
Abstract
We report our experience about somatotrophinomas without clinical manifestation of acromegaly having radiological- and surgical-verified invasion of the cavernous sinus. We present the clinical, radiological and hormonal status of three patients affected by invasive GH-secreting pituitary adenomas without clinical signs and symptoms of acromegaly with elevation of serum IGF-1 from a series of 142 pituitary adenomas operated in our institute with the aid of intraoperative magnetic resonance imaging (MRI). Total tumor removal was possible in two of the three cases; the patients show normal hormonal status and no recurrence at long-term follow-up. In the third case, due to the different features of the tumor, complete resection was not possible and a multimodal treatment was performed that allowed regularization of the hormonal status and control of the residual tumor. GH-secreting adenomas without clinical manifestation of acromegaly are uncommon lesions. Total microsurgical excision can be curative. However, in case of partial removal, a tailored adjuvant treatment should be considered to preserve the quality of life of the patient and avoid regrowth of the lesion. In not resectable tumors, preoperative medical treatment with somatostatin analogues is always an option.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
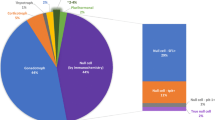
The classification of pituitary adenomas into functional and non-functional is widely accepted and currently used all over the world. In the 1970s, a subtype of functional lesions called “silent adenomas” was introduced [1]. Between 43 and 64% of silent adenomas are gonadotropinomas; the rest are somatotroph (9%), corticotroph (2.9–5.7%) and lactotroph adenomas (1–2%) [2].
Silent adenomas are defined as adenomas showing hormone positivity at the histopatological examination without clinical signs and the early reports regarded silent corticotroph adenomas [3, 4].
Another category of adenomas are pituitary adenomas, which are not clinically symptomatic but causing measurable hormone overproduction in serum [5]. Such cases of GH-producing adenomas, were described by Tourniaire [6] and Klibanski [7]. Since then, few studies have been published [8,9,10,11,12,13,14,15] illustrating morphological and biochemical features of these lesions not focusing on neurosurgical treatment options. In contrast to this clinically quiet disease, silent adenomas can develop aggressively and invasively.
The literature finds the invasion of cavernous sinus by pituitary adenomas in between 6 to more than 10% of patients [16] and reports an increasing resistance to the treatment [17]. In this study, we report three explicative cases of somatotrophinomas without clinical manifestation of acromegaly having radiological and surgical verified invasion of the cavernous sinus. We describe the hormonal pattern of the patients, as well as our neurosurgical treatment strategy and follow-up.
Material and methods
We present the clinical, radiological and hormonal status of three patients affected by invasive somatotrophinomas without clinical signs and symptoms of acromegaly with elevation of serum IGF-1 from a series of 142 pituitary adenomas operated in our institute with the aid of intraoperative magnetic resonance imaging (MRI) (Table 1). The surgical and adjuvant treatment adopted in every case is described together with their follow-up. All the patients were seen by an endocrinologist and the adenomas are categorized using the WHO 2004 classification and its variants successively proposed by Trouillas et al. [18] and Saeger et al. [19] (Table 2). The cut-off values for the determination of proliferation rate were MIB-1 > 3% [19] and p53 > 2% [20] (Table 3).
Case 1
A 44-year-old woman came to our institute with a 10-month history of headache and amenorrhea. She was referred 3 months before the admission to a local endocrinologist who recommended an MRI of the brain and serum pituitary hormones control. The MRI revealed an intra- and suprasellar mass with initial compression of the optic chiasm and invasion of the cavernous sinus on the left side. Initial serum laboratory investigations (Table 1) documented elevated insulin-like growth factor 1 (IGF-1), normal basal GH value and no suppression under 1 ng/ml in oral glucose tolerance test (OGTT) (75 g of glucose). Clinically, there were neither specific nor associated signs of acromegaly (Table 4). We performed a selective removal of the tumor via a transsphenoidal endoscopic-assisted approach using intraoperative MRI control. On histopatological examination, the lesions proved to be a pituitary adenoma and the immunohistochemical study showed GH expression and PRL (Table 3). Soon after the operation and in the following 4 years, the patient showed no signs of acromegaly, the IGF-1 and GH values were in the normal range and the MRI control displayed no tumor recurrence (Table 1).
