
Abstract
The third version of the Japan Society of Gynecologic Oncology guidelines for the treatment of uterine body neoplasms was published in 2013. The guidelines comprise nine chapters and nine algorithms. Each chapter includes a clinical question, recommendations, background, objectives, explanations, and references. This revision was intended to collect up-to-date international evidence. The highlights of this revision are to (1) newly specify costs and conflicts of interest; (2) describe the clinical significance of pelvic lymph node dissection and para-aortic lymphadenectomy, including variant histologic types; (3) describe more clearly the indications for laparoscopic surgery as the standard treatment; (4) provide guidelines for post-treatment hormone replacement therapy; (5) clearly differentiate treatment of advanced or recurrent cancer between the initial treatment and the treatment carried out after the primary operation; (6) collectively describe fertility-sparing therapy for both atypical endometrial hyperplasia and endometrioid adenocarcinoma (corresponding to G1) and newly describe relapse therapy after fertility-preserving treatment; and (7) newly describe the treatment of trophoblastic disease. Overall, the objective of these guidelines is to clearly delineate the standard of care for uterine body neoplasms in Japan with the goal of ensuring a high standard of care for all Japanese women diagnosed with uterine body neoplasms.
Avoid common mistakes on your manuscript.
Introduction
Endometrial cancer is one of the most common malignancies of the female genital tract. In Japan, the age-adjusted incidence rate of endometrial cancer was 17.2 (per 100,000 women) in 2011, indicative of a four- to five-fold increase over the past three decades [1]. It is estimated that 10,300 new uterine cancer cases occurred in 2014 [2], with 2,243 deaths resulting from the disease [1]. Surgery, chemotherapy, radiation, and hormone therapy are used either alone or sequentially to treat endometrial cancer. Surgery is recommended for medically operable disease. When the disease is limited to the uterus, then hysterectomy, bilateral salpingo-oophorectomy, and pelvic/para-aortic lymph node dissection are recommended. However, whether to add para-aortic lymphadenectomy to pelvic node dissection remains controversial. Furthermore, there are differences in the adjuvant therapies employed in Japan and in Western countries. In Western countries, radiation therapy is the mainstay of postoperative adjuvant therapy, whereas in Japan, chemotherapy is more frequently performed. These differences are one reason why evidence from Western countries cannot be directly applied to the development of recommendations for Japanese patients. Under such circumstances, the first edition of the Japan Society of Gynecologic Oncology (JSGO) guidelines for the treatment of endometrial cancer was published in 2006 and revised in 2009 [3]. The second revised version contained two new sections—the treatment of mesenchymal tumors such as leiomyosarcoma and the treatment of serous and clear-cell adenocarcinoma [3].
The third edition of the JSGO guidelines for the treatment of uterine body neoplasms was published in 2013. The guidelines comprise nine chapters and nine algorithms. The highlights of this revision are indicated below.
-
1.
Chapter 1: Overview of guidelines. New specification of costs and conflicts of interests are identified.
-
2.
Chapter 2: Initial treatment for endometrial cancer. The clinical significance of pelvic lymph node dissection and para-aortic lymphadenectomy, including variant histologic types, are described in detail. An additional indication for laparoscopic surgery as the standard treatment is also described more clearly. Finally, the optimal treatment for patients in whom it is evident that endometrial cancer is present after hysterectomy is also described.
-
3.
Chapter 3: Postoperative adjuvant therapy for endometrial cancer. Chemotherapy is described as having priority over radiation therapy in line with the present conditions in Japan, including the above-mentioned variant histologic type.
-
4.
Chapter 4: Post-treatment surveillance for endometrial cancer. The guidelines for hormone replacement therapy after treatment are described first based on “The Guidelines for Hormone Replacement Therapy 2012,” edited by the Japan Society of Obstetrics and Gynecology (JSOG) and the Japan Society for Menopause and Women’s Health.
-
5.
Chapter 5: Treatment for advanced or recurrent endometrial cancer. The difference between the initial treatment and the treatment carried out after the primary operation is clearly described.
-
6.
Chapter 6: Fertility-sparing therapy. Two diseases, namely atypical endometrial hyperplasia and endometrioid adenocarcinoma (corresponding to G1), are collectively described. Relapse therapy after the fertility-preserving treatment is also newly described.
-
7.
Chapter 7: Treatment of uterine carcinosarcoma and uterine sarcoma. This chapter was first included in the 2009 version. In addition, chapter 8 “Treatment of trophoblastic disease” is newly described to support “the general roles for clinical and pathological management of trophoblastic diseases (the third edition)”.
