
Abstract
Background
Since our last publication of algorithms for the management of perianal fistulas in patients with Crohn’s disease, researchers have proposed a treat to target strategy systematic combotherapy for anal lesions, and indications for stem cell injection. In the absence robust publications, the Société Nationale Française de Coloproctologie (French National Society of Coloproctology [SNFCP]) wished to establish a group consensus using the Delphi method.
Methods
From October 2020 to January 2021, a scientific committee and panel of gastroenterologists and surgeons established answers which were submitted to the members of the SNFCP during a national conference in November 2020. Three questions were clarified and reformulated, and then submitted during a third and final round of consultation of members of the SNFCP.
Results
The target was defined as being the response obtained in every domain (symptoms, physical and radiological evaluation) which could be considered satisfactory, without the need to intensify therapeutic management. By consensus, the time required for clinical evaluation of the efficacy of treatment was 6 months. A response on magnetic resonance imaging (MRI) should include the absence of a collection of 10 mm or more in size at 6 months, and a frank decrease or complete disappearance of hyperintensity in T1 and T2 sequences of the main tract at 12 months. Systematic association of an immunosuppressant with tumor necrosis factor inhibitors did not reach the consensus level for adalimumab (50%), but just did for infliximab (70%). The majority of the respondents considered failure of one, or even two lines of different biotherapies to be potential indications for injection of stem cells.
Conclusions
These findings reinforce the importance of composite targets including MRI evaluation, and underscore the need for precise timing of evaluation. Combotherapy is only recommended with infliximab. Injection of stem cells is a second- or third-line option.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the publication by the Société Nationale Française de Coloproctologie (French National Society of Coloproctology [SNFCP]) of algorithms for the management of peri anal fistulas in patients with Crohn’s disease (CD) [1], therapeutic demands have evolved in terms of markers of efficacy and medical/surgical management strategies.
The principle of “treat to target” in CD has led to the definition of increasingly precise treatment goals, some of which combine clinical, biological, endoscopic, radiological, or even microscopic markers [2]. The targets for anal lesions merit further clarification, because they cannot be evaluated with the same tools as luminal disease. In current practice and scientific publications, evaluation is based on a pragmatic approach (the need for a surgical intervention or repeat intervention), out-of-date heterogenous scores (the Perineal Disease Activity Index, PDAI) [3], basic clinical characteristics (open or closed fistula) [4] or more subtle, but currently unvalidated, radiological scores (Magnify-CD) [5].
Recent medical and surgical treatment strategies were developed in the absence of quantitative knowledge about the effect of biotherapies alone or in combination [6,7,8,9], and do not take into account innovative strategies, such as the injection of stem cells in situ [5, 10]. This last technique has market authorization and is reimbursed by the French national health insurance system, even though it has only been evaluated in a limited number of studies.
In the absence of recommendations, and while awaiting new studies providing more robust evidence, the SNFCP wished to establish a consensus based on the Delphi method, to aid physicians in the management of this disease.
Materials and methods
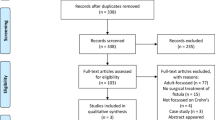
The Scientific Committee, which consists of three elected members of the Board of the SNFCP, formulated a series of questions and possible responses. A first round of consultation took place in October 2020, with a panel of 14 expert gastroenterologists and surgeons from the Study Group for the Treatment of Inflammatory Conditions of the Digestive Tract (GETAID) (n = 8) and the SNFCP (n = 6). The results were analyzed and the Scientific Committee reformulated the questions and responses, which were submitted, during a second round of consultation, to a broad, non-selected panel of gastroenterologists and digestive surgeons from the SNFCP. The results of this survey were presented in a plenary session at the annual meeting of the SNFCP in November 2020, which brought together 400 people with an interest in coloproctology. Based on the questions raised and comments made during this presentation, three questions were clarified and reformulated, and then submitted during a third and final round of consultation of members of the SNFCP. The various steps in the Delphi method are presented in the appendix (Fig. 1).

Steps in the Delphi process. GETAID Groupe d'Etude Thérapeutique des Affections Inflammatoires du Tube Digestif (Study Group on Inflammatory Bowel Disease), SNFCP Société Nationale Française de Coloproctologie (French National Society of Coloproctology)
The questions (and possible responses) written and adapted by the Scientific Committee concerned two domains:
-
The clinical and radiological targets to be achieved, and the time taken to reach them
-
Medical treatment: the place of combination treatment, and the injection of stem cells.