Case 2
A 26-year-old woman was referred to our institute for a sellar tumor. She had a history of oligo-amenorrhea with galactorrhea and visual field deficit of the right eye but no signs of acromegaly (Table 1). The MRI of her brain revealed an intra- and suprasellar space-occupying mass invading the medial wall of the right cavernous sinus and developing subcavernously (Fig. 1). Serum values of IGF-1 and GH were elevated (Table 1). The tumor was totally removed via a transsphenoidal endoscopic-assisted approach using intraoperative MRI control including the portion invading the cavernous sinus with displacement of carotid artery. Accordingly, the first intraoperative MRI control documented a small tumor remnant in the superior middle cavernous sinus. The surgery was continued and the residual lesion was removed, as confirmed by the second intraoperative MRI control (Fig. 2). The histology result was pituitary adenoma with GH-expressing cells. (Table 3). In this case, the tumor can be classified as atypical (invasive, p53 > 2). After the surgery, the patient’s menstrual cycle was regular; 10 months after the surgery, the patient delivered a healthy baby. The early and 3-years postoperative hormonal study are reported in Table 1. At the 3-month follow-up, the MRI of the brain confirmed the total removal of the lesion without sign of recurrence (Fig. 3a, b).

Case 2: preoperative sagittal and coronal T2-weighted images showing the intra- and suprasellar pituitary adenoma invading the right cavernous sinus

Case 2: intraoperative sagittal and coronal T2-weighted images showing the total removal of the lesion via transsphenoidal endoscopic-assisted approach

Case 2: sagittal and coronal T2-weighted images performed 3-months after surgery. The MRI of the brain confirmed the total removal of the lesion without sign of recurrence
Case 3
A man, aged 35, working as general surgeon was examined at our institute with a 4-months history of decreased libido and progressive visual field deficit on the right eye during previous days, without specific or associated signs of acromegaly. The MRI of his brain showed an intrasellar mass of 30 mm in maximal diameter with asymmetric suprasellar extension on the right side and invasion of the right cavernous sinus (Fig. 4). The basal serum hormonal concentration revealed elevated PRL, IGF-1 and GH (Table 1). These values were only available 2 days after the surgery. Because of the partial and retrospectively incomplete hormonal tests, performed in another hospital, the patient was first diagnosed as an inactive adenoma Surgery was performed shortly after admission because of the progressive visual deficit; if the GH and IGF-1 hormonal values had been available at the admission, another option could have been a preoperative medical treatment with potential shrinking of the lesion. The surgical strategy consisted of a two-step approach. First, the patient was surgically treated with a transsphenoidal endoscopic-assisted approach. On histopatological examination, the lesions proved to be an atypical pituitary adenoma with expression of GH and PRL (Table 3). The intraoperative MRI control revealed a partial tumor removal with residual lesion in the right cavernous sinus and suprasellar between the carotid artery and the right optic nerve (Fig. 5). The patient received further treatment with cabergoline 0.5 mg twice/week without tumor shrinkage and a second transcranial surgery was performed to remove the tumor, which was partially compressing the optic nerve, via a right frontolateral approach. The postoperative course was regular with improvement of visual function and the patient received medical treatment with somatostatin analogue. Eight weeks after the second surgery a new hormonal dosage showed nearly normal values (Table 1). In light of such an obviously rapid growth, invasion of cavernous sinus and already mildly elevated values of p53 and MIB-1, a gamma-knife treatment was planned for the intracavernous tumor rest (volume 4.2 cm3). Four months after this therapy, an MRI control revealed a decreasing volume of the residual tumor (volume 3.5 cm3) (Fig. 6). At 3-year follow-up, the IGF-1 value was in the normal range and there was no growth of the residual lesion (Table 1).

Case 3: preoperative sagittal and coronal T2-weighted images showing the pituitary adenoma with extension suprasellar on the right side and invasion of the right cavernous sinus

Case 3: intraoperative sagittal and coronal T2-weighted images showing partial tumor removal with residual lesion in the right cavernous sinus and right suprasellar space between carotid artery and the right optic nerve

Case 3: sagittal and coronal T2-weighted images 4 months after second surgery and gamma-knife treatment showing decreased volume of the residual tumor
Discussion
Acromegaly is a complex disease characterized by an excessive production of GH mostly due to a secreting pituitary adenoma. Characteristics of this pathology are somatic changes such as growth of the extremities, frontal bossing and prognatism together with cardiovascular, respiratory and endocrine dysfunctions. These factors negatively influence both the quality and duration of patient’s life with a mortality rate significantly higher than the normal population [21].
