
Abstract
The objective of this clinical study was to compare conventional caries detection techniques, pen-type laser fluorescence device, and near-infrared light transillumination method in approximal dentin caries lesions. The study included 157 patients, aged 12–18, without any cavity in the posterior teeth. Two calibrated examiners carried out the assessments of selected approximal caries sites independently. After the assessments, the unopened sites were excluded and a total of 161 approximal sites were included in the study. When both the examiners arrived at a consensus regarding the presence of dentin caries, the detected lesions were opened with a conical diamond burr, the cavity extent was examined and validated (gold standard). Sensitivity, specificity, negative predictive value, positive predictive value, accuracy, and area under the ROC curve (Az) values among the caries detection methods were calculated. Bitewing radiography and near-infrared (NIR) light transillumination methods showed the highest sensitivity (0.83–0.82) and accuracy (0.82–0.80) among the methods. Visual inspection showed the lowest sensitivity (0.54). Laser fluorescence device and visual inspection showed nearly equal performance. Near-infrared light transillumination can be used as an alternative method to approximal dentin caries detection. Visual inspection and laser fluorescence device alone should not be used for approximal dentin caries.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
With the advent of preventive programs, the number of caries lesions in children and adolescents has declined [1, 2]. However, caries detection is still a critical issue in carrying out appropriate preventive and treatment procedures. In particular, non-cavitated caries lesions pose major difficulties in the treatment process [2, 3]. Determining the presence of a lesion in non-cavitated approximal caries lesions is difficult. Visual examination and radiographs are the most commonly used diagnostic techniques for approximal caries detection. However, clinical examination with a probe and dental mirror may not be adequate to detect caries lesions. Radiographs may lead to superimposition of caries due to the issues in the imaging techniques in addition to the problem of X-ray exposure [4, 5]. In order to offer a proper treatment plan, new methods should be explored to avoid disadvantages of these conventional methods. The new methods should be accurate, precise, and easy to handle. For this purpose, new technologies, such as quantitative laser or light fluorescence, light emitting diode (LED)-based or transillumination-based methods, and electrical conductance measurements, have been proposed [6,7,8,9].
The first application of laser in dentistry was for oral soft tissue surgery [10]. It has subsequently been used in various applications. A few other applications of laser in dentistry are tooth surface preparation, tooth bleaching, pulpotomy, pulp coagulation, root canal preparation, testing pulp vitality, frenectomy, gingivectomy, gingivoplasty, treatment of mucosal lesions, disinfection, discontamination, anesthetization, caries removal, cavity preparation, and caries detection [11, 12].
A non-invasive and cost-effective laser-based caries detection method is fiber-optic transillumination (FOTI) which can be applied for both occlusal and approximal caries lesions. It uses narrow beam white light to transilluminate the tooth structures. The digitized version of FOTI is digital imaging fiber-optic transillumination (DIFOTI) which can be used for initial and advanced caries lesions, cracks, and secondary caries lesions. DIFOTI can capture real-time images from occlusal, buccal, and lingual surfaces via a charge-coupled device (CCD) camera. Both of the devices, using cold visible light, are not useful for the determination of caries depth [13,14,15]. Quantitative light-induced fluorescence (QLF) uses autofluorescence of dental structures which decrease with demineralization. It uses argon laser at a wavelength of 488 nm (blue-green color) which allows detection of caries in approximal and occlusal surfaces [15,16,17]. LED-based caries detection (MID; Midwest Caries I.D., Dentsply Professional, York, PA, USA) is based on the reflectance and refraction of the emitted light (from green to red) from demineralized tooth structures, which is captured by fiber optics and converted into signals for analysis. The speed of concurrent audible signal is associated with depth of the caries [17, 18]. A fluorescence camera (VistaProof Dürr Dental, Bietigheim-Bissingen, Germany) which emits light with a wavelength 400 nm was introduced to detect caries on occlusal surfaces. Healthy tissue generates green fluorescence. A specific software quantifies the fluorescence on a numerical scale 0–5 [18, 19].