A consensus was considered to have been reached if at least 70% of the responses to a given question were positive and no change to the formulation was proposed.
The responses to this survey were integrated into the algorithms proposed in 2018 [1].
Results
The process took place between October 2020 and January 2021, and is summarized in Fig. 1.
In the initial questionnaire, the term “target to reach” was too vague for the experts. Therefore, in the following questionnaires, the target was defined as being “the response obtained in every domain (symptoms, physical and radiological evaluation) which could be considered satisfactory, without the need to intensify therapeutic management”.
An evaluation of the therapeutic targets thus defined is summarized in Table 1. The three categories of targets proposed (symptoms, clinical examination data, and magnetic resonance imaging [MRI] data) were retained in the consensus. Positive responses were obtained 83 times (98%; for symptoms), 85 times (100%, for clinical examination data) and 74 times (87%, MRI data) for the 85 responses obtained (Fig. 2). No other domain of evaluation was proposed in response to the open question “Others?”. For MRI data, neither the direct nature of the tract of the fistula nor the presence of proctitis was retained (31 (36%) and 35 (41%) positive responses, respectively, of 85 possible). For evaluation of collections or inflammatory masses, three maximal size thresholds were proposed (3, 10 and 20 mm), resulting in cumulative positive response rates of 11 (18%), 38 (80%) and 12 (100%), respectively, for the 61 responses obtained. A threshold of 10 mm was retained for the consensus.

Domains taken into account for the establishment of treatment targets. MRI magnetic resonance imaging
By consensus, the time required for clinical evaluation of the efficacy of treatment was 6 months. A response on MRI should include the absence of a collection of equal to or greater than 10 mm or more in size at 6 months, and a frank decrease or complete disappearance of the hyperintensity of the principal trajectory at 12 months. For the question “Do you use a global MRI activity score and a score defined by publications?”, 32 of the 85 responses were positive (38%). Therefore, the threshold for consensus was not reached.
An evaluation of the therapeutic strategies used to treat anal fistulas in patients with Crohn’s disease is reported in Table 2. Systematic association of an immunosuppressant with tumor necrosis factor (TNF) inhibitors was frequent and reached consensus infliximab (70%). but not for adalimumab (50%), Only 5% felt that there was no indication for the use of allogeneic stem cells with the majority of the respondents considering such treatment after failure of first-line and second-line biotherapy.
The algorithms describing the principal clinical situations, published in 2018 [1] and updated here, are shown in Figs. 3, 4, 5.

Decision-support algorithm for the management of ano-perineal suppurations associated with Crohn’s disease, updated. Management of an abscess or collection. MRI magnetic resonance imaging, TNF tumor necrosis factor

Decision-support algorithm for the management of ano-perineal suppuration associated with Crohn’s disease, updated. Management of an active anal fistula with no prior treatment. MRI magnetic resonance imaging, TNF tumor necrosis factor

Decision-support algorithm for the management of ano-perineal suppuration associated with Crohn’s disease, updated. Management of an active anal fistula with anti-TNF treatment. MRI magnetic resonance imaging, TNF tumor necrosis factor
Discussion
This survey confirms the use of a combination of data from symptoms, clinical examination and MRI for evaluation of the activity of perianal fistulas. These findings provide support for the importance of composite targets combining patient-reported outcomes with more objective criteria, such as radiological and endoscopic scores [11, 12].
The symptoms included in the consensus (pain, discharge, and induration) are those included in the PDAI [3]. The clinical examination data retained are also simple, and similar to those proposed in the early clinical trials for biotherapy [4]. However, the presence or absence of “an open external orifice” gained only just enough responses to be retained. Indeed, an open cutaneous orifice, in the absence of other physical signs reflecting inflammatory activity, may not be sufficient for an intensification of treatment if the other functional and radiological criteria for remission are satisfied. However, our survey did not evaluate any combination of associations of targets.
