deviation for normally distributed continuous variables, median and interquartile range for non-normally distributed continuous variables, and percentage for categorical variables. To evaluate trends in continuous and categorical values, we used the Jonckheere–Terpstra and Cochran–Armitage tests, respectively. Logistic regression analysis was used to calculate age- and sex-adjusted, and multivariable-adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for the relationships between CKD stage and the presence of dyslipidemia. The multivariable-adjusted model was adjusted for age, sex, the presence of diabetes, a history of CVD, systolic blood pressure, heart rate, BMI, hemoglobin concentration, serum albumin concentration, log-CRP, and urinary protein/creatinine ratio. Sensitivity analyses were performed to examine the odds ratio of hypertriglyceridemia using the American Heart Association/American College of Cardiology Foundation (AHA/ACC) guidelines 2018 [21] and to confirm the odds ratio after excluding the patients taking lipid-lowering drugs. Statistical analyses were conducted using IBM SPSS version 22 (IBM Corp., Armonk, NY, USA) and R version 3.5.2 (http://www.r-project.org). A two-tailed P value of < 0.05 was deemed to indicate statistical significance.
Results
Study participants and baseline characteristics
The clinical characteristics of participants at each stage of CKD are shown in Table 1. Advanced CKD stages were positively associated with age, male sex, the presence of diabetes, a history of CVD, high systolic blood pressure, high diastolic blood pressure, high CRP concentration, high urinary protein/creatinine ratio, and the use of lipid-lowering drugs but negatively associated with hemoglobin and serum albumin concentrations.
Relationship between CKD stage and serum lipid concentrations after adjustment of confounding factors
To adjust for patients’ nutritional status and background, we investigated whether progression of CKD was associated with a high prevalence of dyslipidemia using logistic regression models (Tables 2, 3, 4, 5). CKD stage G3a was associated with the highest odds of hyper-LDL-cholesterolemia, but CKD stages were not associated with a trend of hyper-LDL-cholesterolemia (Table 2). CKD stages G3a, G3b, G4 and G5 were associated with higher odds of hypertriglyceridemia [OR 2.16 (95% CI 1.03–4.56), OR 2.24 (95% CI 1.04–4.84), OR 2.62 (95% CI 1.19–5.78), and OR 2.47 (95% CI 1.04–5.88) for CKD stages G3a, G3b, G4, and G5, respectively) in comparison with CKD stage G1 (Table 3). CKD stages were also associated with a trend of hypertriglyceridemia (P = 0.03, Table 3). CKD stages G2, G3a, G3b, and G4 were associated with high odds of hyper-non-HDL-cholesterolemia [OR 2.47 (95% CI 1.18–5.17), OR 3.30 (95% CI 1.53–7.12), OR 3.23 (95% CI 1.46–6.83), and OR 3.03 (95% CI 1.34–6.83) for CKD stage G2, G3a, G3b, and G4, respectively] compared with CKD stage G1, but there was no significant trend for the odds of hyper-non-HDL-cholesterolemia across all stages of CKD (Table 4). CKD stages G3a, G3b, G4 and G5 were associated with higher odds of hypo-HDL-cholesterolemia [OR 2.79 (95% CI, 1.27–6.14) OR 3.31 (95% CI 1.47–7.45), OR 3.03 (95% CI 1.32–6.95), and OR 3.62 (95% CI 1.47–8.90) for CKD stages G3a, G3b, G4, and G5, respectively] in comparison with CKD stage G1 (Table 5). CKD stages were also associated with a trend of hypo-HDL-cholesterolemia (P < 0.01, Table 5).
Relationship between proteinuria and serum lipid concentrations
Proteinuria also affects dyslipidemia in patients with CKD. We, therefore, investigated the relationship between proteinuria and dyslipidemia, including hyper-LDL-cholesterolemia, hyper-non-high-density lipoprotein (HDL)-cholesterolemia, hypertriglyceridemia, and hypo-HDL-cholesterolemia, after adjustment for potentially confounding factors in patients with CKD (Table 6 and Supplementary Table 1). Proteinuria was associated with a trend of hyper-LDL-cholesterolemia (P = 0.04) and hyper-non-HDL-cholesterolemia (P < 0.01), but was not associated with a trend of hypertriglyceridemia (P = 0.07) and hypo-HDL-cholesterolemia (P = 0.07).