Chapter 1: Overview of guidelines
1. How to use these guidelines
These guidelines are intended for doctors (general practitioners and specialists) who provide medical care for patients with uterine tumors and are meant to provide useful treatment methods by integrating previous evidence of benefit. However, the guidelines are not intended to be limited to the therapies listed. The main purposes of the guidelines are (1) to indicate current treatment that is considered appropriate for endometrial cancer, carcinosarcoma/sarcoma, and trophoblastic diseases; (2) to reduce differences in therapy among institutions; (3) to improve the prognosis and safety of treatments; (4) to reduce the economic and psychosomatic burden of patients by promoting the performance of appropriate treatment; and (5) to aid mutual understanding of healthcare professionals and patients.
2. Intended audience
These guidelines are intended for practicing physicians engaged in the treatment of patients with endometrial cancer, carcinosarcoma/sarcoma, and trophoblastic diseases.
3. Diseases addressed by these guidelines
Endometrial cancer was mainly described in the first edition. Variant histologic types of uterine cancer and carcinosarcoma/sarcoma were added in the revised edition. Trophoblastic disease was added to the latest revised edition, and these tumors and their recurrence are described in these guidelines. The characteristics of these guidelines are as follows. Initial, postoperative and advanced/recurrent treatment of variant histologic type was discussed in two separate chapters. Lymph node dissection and laparoscopic surgery are described in detail. In addition, postoperative hormone adjuvant therapy is described in the chapter regarding post-treatment follow-up. Atypical endometrial hyperplasia is included in the chapter regarding fertility-sparing therapy. The chapter regarding treatment of trophoblastic disease is based on the third edition of the general rules for clinical anc pathological management of trophoblastic diseases by Japan society of obstetrics and gynecology and the Japanese pathological society.
4. Basic policies in creating the guidelines
To create these guidelines, the Guidelines Formulation Committee and Evaluation Committee were independently established within the Committee for Treatment Guidelines for Uterine Body Neoplasms. The initial draft was created after a thorough evaluation. Opinions from within and outside the JSGO were incorporated into the final draft. The guidelines were published after approval by the JSGO. Much of the evidence that formed the basis for the Japanese guidelines was obtained from clinical trials in Western countries. However, given the differences between practice in Japan and other countries, the consensus regarding clinical practice in Japan took priority in the event of discrepancies. Wherever possible, high-level Japanese evidence was used to formulate these guidelines. The following items are assumed to underlie the basic policy of the guidelines:
-
(1)
These guidelines were created in accordance with the principles of evidence-based medicine, considered to be the international standard for creating clinical practice guidelines.
-
(2)
Searches were performed of data and literature published until December 2011, including Japanese and non-Japanese studies in Japan and overseas.
-
(3)
The collected evidence was evaluated for quality using the criteria of the Japan Society of Clinical Oncology and its Formulation Committee of Clinical Practice Guidelines for the Use of Anticancer Agents [4, 5]. However, some of the contents were modified in line with these guidelines (Table 1).
Table 1 Classification of evaluation criteria for evidence quality -
(4)
The strengths of the recommendations in our guidelines were also determined by the recommendation criteria of the Japan Society of Clinical Oncology and its Formulation Committee of Clinical Practice Guidelines for the Use of Anticancer Agents. These were modified while referring to the “Minds clinical practice guidelines 2007” [6] (Table 2).
Table 2 Classification of recommendation categories -
(5)
The surgical staging criteria described in the 2013 edition were based on the surgical staging system developed in 2008 by the International Federation of Gynecology and Obstetrics (FIGO). In the text, we did not use clinical stage (JSOG 1983, FIGO 1982), but used a description ‘considered to be stage X preoperatively’ instead.
-
(6)
Therapy is often difficult to administer under the Japanese medical care insurance system. In this regard, the present guidelines follow the Formulation Committee of Clinical Practice Guidelines for the Use of Anticancer Agents.
5. Disclosure of information
These guidelines are published as a pamphlet and are shown on the homepage of JSCO to facilitate widespread use.
6. Responsibility for treatment
The JSGO bears the responsibility for the content and descriptions of these guidelines. However, the final decision to use these guidelines should be made by the individual user. Thus, the responsibility for the treatment outcomes should be directly attributed to the person in charge.
7. Revision
-
(1)
These guidelines are continuously being revised by the Committee for Treatment Guidelines for Uterine Body Neoplasms with medical advances and medical changes.
-
(2)
Newly accumulated evidence after publishing these guidelines is saved in a database.
-
(3)
Any associated information regarding clinical inconvenience occurring with the use of these guidelines is collected.
-
(4)
Revision work is conducted by the Guidelines Formulation Committee and Evaluation Committee based on new evidence and information. Opinions from associated academic societies, groups or JSGO members are widely gained.