The use of MRI data still lacks objective quantification, as demonstrated by the restricted use of the available scores. However, the MRI evaluation of two simple items, most frequently mentioned in publications, was retained as necessary in the consensus. Although proctitis is a factor associated with severe prognosis in perianal lesions, its presence was excluded from the list of targets to be taken into account in fistula treatment. Collections/masses above a significance threshold of 10 mm in size, and changes in the hyperintensity of fistula tract were retained. Several threshold sizes were proposed for collections/masses (3, 10 and 20 mm). A value of 10 mm was retained. This threshold is more strict than that used in studies on stem cells [5, 10] and that proposed in the 2018 SNFCP algorithms [1]. This more rigorous demand, which came from members of the SNFCP, may be explained by surgical culture and greater demands concerning the quality of the result obtained through a combined medical and surgical management approach.
The response to therapeutic management should not be evaluated too early and this evaluation may differ according to the analytical criteria used. There is a difference between the expected clinical (clinical symptoms and signs, within a maximum of 6 months) and radiological (cavity/collection at 6 months, disappearance or frank improvement of tracts hyperintensity at 12 months).
Drug-based treatment strategies mostly involve a combination of a TNF inhibitor with an immunosuppressant: in 70% of cases when the TNF inhibitor is infliximab (positive consensus), but in only 50% of cases when the TNF inhibitor is adalimumab (absence of a positive consensus). Several published studies [7, 13] have suggested a possible benefit of combined therapies for perianal Crohn’s fistulas, but the evidence remains weak [14,15,16].
The use of local injections of adipocyte stem cells was not strongly supported other than in cases of the persistence of active suppuration after the failure of one or two lines of biotherapy (74%).
The limitations of this work stem from the fact that only medical doctors involved in fistula management (proctologists, gastroenterologists and surgeons) were consulted. The opinions of healthcare professionals other than doctors, and the views of patients might reveal other targets. Despite the reformulation of the questions during each round of consultation, uncertainties exist that might be resolved by rewording the questions.
This survey made it possible to incorporate a consensus-based evidence into the algorithms guiding management. New studies or consensus surveys should determine the role of combinations of immunosuppressants and TNF inhibitors, and that of stem cell injections.
Conclusions
From the treating physicians’ viewpoint, the targets to be considered when evaluating management of ano-perineal fistulas in Crohn’s disease are based on symptomatic criteria, physical examination data, and MRI evaluations. Anatomic and clinical items remain important, and are acheieved with simple MRI criteria. Additional targets should be added, based on patient opinion, with a combination of targets optimizing decision-making for treatment.
Combination treatments are recommended when infliximab is used.
The injection of stem cells is recommended in the presence of perineal signs of inflammation after the failure of one or two lines of biotherapy.
References
Bouchard D, Pigot F, Staumont G, Siproudhis L, Abramowitz L, Benfredj P et al (2018) Management of anoperineal lesions in Crohn’s disease: a French National Society of Coloproctology national consensus. Tech Coloproctol 22:905–917
Hommes D, Colombel JF, Emery P, Greco M, Sandborn WJ (2012) Changing Crohn’s disease management: need for new goals and indices to prevent disability and improve quality of life. J Crohns Colitis 6(Suppl2):S224–S234
Irvine EJ (1995) Usual therapy improves perianal Crohn’s disease as measured by a new disease activity index McMaster IBD Study Group. J Clin Gastroenterol 20:27–32
Present DH, Rutgeerts P, Targan S, Hanauer SB, Mayer L, van Hogezand RA et al (1999) Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med 340:1398–1405
Panés J, García-Olmo D, Van Assche G, Colombel JF, Reinisch W, Baumgart DC et al (2016) Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn’s disease: a phase 3 randomised double-blind controlled trial. Lancet 388:1281–1290