Laser fluorescence (LF) of wavelength 655 nm has been reported to be a valuable device for early diagnosis of approximal and occlusal caries [8, 20]. The devices based on this mechanism include DIAGNOdent 2095 and DIAGNOdent 2190 (LF and LF Pen, KaVo, Biberach, Germany). DIAGNOdent 2190 is a pen-type laser fluorescence (LF Pen) device which uses a diode laser that emits red light. When this light reaches the demineralization, it disperses [21]. Re-emission of fluorescence from tooth tissues differs in sound and caries sites. When the waves reach the detector, the signals are modulated and strengthened. LF pen captures the back-scattered fluorescence from the tooth surface, which is translated into a numerical scale 0–99, which appears on the screen of the device. Healthy tooth structure exhibits little or no fluorescence, whereas a higher degree of demineralization implies a greater intensity of fluorescence. Hence, higher readings imply deeper caries lesions [22, 23].
The next device produced by the same manufacturer was DIAGNOcam (Kavo, Biberach, Germany), which emits invisible near-infrared light for transillumination (NILT) of a tooth suspected of having caries lesion [14]. The device, which was introduced in 2012, comprises elastic arms containing optical fibers, a USB connection to the computer, a specific software, and a camera system including a NIR light source. The near-infrared light (NIR) light wavelength is in the range 700–1500 nm (longer than visible light), which is scattered less and therefore can penetrate objects more deeply. NIR with a wavelength of 780 nm allows for better light transmission and deeper penetration through tissues [24]. Through this method, good contrast can be obtained between carious areas and surrounding caries-free hard tissues. The elastic arms of the device, which contain optical fibers, transmit NIR light through the alveolar process to the root of the tooth. The NIR light is scattered from the occlusal surface of a tooth and a CCD sensor captures the data. The final image is displayed on the computer screen through a software developed by the manufacturer. The caries lesions appear as dark spots. The generated image indicates the tooth from its occlusal surface [14, 24,25,26]. Although NILT can detect occlusal, approximal, secondary, and smooth surface caries and cracks, it cannot diagnose caries which is subgingival and under a crown or a large filling (product limitations as shared by the manufacturer). The aim of this study was to perform an in vivo comparison of the conventional methods, pen-type laser fluorescence device, and the NILT method in terms of their efficacy in detecting approximal dentin caries lesions using the opening of the caries as the gold standard.
Materials and methods
The study was approved by the ethics committee at the Medical Faculty of Adnan Menderes University, Aydın, Turkey. Before the assessments, a power calculation was carried out. With 95% confidence interval, a minimum of 145 approximal caries lesions is required to be included. A total of 157 patients, aged 12–18, who were referred to Faculty of Dentistry at Adnan Menderes University, were included. Written informed consent was obtained from each patient’s parent. Unwilling patients and those had systemic diseases were not included in the study. Furthermore, those who had teeth with visible approximal dentin cavitations, dental anomalies, restorations, and stains on their teeth were also excluded. The inclusion criterion was the presence of approximal dentin caries without any cavity in posterior teeth. The regions of interest were marked on sheets. All the teeth were cleaned with a rotating brush and pumice/water slurry. When plaque and debris were detected, professional cleaning was carried out. Two calibrated examiners carried out the assessments of selected caries sites independently. For calibration, the examiners were trained in methods on 30 extracted teeth, placed in silicone blocks in accordance with the manufacturer’s instructions before the assessments.
Macroscopically, non-cavitated approximal sites of premolars and permanent molars were examined using visual inspection with a blunt probe, dental mirror, compressed air, and light source of the dental unit. For caries scoring, ICDAS caries classification system was used [26]. The recommended criteria were 0, sound tooth; 1, first visual change in enamel; 2, distinct visual change in enamel; 3, localized enamel breakdown; 4, underlying dark shadow originating from dentin; 5, distinct cavity with visible dentin; and 6, extensive distinct cavity with visible dentin. Code 4 was the cutoff point for dentin caries.
If bitewing radiographs of the patients were available, taken less than 4 months prior to the study, they were evaluated for the presence or absence of caries. In case of the presence of individual caries risk, such as insufficient oral hygiene, non-cavitated carious lesions at smooth and/or approximal surfaces, existing caries risk in visual examination, new bitewing radiographs were obtained with a film holder using phosphor plates. The X-ray machine operating parameters (Planmeca, Helsinki, Finland) were set to 60 kV, 7 mA, and 0.08 s exposure times. The focus-to-film distance was 20 cm. The images were obtained using a phosphor plate scanner and the manufacturer’s software (Vistascan Mini Easy, Dürr Dental, Bietigheim-Bissingen, Germany). The presence or absence of approximal dentin caries was determined using the criteria recommended by Manji et al. [27], as follows: (1) lesion in outer half of enamel, (2) lesion in inner half of enamel, (3) lesion in outer third of dentin, (4) lesion in middle third of dentin, and (5) lesion in inner third of dentin. Code 3 was the cutoff point for dentin caries.