-
(5)
After the above-mentioned process, the Committee for Treatment Guidelines for Uterine Body Neoplasms provides a revised version with the approval of the JSGO.
8. Funding
Preparation of these guidelines was funded by the JSGO. We also acknowledge support by grants from the Ministry of Health, Labour and Welfare and H24-Clinical Cancer Research-001 (chief researcher, Koichi Hirata). The expense incurred had no influence on the contents of these guidelines.
9. Conflicts of interest
The Board of the Society Conflict of Interest Committee confirmed the absence of any conflicts of interest. Although some committees had conflicts of interest through study or lecture activity with the company, the contents of these guidelines are based on scientific evidence and thus unaffected by any interest with specific groups or products.
10. Summary of recommendations
In general, each chapter comprises a clinical question (CQ), recommendations, background, objectives, explanations, and references. This article summarizes the guidelines in a question-and-answer format. Recommendations from each chapter are listed below under their respective chapter titles.
11. Algorithms
These guidelines contain the following nine algorithms:
-
1.
Initial treatment for patients with endometrial cancer considered to be stage I or II preoperatively (Fig. 1).
Fig. 1 
Initial treatment for patients with endometrial cancer considered to be stage I or II preoperatively. a Radiation therapy or chemotherapy are considered when surgery is impossible. b Pelvic and para-aortic lymphadenectomy/lymph node biopsy and omentectomy are considered in addition to total hysterectomy with bilateral salpingo-oophorectomy for patients with serous adenocarcinoma or clear-cell adenocarcinoma. CQ clinical question
-
2.
Initial treatment for patients who are confirmed as having endometrial cancer after hysterectomy (Fig. 2).
Fig. 2 
Initial treatment for patients who are confirmed as having endometrial cancer after hysterectomy. a Postoperative chemotherapy is considered for positive lymphovascular space invasion
-
3.
Initial treatment for patients with endometrial cancer considered to be stage III or IV preoperatively (Fig. 3).
Fig. 3 
Initial treatment for patients with endometrial cancer considered to be stage III or IV preoperatively. a Because serous adenocarcinoma/clear cell adenocarcinoma is likely to become disseminated, the omentectomy is useful for a diagnosis. b Surgery is considered for the purpose of hemostasis even if there is extra-peritoneal metastasis or liver metastasis
-
4.
Postoperative adjuvant treatment for endometrial cancer (Fig. 4, Table 3).
Fig. 4 
Postoperative adjuvant treatment for endometrial cancer
Table 3 Classification of postoperative recurrence risk of endometrial cancer -
5.
Treatment of recurrent endometrial cancer (Fig. 5).
Fig. 5 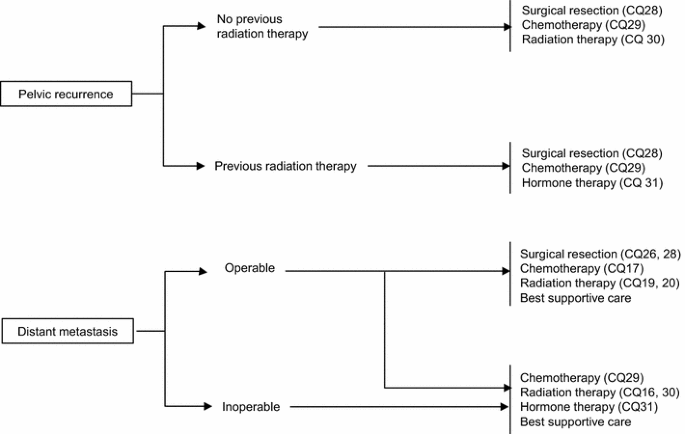
Treatment of recurrent endometrial cancer
-
6.
Strategies for fertility-sparing therapy (atypical endometrial hyperplasia and endometrioid adenocarcinoma; corresponding to G1) (Fig. 6).
Fig. 6 
Strategies for fertility-sparing therapy (atypical endometrial hyperplasia and endometrioid adenocarcinoma; corresponding to G1)
-
7.
Treatment for uterine carcinosarcoma (Fig. 7).
Fig. 7 
Treatment for uterine carcinosarcoma
-
8.
Treatment for uterine sarcoma (Fig. 8).
