
Abstract
Emergency department (ED) computed tomography (CT) use has increased substantially in recent years, resulting in increased radiation exposure for patients. Few studies have assessed which parties contribute to CT ordering in the ED. The objective of this study was to determine the proportion of CT scans ordered due to explicit requests by various stakeholders in ED patient care. This is a prospective, observational study performed at three university hospital EDs. CT scans ordered during research assistant hours were eligible for inclusion. Attending emergency physicians (EPs) completed standardized data forms to indicate all parties who had explicitly requested that a specific CT be performed. Forms were completed before the CT results were known in order to minimize bias. Data were obtained from 77 EPs regarding 944 CTs. The parties most frequently requesting CTs were attending EPs (82.0 %, 95 % CI 79.4–84.3), resident physicians (28.6 %, 95 % CI 25.8–31.6), consulting physicians (24.4 %, 95 % CI 21.7–27.2), and admitting physicians (3.9 %, 95 % CI 2.9–5.4). In the 168 instances in which the attending EP did not explicitly request the CT, requests most commonly came from consulting physicians (51.2 %, 95 % CI 43.7–58.6), resident physicians in the ED (39.9 %, 95 % CI 32.8–47.4), and admitting physicians (8.9 %, 95 % CI 5.5–14.2). EPs were the sole party requesting CT in 46.2 % of cases while multiple parties were involved in 39.0 %. Patients, families, and radiologists were uncommon sources of such requests. Emergency physicians requested the majority of CTs, though nearly 20 % were actually not desired by them. Admitting, consulting, and resident physicians in the ED were important contributors to CT utilization.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
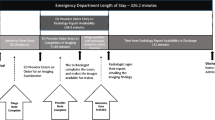
Utilization of computed tomography (CT) in the emergency department (ED) has increased substantially due to its diagnostic accuracy, accessibility, ease and speed of use, as well as physician concerns of malpractice [1–5]. A number of studies report that CT utilization in the ED has increased approximately 300–600 % in the last 15 years [1–5]. That statistic is further reflected in the National Hospital Ambulatory Medical Care database, which reported that 2.8 % of patients seen in the ED underwent CT scanning in 1995 as compared to 16.4 % of patients in 2010 and 15.8 % in 2011 [3, 6]. Though of significant diagnostic value, CT scanning results in exposure to ionizing radiation and is implicated in up to 2 % of US cancers [7, 8]. CT is also associated with increased ED length of stay [9], risk of contrast-induced nephropathy [10], incidental findings that may result in more diagnostic testing or interventions [11], and increased cost to patients and national health expenditures [12].
Emergency departments function as diagnostic arenas in which numerous stakeholders including consulting and admitting physicians, referring providers, patients, and patients’ families can exert considerable pressure on emergency physicians (EPs) to make rapid diagnoses and expedite dispositions, potentially influencing CT ordering behavior. While the lay press may be quick to point to EPs as the driving force behind the increasing number of CT scans ordered in the ED [9], few studies have actually examined the impact of other stakeholders on this behavior. For instance, patients feel greater confidence in their evaluation when it includes CT [10], leading some to hypothesize that patients and their families may be a significant factor in this imaging trend. This is likely compounded by the increased interest in shared decision-making in healthcare [11].
Moreover, other factors beyond patient requests could potentially play a role in the CT ordering behaviors of EPs. For example, one study found that 89 % of EPs sometimes order CT scans only because of a consultant request while 92 % sometimes ordered CT scans simply to appease patients or their family [5]. Another report specifically evaluating CT decision-making in trauma found that 7 % of CTs ordered on trauma patients in the ED were not desired by either the EP or the trauma surgeon [12, 13]. Thus, though there are some preliminary data to help understand the reasons for CT ordering behavior in the ED, it is unclear how many parties may be explicitly requesting that CTs be performed in the ED setting. This is problematic because interventions such as education and incentives for compliance with evidence-based practice cannot be appropriately directed without this information.
Therefore, the primary objective of this study was to determine which parties explicitly request that CTs be ordered on patients seen in the ED. Based on previous work, we hypothesized that EPs would report that 28 % of CT scans were not desired by them, but rather attribute these to other parties [12]. Although previous studies have examined CT order attribution in the setting of trauma [12] or through surveys of general CT ordering behaviors [11], we sought to prospectively investigate attribution at the level of individual CTs, as reported by the attending EP.