Past studies reported a particular type of tumor, silent GH adenomas, expressing GH immunohistochemically but not causing elevation of IGF-1 and GH serum level clinical manifestations of acromegaly has been reported [1]. Another category of adenomas is made of by somatotrophinomas with a serum elevation of IGF-1 but not manifested signs of acromegaly [5, 22].
The pathogenetical mechanism leading to the lack of clinical signs despite presence of a GH-secreting adenoma and elevated GH/ IGF-1 values is still matter of debate. The hypothesis of secretion of an “inactive” form of GH seems not to be valid in somatrotopinomas due to the high values of IGF-1 stimulated by the action of GH [22]. Some studies postulate a relation with duration of secretion [22, 23], even if it has been observed that some of the patients with silent somatotrophinomas had been exposed to surplus of GH secretion for many years [11]. Another theory supports the concept of continuum of hormonal expression with a completely silent adenoma on the lower part of the scale and a fully active adenoma with biochemical and clinical sign of the pathology on the other end [23]. This notion relates to the concept of a diminished efficacy of secretion in silent GHomas. Finally, other authors find a greater resistance of young women to GH due to the observation that GH-producing adenomas without clinical signs are more frequent in this population.
There are few previous studies on GH-producing tumor without acromegaly give data about proliferation parameters (MIB-1, p53) and invasion of adjacent structures [9, 13, 24, 25].
In the population studied by Naritaka et al. [9], three of the seven patients with silent GHomas presented invasion of the cavernous sinus. However, none of the cases had an overexpression of MIB-1 and/or p53. Other cases presented in the literature showed aggressive behavior due to their invasiveness [13] that could have been associated with high proliferation rate [24, 25]. In our cases, we find (Table 3) that all three patients presented an invasion of the cavernous sinus and increased proliferation parameters in two of them. Thus, Case 2 and 3 can be classified as atypical (invasive and p53 > 2%) confirming the tendency of corticotrophinomas without acromegaly to be more aggressive than the classic counterpart. We also classified our lesion following the variants proposed by Trouillas et al. [18] and Saeger et al. [19]. These classifications can better highlight some differences between these tumors that can affect their subsequent treatment, such as the different invasion pattern between case 2 and 3.
Due to the low frequency of these lesions, there are not sufficient data available in the literature to choose the optimal treatment. Our population includes three clinically silent lesions with different morphological and histopathological features. Thus, a different management strategy was applied for every case.
Both cases 1 and 2 were treated only surgically with the aid of intraoperative MRI. An approach that can be useful especially in presence of invasive lesions where residual tumor can be overlooked. This occurred in case 2, where the first intraoperative imaging revealed a rest in the superior part of the cavernous sinus that was definitively removed during the same surgical session. In both patients, the surgical goal was reached. After the documented complete removal of their adenoma, the patients did not need further treatment and/or hormonal substitution during the postoperative period. At the 3-months follow-up, we found normal serum values of GH and IGF-1 in both patients with a better suppression in OGTT for case 1(0.72 ng/ml) than case 2 (1.3 ng/ml). Both patients showed no recurrence at long-term follow-up. The difference in OGTT results could be due to the different quantity of GH-producing cell in the two lesions. Nevertheless, this factor and the higher values of proliferative parameters (MIB-1, p53) did not influence the clinical course of the patients after the microsurgical complete removal, as proved by the regular hormonal values and absence of recurrence after 3 years.
Case 3 has different features, thus a tailored management strategy was applied. Its appearance in MRI showed an invasion in two points (type 2c of Saeger). After the first transsphenoidal approach, we achieved the removal of the sellar mass with residual at cavernous sinus and in suprasellar area demonstrated with intraoperative MRI. The histology revealed an expression of GH and PRL in diffuse cell groups and elevated proliferation parameters. The treatment with cabergoline during the 4 weeks interval before the second operation did not show volume reduction of the residual lesion. The second surgery was performed, as initially planned, to remove the suprasellar part compressing the optic nerve. Thus, as a complete removal of the lesion was unfeasible, we chose to combine an adjuvant medical and radiotherapy treatment obtaining control of the residual lesion at 1 year. This patient could have been a candidate for medical treatment at first step if the hormonal status had been available preoperatively; but due to the local incarceration of tumor between optic nerve and carotid observed intraoperatively, we doubt that surgery could have been avoided in order to improve the visual deficit.
