
Abstract
The objective of this study is to characterize changes in computed tomography (CT) utilization in the pediatric emergency department (ED) over a 6-year period. CT scans ordered on pediatric (ages 0 to 17 years) ED patients from July 2000 to July 2006 were analyzed in five groups: head, cervical spine, chest, abdomen, and miscellaneous. Pediatric ED patient volume and triage acuity scores were determined. There were 6,073 CT scans performed on 4,138 pediatric patients in the ED during the study period. During this same period, 78,932 pediatric patients were evaluated in the ED. From 2000 to 2006, pediatric ED patient volume increased by 2%, while triage acuity remained stable. During this same period, head CT increased by 23%, cervical spine CT by 366%, chest CT by 435%, abdominal CT by 49%, and miscellaneous CT by 96%. Increases in CT utilization were most pronounced in adolescents ages 13 to 17 years. Increases in CT utilization in this age group met or exceeded increases seen in the adult population. In children less than 13 years of age, increases were substantially smaller. Pediatric ED CT utilization particularly in the adolescent population has increased at a rate far exceeding the growth in ED patient volume, mimicking the adult trend. This increase has occurred despite considerable discussion in the medical literature about the radiation risks of CT in the pediatric population and may reflect increased availability of CT, improvements in CT diagnostic capabilities, and increased desire on the part of physicians and patients for diagnostic certainty. Whether this increased utilization results in improved patient outcomes is uncertain and deserves further study.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the adult emergency department (ED), computed tomography (CT) has become the most important diagnostic imaging modality, with substantial increases in utilization in recent years [1]. The pediatric population, however, is considerably more sensitive to the harmful effects of radiation than is the adult population, a fact which has been emphasized in the medical literature and the lay press over the past 5 years. In a seminal paper in 2001, Brenner et al. [2] estimated that, with approximately 600,000 abdominal and head CT examinations performed per year in children less than 15 years of age, 500 children would ultimately die from radiation-induced cancer. There has been considerable discussion focusing on limiting CT dose by appropriate choice of technical parameters and limiting CT utilization to an appropriate clinical question [3]. Because of this attention in the medical literature, we hypothesized that pediatric CT utilization and its rate of growth would be lower than that in the adult population. In this study, we examine that hypothesis and characterize the rate of CT utilization in the pediatric ED population over the past 6 years.
Materials and methods
We analyzed the radiology database at a tertiary care academic medical center with a children’s hospital and a level 1 trauma center. We identified CT scans performed on pediatric (age 0 to 17 years) ED patients from July 1, 2000 to June 30, 2006. CT scans were organized by body region into five groups: “head,” “cervical spine,” “chest,” “abdomen,” and “miscellaneous.” Abdominal CT included any CT of the abdomen as well as any CT of the abdomen and pelvis. Miscellaneous CT included a variety of relatively uncommon scans examining the extremities, thoracic or lumbar spine, soft tissue of the neck, sinuses, or face. CT data were stratified by age into three groups: infants (0–2 years), children (3–12 years), and adolescents (13–17 years). Only CT scans ordered from the ED and performed on patients in the ED were included.
An ED database was analyzed to determine the total number of pediatric patient encounters during the same period. We then compared the rate of growth of CT scan utilization to growth in pediatric ED patient volume. Triage acuity scores from the ED database were recorded to assess potential changes in severity of patients’ disease or injury during the study period. Triage acuity scores are standardized scores used to evaluate illness or injury severity to determine the need for immediate evaluation and treatment. The emergency severity index version 3, used in our center, is a validated scoring system with excellent inter-rater reliability and good correlation with patient outcomes including admission, level of care (e.g., telemetry, intensive care unit) and mortality [4]. We used triage acuity to assess potential changes in the ED population during the study period, which might affect CT utilization.
We also determined the number of patients who had received multiple CT scans of the chest or abdomen on different ED visits during the 6-year time period.
The university institutional review board approved this study.
Results
A total of 6,073 CT scans were ordered from and performed on 4,138 pediatric patients in the ED during the study period. During this same period, a total of 78,932 pediatric patient visits were logged in the ED. Pediatric ED patients undergoing CT had a median age of 12 and a male/female ratio of 1.3:1 (57% boys, 43% girls). During the study period, pediatric ED patient volume increased by 2%.