Methods
Study design
This was a prospective, multicenter, observational study in a convenience sample of patients seen in the ED who had one or more CTs ordered during their visit. Attending EPs completed standardized data forms in which they attributed CT order requests to specific parties. Institutional review board approval was obtained at all three clinical sites, and the study was registered with ClinicalTrials.gov (NCT02040896).
Study setting
The study was conducted at three large, tertiary care university EDs located in urban centers of the South and Midwest United States with a combined annual census of greater than 200,000 patient visits. All three have level 1 trauma center designation. Due to differing timing of regulatory approvals at each site, the dates of study enrollment varied by site and are listed in Table 1.
Selection of participants
In this study, there were two participant populations: ED patients who underwent CT imaging and the attending physicians who were responsible for the CT order. Patients were eligible for enrollment during study hours if they underwent one or more CT scans during their ED visit. There was no intervention at the patient level, only gathering information regarding their CT scan and ED visit. Physician participants were eligible for enrollment if they acted as attending physicians in one of the three EDs involved in this study. Their CT ordering behavior was the topic of interest for this study.
Beyond this basic study scheme, there were a few site-specific eligibility criteria. At site 2, patients cared for by the trauma team were excluded, although patients not meeting trauma team activation criteria could be enrolled. At site 1, patient participants were required to provide written informed consent, while the other sites did not have this requirement due to using only de-identified patient data. Additionally, site 2 serves only an adult population and, therefore, did not include pediatric subjects.
Methods of measurement
Each site used a unique standardized REDCap (Research Electronic Data Capture) form for data collection [14]. These forms were initially piloted and revised based on respondent feedback regarding integrity of data acquisition, question clarity, and ease of use. The forms’ questions aimed to identify which parties explicitly requested that the scan be performed, as reported by the attending emergency physician. We defined “explicit requests” as when a party specifically asked in written or verbal form for the CT to be done. Additionally, if the attending EP reported that he/she desired the CT to be done, this was counted as an explicit request. If not communicated as described here, requests were considered to be implicit or anticipated and, therefore, were not included in this analysis. When a patient underwent CT of multiple body regions at the same ED visit, data on the explicit requests for each body region were individually obtained (e.g., “trauma pan-scans” were divided into individual body regions). As previously mentioned, there is evidence that portions of the pan-scan, which typically images the head, spine, chest, abdomen, and pelvis, would be desired by EPs, though other portions of the scan would not.
EPs were required to complete data forms prior to knowledge of CT scan results. This was because knowledge of CT results was felt to potentially influence the EPs’ attribution of the scan (e.g., EPs might be more likely to attribute a normal CT to others or to claim attribution for abnormal CTs).
Sample size calculation
As mentioned previously, roughly 25 % of CT scans ordered in one study were deemed unnecessary by EPs. In order to show that this same proportion held for our study population within a 95 % confidence interval with 3 % precision on each tail of the estimate, 801 patients were needed.
Data analysis
Descriptive statistics are used to report the proportion of CT scans explicitly requested by each party, calculated as point estimates with 95 % confidence intervals assuming a binomial distribution. Data were exported to Microsoft Excel Version 14 for analysis.
Results
Characteristics of study subjects
During the study period, 77 EPs completed data forms detailing the CT ordering requests for 944 CTs. Table 1 depicts study site characteristics including the enrollment periods at each site and information concerning physicians completing the data forms. The mean patient age at site 1 was 52 years (SD 21 years) with 46.8 % of enrollees being male while site 3 had a mean patient age of 52.5 years (SD 20.2 years) and 39 % males. Further patient demographics are described by site in Table 2.
Main results
CT ordering requests were most frequently attributed to attending EPs (82.0 %, 95 % CI 79.4–84.3), resident physicians in the ED (multiple specialties) (28.6 %, 95 % CI 25.8–31.6), consulting physicians (24.4 %, 95 % CI 21.7–27.2), and admitting physicians (3.9 %, 95 % CI 2.9–5.4). EPs were the only party to explicitly request CT in 46.2 % (95 % CI 43.0–49.4) of cases. Multiple parties explicitly requested 39.0 % (95 % CI 35.9–42.1) of CTs. Other parties, including patients, families, allied health professionals, and radiologists, were uncommon sources of these requests (Table 3).