Then, selected approximal sites were assessed with LF pen using probe tip 1 (for approximal surfaces) of the device. Before evaluation, the device was calibrated with a ceramic disk. For each tooth, the device was calibrated on a sound smooth surface. Every tooth selected for the study was air-dried for 5 s. The tip of the device was placed on the selected approximal site and rotated around its vertical axis. Selected sites were evaluated twice by each examiner to avoid individual mistakes and the peak value was recorded. When a suspicious score showed up, the measurement was repeated until agreement was reached. Obtained scores were interpreted according to criteria proposed by Huth et al. [28] for approximal caries detection in vivo. The cutoff values according to this study were in the following intervals: 0–7 sound, 8–16 enamel caries, and >16 dentin caries. The median zero fluorescence value added to the cutoffs without zero value subtraction. The scores, which were higher than 16, were accepted as dentin caries.
Next, all the posterior teeth were air-dried and evaluated using NILT. The camera was focused on the associated tooth at the correct focus-object distance, and when the tip of the camera was centered parallel to the occlusal surfaces of teeth, the image was captured. The optimal image on the computer screen could be verified by re-positioning of the intraoral tip with the sensor. After each examination, the tip of the device was sterilized and other equipment was cleaned according to the manufacturer’s instructions.
After 1 week, randomly selected patients were recalled and measurements were repeated independently by the examiners on 60 approximal caries sites to ascertain interexaminer and intraexaminer reproducibility of the devices [29].
If the examiners detected enamel caries or considered only a stained area on teeth, these samples were excluded from the study and not opened. It is required to include only dentin caries for ethical reasons. This detection was carried out when both the examiners arrived at a consensus about the presence of enamel caries and sound surface. Eventually, a total of 161 approximal caries sites were included in the study for further analysis. For ethical reasons, when both the examiners arrived at a consensus regarding dentin caries presence, detected lesions were opened with a conical diamond burr and hand excavator until soft carious tissue was completely removed by assessing the hardness of the depth via a periodontal probe [29, 30]. The cavity extent was examined and validated (gold standard). Scores according to the severity of the lesion were recorded for each examined and validated tooth. The criteria [31] used in examination after caries opening were 0, no caries; 1–2, enamel caries; 3, caries up to half of dentin; and 4, caries beyond half of dentin. Code 3 was cutoff point for dentin caries.
After the evaluation, opened cavities were restored with an appropriate restorative material.
Statistics
The obtained data were evaluated using SPSS 17.0 statistical program. Accuracy, sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), and area under the ROC curve (Az) values between test methods were calculated. McNemar test was used to compare the methods for paired samples. P < 0.05 was considered statistically significant.
Reproducibility of examiners was evaluated by using Cohen’s kappa. The criteria recommended by Viera and Garrett [32] were used for the interpretation.
Results
After excluding the unopened approximal sites, a total of 161 sites were included in the study. There was no caries-free area in the samples. Five teeth had only enamel caries that had not reached the enamel-dentin junction and overscored according to investigated diagnostic methods. A large amount of the samples were restricted to enamel-dentin junction (n = 62) and dentin caries (n = 94).
Reproducibility of examiners are represented in Table 1, and sensitivity, specificity, NPV, PPV, accuracy, and Az values of methods are represented in Table 2.
Reproducibility of a test is based on the difference between how much agreement is actually present. The kappa coefficient is the most commonly used statistic for this purpose. The criteria for kappa agreement is <0, less than chance agreement; 0.01–0.20, slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–0.99, almost perfect agreement [32]. In this study, visual inspection indicated substantial agreement regarding intraexaminer reproducibility for both examiners while this method indicated moderate agreement for interexaminer reproducibility. Bitewing radiography indicated fair agreement for interexaminer reproducibility and intraexaminer reproducibility for examiner 1. LF pen for examiner 1 and NILT for both examiners indicated substantial agreement regarding intraexaminer reproducibility.