Sensitivity analysis of odds ratios for hypertriglyceridemia using the 2018 AHA/ACC guideline
In this study, we measured triglyceride in a non-fasting state. Although the Japan Atherosclerosis Society guidelines did not mention the definition of hypertriglyceridemia in a non-fasting state [19], the 2018 AHA/ACC guideline proposed a cutoff of 175 mg/dL for a non-fasting triglyceride [21]. We conducted a sensitivity analysis of odds ratios for hypertriglyceridemia using the 2018 AHA/ACC guideline (Supplementary Table 2). CKD stages G2, G3a, G3b, G4, and G5 were associated with high odds of hypertriglyceridemia [OR 2.51 (95% CI 1.18–5.34), OR 3.01 (95% CI 1.38–6.60), OR 3.08 (95% CI 1.37–6.90), OR 3.74 (95% CI 1.63–7.68), and OR 3.12 (95% CI 1.27–7.68) for CKD stage G2, G3a, G3b, G4, and G5, respectively] compared with CKD stage G1 (Supplementary Table 2). The result was similar to that obtained using the Japan Atherosclerosis Society guidelines (Table 3).
Sensitivity analyses of patients not taking lipid-lowering drugs
Since lipid-lowering therapy improves dyslipidemia, we reanalyzed the ORs of dyslipidemia only in patients not taking lipid-lowering drugs in a sensitivity analysis (Supplementary Tables 3, 4, 5, 6). CKD stages in patients not on lipid-lowering therapy were also associated with a trend of hypertriglyceridemia (P = 0.01, Supplementary Table 4) and a trend of hypo-HDL-cholesterolemia (P < 0.01, Supplementary Table 6). There was no significant trend in the odds of hyper-LDL-cholesterolemia or hyper-non-HDL-cholesterolemia across all CKD stages (Supplementary Tables 3 and 5). No essential difference was seen with respect to characteristics of the lipid profile in CKD without lipid-lowering drugs.
Analysis of subgroups created according to baseline clinical characteristics
To evaluate interactions between the prevalence of dyslipidemia and patient characteristics, we evaluated the effects of patient stratification on the prevalence of hypertriglyceridemia and hypo-HDL-cholesterolemia (Supplementary Tables 7 and 8). Advanced CKD stage appeared to be associated with hypertriglyceridemia and hypo-HDL-cholesterolemia in patients age < 65 years (both P < 0.01), but there was no significant difference in prevalence between patients age < 65 years and those age ≥ 65 years (P = 0.30 and P = 0.26 for interaction, Supplementary Tables 7 and 8). Finally, patients with CKD who had no history of CVD were more likely to have hypo-HDL-cholesterolemia (P < 0.01, Supplementary Table 8).
Discussion
In this cohort study of 4476 patients with CKD, CKD stages were significantly associated with hypertriglyceridemia and hypo-HDL-cholesterolemia after adjusting for confounding factors, but there were no linear relationships between abnormal LDL-C or non-HDL-C concentrations and CKD stage. CKD stage was significantly associated with hypo-HDL-cholesterolemia in patients who were < 65 years of age. To the best of our knowledge, this is the first study showing the characteristics of lipid profiles in patients with CKD using the Japan Atherosclerosis Society guidelines after adjustment for all confounding factors. In the present study, we showed that hypertriglyceridemia and hypo-HDL-cholesterolemia are the specific types of dyslipidemia that occur in patients with CKD.
The results of the recent CRIC study revealed that high triglyceride-rich lipoprotein concentrations and low HDL-C concentrations are associated with a higher risk of ASCVD whereas a high LDL-C concentration is not [14]. These findings differ from those of the ARIC study [11]. In the present study, over 40% of patients with CKD stages G3–5 were being treated with lipid-lowering therapy (Table 1). Statin treatment reduces serum LDL-C concentration; therefore, it is possible that the serum cholesterol concentrations of this recently enrolled cohort were lower than those of participants in previous studies. In addition, hypertriglyceridemia is difficult to treat safely in patients with CKD because fibrates occasionally induce rhabdomyolysis in patients with renal impairment. In the present study, hypertriglyceridemia was more common in patients with advanced CKD (Table 2), which might suggest that hypertriglyceridemia is a risk factor for ASCVD in patients with CKD.