In the 168 instances (17.8 %, 95 % CI 15.5–20.4) in which the EP did not report that the CT was necessary, the most common explicit requests came from consulting physicians (51.2 %, 95 % CI 43.7–58.6), resident physicians in the ED (multiple specialties) (39.9 %, 95 % CI 32.8–47.4), and admitting physicians (8.9 %, 95 % CI 5.5–14.2) (Table 4). Other health care providers, including radiologists (3 %, 95 % CI 1.3–6.8 %), primary care physicians (1.8 %, 95 % CI 0.6–5.1 %), and triage physicians (1.25 %, 95 % CI 0.3–4.2 %), infrequently requested CTs. Similarly, patients (3 %, 95 % CI 1.3–6.8 %) and patient family/friend (0.6 %, 95 % CI 0.1–3.3 %) did not frequently request CT imaging to be performed.
Discussion
The ED is a diagnostic arena where multiple parties, including EPs, residents, admitting and consulting physicians, radiologists, advanced practice providers, nurses, patients, and patients’ families and friends, may play a role in the decision to order a CT. These stakeholders can influence decisions through various means of communication, which we have dichotomized as either explicit or not for the purposes of this study. In our analysis of these prospectively gathered data, EPs were the most common source of all explicit requests, though 18 % of scans were undesired by EPs. Conversely, for 46 % of CTs, the EP was the only party who explicitly requested the scan. This is not to say that CT scans desired by EPs were indicated while those not desired were not indicated, but rather documents the proportion of scans directly attributable to key stakeholders in the care of ED patients.
Previous studies have examined the involvement of non-EPs in the decision to order a CT scan, though in more indirect ways or in more limited populations. In one survey study of CT ordering behaviors, 89 % of EPs reported that they sometimes ordered CT scans that they did not consider clinically indicated because of requests from a consulting physician [5]. Another recent survey found that 85 % of EPs felt that too many advanced diagnostic tests (CT and MRI) were being ordered in their own EDs and 97 % responded that some (mean 22 %) of the studies they personally ordered were not needed [15].
The use of trauma “pan-scans” has been debated at length. Proponents argue that comprehensive CT scanning ensures that occult injuries are not missed while opponents contend that the routine use of such scans is both costly and without significant clinical benefit when compared with selective CT scanning. One study of decision-making for “pan-scans” demonstrated that 35 % of CTs were undesired by at least one physician, 28 % were desired by the trauma surgeon but not by the EP, and 7 % were desired by neither the EP nor the trauma surgeon [12]. In our study, only one of 944 CTs (0.1 %) was specifically noted to be explicitly desired by “No One.”
The relatively high rate of ordering of CTs by resident physicians when EPs did not feel it was necessary deserves attention. Academic medical centers may be at higher risk (compared with non-teaching facilities) of CT overutilization due to the presence of trainees. In these centers, consultants and admitting physicians may also be trainees, potentially compounding this problem. This use could be tempered by closer supervision by faculty physicians. In the past, trainees were often allowed to order diagnostic tests not considered essential by faculty as part of a learning process. This may be inappropriate for tests with the expense and potential harms of CT.
In all the CTs ordered, patients and their friends/families were uncommon sources of explicit CT requests, accounting for 1.9 and 1.2 % of all requests, respectively. In the subset of CTs not desired by the EP, patients explicitly requested 3 % of CTs and families/friends 0.6 %. In a previously published survey, 92 % of EPs reported sometimes ordering CTs that they felt were not clinically indicated to satisfy the patient’s or patient’s family’s expectations [5]. Our finding does not necessarily contradict this since we report only explicit requests for CT, not anticipated or implied requests. In our study, patients may not have felt it necessary to explicitly request CT in cases in which the physician declared CT to be part of the diagnostic plan, and EPs likely did not solicit the patient’s or family’s opinion systematically. If patients and families rarely request CT, improved patient education on the advantages and disadvantages of advanced imaging modalities in the ED might not substantially affect the number of CTs ordered. On the other hand, if EPs begin to curtail their use of CT, patients and families may increasingly voice previously latent desires for CTs, requiring further patient education.