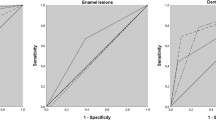
Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy address the validity of a diagnostic test. These values are associated with true-positive (TP), true-negative (TN), false-positive (FP), and false-negative (FN) rates of a diagnostic test. Sensitivity (positivity in disease) = (TP/(TP + FN)); specificity (negativity in health) = (TN/(FP + TN)); positive predictive value = (TP/(TP + FP)); negative predictive value = (TN/(FN + TN)); and accuracy = ((TP + TN)/(TP + TN + FP + FN)). Area under the ROC curve (Az) also indicates the discriminating ability of a test. ROC curves graphically display true positives versus false-positives across a range of cutoffs [33, 34]. In the present study, bitewing radiography and NILT methods showed highest sensitivity (0.83–0.82) whereas visual inspection showed lowest sensitivity (0.54). Visual inspection showed the greatest specificity (1.00) whereas LF pen and NILT methods showed lowest specificity (0.20–0.20). Bitewing radiography and NILT methods showed the highest accuracy (0.82–0.80). When McNemar test was carried out to compare the methods for paired samples, no statistically significant difference was observed between the results of radiography and NILT. Both methods showed statistically significant difference when compared to visual inspection and LF pen methods.
Discussion
Clinical indicators of caries lesions have been changing. Non-cavitated lesions are more widespread than visible cavity [35]. For this reason, it is important to detect caries in non-cavitated stages without using ionizing radiation. In these non-cavitated lesions, visual inspection is not sufficiently sensitive, particularly in approximal surfaces [36]. Sensitivities and penetration capabilities of new technologies, such as FOTI and DIFOTI or laser fluorescence methods are controversial in published data [2, 6, 8, 29, 37]. These methods use visible light, whereas NILT uses NIR light. The light intensity may decrease in hard tissues or caries lesions in these photo optical methods. Therefore, longer wavelengths which are scattered less and can penetrate more deeply are used [12, 24, 25].
In this study, which aims to compare the test methods in the detection of non-cavitated approximal caries lesions, opening of the detected caries lesions has been considered as the gold standard. If both the examiners arrived at a consensus about the presence of dentin caries, detected lesions were opened. This validation was compared with the findings of ICDAS caries scoring system, pen-type laser fluorescence device, and NIR light transillumination.
Whereas visual inspection indicated lowest sensitivity (0.54) and accuracy (0.56), specificity (1.00), Az (0.77), and PPV (1.00) were highest for this method. Visual examination showed similar performance with laser fluorescence device and lower than bitewing radiography and NILT in the study. Specificity and PPV largely depend on false-positive rates, and related results could be calculated more accurately if a larger number of enamel lesions could be included in the study. Apart from this study, a new study design should be carried out for this purpose.
The sensitivity of digital radiography was 0.83 whereas this value was 0.82 for NILT. Besides, the accuracy of digital radiography was 0.82, and it was 0.80 for NILT. Other methods showed lower performance. Low specificity (0.20) in spite of high accuracy (0.80) of NILT may be associated with the small number of false-positive cases. This study was conducted for clinical evaluation, and a large number of the samples were with dentin caries. This may lead to higher true positive rates in terms of NILT scores. In five over scores, NILT overscored 4 teeth, and radiography overscored 2 teeth. To understand these contradictions, different samples can be assessed with a study design in laboratory conditions because of ethical reasons. Intra- and interexaminer reliabilities of both methods ranged between fair and substantial agreement. The fair and moderate kappa values may result from the study design, samples selected, and different types of methods used. In recent studies, NILT and digital radiography displayed similar performance in terms of approximal dentin caries detection [14, 25]. Kühnisch et al. [25] demonstrated that the diagnostic accuracy of NILT achieved the same level as bitewings for the detection of approximal dentin caries and visual inspection displayed the worst performance. In research conducted with a different NILT source, Maia et al. [4] reported that NIR light can be useful for early approximal caries detection. Abdelaziz et al. [24] also reported that NILT is a useful diagnostic tool, mainly in approximal caries detection and suggested coupling of NILT technology with a head-mounted retinal image system to increase its efficiency.
Between NILT and LF pen, both methods indicated similar results in interexaminer and intraexaminer reproducibility. On the other hand, sensitivity, accuracy, and Az values of NILT (0.82, 0.80, and 0.51, respectively) were higher than LF pen (0.60, 0.59, and 0.40, respectively), and this difference was statistically significant. This may be attributed to different mechanisms of these methods; measuring caries from different surfaces (approximal-LF pen and occlusal-NILT) using light of different wavelengths, displaying caries on a numerical scale (LF pen) or on computer screen with a camera system (NILT). In NILT method, light is transmitted through the alveolar process (from occlusal surface to the root) that results in better image quality [14]. Furthermore, the software of NILT device visualizes the real-time image, which allows to change the viewing angle to capture and record the best image [24]. Marinova-Takorova et al. [15] have suggested usage of NILT for detection of both approximal and occlusal caries lesions instead of bitewing radiography, and recommended laser fluorescence to be used as an adjunct method. In addition, Huth et al. [28] also reported that LF pen should be used as an adjunct tool in the approximal caries detection. In an in vitro study, LF pen showed low correlation for approximal caries detection in primary teeth [5].