Fig. 8 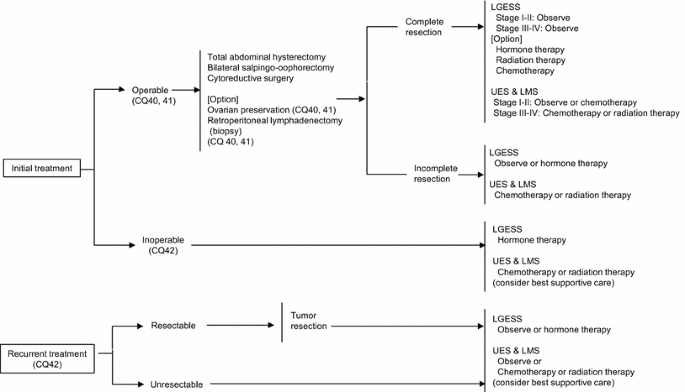
Treatment for uterine sarcoma. LGESS low-grade endometrial stromal sarcoma, UES undifferentiated endometrial sarcoma, LMS leiomyosarcoma
-
9.
Treatment for choriocarcinoma (Fig. 9).
Fig. 9 
Treatment for choriocarcinoma









Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Recommendations:
-
1.
Abdominal total hysterectomy (extrafascial technique) is recommended (Grade B).
-
2.
Modified radical (extended) hysterectomy is also considered (Grade C1).
[See Fig. 1].
CQ02. Which surgical hysterectomy techniques are recommended for patients considered to be stage II?
Recommendations:
Either radical hysterectomy or modified radical hysterectomy should be considered for patients with clinically apparent cervical stromal involvement (Grade C1).
[See Fig. 1].
CQ03 What are the benefits of pelvic lymphadenectomy?
Recommendations:
-
1.
The diagnostic significance of pelvic lymph node dissection in the determination of correct surgical staging has been established (Grade A).
-
2.
The therapeutic benefits of pelvic lymphadenectomy are not established. However, this procedure should be considered in intermediate-risk or high-risk patients (Grade C1).
[See Fig. 1].
CQ04 What are the benefits of para-aortic lymphadenectomy (biopsy)?
Recommendations:
-
1.
Para-aortic lymphadenectomy (biopsy) is necessary to determine correct surgical staging (Grade A).
-
2.
The therapeutic benefits of para-aortic lymphadenectomy (lymph node biopsy) are not established. However, this procedure should be considered in intermediate-risk or high-risk patients (Grade C1).
[See Fig. 1].
CQ05 Is omentectomy necessary?
Recommendations:
-
1.
Searching the omentum by careful ocular inspection and palpation is necessary in all cases. When metastasis is suspected, omentectomy should be performed to determine the correct stage (Grade A).
-
2.
Omentectomy is considered when deep myometrial invasion, positive intraoperative peritoneal cytology, Grade 3 endometrial carcinoma, serous or clear cell adenocarcinoma, or macroscopic extrauterine disease is present, even if no gross abnormalities are detected in the omentum (Grade C1).
[See Fig. 1].
CQ06 Is ovarian preservation possible?
Recommendations:
-
1.
In principle, bilateral adnexectomy is conducted to determine the correct surgical stage during initial treatment (Grade A).
-
2.
Ovarian preservation is considered after having explained the risks to young patients with well-differentiated tumors and shallow myometrial invasion (Grade C1).
[See Fig. 1].
CQ07 What surgical technique is recommended for serous adenocarcinoma and clear-cell adenocarcinoma?
Recommendations:
-
1.
Total hysterectomy with bilateral salpingo-oophorectomy is recommended (Grade B).
-
2.
Additionally, pelvic and para-aortic lymphadenectomy (lymph node biopsy) and omentectomy are considered (Grade C1).
[See Fig. 1].
CQ08 Is an inguinal lymph node biopsy noted in the surgical staging guidelines necessary?
Recommendations:
-
1.
When an enlarged inguinal lymph node is detected in preoperative imaging such as a computed tomography (CT) scan, then a biopsy is recommended to determine the surgical stage (Grade A).
-
2.
When an enlarged inguinal lymph node is not detected, the benefits of biopsy are not evident. Therefore, routine inguinal lymph node biopsy is not recommended (Grade C2).
[See Fig. 1].
CQ09 What is the significance of preoperative diagnostic imaging?
Recommendations:
-
1.
Evaluation for myometrial invasion and cervical invasion by preoperative magnetic resonance imaging (MRI) is recommended (Grade A).
-
2.
Evaluation for lymph node metastases or distant metastases by preoperative imaging such as CT scan or MRI is recommended (Grade C1).
CQ10 Is intraoperative frozen-section diagnosis useful to determine the optimal operative method?
Recommendations:
-
1.
Intraoperative frozen-section diagnosis may be useful for predicting high-risk disease for which pelvic and para-aortic lymphadenectomy or omentectomy would be appropriate (Grade C1).
-
2.
Intraoperative frozen-section diagnosis is not recommended for a definite diagnosis in terms of histological type, histologic differentiation, and myometrial invasion (Grade C2).