Lichtenstein GR, Diamond RH, Wagner CL, Fasanmade AA, Olson AD, Marano CW et al (2009) Benefits and risks of immunomodulators and maintenance infliximab for IBD-subgroup analyses across four randomized trials. Alimentary Pharmacol Therap 30:210–226
Bouguen G, Siproudhis L, Gizard E, Wallenhorst T, Billioud V, Bretagne JF et al (2013) Long-term outcome of perianal fistulizing Crohn’s disease treated with infliximab. Clin Gastroenterol Hepatol 11:975–981
Kopylov U, Al-Taweel T, Yaghoobi M, Nauche B, Bitton A, Lakatos PL et al (2014) Adalimumab monotherapy versus combination therapy with immunomodulators in patients with Crohn’s disease: a systematic review and meta-analysis. J Crohns Colitis 8:1632–1641
Colombel JF, Jharap B, Sandborn WJ, Feagan B, Peyrin-Biroulet L, Eichner SF et al (2017) Effects of concomitant immunomodulators on the pharmacokinetics, efficacy and safety of adalimumab in patients with Crohn’s disease or ulcerative colitis who had failed conventional therapy. Aliment Pharmacol Ther 45:50–62
Molendijk I, Bonsing BA, Roelofs H, Peeters KC, Wasser MN, Dijkstra G et al (2015) Allogeneic bone marrow-derived mesenchymal stromal cells promote healing of refractory perianal fistulas in patients with Crohn’s disease. Gastroenterology 149:918–927
Levesque BG, Sandborn WJ, Ruel J, Feagan BG, Sands BE, Colombel JF (2015) Converging goals of treatment of inflammatory bowel disease from clinical trials and practice. Gastroenterology 148:37–51
Sahnan K, Tozer PJ, Adegbola SO, Lee MJ, Heywood N, McNair AGK et al (2019) Developing a core outcome set for fistulising perianal Crohn’s disease. Gut 68:226–238
Malian A, Rivière P, Bouchard D, Pigot F, Eléouet-Kaplan M, Favreau-Weltzer C et al (2020) Predictors of perianal fistula relapse in Crohn’s disease. Inflamm Bowel Dis 26:926–931
Kennedy NA, Heap GA, Green HD, Hamilton B, Bewshea C, Walker GJ et al (2019) UK Inflammatory Bowel Disease Pharmacogenetics Study Group. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: a prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol 4:341–353
Davidov Y, Ungar B, Bar-Yoseph H, Carter D, Haj-Natour O, Yavzori M et al (2017) Association of induction infliximab levels with clinical response in perianal Crohn’s disease. J Crohns Colitis 11:549–555
Yarur AJ, Kanagala V, Stein DJ, Czul F, Quintero MA, Agrawal D et al (2017) Higher infliximab trough levels are associated with perianal fistula healing in patients with Crohn’s disease. Aliment Pharmacol Ther 45:933–940
Acknowledgements
The members of the SNFCP and Members of the GETAID: Guillaume Bouguen (Digestive Diseases Unit, CHU Pontchaillou, 2 rue Henri Le Guilloux 35033 Rennes, France), David Laharie (Hepato-Gastroenterology Unit, CHU Haut Lévèque, 33600 Pessac ), Eddy Cotte (Digestive and Endocrine Surgery Unit, Hospital Lyon-Sud, 165 chemin du grand Revoyet, 69495 Pierre Bénite cedex ), Yves Panis (Digestive Surgery Unit, Beaujon Hospital, 100 boulevard du Général Leclerc, 92110 Clichy), L Peyrin-Biroulet (Hepato-Gastroenterology Unit, CHRU Nancy, 54511 Vandoeuvre les Nancy), Xavier Roblin (Gastroenterology, Hepatology and Inflammatory Bowel Diseases Unit, CHU Saint Etienne, 25 boulevard Pasteur, 42055 Saint-Etienne), Philippe Zerbib (Digestive Unit, Hospital Huriez, rue Michel Polonowski, 59037 Lille) as co-authors, Emmanuelle Babin-Pigot and Marie Ferry for essential logistic assistance.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
DB: Takeda as consultant, Abbvie Janssen Takeda for learning. LS: Takeda Abbvie Janssen MSD for clinical research, Takeda as consultant, Takeda Abbvie Janssen Amgen Ferring for learning. VdP: Takeda as consultant, Abbvie, Amgen, Tillots for learning. GS: Takeda, Janssen as consultant, Abbvie, Takeda for learning. LA: Abbvie, Takeda, Celltrion for clinical research, Takeda as consultant, Takeda, Abbvie, Janssen, Ferring for learning. FP: Abbvie, Takeda for learning.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The Members of SNFCP and Members of GETAID were listed in Acknowledgement section.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bouchard, D., Pigot, F., de Parades, V. et al. Management of perianal fistulas in Crohn’s disease: a 2021 update of the French National Society of Coloproctology consensus. Tech Coloproctol 26, 805–811 (2022). https://doi.org/10.1007/s10151-022-02678-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-022-02678-x