Conclusions
Somatothropinomas without clinical manifestation of acromegaly are uncommon lesions. Every case should be evaluated initially, taking into consideration patient’s clinical condition, MRI appearance and immunohistochemical features of the tumor. Total microsurgical excision can be curative; however, in case of partial removal, a tailored adjuvant treatment should be considered to preserve the patient’s quality of life and avoid regrowth of the lesion. In not resectable tumors, preoperative medical treatment with somatostatin analogues remains always an option.
References
Kovacs K, Horvath E, Bayley TA, Hassaram ST, Ezrin C (1978) Silent corticotroph cell adenoma with lysosomal accumulation and crinophagy. A distinct clinicopathologic entity Am J Med 64(3):492–499
Mayson SE, Snyder PJ (2015) Silent pituitary adenomas. Endocrinol Metab Clin N Am 44(1):79–87. https://doi.org/10.1016/j.ecl.2014.11.001
Horvath E, Kovacs K, Killinger DW, Smyth HS, Platts ME, Singer W (1980) Silent corticotropic adenomas of the human pituitary gland: a histologic, immunocytologic, and ultrastructural study. Am J Pathol 98(3):617–638
Hassoun J, Charpin C, Jaquet P, Lissitzky JC, Grisoli F, Toga M (1982) Corticolipotropin immunoreactivity in silent chromophobe adenomas: a light and electron microscopic study. Arch Pathol Lab Med 106(1):25–30
Cooper O, Melmed S (2012) Subclinical hyperfunctioning pituitary adenomas: the silent tumors. Best Pract Res Clin Endocrinol Metab 26(4):447–460. https://doi.org/10.1016/j.beem.2012.01.002
Tourniaire J, Trouillas J, Chalendar D, Bonneton-Emptoz A, Goutelle A, Girod C (1985) Somatotropic adenoma manifested by galactorrhea without acromegaly. J Clin Endocrinol Metab 61(3):451–453. https://doi.org/10.1210/jcem-61-3-451
Klibanski A, Zervas NT, Kovacs K, Ridgway EC (1987) Clinically silent hypersecretion of growth hormone in patients with pituitary tumors. J Neurosurg 66(6):806–811. https://doi.org/10.3171/jns.1987.66.6.0806
Kalavalapalli S, Reid H, Kane J, Buckler H, Trainer P, Heald AH (2007) Silent growth hormone secreting pituitary adenomas: IGF-1 is not sufficient to exclude growth hormone excess. Ann Clin Biochem 44(Pt 1):89–93. https://doi.org/10.1258/000456307779596075
Naritaka H, Kameya T, Sato Y, Furuhata S, Otani M, Kawase T (1999) Morphological characterization and subtyping of silent somatotroph adenomas. Pituitary 1(3–4):233–241. https://doi.org/10.1023/A:1009942122673
Matsuno A, Ogino Y, Katayama H, Osamura RY, Nagashima T (2001) Identification of a silent pituitary somatotropic adenoma based on a paradoxic response of growth hormone on a thyrotropin-releasing hormone or gonadotropin-releasing hormone provocation test. Am J Obstet Gynecol 184(3):286–288. https://doi.org/10.1067/mob.2001.109396
Pestell R, Herington A, Best J, Boolell M, McKelvie P, Arnott R, Alford F (1991) Growth hormone excess and galactorrhoea without acromegalic features. Case reports. Br J Obstet Gynaecol 98(1):92–97. https://doi.org/10.1111/j.1471-0528.1991.tb10317.x
Sakharova AA, Dimaraki EV, Chandler WF, Barkan AL (2005) Clinically silent somatotropinomas may be biochemically active. J Clin Endocrinol Metab 90(4):2117–2121. https://doi.org/10.1210/jc.2004-0875
Sidhaye A, Burger P, Rigamonti D, Salvatori R (2005) Giant somatotrophinoma without acromegalic features: more “quiet” than “silent”: case report. Neurosurgery 56(5):E1154; discussion E1154
Syro LV, Rotondo F, Serna CA, Ortiz LD, Kovacs K (2017) Pathology of GH-producing pituitary adenomas and GH cell hyperplasia of the pituitary. Pituitary 20(1):84–92. https://doi.org/10.1007/s11102-016-0748-8