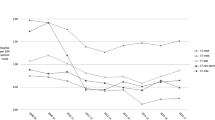
Numerical data by CT type and year is shown in Fig. 1 with percentage increase in CT group compared with pediatric ED volume shown in Fig. 2. Table 1 stratifies the increase by age group and compares it to previously published adult data that we have now extended thru June 2006. The percentage of all pediatric ED evaluations that led to patients undergoing CT is displayed by CT group in Fig. 3.

CT utilization in the pediatric ED by CT type

Increase in CT utilization by CT type, compared with ED volume

Percentage of ED evaluations involving CT
A total of 1,077 patients underwent CT of the abdomen, and 238 patients underwent CT of the chest during one or more ED visits in the study period. Thirty (3%) of these patients underwent two abdominal CTs during one or more ED visits, and four (0.4%) underwent three abdominal CTs during the study period. One percent of patients undergoing chest CT underwent a second ED chest CT during our study period. No patient underwent more than three ED abdominal CTs or more than two ED chest CTs during the study period.
The distribution of triage acuity scores remained relatively stable during the study period consistent with no major change in severity of patient illness.
Discussion
CT is the single most important contributor to radiation exposure from diagnostic imaging. In 1999, it was estimated that CT was responsible for 67% of the total collective dose from diagnostic imaging [5]. Since that time, the introduction of multidetector scanning has increased the clinical indications for CT. In the adult ED population, this had led to a dramatic rise in CT utilization [1].
The pediatric population is significantly more sensitive to radiation exposure both because of the increased number of dividing cells in growing children and because of the longer lead time children have to develop a cancer [2]. It has been estimated that, given the same dose of radiation, a 1-year old is 10–15 times more likely to develop a cancer than a 50 years old [2]. Over the last decade, much attention has been focused on decreasing radiation dose by optimizing CT settings (mAs and kVp) [6–8]. Automatic exposure control systems utilizing angular and longitudinal tube current modulation have also been introduced to further limit exposure per exam [7]. Attention has also been focused on decreasing unnecessary exams [7]. Appropriateness criteria for symptoms sets have been published by the American College of Radiology, but their impact in practice is unclear [9]. Clinical decision rules aimed at reducing unnecessary CT exams have been proposed for a variety of clinical scenarios, including head trauma, pulmonary embolism, and appendicitis [10–12].
Little work has been undertaken to evaluate the impact of the above literature and discussion in the pediatric population. In particular, to our knowledge, there have been no prior longitudinal tracking studies looking at CT utilization in children. In this paper, we undertake such a study. We looked at a discreet subset of pediatric practice, those undergoing evaluation in the ED. We chose the ED because its broad scope would encompass both traumatic and non-traumatic presentations and because the practice was relatively stable without confounding major changes in population, practitioners, or setting at our institution.
We expected CT utilization in the pediatric ED to be balanced by competing interests. In comparison with the adult ED population, concerns about radiation exposures in the pediatric population as discussed above would be expected to limit utilization, while the inherent difficulty of obtaining a reliable history and physical exam in infants and young children might be expected to favor increased use of CT, as would fear of litigation.
Our study does demonstrate that the overall rate of CT utilization in children has remained lower than that in adults. However, our findings also indicate a potentially troubling increase in CT utilization in the pediatric ED population. This increase surprisingly has occurred disproportionately in older children in whom history and physical might be expected to be useful in evaluation, limiting the need for CT. Involvement of more adolescents in vehicular blunt trauma in which CT plays an integral diagnostic role (Centers for Disease Control and Prevention data) may offer a partial explanation [13]. It may also be the case that emergency physicians believe the radiation risk from CT is restricted to the youngest children, with less concern in adolescents despite evidence suggesting that the “adult level” for cancer risk attributable to CT radiation exposures does not occur until well into the fourth decade [2]. Prior studies have shown that emergency physicians and pediatricians underestimate the radiation exposures and related cancer risks attributable to CT [14–16]. We also suspect that emergency physicians may be adopting adult evaluation strategies in their diagnostic approach to the adolescent population, as these older children physically resemble the adult patient.
Repetitive CT evaluations in children are rare and less common than in the adult population [1]. These figures for the pediatric population are somewhat reassuring but constitute only a partial picture of total CT utilization as inpatient and other outpatient settings were not included in this survey nor did we follow patients who progressed into the adult population (>17 years of age) during the time frame of the study.