In a 2007 survey of patients undergoing outpatient CT, 44 % of patients endorsed shared decision-making for CT use with their physician, while only 6 % were aware of an increased risk of cancer associated with CT [11]. A 2009 ED-based survey found that patients are more confident with their medical assessment when it includes CT imaging compared to history and physical examination alone, but had poor understanding of cancer risks [10]. Media attention to cancer risks since that time may shift the balance, and the influence of patients on CT ordering decisions in the ED deserves continued attention.
Radiologists have been on the vanguard of recommendations to curtail unnecessary CT exams to prevent radiation exposures, particularly the Image Wisely [16] and Image Gently [17] campaigns. However, it is not uncommon to have recommendations for additional imaging after an index scan/image in the emergency department. These are often recommended for follow-up of abnormal, incidental findings on the index scan or further delineation of potentially pathologic findings. Previous studies show that radiologists recommend additional imaging following 6.5 % of plain radiography exams and 13.5 % of ultrasound exams [18, 19]. Our study found that radiologists explicitly requested only 1.5 % of all ED CTs (3 % of ED CTs not desired by EPs). However, this lower prevalence of recommended follow-up imaging may simply be due to most follow-up scans for incidental findings (nodules, lymphadenopathy, etc.) being done at a later point in time.
Our study found that multiple parties explicitly requested 39 % of all CTs. This shared input in diagnostic decisions suggests that reducing CT utilization would require educating and influencing multiple parties. Further research efforts could seek to determine if having multiple explicit requests for CT is a marker of more highly indicated CTs, though multiple requests may simply reflect that more than one party may be ignorant of the indications for CT. Moreover, parties may have influenced each other’s desires for CT, as no party was blinded to the ordering requests of others.
We identified several limitations in our study design and data collection. First, our data are from a convenience sample of patients undergoing CT during study hours, which may have introduced selection bias. For example, a physician with a biased belief about the overutilization of CT by other specialties might be more inclined to respond to the data form and to attribute CT to other parties. However, we collected data from 77 physicians, and no single physician’s responses accounted for more than 5 % of all study data. Secondly, limited study hours might have also led to selection bias since patient populations and care practices may differ depending on the time of the day. Thirdly, the study may have limited external validity due to the use of the three academic medical centers as recruitment sites representing the Midwest and Southern populations. A broader geographic distribution and inclusion of community sites would have been desirable and may be a key improvement in further research endeavors. Fourth, EPs engaged in the care of critically ill patients may have been less likely to respond to the data form as a consequence of patient care demands. Thus, critically ill patients might be under-represented in this study; however, these patients are not the target of efforts to curb CT overutilization. Fifth, there is likely information bias related to EPs not systematically or reliably ascertaining the wishes of other parties regarding a CT being ordered, likely resulting in under-reporting of explicit requests from these parties. For example, patients and their friends/families may have explicitly asked for a CT to be done had an EP not discussed a plan that already included a CT. Additionally, consultants or admitting physicians may have explicitly asked for a scan to be done had it not been done already. Directly querying each party contributing to the ordering of a CT scan would have more accurately reflected those party’s wishes. However, doing so may have led to over-reporting of explicit requests from parties who otherwise would not have verbalized such a request.
Conclusion
Multiple parties explicitly request the ordering of CT scans for emergency department patients. Though emergency physicians requested the majority of CTs, almost 20 % were not explicitly requested by them. Admitting and/or consulting physicians and resident physicians in the emergency department were important contributors to CT utilization. Efforts to optimize utilization must include all stakeholders who contribute to CT ordering, not solely emergency physicians. To further advance this field, future research should focus on non-explicit forms of communication involved in CT ordering, the indications for CT orders, and the imaging results and clinical outcomes of CTs desired and not desired by key stakeholders.