Moreover, a recent sub-analysis of the SHARP (Study of Heart and Renal Protection) trial revealed that higher levels of triglycerides, LDL-C, and non-HDL-C, and a lower level of HDL-C had a significantly higher risk of ASCVD in 9270 patients with CKD [22]. That study also demonstrated that a higher level of LDL-C in simvastatin and ezetimibe groups did not have a higher risk of ASCVD, suggesting that the risk of ASCVD from higher LDL-C may possibly be suppressed by statins and ezetimibe. We presume from this result that hypertriglyceridemia and hypo-HDL-cholesterolemia might be residual risks for ASCVD in CKD patients.
Plasma triglyceride concentrations have been reported to increase during the early stages of CKD [3, 4]. Degradation of triglyceride-rich VLDL is not high in patients with CKD [23], plasma lipoprotein lipase activity has been reported to be low [9], and patients with CKD also demonstrate low hepatic triglyceride lipase activity [9]. Alterations in the activity of these lipases cause the accumulation of triglyceride-rich lipoproteins in patients with CKD. In the present study, hypertriglyceridemia was a feature of advanced CKD (Table 2) and the use of fibrates was uncommon because of their side effects (Table 1). However, a recent report showed that pemafibrate, a new type of fibrate, did not significantly increase serum creatinine kinase activity in patients with advanced CKD [24]. Therefore, pemafibrate may be a useful means of reducing the risk of ASCVD in patients with CKD.
HDL-C plays an important role in reverse cholesterol transport; however, in the present study, hypo-HDL-cholesterolemia was more common in advanced CKD (Table 5). The conversion of HDL has been reported to be lower in CKD because lecithin–cholesterol acyltransferase activity is lower in these patients [3]. The lower ability of HDL particles to carry cholesterol causes impairment of reverse cholesterol transport, which promotes atherosclerosis. The CRIC study revealed that a low HDL-C concentration is associated with a high risk of ASCVD in CKD [14]; another study showed that an increase in HDL-C concentration induced by the inhibition of cholesteryl ester transfer protein does not reduce the risk of acute coronary syndrome [25]. Thus, there is no effective strategy to increase HDL-C concentration as a means of preventing ASCVD; this should be a priority of future research.
A previous study showed that the non-HDL-C concentration is superior to the LDL-C concentration for the prediction of myocardial infarction in patients receiving hemodialysis [26]. This can be explained by the fact that non-HDL-C includes all the cholesterol present in lipoprotein particles that is considered to be atherogenic, including LDL, lipoprotein(a), intermediate-density lipoprotein, and VLDL remnants [27]. In the present study, patients with CKD stages G3a and G4 were more likely to have a high non-HDL-C concentration (Table 4). Further investigation is needed to clarify whether high non-HDL-C concentrations are associated with a higher risk of ASCVD.
The present study has several limitations. First, we did not measure triglyceride concentration in the fasting state. However, a recent study showed that non-fasting triglyceride concentrations are related to the incidence of cardiovascular events [28], which implies that this measurement should also be useful. Second, all included patients were Japanese; thus, our findings might not be applicable to other ethnic groups. Third, given the cross-sectional design of this study, we are unable to ascribe causality to the relationships between serum lipid concentrations and kidney function. We intend to observe this study prospectively and reveal these causal relationships. Finally, we did not evaluate the incidence of ASCVD; therefore, we are continuing to follow participants in a prospective study, and we will determine the relationship between dyslipidemia and the incidence of ASCVD in patients with CKD using this sample in the future.
Conclusion
Patients with advanced CKD are more likely to have dyslipidemia, and especially to show hypertriglyceridemia and hypo-HDL-cholesterolemia, in comparison with those in the early stages of CVD. These serum lipid abnormalities might represent a risk for ASCVD; therefore, treatment for dyslipidemia should be considered in patients with CKD.
References
Tonelli M, Karumanchi SA, Thadhani R. Epidemiology and mechanisms of uremia-related cardiovascular disease. Circulation. 2016;133(5):518–36.
Drueke TB, Massy ZA. Atherosclerosis in CKD: differences from the general population. Nat Rev Nephrol. 2010;6(12):723–35.
Kwan BC, Kronenberg F, Beddhu S, Cheung AK. Lipoprotein metabolism and lipid management in chronic kidney disease. J Am Soc Nephrol. 2007;18(4):1246–61.