Chinezu L, Vasiljevic A, Trouillas J, Lapoirie M, Jouanneau E, Raverot G (2017) Silent somatotroph tumour revisited from a study of 80 patients with and without acromegaly and a review of the literature. Eur J Endocrinol 176(2):195–201. https://doi.org/10.1530/EJE-16-0738
Ceylan S, Koc K, Anik I (2010) Endoscopic endonasal transsphenoidal approach for pituitary adenomas invading the cavernous sinus. J Neurosurg 112(1):99–107. https://doi.org/10.3171/2009.4.JNS09182
Rieger A, Rainov NG, Ebel H, Sanchin L, Shibib K, Helfrich C, Hoffmann O, Burkert W (1997) Factors predicting pituitary adenoma invasiveness in acromegalic patients. Neurosurg Rev 20(3):182–187. https://doi.org/10.1007/BF01105562
Trouillas J, Roy P, Sturm N, Dantony E, Cortet-Rudelli C, Viennet G, Bonneville JF, Assaker R, Auger C, Brue T, Cornelius A, Dufour H, Jouanneau E, Francois P, Galland F, Mougel F, Chapuis F, Villeneuve L, Maurage CA, Figarella-Branger D, Raverot G, Barlier A, Bernier M, Bonnet F, Borson-Chazot F, Brassier G, Caulet-Maugendre S, Chabre O, Chanson P, Cottier JF, Delemer B, Delgrange E, Di Tommaso L, Eimer S, Gaillard S, Jan M, Girard JJ, Lapras V, Loiseau H, Passagia JG, Patey M, Penfornis A, Poirier JY, Perrin G, Tabarin A (2013) A new prognostic clinicopathological classification of pituitary adenomas: a multicentric case-control study of 410 patients with 8 years post-operative follow-up. Acta Neuropathol 126(1):123–135. https://doi.org/10.1007/s00401-013-1084-y
Saeger W, Honegger J, Theodoropoulou M, Knappe UJ, Schofl C, Petersenn S, Buslei R (2016) Clinical impact of the current WHO classification of pituitary adenomas. Endocr Pathol 27(2):104–114. https://doi.org/10.1007/s12022-016-9418-7
Miermeister CP, Petersenn S, Buchfelder M, Fahlbusch R, Ludecke DK, Holsken A, Bergmann M, Knappe HU, Hans VH, Flitsch J, Saeger W, Buslei R (2015) Histological criteria for atypical pituitary adenomas—data from the German pituitary adenoma registry suggests modifications. Acta Neuropathol Commun 3(1):50. https://doi.org/10.1186/s40478-015-0229-8
Krzentowska-Korek A, Golkowski F, Baldys-Waligorska A, Hubalewska-Dydejczyk A Efficacy and complications of neurosurgical treatment of acromegaly. Pituitary 14(2):157–162. https://doi.org/10.1007/s11102-010-0273-0
Wade AN, Baccon J, Grady MS, Judy KD, O'Rourke DM, Snyder PJ (2011) Clinically silent somatotroph adenomas are common. Eur J Endocrinol 165(1):39–44. https://doi.org/10.1530/eje-11-0216
Daems T, Verhelst J, Michotte A, Abrams P, De Ridder D, Abs R (2009) Modification of hormonal secretion in clinically silent pituitary adenomas. Pituitary 12(1):80–86. https://doi.org/10.1007/s11102-008-0085-7
Batisse M, Raverot G, Maqdasy S, Durando X, Sturm N, Montoriol PF, Kemeny JL, Chazal J, Trouillas J, Tauveron I (2013) Aggressive silent GH pituitary tumor resistant to multiple treatments, including temozolomide. Cancer Investig 31(3):190–196. https://doi.org/10.3109/07357907.2013.775293
Chinezu L, Jouanneau E, Vasiljevic A, Trouillas J, Raverot G (2013) Silent GH pituitary tumor: diagnostic and therapeutic challenges. Ann Endocrinol 74(5–6):491–495. https://doi.org/10.1016/j.ando.2013.09.003
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Not needed
Informed consent
Yes
Rights and permissions
About this article

Cite this article
Giordano, M., Samii, A. & Fahlbusch, R. Aggressive somatotrophinomas lacking clinical symptoms: neurosurgical management. Neurosurg Rev 41, 999–1005 (2018). https://doi.org/10.1007/s10143-017-0940-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-017-0940-y