CQ11 Should intraoperative frozen-section diagnosis be performed to detect lymph node metastases?
Recommendations:
-
1.
Intraoperative frozen-section diagnosis is useful in the diagnosis of metastasis when apparent lymph node enlargement is detected (Grade C1).
-
2.
There is insufficient evidence to recommend modification of the surgical technique based on the lymph node metastasis status assessed with intraoperative frozen sections. It is not recommended in daily practice (Grade C2).
CQ12 Can lymphadenectomy be omitted if a sentinel node biopsy is performed?
Recommendations:
There is insufficient evidence to omit retroperitoneal lymphadenectomy (lymph node biopsy) based on the sentinel lymph node status. It is not recommended in daily practice (Grade C2).
CQ13 Should peritoneal cytology be performed at the same time as surgery?
Recommendations:
The performance of peritoneal cytology should be continued regardless of whether it is a prognostic factor. Positive cases should be reported separately from surgical staging (Grade A).
CQ14 Can laparoscopic surgery become a standard surgical technique?
Recommendations:
-
1.
Laparoscopic surgery is considered for patients with atypical endometrial hyperplasia or an early endometrial cancer limited to the uterus (stage I) (Grade B).
-
2.
Laparoscopic surgery is not recommended for patients with advanced endometrial cancer (Grade C2).
[See Fig. 1].
Additional statement
-
It is advisable to decide upon the appropriate surgical procedure and to use a surgical team which includes a qualified surgeon of the Japan Society of Gynecologic and Obstetric Endoscopy and Minimally Invasive Therapy or the Japan Society for Endoscopic Surgery, and board-certified gynecologic oncologists of the JSGO. Otherwise, it is recommended that the surgery be performed according to the instructions of these physicians.
-
The decision regarding the appropriate surgical procedure for laparoscopic surgery is carried out according to a basic policy described in CQ01, CQ03, and CQ04.
CQ15 How should patients be treated who are confirmed as having endometrial cancer after hysterectomy?
Recommendations:
-
1.
Follow-up is possible when an extrauterine lesion is negative for myometrial invasion <1/2, G1, or G2. However, adjuvant therapy is considered when vascular invasion is detected (Grade C1).
-
2.
Reoperation is considered when an extrauterine lesion is suspected or when G3, a variant histologic type, or stage >IB disease is present, even if myometrial invasion is <1/2. Based on the results, restaging is recommended, metastasis is confirmed, and the necessity for adjuvant therapy should be discussed.
[See Fig. 2].
CQ16 What are the indications for definitive radiation therapy?
Recommendations:
Radiation therapy is considered when surgery is undesirable because of advanced age, complications, or when patients have unresectable tumors (Grade C1).
[See Fig. 3].
Chapter 3: Postoperative adjuvant therapy for endometrial cancer (including histologic variant type)
CQ17 What are the indications and drugs recommended for postoperative chemotherapy?
Recommendations:
-
1.
Chemotherapy with adriamycin (doxorubicin hydrochloride) and cisplatin is recommended for high-risk patients (Grade B).
-
2.
Taxane-based and platinum-based drug combination therapy (e.g., paclitaxel/carboplatin) is also considered (Grade C1).
-
3.
Postoperative adjuvant chemotherapy is considered for intermediate-risk patients (Grade C1).
-
4.
Postoperative adjuvant chemotherapy is not recommended for low-risk patients (Grade D).
CQ18 Is hormone therapy effective as postoperative adjuvant therapy?
Recommendations:
Postoperative progesterone therapy is not recommended (Grade D).
CQ19 What are the indications for postoperative whole-pelvis external-beam irradiation?
Recommendations:
-
1.
Postoperative whole-pelvis external-beam irradiation is considered for patients with risk factors for recurrence (Grade C1).
-
2.
Postoperative vaginal brachytherapy is considered to reduce the risk of vaginal recurrence (Grade C1).
CQ20 What are the indications for postoperative irradiation of the para-aortic lymph node region and whole abdomen?
Recommendations:
-
1.
Postoperative irradiation of the para-aortic lymph node region is considered for patients with advanced diseases (Grade C1).
-
2.
Postoperative whole-abdominal irradiation may be used in patients with a variant histologic type, but it is not common in daily practice in Japan (Grade C2).
Chapter 4: Post-treatment surveillance for endometrial cancer
CQ21 What intervals are recommended for post-treatment surveillance?
Recommendations:
Standard intervals between routine follow-up appointments are shown below (Grade C1):
-
1.
Every 1−3 months for the first 1–3 years after treatment.
-
2.
Every 6 months for the fourth and fifth years after treatment.
-
3.
Annually from the sixth year after treatment.
[See Fig. 4].
