
Abstract
Background
Epidemiological studies in Western countries have documented an increase of hospitalizations for acute diverticulitis (AD) but Italian evidence is scarce. The aim of the present study was to analyse the trend in hospitalization for AD, including in-hospital mortality, in Italy from 2008 to 2015.
Methods
Through the Italian Hospital Information System of the National Health System, we identified diverticulitis of the colon as a discharge diagnosis. Age- and gender-specific rates of hospitalization for AD were assessed.
Results
174,436 hospitalizations were identified with an increasing rate in 2008–2015 from 39 to 48 per 100,000 inhabitants (p < 0.001). The rate of hospitalization was higher for women, but the increasing trend over time was even more pronounced among men (mean increase per year 3.9% and 2.1% among men and women, respectively) (p < 0.001). The increased rate of hospitalization was accounted for by patients less than 70 years old, especially those under 60. In contrast, the hospitalization rate for older patients (age ≥ 70 years) was higher but remained unchanged during the study period. The number of patients with one hospital admissions was significantly higher than the number of patients with at least two hospitalizations (p < 0.001) and both groups showed a significant and comparable increase year by year. The overall in-hospital mortality rate increased from 1.2 to 1.5% (p = 0.017). More specifically, the increase was observed in patients at their first hospitalization [from 1 to 1.4% (mean increase per year of 3%, p = 0.003)]. An increase in mortality was most evident among women (from 1.4 to 1.8% p = 0.025) and in older patients [age 70–79 years from 1.2 to 1.7% (p = 0.034), ≥ 80 years from 2.9 to 4% (p = 0.001)].
Conclusions
In Italy, between 2008 and 2015, the rate of hospitalization for AD has been constantly increasing due to the hospitalization of younger individuals, especially men. There was a significant increase of in-hospital mortality especially among women, elderly and during the first hospitalization. These findings suggest the need for increased awareness and clinical skills in the management of this common condition.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colonic diverticula are particularly common in Western countries and their prevalence increases with age, affecting up to 60% of individuals over 70 years of age [1]. Although the majority of patients with colonic diverticula remain asymptomatic, about 4% develop acute diverticulitis (AD) [2]. Among gastrointestinal illnesses, diverticulitis is the most common cause of hospitalization in the USA with aggregate hospital costs estimated at $2.6 billion annually [3]. Several epidemiological studies, conducted in Northern Europe and the USA, have documented an increase in hospital admissions for AD in recent years from the 1990s through 2012 [4,5,6,7,8,9,10,11]. This increased rate of hospital admissions is especially evident among women and younger individuals [5,6,7,8, 11]. In Italy, a consensus statement [12] and clinical guidelines [13] about colonic diverticulosis and diverticular disease have been recently published, but no analysis of the trend of hospital admissions for AD has ever been performed.
The primary endpoint of our study was to analyse the nationwide hospital admission rates for AD between 2008 and 2015 in Italy, using administrative data. As secondary endpoint, we investigated the association between hospital admissions for AD with gender, age categories, and in-hospital mortality during admission.
Materials and methods
Data sources and patient population
Data were extracted from the Italian Hospital Information System (HIS) that collects clinical and administrative information regarding each hospital admission of every patient discharged from any hospital in Italy. This data source contains patient demographic data (gender, age), admission and discharge dates, up to six discharge diagnoses [International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM)], and living status at discharge (alive, dead, transferred to another hospital). The National Outcome Program (PNE) of the National Agency for Regional Health Services (AgeNaS) is in charge of the management and analysis of data.
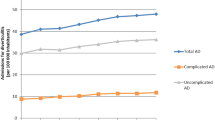
All hospital admissions that occurred between 2008 and 2015 were analysed. Then, we extracted information on every admission with a diagnosis of diverticulitis of the colon [ICD-9-CM code 562.11 (diverticulitis without mention of haemorrhage) and 562.13 (diverticulitis with mention of haemorrhage)] either as a primary diagnosis or as secondary diagnosis but with a complication of diverticulitis as a primary diagnosis. Hospital admissions regarding patients under 18 years of age and those with a diagnosis of colon or rectal cancer (ICD-9-CM 153.0-153.9, 197.5) were excluded.
Rates of hospital admissions were analysed based on the following variables: (1) six age categories (18–39, 40–49, 50–59, 60–69, 70–79, ≥ 80 years); (2) gender. Patients with more than one hospital admission for AD (1+) were also identified for each given year. In-hospital mortality was calculated considering all hospital admissions for AD that ended with the death of the patient as opposed to discharge or transfer.