Enamel caries could not be validated by the selected diagnostic methods in the present study. A lesion that does not reach the enamel-dentin junction should not be opened as per preventive dentistry norms. To assess the exact performance of a caries detection method, caries-free areas, enamel, and dentin caries extents must be validated [3, 6]. On the other hand, soft tissues in oral mucosa, saliva, periodontal tissues, and other patient-related factors can influence the measurements to adopt a diagnostic task in clinical conditions. Bitewing radiographs can display caries extents associated with enamel-dentin junction and dental pulp. NILT images did not indicate the relationship between caries and dental pulp for the determination of caries extension in the present study. In addition, deep approximal caries lesions that are not in the outer part of the dentin may result in less translucent shadows in the dentin which can complicate the interpretation process by NILT.
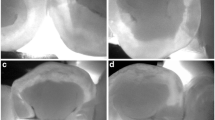
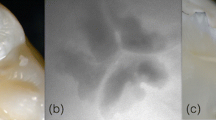
Within the limitations of the study, considering X-ray exposure by radiographs, NILT can be preferred to detect approximal dentin caries lesions instead of radiographic methods. LF pen can only be used as an adjunct diagnostic tool for approximal caries detection (Fig. 1).

Images of caries detection methods in a tooth sample with dentin caries
References
Anttonen V, Seppä L, Hausen H (2003) Clinical study of the use of the laser fluorescence device DIAGNOdent for detection of occlusal caries in children. Caries Res 37:17–23
Biesbrock A, Chesters R, Ellwood R, Smith S (2004) The challenges of validating diagnostic methods relative to a conventional two-year caries clinical trial. J Dent Res 83:C53–C55
Manton D (2013) Diagnosis of the early carious lesion. Aust Dent J 58:35–39
Maia A, Karlsson L, Margulis W, Gomes A (2014) Evaluation of two imaging techniques: near-infrared transillumination and dental radiographs for the detection of early approximal enamel caries. Dentomaxillofac Radiol 40:429–433
Celiberti P, Leamari V, Imparato J, Braga M, Mendes F (2010) In vitro ability of a laser fluorescence device in quantifying approximal caries lesions in primary molars. J Dent 38:666–670
Tassery H, Levallois B, Terrer E, Manton D, Otsuki M, Koubi S, Gugnani N, Panayotov I, Jacquot B, Cuisinier F (2013) Use of new minimum intervention dentistry technologies in caries management. Aust Dent J 58:40–59
Aktan AM, Cebe MA, Çiftçi ME, Karaarslan EŞ (2012) A novel LED-based device for occlusal caries detection. Lasers Med Sci 27:1157–1163
Pretty IA (2006) Caries detection and diagnosis: novel technologies. J Dent 34:727–739
Teo TK-Y, Ashley PF, Louca C (2014) An in vivo and in vitro investigation of the use of ICDAS, DIAGNOdent pen and CarieScan PRO for the detection and assessment of occlusal caries in primary molar teeth. Clin Oral Investig 18:737–744
Aoki A, Takasaki AA, Nagai S, Yoshida I, Zeredo JL, Mizutani K, Sasaki KM, Schwarz F, Eguro T, Izumi Y (2008) Current status of clinical laser applications in periodontal therapy. Gen Dent 56:674–687
Stabholz A, Zeltser R, Sela M, Peretz B, Moshonov J, Ziskind D (2003) The use of lasers in dentistry: principles of operation and clinical applications. Compend Contin Educ Dent 24:935–948
Nazemisalman B, Farsadeghi M, Sokhansanj M (2015) Types of lasers and their applications in pediatric dentistry. J Lasers Med Sci 6:96–101
Abogazalah N, Ando M (2017) Alternative methods to visual and radiographic examinations for approximal caries detection. J Oral Sci doi. doi:10.2334/josnusd.16-0595
Söchtig F, Hickel R, Kühnisch J (2014) Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quintessence Int 45:531–538
Marinova-Takorova M, Panov V, Anastasova R (2016) Effectiveness of near-infrared transillumination in early caries diagnosis. Biotechnol Biotechnol Equip 30:1207–1211
Ando M, van Der Veen MH, Schemehorn BR, Stookey GK (2001) Comparative study to quantify demineralized enamel in deciduous and permanent teeth using laser- and light-induced fluorescence techniques. Caries Res 35:464–470