Shoji T, Abe T, Matsuo H, Egusa G, Yamasaki Y, Kashihara N, Shirai K, Kashiwagi A, Committee of R, Peripheral Arteries JAS. Chronic kidney disease, dyslipidemia, and atherosclerosis. J Atheroscler Thromb. 2012;19(4):299–315.
Ferro CJ, Mark PB, Kanbay M, Sarafidis P, Heine GH, Rossignol P, Massy ZA, Mallamaci F, Valdivielso JM, Malyszko J, Verhaar MC, Ekart R, Vanholder R, London G, Ortiz A, Zoccali C. Lipid management in patients with chronic kidney disease. Nat Rev Nephrol. 2018;14(12):727–49.
Bagdade JD, Porte D Jr, Bierman EL. Hypertriglyceridemia. A metabolic consequence of chronic renal failure. N Engl J Med. 1968;279(4):181–5.
Bagdade JD, Albers JJ. Plasma high-density lipoprotein concentrations in chronic-hemodialysis and renal-transplant patients. N Engl J Med. 1977;296(25):1436–9.
Brunzell JD, Albers JJ, Haas LB, Goldberg AP, Agadoa L, Sherrard DJ. Prevalence of serum lipid abnormalities in chronic hemodialysis. Metabolism. 1977;26(8):903–10.
Shoji T, Nishizawa Y, Nishitani H, Yamakawa M, Morii H. Impaired metabolism of high density lipoprotein in uremic patients. Kidney Int. 1992;41(6):1653–61.
Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Trevino-Becerra A, Wanner C. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008;73(4):391–8.
Muntner P, He J, Astor BC, Folsom AR, Coresh J. Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: results from the atherosclerosis risk in communities study. J Am Soc Nephrol. 2005;16(2):529–38.
Tonelli M, Isles C, Curhan GC, Tonkin A, Pfeffer MA, Shepherd J, Sacks FM, Furberg C, Cobbe SM, Simes J, Craven T, West M. Effect of pravastatin on cardiovascular events in people with chronic kidney disease. Circulation. 2004;110(12):1557–63.
Sever PS, Dahlof B, Poulter NR, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O’Brien E, Ostergren J, Investigators A. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361(9364):1149–58.
Bajaj A, Xie D, Cedillo-Couvert E, Charleston J, Chen J, Deo R, Feldman HI, Go AS, He J, Horwitz E, Kallem R, Rahman M, Weir MR, Anderson AH, Rader DJ, Investigators CS. Lipids, apolipoproteins, and risk of atherosclerotic cardiovascular disease in persons with CKD. Am J Kidney Dis. 2019;73(6):827–36.
Tanaka S, Ninomiya T, Fujisaki K, Yoshida H, Nagata M, Masutani K, Tokumoto M, Mitsuiki K, Hirakata H, Fujimi S, Kiyohara Y, Kitazono T, Tsuruya K, Fukuoka Kidney disease Registry Study Collaboration G. The Fukuoka Kidney disease Registry (FKR) study: design and methods. Clin Exp Nephrol. 2017;21(3):465–73.
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, De Zeeuw D, Hostetter TH, Lameire N, Eknoyan G. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005;67(6):2089–100.
Levin A, Stevens PE. Summary of KDIGO 2012 CKD Guideline: behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014;85(1):49–61.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A, Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982–92.
Kinoshita M, Yokote K, Arai H, Iida M, Ishigaki Y, Ishibashi S, Umemoto S, Egusa G, Ohmura H, Okamura T, Kihara S, Koba S, Saito I, Shoji T, Daida H, Tsukamoto K, Deguchi J, Dohi S, Dobashi K, Hamaguchi H, Hara M, Hiro T, Biro S, Fujioka Y, Maruyama C, Miyamoto Y, Murakami Y, Yokode M, Yoshida H, Rakugi H, Wakatsuki A, Yamashita S, Committee for E, Clinical Management of A. Japan Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases 2017. J Atheroscler Thromb. 2018;25(9):846–984.
Chapter 1: definition and classification of CKD. Kidney Int Suppl (2011). 2013;3(1):19–62.
Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd-Jones D, Lopez-Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082–143.