Statistical analysis
Prevalence rates are reported by 100,000 individuals. Statistical analysis was performed using Student’s t test and the Wald test as appropriate. A two-tailed p value < 0.05 was considered statistically significant. Statistical analysis was performed using Stata 13 Software [14].
Results
Hospital admissions for AD
Between 2008 and 2015, a total of 174,436 patients were hospitalized for AD. Patient characteristics are listed in Table 1. Women (54.9%) were more frequently hospitalized and the median age was 70 years. Over the study period, the number of hospital admissions for AD increased by 30% (from 18,797 to 24,342) (p < 0.001), whereas during the same time, the overall number of all-cause hospitalizations decreased by 25% (from 9,890,961 to 7,827,402) (p < 0.001).
The overall rate of hospital admissions for AD per 100,000 inhabitants was 44 increasing progressively from 39 in 2008 to 48 in 2015, a yearly increase of over 3% (p < 0.001) (Fig. 1a). The overall rate of hospital admissions for AD per 100,000 hospitalizations was 248 increasing from 190 in 2008 to 310 in 2015, with a 7.5% increase per year (p < 0.001) (Fig. 1b).

Hospitalization rate for diverticulitis per 100,000 individuals (a) and per 100,000 total hospitalizations (b)
Rates of hospital admissions for AD by gender and age
Rates of hospital admissions for AD per 100,000 individuals by gender are illustrated in Fig. 2. Women had higher rates of hospital admissions than men (p < 0.001). Rates of hospital admissions for AD increased significantly (p < 0.001) for both gender categories, but to a greater extent among men (mean increase per year 3.9% compared to 2.1% among women).

Prevalence of hospitalization for diverticulitis for 100,000 individuals by gender categories
Rates of hospital admissions for AD per 100,000 individuals by age categories are reported in Fig. 3. Rates were higher for patients over 80 years old (mean number of hospitalizations 152.94 ± SD 2.87) and for those 70–79 years old (mean number of hospitalizations 99.23 ± SD 1.49). However, the rates in these two age groups were unchanged between 2008 and 2015 with a no significant 0.2% decrease per year for both groups. Individuals 18–39 years old experienced the lowest rate of hospitalizations for AD (mean 6.32 ± SD 0.93). However, in this age category, the rate of hospital admissions for AD increased over the study period, with a mean increase of 6.6% per year (p < 0.001). A statistically significant increase in the rate of hospital admissions was also documented for patients 60–69 years old (mean increase 2.7% per year), patients 50–59 years (mean increase 5.1% per year), and it was greatest for patients 40–49 years old (mean increase 7.1% per year).

Prevalence of hospitalization for acute diverticulitis per 100,000 individuals by age categories
Figure 4 illustrates the hospitalization rate for AD in age categories, stratified by sex. Among patients below the age of 60 men predominated and the male-to female ratio for admissions was 4.32 (95% CI 4.09–4.58), 2.44 (95% CI 2.36–2.52) and 1.24 (95% CI 1.21–1.27) for patients 18–39, 40–49 and 50–59 years, respectively. In contrast, among those over 60 years old women predominated with a male–female ratio of 0.87 (95% CI 0.85–0.89), 0.78 (95% CI 0.77–0.80), 0.80 (95% CI 0.78–0.81) for patients 60–69, 70–79 and ≥ 80 years, respectively.

Hospitalization rate for acute diverticulitis in age categories, stratified by sex
Number of hospital admissions for AD for each patient
Between 2008 and 2015, the annual number of patients with one hospital admission for AD increased from 16,529 to 21,279 (p < 0,001) (Fig. 5a) and the number of those with at least two hospital admissions increased from 1048 to 1519 (p < 0.001) (Fig. 5b). The growth trend of both groups was comparable with no significant differences. The number of patients with one hospital admission was significantly higher than the number of patients with at least two hospitalizations (p < 0.001).

Trend of patients with 1 (a) and with ≥ 2 hospitalizations (b) from 2008 to 2015
In-hospital mortality
During the study period, the overall in-hospital mortality rate increased significantly from 1.2 to 1.5% (p = 0.017). An increase of in-hospital mortality was only evident for women (p = 0.025) and for patients in age categories above 70 years (Table 2). Between 2008 and 2015, in-hospital mortality of patients with one hospitalization increased from 1 to 1.4% (mean increase per year of 3%, p = 0.003) whereas in patients with ≥ 2 hospitalization it was almost stable changing from 1.2 to 1.3% (mean increase per year of 1.4%, p = 0.717).