CQ22 Should pelvic examinations and vaginal vault smears be performed at post-treatment follow-up?
Recommendations:
-
1.
Pelvic examination should be performed to diagnose recurrence in the pelvis (Grade A).
-
2.
Vaginal vault smears are considered to detect vaginal stump recurrence (Grade C1).
[See Fig. 4].
CQ23 Should serum tumor markers be measured at post-treatment follow-up?
Recommendations:
Measurement of CA-125 or CA19-9 is considered in post-treatment follow-up (Grade C1).
[See Fig. 4].
CQ24 Should diagnostic imaging be performed in post-treatment follow-up?
Recommendations:
-
1.
Annual chest X-rays are considered for early detection of recurrence (Grade C1).
-
2.
Diagnostic imaging methods such as MRI or CT scan are recommended when recurrence is clinically suspected (Grade B).
[See Fig. 4].
CQ25 Is hormone replacement therapy recommended after treatment?
Recommendations:
Hormone replacement therapy after treatment is carefully considered after having explained the advantages and disadvantages to the patient (Grade C1).
Chapter 5: Treatment for advanced or recurrent endometrial cancer
CQ26 What are the indications for surgery for clinical stages III and IV?
Recommendations:
Surgery is considered whenever a hysterectomy and cytoreduction are possible (Grade C1).
[See Fig. 3].
CQ27 Should neoadjuvant chemotherapy or preoperative radiation therapy be conducted for advanced cancer?
Recommendations:
-
1.
Preoperative chemotherapy is considered in patients with peritoneal dissemination (Grade C1).
-
2.
Preoperative radiation therapy may be conducted for patients with cervical invasion and enlargement; however, it is not common in daily practice in Japan (Grade C2).
[See Fig. 3].
CQ28 What are the indications for surgery for recurrent cancer?
Recommendations:
-
1.
Surgical resection is considered for patients with pelvic recurrence without obvious distant metastasis (Grade C1).
-
2.
Partial resection of the lung is also considered for patients with a few small lung metastases (Grade C1).
[See Fig. 5].
CQ29 Should chemotherapy be conducted for advanced cancer of imperfect resection and recurrent cancer?
Recommendations:
-
1.
Chemotherapy is recommended (Grade B).
-
2.
Paclitaxel/carboplatin, doxorubicin/cisplatin, or paclitaxel/doxorubicin/cisplatin is considered for patients with advanced diseases (Grade C1).
-
3.
Paclitaxel/carboplatin, doxorubicin/cisplatin, or monotherapy is considered for patients with recurrent cancer by taking the situation of the patient and the initial treatment into consideration (Grade C1).
CQ30 Should radiation therapy be conducted for recurrent and inoperable advanced cancer?
Recommendations:
-
1.
Radiation therapy is recommended for patients with recurrence at the vaginal cuff (Grade B).
-
2.
Radiation therapy is considered as a palliative option for recurrent cancer, unresectable advanced cancer, and metastatic cancer (Grade C1).
CQ31 Should hormone therapy be conducted for advanced and recurrent cancer?
Recommendations:
Progesterone therapy is considered for patients with endometrioid adenocarcinoma (G1) and advanced or recurrent cancer with positive progesterone receptors (Grade C1).
Chapter 6: Fertility-sparing therapy
CQ32 When patients with atypical endometrial hyperplasia desire fertility preservation, is progesterone therapy recommended?
Recommendations:
Progesterone therapy is considered in patients with atypical endometrial hyperplasia (Grade C1).
[See Fig. 6].
CQ33 When patients with endometrioid adenocarcinoma (corresponding to G1) desire fertility preservation, is progesterone therapy recommended?
Recommendations:
Progesterone therapy is considered for patients with endometrioid adenocarcinoma (corresponding to G1) suspected to be confined to the endometrium (Grade C1).
[See Fig. 6].
CQ34 What are suitable follow-up periods and examinations?
Recommendations:
Endometrial biopsy and transvaginal ultrasonography are considered every 3 months after completion of progesterone therapy (Grade C1).
[See Fig. 6].
CQ35 What treatments are recommended for patients with recurrence after fertility preservation therapy?
Recommendations:
-
1.
Total hysterectomy is recommended for patients with recurrent disease, an incomplete response, or progressive disease (Grade B).
-
2.
The effectiveness of retreatment with progesterone has not been established in patients with recurrent disease. Retreatment with progesterone is not recommended in routine practice (Grade C2).
[See Fig. 6].
CQ36 Is ovulation induction permissible in patients after fertility preservation therapy?
Recommendations:
Induction of ovulation for pregnancy is considered (Grade C1).
[See Fig. 6].