Although our study data suggest that educational efforts regarding limiting CT use in the pediatric ED have only been partially successful, this conclusion must be tempered by the fact that we have only looked at data in the aggregate and have not evaluated the impact of CT on individual patient outcomes. Such a more detailed study would be a logical next step to ensure that increased CT utilization results in improved health outcomes.
Patterns of CT use in individual body regions warrant further discussion. Head CT showed a substantial increase in the adolescent group but minimal changes in younger children. This is perhaps surprising in light of the emerging pediatric literature, such as the 2001 guidelines for head CT after minor head trauma in young children, which recommended liberal use of CT in all but the lowest risk children [17]. The stability of head CT use in young children is also surprising given the difficulty in assessing the neurological exam of very young children. Increasing utilization in adolescents may reflect the high rate of blunt vehicular trauma and potential substance abuse complicating the neurological exam of adolescents [13].
Cervical spine CT showed a 435% increase from 2000 to 2006. This increase occurred predominately in adolescents, ages 13 to 17 years. We suspect that the rate of injuries detected by these additional scans was low, as the rate of pediatric cervical spine fracture is low, approximately 1% (NeXus data) [18]. Unnecessary cervical CT may be responsible for an increased risk of thyroid cancer, so the substantial increase in CT use observed in our study warrants careful monitoring [19].
Chest CT utilization increased from 0.1 to 0.7% of all pediatric ED visits. Virtually all of this increase was due to evaluation of trauma in adolescent patients between the ages of 13 and 17 years. Salim et al. [20] have recommended ubiquitous utilization of chest CT for the evaluation of adult trauma patients, although their study has been criticized for methodological flaws. Others have remarked on the low rate of clinically significant findings in chest CT of the pediatric trauma population and suggested that chest CT should not be the primary thoracic imaging modality for pediatric trauma, as nearly 200 exams would be needed to be performed to identify a single clinically significant finding [21]. The incidence of thoracic aortic trauma in the pediatric population, perhaps the single most important potential finding on chest CT for trauma, is extremely low, less than 1% [22].
Abdominal CT showed a 49% increase from 2000 to 2006. Unlike chest CT, where the predominant increase was in the adolescent trauma population, abdominal CT showed an increase with both trauma and non-trauma indications. Prior investigators have reported a high utilization of abdominal CT for blunt pediatric trauma, exceeding 50% in one series, but only 2% of those undergoing abdominal CT required surgical management [23]. Observation without CT may be a reasonable approach in the stable, low-risk young trauma patient.
Although the utilization of various forms of CT in the pediatric population appears relatively low, between 0.7 and 4.2%, this may underestimate the actual intensity of utilization, which should be considered in the context of the maximum theoretical utilization given the percentage of patients actually presenting with a “CTable” complaint. For example, if only 10% of pediatric patients present with a complaint possibly indicating a head CT (e.g., head trauma, headache, fever, seizure, altered mental status) and approximately 4% of all pediatric ED patients undergo head CT, nearly 40% of the maximum possible number of head CTs are being performed. The increase in utilization toward this theoretical limit may represent an erosion of clinical assessment skills and judgment handed down from one generation of physician to the next, which may be a hard-won skill set not easily regained if lost from the medical community.
In our center, we have attempted to limit radiation exposures in children, although the measures taken may be overwhelmed by the increases in CT utilization we observed. We routinely use automatic tube current modulation (Siemans Care Dose) set at a reference mAs of 30 for children less than 12 years of age and 45 for those over 12 years. The scan parameters are recorded on a data page that is included with the study. Cases not following protocol are reviewed periodically with the chief CT technologist. Physicians are encouraged to request ultrasound studies rather than CT scans for children with nontraumatic abdominal pain.
Limitations
Several caveats should be considered when reading this paper. First, our study represents utilization trends from a single tertiary care center and may not reflect patterns of use in other geographic regions or community hospitals.
Second, we did not investigate the diagnostic yield of CTs in our population. It may be that many of the CTs were strongly clinically indicated and provided clinically meaningful diagnostic information which changed patient management.
Third, our population also represents several different groups of patients: pediatric patients evaluated by pediatricians (some with fellowships in emergency medicine) during daylight hours (approximately 10 a.m. until 11 p.m.); a mixed group of pediatric patients evaluated by emergency physicians during nighttime hours (approximately 11 p.m. until 10 a.m.); and severely injured or ill patients triaged by protocol to the adult ED regardless of time of presentation. It may be that the specialty of the physicians evaluating patients was a major determinant of CT utilization.