Discussion
The findings of this Italian nationwide study show a significant increase of the number and the rate of hospital admission for AD between 2008 and 2015 of 30% and 3.2% per year respectively, while in the same period, the global number of hospital admissions in Italy significantly declined by 25%. These temporal trends suggest true changes in the epidemiology of AD in terms of incidence and severity of the disease rather than a lower threshold for hospitalization.
Our figures are consistent with those obtained by several studies from other Western countries (Table 3). However, these data are not fully comparable due to the different organizations of the health systems and the heterogeneous administrative source. Some countries manage health care according to the Beveridge model (the government provides funding through tax payments), some according to the Bismarck model (insurance system financed jointly by employers and employees), and others by means of a hybrid system.
Our study reports the largest national analysis from a Beveridge-type system. Among similar countries, Paterson et al. [8] investigated the burden of diverticular disease in Scotland over a decade founding an average increase in the incidence of hospital admissions for AD of 4.5% per year but the sample includes elective day-case admissions for colonoscopy. In New Zealand, Vather et al. [17] described the trend of acute hospital admission for diverticular disease showing a steady increase over the 12.5-year study period but potential bias could affect the data extraction from the national database. It does not reliably differentiate diverticular bleeding from acute diverticulitis and does not provide for mandatory recording of the secondary diagnoses. Jeyarajah and Papagrigoriadis [5] found a remarkable threefold increase of hospital admissions over a decade in a small series from a single institution.
Several investigations examined the same subject in the USA and reported similar epidemiological trends of admission for AD in the context of a hybrid health system [6, 7, 9, 11, 15,16,17]. Most of them [6, 7, 9, 15] were able to analyse very large sample using the National Inpatient Sample database, which is a nationally representative sample of approximately 20% of the hospital discharges within the USA [6]. Our source of data was able to collect every hospital admission to any Italian hospital, avoiding any potential selection bias due to their public or private nature rather than to the regional areas (north / south, urban/rural).
As previously reported in the literature, we found that the overall rate of hospital admissions for AD was significantly higher among women than men. The trend significantly increases year by year for both gender group, but unlike other authors [4, 7, 9], we found that the male–female ratio constantly decreased over the study period.
The analysis of our data categorized by age shows that elderly patients over 70 years of age had the highest rate of hospital admission during the 8-year period but the trend is stable, whereas the increase of the number of hospitalizations over time is to be entirely attributed to the younger cohorts of patients under the age of 60. These findings are consistent with previous epidemiological studies carried out in other European countries and in USA and Jeyarajah and Papagrigoriadis [5] reported that the mean age at admission decreased between 1995 and 2004 [5, 6, 8, 9, 11, 17, 18].
Nguyen and colleagues [7] and Kang and colleagues [4] found that in the age category < 45 years, AD-related hospital admissions were more common among men whilst the opposite was true in older age groups; Talabani et al. [10] found that the effect of age over time is linear for females and non linear for the males. Similarly, the stratification of our sample by sex and age demonstrates that AD is male predominant among younger patients and female predominant among older ones. There is no clear-cut explanation of these epidemiological features but they suggest two pathways in the pathogenesis of the disease: the first is age-related as the prevalence of the diverticular disease rises with age [1], the second is probably related to different risk factors such as fibre intake, dietary habits, obesity, colonic functional or structural abnormalities, but further studies are needed to elucidate these issues. Ethnic susceptibility was suggested in the past but to date no definitive conclusion regarding this have been drawn [9, 19]. In our study, a large cohort of patients from a Mediterranean country was investigated for the first time and our results show that the epidemiological trends are similar to those in other Western developed countries. This could give rise to debate about the supposed protective role of the so-called “Mediterranean diet”, vs. the dietary habits of the fast-food generation.
According to the natural history of diverticulitis, the number of patients with one hospital admission was significantly higher than the number of patients with two or more hospitalizations. The significantly increasing annual number of patients with one hospital admission during the study period confirms that the growing overall hospitalization for AD is related to a true rising incidence of the disease.
Overall in-hospital mortality significantly increased from 1.2% to 1.5%: the increased rate was observed exclusively in the patients with one admission, confirming that the most severe presentation of AD is during the first episodes [20,21,22]. This increase in hospital mortality over time was not observed by similar studies [4, 6, 18] and deserves further investigation. Mortality rates were higher in patients 70 + years old and in women which is consistent with results of other studies [4, 6, 8]. A further analysis, already planned, about complications of AD from this database, will give more detailed explanations about in-hospital mortality.