Chapter 7: Treatment of uterine carcinosarcoma and uterine sarcoma
CQ37 What surgical techniques are recommended for uterine carcinosarcoma?
Recommendations:
-
1.
Total hysterectomy with bilateral salpingo-oophorectomy should be performed (Grade B).
-
2.
In addition to the surgical method mentioned above, pelvic and para-aortic lymphadenectomy (biopsy) are recommended (Grade C1).
-
3.
Radical hysterectomy or modified radical hysterectomy is considered for patients with obvious cervical stromal invasion in whom complete resection is anticipated (Grade C1).
[See Fig. 7].
CQ38 What postoperative adjuvant therapy is recommended for uterine carcinosarcoma?
Recommendations:
-
1.
When postoperative chemotherapy is selected, regimens including ifosfamide, platinum-based drugs, and paclitaxel are considered (Grade C1).
-
2.
Radiation therapy (whole-pelvis external-beam irradiation) is also considered (Grade C1).
[See Fig. 7].
CQ39 What treatments are recommended for advanced and recurrent uterine carcinosarcoma?
Recommendations:
-
1.
If total hysterectomy and cytoreductive surgery are possible, surgical treatment is recommended (Grade C1).
-
2.
Regimens including ifosfamide, platinum-based drugs, and paclitaxel are recommended for chemotherapy in patients with advanced or recurrent disease (Grade C1).
[See Fig. 7].
CQ40 What surgical techniques and postoperative adjuvant therapy are recommended for uterine leiomyosarcoma?
Recommendations:
-
1.
Complete extraction including total hysterectomy with bilateral salpingo-oophorectomy is recommended (Grade B).
-
2.
Chemotherapy is considered as postoperative adjuvant therapy (Grade C1).
-
3.
Postoperative radiation is less efficacious and is therefore not recommended in routine practice (Grade C2).
[See Fig. 8].
CQ41 What surgical techniques and postoperative adjuvant therapy are recommended for endometrial stromal sarcoma (ESS)?
Recommendations:
-
1.
Total hysterectomy with bilateral salpingo-oophorectomy is recommended as a standard surgical procedure (Grade B).
-
2.
Pelvic and para-aortic lymphadenectomy (biopsy) or cytoreductive surgery is also considered (Grade C1).
-
3.
For stage I or II low-grade ESS, follow-up without postoperative adjuvant therapy is recommended (Grade B).
-
4.
When adjuvant therapy is necessary for high-grade ESS, chemotherapy is recommended (Grade C1).
[See Fig. 8].
CQ42 What treatments are recommended for unresectable or recurrent ESS/leiomyosarcoma?
Recommendations:
-
1.
Surgery is considered for recurrence if the tumor is resectable (Grade C1).
-
2.
Chemotherapy is also considered (Grade C1).
-
3.
Hormonal therapy is also considered for low-grade ESS (Grade C1).
-
4.
Radiation therapy for the purpose of palliative care is considered (Grade C1).
[See Fig. 8].
Chapter 8: Treatment of trophoblastic disease
CQ43 What chemotherapy is recommended for an invasive mole, clinical invasive mole, or post-molar persistent human chorionic gonadotropin (hCG)?
Recommendations:
Monotherapy with methotrexate or actinomycin D is recommended (Grade B).
CQ44 What chemotherapy is recommended for choriocarcinoma?
Recommendations:
A multidrug regimen including methotrexate, actinomycin D, and etoposide is recommended (Grade C1).
[See Fig. 9].
CQ45 What are the indications for surgery for choriocarcinoma?
Recommendations:
-
1.
Surgical resection is considered for patients with a uterine lesion or metastatic lesion associated with chemoresistance (Grade C1).
-
2.
Surgical resection is also considered for patients with a uterine lesion in which hemorrhage is difficult to control or those who have brain metastasis with symptoms of intracranial hypertension (Grade C1).
[See Fig. 9].
CQ46 What are the indications for radiation therapy for choriocarcinoma?
Recommendations:
Whole-brain irradiation and/or stereotactic radiosurgery are considered to treat brain metastasis (Grade C1).
[See Fig. 9].
CQ47 What treatments are recommended for cases with placental site trophoblastic disease or epithelioid trophoblastic tumor?
Recommendations:
-
1.
Total hysterectomy is recommended for patients with disease limited to the uterus (Grade B).
-
2.
Combination therapy with surgical treatment including total hysterectomy and chemotherapy are desirable for patients with metastasis (Grade C1).
CQ48 How should patients with persistent low-positive hCG be treated?
Recommendations:
After every gestation including hydatidiform mole or after treatment of trophoblastic disease, strict follow-up is recommended when ‘real’ low-unit hCG persists long term without an obvious lesion (Grade C1).