Diniz MB, Eckert GJ, González-Cabezas C, Cordeiro Rde C, Ferreira-Zandona AG (2016) Caries detection around restorations using ICDAS and optical devices. J Esthet Restor Dent 28:110–121
Javed F, Romanos GE (2015) A comprehensive review of laser-based systems used in early detection of dental caries. Stoma Edu J 2:106–111
Achilleos EE, Rahiotis C, Kakaboura A, Vougiouklakis G (2013) Evaluation of a new fluorescence-based device in the detection of incipient occlusal caries lesions. Lasers Med Sci 28:193–201
Lussi A, Hibst R, Paulus R (2004) DIAGNOdent: an optical method for caries detection. J Dent Res 83:C80–C83
Tomczyk J, Komarnitki J, Zalewska M, Lekszycki T, Olczak-Kowalczyk D (2014) Fluorescence methods (VistaCam iX proof and DIAGNODent pen) for the detection of occlusal carious lesions in teeth recovered from archaeological context. Am J Phys Anthropol 154:525–534
Lussi A, Hack A, Hug I, Heckenberger H, Megert B, Stich H (2006) Detection of approximal caries with a new laser fluorescence device. Caries Res 40:97–103
Lussi A, Hellwig E (2006) Performance of a new laser fluorescence device for the detection of occlusal caries in vitro. J Dent 34:467–471
Abdelaziz M, Krejci I (2014) DIAGNOcam—a near infrared digital imaging transillumination (NIDIT) technology. Int J Esthet Dent 10:158–165
Kühnisch J, Söchtig F, Pitchika V, Laubender R, Neuhaus KW, Lussi A, Hickel R (2015) In vivo validation of near-infrared light transillumination for interproximal dentin caries detection. Clin Oral Investig 20:821–829
Ekstrand KR, Ricketts DN, Kidd EA (1997) Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res 31:224–231
Manji F, Fejerskov O, Baelum V (1989) Pattern of dental caries in an adult rural population. Caries Res 23:55–62
Huth K, Lussi A, Gygax M, Thum M, Crispin A, Paschos E, Hickel R, Neuhaus K (2010) In vivo performance of a laser fluorescence device for the approximal detection of caries in permanent molars. J Dent 38:1019–1026
Menem R, Barngkgei I, Beiruti N, Al Haffar I, Joury E (2017) The diagnostic accuracy of a laser fluorescence device and digital radiography in detecting approximal caries lesions in posterior permanent teeth: an in vivo study. Lasers Med Sci 32:621–628
Melo M, Pascual A, Camps I, Del Campo Á (2015) In vivo study of different methods for diagnosing pit and fissure caries. J Clin Exp Dent 7:e387–e391
Ekstrand K, Zero DT, Martignon S, Pitts NB (2009) Lesion activity assessment. Monogr Oral Sci 21:63–90
Viera AJ, Garrett JM (2005) Understanding interobserver agreement: the kappa statistic. Fam Med 37:360–363
Florkowski CM (2008) Sensitivity, specificity, receiver-operating characteristic (ROC) curves and likelihood ratios: communicating the performance of diagnostic tests. Clin Biochem Rev 29:S83–S87
Zhu W, Zeng N, Wang N (2010) Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS implementations. NESUG proceedings: health care and life sciences, Baltimore, Maryland:1–9
Ricketts D, Kidd E, Weerheijm K, Soet H (1997) Hidden caries: what is it? Does it exist? Does it matter? Int Dent J 47:259–265
Marinova-Takorova M, Anastasova R, Panov VE (2014) Comparative evaluation of the effectiveness of five methods for early diagnosis of occlusal caries lesions-in vitro study. J of IMAB 20:533–536
Young D (2001) New caries detection technologies and modern caries management: merging the strategies. Gen Dent 50:320–331
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Role of funding source
There is no source of funding.
Ethical approval
This study has been approved by the appropriate institutional and/or national research ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Ozkan, G., Guzel, K.G.U. Clinical evaluation of near-infrared light transillumination in approximal dentin caries detection. Lasers Med Sci 32, 1417–1422 (2017). https://doi.org/10.1007/s10103-017-2265-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-017-2265-z