Lamprea-Montealegre JA, Staplin N, Herrington WG, Haynes R, Emberson J, Baigent C, de Boer IH, Group SC. Apolipoprotein B, Triglyceride-Rich Lipoproteins, and Risk of Cardiovascular Events in Persons with CKD. Clin J Am Soc Nephrol. 2020;15(1):47–60.
Ikewaki K, Schaefer JR, Frischmann ME, Okubo K, Hosoya T, Mochizuki S, Dieplinger B, Trenkwalder E, Schweer H, Kronenberg F, Koenig P, Dieplinger H. Delayed in vivo catabolism of intermediate-density lipoprotein and low-density lipoprotein in hemodialysis patients as potential cause of premature atherosclerosis. Arterioscler Thromb Vasc Biol. 2005;25(12):2615–22.
Yokote K, Yamashita S, Arai H, Araki E, Suganami H, Ishibashi S, Of The KSGOB. Long-term efficacy and safety of pemafibrate, a novel selective peroxisome proliferator-activated receptor-alpha modulator (SPPARMalpha), in dyslipidemic patients with renal impairment. Int J Mol Sci. 2019;20(3):5537.
Schwartz GG, Olsson AG, Abt M, Ballantyne CM, Barter PJ, Brumm J, Chaitman BR, Holme IM, Kallend D, Leiter LA, Leitersdorf E, McMurray JJ, Mundl H, Nicholls SJ, Shah PK, Tardif JC, Wright RS, Dal OI. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367(22):2089–99.
Shoji T, Masakane I, Watanabe Y, Iseki K, Tsubakihara Y, Committee of Renal Data Registry jsfdt. Elevated non-high-density lipoprotein cholesterol (non-HDL-C) predicts atherosclerotic cardiovascular events in hemodialysis patients. Clin J Am Soc Nephrol. 2011;6(5):1112–20.
Cui Y, Blumenthal RS, Flaws JA, Whiteman MK, Langenberg P, Bachorik PS, Bush TL. Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Arch Intern Med. 2001;161(11):1413–9.
Bansal S, Buring JE, Rifai N, Mora S, Sacks FM, Ridker PM. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA. 2007;298(3):309–16.
Acknowledgements
We would like to thank all the doctors and medical staff who participated in the FKR Study. Steering Committee and Principal Collaborators of the FKR Study Group: Satoru Fujimi (Fukuoka Renal Clinic), Hideki Hirakata (Fukuoka Renal Clinic), Tadashi Hirano (Hakujyuji Hospital), Tetsuhiko Yoshida (Hamanomachi Hospital), Takashi Deguchi (Hamanomachi Hospital), Hideki Yotsueda (Harasanshin Hospital), Kiichiro Fujisaki (Iizuka Hospital), Keita Takae (Japanese Red Cross Fukuoka Hospital), Koji Mitsuiki (Japanese Red Cross Fukuoka Hospital), Akinori Nagashima (Japanese Red Cross Karatsu Hospital), Ritsuko Katafuchi (Kano Hospital), Hidetoshi Kanai (Kokura Memorial Hospital), Kenji Harada (Kokura Memorial Hospital), Tohru Mizumasa (Kyushu Central Hospital), Takanari Kitazono (Kyushu University), Toshiaki Nakano (Kyushu University), Toshiharu Ninomiya (Kyushu University), Kumiko Torisu (Kyushu University), Akihiro Tsuchimoto (Kyushu University), Shunsuke Yamada (Kyushu University), Hiroto Hiyamuta (Kyushu University), Shigeru Tanaka (Kyushu University), Dai Matsuo (Munakata Medical Association Hospital), Yusuke Kuroki (National Fukuoka-Higashi Medical Center), Hiroshi Nagae (National Fukuoka-Higashi Medical Center), Masaru Nakayama (National Kyushu Medical Center), Kazuhiko Tsuruya (Nara Medical University), Masaharu Nagata (Shin-eikai Hospital), Taihei Yanagida (Steel Memorial Yawata Hospital), and Shotaro Onaka (Tagawa Municipal Hospital).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors have declared no competing interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted (IRB approval number UMIN000007988) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Nakano, T., Tanaka, S., Tsuruya, K. et al. Relationship between serum lipid concentrations and impaired renal function in patients with chronic kidney disease: the Fukuoka Kidney Disease Registry Study. Clin Exp Nephrol 25, 385–393 (2021). https://doi.org/10.1007/s10157-020-02000-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-020-02000-9