Conclusions
This study investigated the largest sample of patients hospitalized for AD in a Beveridge-type health system and it is the first report from a Mediterranean country. In Italy, between 2008 and 2015, the rate of hospital admissions for AD significantly increased. The hospitalization rate was higher in the elderly ≥ 70 years of age but its rise over time was due to the increasing hospitalization of younger individuals, especially men. The causes of this emerging pattern are unknown but these findings suggest that there are two pathways in the pathogenesis of AD. Furthermore, these results emphasise the need for an increased awareness regarding AD and for the development of appropriate clinical skills in the management of this increasingly common clinical entity.
References
Stollman N, Raskin JB (2004) Diverticular disease of the colon. Lancet 363:631–639
Shahedi K, Fuller G, Bolus R et al (2013) Long-term risk of acute diverticulitis among patients with incidental diverticulosis found during colonoscopy. Clin Gastroenterol Hepatol 11:1609–1613
Peery AF, Dellon ES, Lund J et al (2012) Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 143:1179–1187
Kang JY, Hoare J, Tinto A et al (2003) Diverticular disease of the colon—on the rise: a study of hospital admissions in England between 1989/1990 and 1999/2000. Aliment Pharmacol Ther 17:1189–1195
Jeyarajah S, Papagrigoriadis S (2008) Diverticular disease increases and effects younger ages: an epidemiological study of 10-year trends. Int J Colorectal Dis 23:619–627
Etzioni DA, Mack TM, Beart RW Jr, Kaiser AM (2009) Diverticulitis in the United States: 1998–2005: changing patterns of disease and treatment. Ann Surg 249:210–217
Nguyen GC, Sam J, Anand N (2011) Epidemiological trends and geographic variation in hospital admissions for diverticulitis in the United States. World J Gastroenterol 17:1600–1605
Paterson HM, Arnott ID, Nicholls RJ et al (2015) Diverticular disease in Scotland: 2000–2010. Colorectal Dis 17:329–334
Wheat CL, Strate LL (2016) Trends in hospitalization for diverticulitis and diverticular bleeding in the United States from 2000 to 2010. Clin Gastroenterol Hepatol 14:96–103
Talabani A, Lydersen S, Endreseth BH, Edna TH (2014) Major increase in admission- and incidence rates of acute colonic diverticulitis. Int J Colorectal Dis 29:937–945
Bharucha AE, Parthasarathy G, Ditah I et al (2015) Temporal trends in the incidence and natural history of diverticulitis: a population-based study. Am J Gastroenterol 110:1589–1596
Cuomo R, Barbara G, Pace F et al (2014) Italian consensus conference for colonic diverticulosis and diverticular disease. United Eur Gastroenterol J 2:413–442
Binda GA, Cuomo R, Laghi A et al (2015) Italian Society of Colon and Rectal Surgery. Practice parameters for the treatment of colonic diverticular disease: Italian Society of Colon and Rectal Surgery (SICCR) guidelines. Tech Coloproctol 19:615–626
StataCorp (2013) Stata statistical software: release 13. StataCorp LP, College Station
Masoomi H, Buchberg B, Nguyen B, Tung V, Stamos MJ, Mills S (2011) Outcomes of laparoscopic versus open colectomy in elective surgery for diverticulitis. World J Surg 35:2143–2148
Simianu VV, Fichera A, Bastawrous AL et al (2016) Number of diverticulitis episodes before resection and factors associated with earlier interventions. JAMA Surg 151:604–610
Vather R, Broad JB, Jaung R, Robertson J, Bissett IP (2015) Demographics and trends in the acute presentation of diverticular disease: a national study. ANZ J Surg 85:744–748
Bollom A, Austrie J, Hirsch W et al (2017) Emergency Department burden of diverticulitis in the USA, 2006–2013. Dig Dis Sci 62:2694–2703
Kyle J, Adesola AO, Tinckler LF, de Beaux J (1967) Incidence of diverticulitis. Scand J Gastroenterol 2:77–80
Janes S, Meagher A, Frizelle FA (2005) Elective surgery after acute diverticulitis. Br J Surg 92:133–142
Chapman JR, Dozois EJ, Wolff BG, Gullerud RE, Larson DR (2006) Diverticulitis: a progressive disease? Do multiple recurrences predict less favorable outcomes? Ann Surg 243:876–830
Ritz JP, Lehmann KS, Frericks B, Stroux A, Buhr HJ, Holmer C (2011) Outcome of patients with acute sigmoid diverticulitis: multivariate analysis of risk factors for free perforation. Surgery 149:606–613
Funding
No source of funding has been provided.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human partecipants performed by any authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Binda, G.A., Mataloni, F., Bruzzone, M. et al. Trends in hospital admission for acute diverticulitis in Italy from 2008 to 2015. Tech Coloproctol 22, 597–604 (2018). https://doi.org/10.1007/s10151-018-1840-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-018-1840-z