Fourth, percentage increases over baseline utilization may be misleading given the small starting numbers. Nonetheless, the large increases in our study deserve continued observation in the future.
Conclusions
Pediatric ED CT utilization has increased at a concerning rate, mimicking that seen in the adult population. Increases were most pronounced in the adolescent population, while remaining less substantial in patients under 13 years of age. Whether this increase with its inherent risks represents an improvement in health care is uncertain. Further investigation and close tracking of CT utilization appear warranted.
References
Broder J, Warshauer DM (2006) Increasing utilization of computed tomography in the adult emergency department, 2000–2005. Emerg Radiol 13(1):25–30
Brenner D et al (2001) Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol 176(2):289–296
Linton OW, Mettler FA Jr (2003) National conference on dose reduction in CT, with an emphasis on pediatric patients. AJR Am J Roentgenol 181(2):321–329
Tanabe P et al (2004) Reliability and validity of scores on the emergency severity index version 3. Acad Emerg Med 11(1):59–65
Mettler FA Jr et al (2000) CT scanning: patterns of use and dose. J Radiol Prot 20(4):353–359
Donnelly LF et al (2001) Minimizing radiation dose for pediatric body applications of single-detector helical CT: strategies at a large children’s hospital. AJR Am J Roentgenol 176(2):303–306
Donnelly LF (2005) Reducing radiation dose associated with pediatric CT by decreasing unnecessary examinations. AJR Am J Roentgenol 184(2):655–657
McCollough CH, Bruesewitz MR, Kofler JM Jr (2006) CT dose reduction and dose management tools: overview of available options. Radiographics 26(2):503–512
Hadley JL, Agola J, Wong P (2006) Potential impact of the American College of Radiology appropriateness criteria on CT for trauma. AJR Am J Roentgenol 186(4):937–942
Kharbanda AB et al (2005) A clinical decision rule to identify children at low risk for appendicitis. Pediatrics 116(3):709–716
Oman JA et al (2006) Performance of a decision rule to predict need for computed tomography among children with blunt head trauma. Pediatrics 117(2):e238–e246
van Belle A et al (2006) Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 295(2):172–179
Centers for Disease Control and Prevention (2007) WISQARS (Web-based Injury Statistics Query and Reporting System). Available from: http://www.cdc.gov/ncipc/wisqars/ (cited; an interactive database system that provides customized reports of injury-related data)
Thomas KE et al (2006) Assessment of radiation dose awareness among pediatricians. Pediatr Radiol 36(8):823–832
Lee CI et al (2004) Diagnostic CT scans: assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 231(2):393–398
Shiralkar S et al (2003) Doctors’ knowledge of radiation exposure: questionnaire study. BMJ 327(7411):371–372
Schutzman SA et al (2001) Evaluation and management of children younger than two years old with apparently minor head trauma: proposed guidelines. Pediatrics 107(5):983–993
Viccellio P et al (2001) A prospective multicenter study of cervical spine injury in children. Pediatrics 108(2):E20
Mazonakis M et al (2007) Thyroid dose from common head and neck CT examinations in children: is there an excess risk for thyroid cancer induction? Eur Radiol 17(5):1352–1357
Salim A et al (2006) Whole body imaging in blunt multisystem trauma patients without obvious signs of injury: results of a prospective study. Arch Surg 141(5):468–473, discussion 473–475
Renton J, Kincaid S, Ehrlich PF (2003) Should helical CT scanning of the thoracic cavity replace the conventional chest X-ray as a primary assessment tool in pediatric trauma? An efficacy and cost analysis. J Pediatr Surg 38(5):793–797
Tiao GM et al (2000) Cardiac and great vessel injuries in children after blunt trauma: an institutional review. J Pediatr Surg 35(11):1656–1660
Fenton SJ et al (2004) CT scan and the pediatric trauma patient—are we overdoing it? J Pediatr Surg 39(12):1877–1881
Acknowledgments
The authors would like to thank Sergio Rabinovich, Tech Support Analyst, Department of Emergency Medicine, University of North Carolina at Chapel Hill.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Broder, J., Fordham, L.A. & Warshauer, D.M. Increasing utilization of computed tomography in the pediatric emergency department, 2000–2006. Emerg Radiol 14, 227–232 (2007). https://doi.org/10.1007/s10140-007-0618-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-007-0618-9