References
Broder J, Warshauer DM (2006) Increasing utilization of computed tomography in the adult emergency department, 2000–2005. Emerg Radiol 13(1):25–30
Broder J, Fordham LA, Warshauer DM (2007) Increasing utilization of computed tomography in the pediatric emergency department, 2000–2006. Emerg Radiol 14(4):227–232
Ginde AA, Foianini A, Renner DM, Valley M, Camargo CA Jr (2008) Availability and quality of computed tomography and magnetic resonance imaging equipment in U.S. emergency departments. Acad Emerg Med Off J Soc Acad Emerg Med 15(8):780–783
McBride JF, Wardrop RM, Paxton BE, Mandrekar J, Fletcher JG (2012) Effect on examination ordering by physician attitude, common knowledge, and practice behavior regarding CT radiation exposure. Clin Imaging 36(5):455–61.e1
Weigner MB, Dewar KM, Basham HF, Rupp VA, Greenberg MR (2012) Impact of education on physician attitudes toward computed tomography utilization and consent. J Emerg Med 43(5):e349–e353
National Hospital Ambulatory Medical Care Survey: 2011 emergency department summary tables—2011_ed_web_tables.pdf [Internet]. [cited 2015 Jul 17]. Available from: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2011_ed_web_tables.pdf
Smith-Bindman R, Lipson J, Marcus R, Kim K-P, Mahesh M, Gould R et al (2009) Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med 169(22):2078–2086
Berrington de González A, Mahesh M, Kim K-P, Bhargavan M, Lewis R, Mettler F et al (2009) Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med 169(22):2071–2077
Redberg RF, Smith-bindman R. We are giving ourselves cancer. The New York Times [Internet]. 2014 Jan 30 [cited 2015 Jul 17]; Available from: http://www.nytimes.com/2014/01/31/opinion/we-are-giving-ourselves-cancer.html
Baumann BM, Chen EH, Mills AM, Glaspey L, Thompson NM, Jones MK et al (2011) Patient perceptions of computed tomographic imaging and their understanding of radiation risk and exposure. Ann Emerg Med 58(1):1–7.e2
Caoili EM, Cohan RH, Ellis JH, Dillman J, Schipper MJ, Francis IR (2009) Medical decision making regarding computed tomographic radiation dose and associated risk: the patient’s perspective. Arch Intern Med 169(11):1069–1071
Gupta M, Schriger DL, Hiatt JR, Cryer HG, Tillou A, Hoffman JR et al (2011) Selective use of computed tomography compared with routine whole body imaging in patients with blunt trauma. Ann Emerg Med 58(5):407–16.e15
Moak JH, Sochor MR (2012) Mutually undesired computed tomography for patients with blunt trauma: I don’t want it. You don’t want it. Who does want it? Ann Emerg Med 60(2):244–245, author reply 245–6
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG (2009) Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 42(2):377–381
Kanzaria HK, Hoffman JR, Probst MA, Caloyeras JP, Berry SH, Brook RH (2015) Emergency physician perceptions of medically unnecessary advanced diagnostic imaging. Acad Emerg Med Off J Soc Acad Emerg Med 22(4):390–398
Radiation Safety in Adult Medical Imaging—Image Wisely [Internet]. [cited 2015 Sep 8]. Available from: http://www.imagewisely.org/
Society for Pediatric Radiology. Image Gently [Internet]. Image Gently. [cited 2015 Sep 8]. Available from: http://www.imagegently.org/
Margolis NE, Rosenkrantz AB, Babb JS, Macari M (2015) Frequency of recommendations for additional imaging in diagnostic ultrasound examinations: evaluation of radiologist, technologist, and other examination-related factors. J Clin Ultrasound JCU
Sistrom CL, Dreyer KJ, Dang PP, Weilburg JB, Boland GW, Rosenthal DI et al (2009) Recommendations for additional imaging in radiology reports: multifactorial analysis of 5.9 million examinations. Radiology 253(2):453–461
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The work presented in this manuscript received no funding from any organization or institution.
One of the authors (M.D.R.) holds a career development award from the NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR000427 and KL2TR000428. Another author (A.L.) holds a grant from the Department of Defense. Lastly, J.S.B. has a patent pending for a novel method of creating volumetric ultrasound images using orientation sensors and mechanically limited angular range of motion.
Grant support
NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR000427 and KL2TR000428.
Rights and permissions
About this article

Cite this article
Broder, J.S., Bhat, R., Boyd, J.P. et al. Who explicitly requests the ordering of computed tomography for emergency department patients? A multicenter prospective study. Emerg Radiol 23, 221–227 (2016). https://doi.org/10.1007/s10140-016-1382-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-016-1382-5