References
Matsuda A, Matsuda T, Shibata A et al (2014) Cancer incidence and incidence rates in Japan in 2008: a study of 25 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol 44(4):388–396
For act on anti-cancer measures based on the data of statistics white paper 2012 (Shinoharashinsha Publishers Inc.) Cancer Information Service, National Cancer Center, Japan
Nagase S, Katabuchi H, Hiura M et al (2010) Evidence-based guidelines for treatment of uterine body neoplasmin Japan: Japan Society of Gynecologic Oncology (JSGO) 2009 edition. Int J Clin Oncol 15:531–542
Ariyoshi H (2002) Guideline for correct use of antineoplastic agents (draft). General theory. Gan To Kagaku Ryoho 29(6):970–977 (in Japanese)
Ochiai K, Okamoto A, Katsumata N (2002) Guidelines for proper use of antineoplastic agents. Gynecologic cancer. Gan To Kagaku Ryoho 29(6):1047–1054 (in Japanese)
Fukui T, Yoshida M, Yamaguchi N (2007) Minds clinical practice guideline. Igaku-Shoin, Tokyo, p 40 (in Japanese)
Dowdy SC, Mariani A, Lurain JR (2012) Uterine cancer. In: Berek JS (ed) Berek and Novak’s gynecology, 15th edn. Lippincot Williams & Wilkins, Philadelphia, PA, pp 1250−1303
Miller DS, Creasman WT (2012) Adenocarcinoma of the uterine corpus. In: DiSaia PJ, Creasman WT (eds) Clinical gynecologic oncology, 8th edn. Elsevier Saunders, Philadelphia, pp 141–174
Acknowledgments
We thank the Japan Society of Obstetrics and Gynecology, the Japan Association of Obstetricians and Gynecologists, the Japanese Gynecologic Oncology Group, the Japan Society of Clinical Oncology, and the Japanese Society for Therapeutic Radiology and Oncology for their comments and contributions throughout the project. We also acknowledge the support by grants from the Ministry of Health, Labour and Welfare and H24-Clinical Cancer Research-001 (chief researcher, Koichi Hirata).
Members of guidelines formulation committee Yasuhiko Ebina, Hisaya Fujiwara, Shinji Fukunaga, Yasuyuki Hasuo, Atsushi Hongo, Kazuhiko Ino, Yuko Kaneyasu, Hidenori Kato, Naoki Kawamura, Yoichi Kobayashi, Kaneyuki Kubushiro, Masataka Kudo, Hideo Matsui, Koji Matsumoto, Yoshiki Mikami, Toshinari Muramatsu, Shoji Nagao, Satoru Nagase, Takafumi Nakamura, Toru Nakanishi, Satoru Nakayama, Hideyuki Ohtake, Yoshikazu Ozaki, Nobuyuki Susumu, Tsutomu Tabata, Kiyoshi Takamatsu, Masashi Takano, Satoshi Takeuchi, Yoshito Terai, Takafumi Toita, Akiko Tozawa, Takashi Uno, Hidemichi Watari, Tetsuro Yahata, Hideko Yamamoto, Koji Yamazawa, Nozomu Yanaihara, Masami Yasuda, Yoshihito Yokoyama.
Members of guidelines evaluation committee Daisuke Aoki, Yoichi Aoki, Makoto Emoto, Takayuki Enomoto, Toru Hachisuga, Seiryu Kamoi, Takahiro Kasamatsu, Noriyuki Katsumata, Junzo Kigawa, Hiroaki Kobayashi, Takeshi Kodaira, Junichi Kodama, Shinichi Komiyama, Hiroyuki Kuramoto, Makoto Kuroda, Masaki Mandai, Etsuko Miyagi, Takashi Nakano, Kaei Nasu, Fumitaka Numa, Kazunori Ochiai, Tsuyoshi Saito, Toshiaki Saito, Masaru Sakamoto, Noriaki Sakuragi, Nobuhiro Takeshima, Toshimitsu Toya, Satoshi Umezawa, Yoh Watanabe, Hiroyuki Yanai.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Kiyoshi Takamatsu received lecture fees from Bayer Yakuhin, Ldt, and Pfizer Japan Inc.
Additional information
This article originally appeared in Japanese as Shikyu taigan chiryo gaidorain 2013 nen ban, published by Kanehara, Tokyo, 2013.
About this article

Cite this article
Ebina, Y., Katabuchi, H., Mikami, M. et al. Japan Society of Gynecologic Oncology guidelines 2013 for the treatment of uterine body neoplasms. Int J Clin Oncol 21, 419–434 (2016). https://doi.org/10.1007/s10147-016-0981-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-016-0981-1