
Abstract
We aimed to detect possible changes in Candida species distribution over time and to know the antifungal susceptibility profile of isolates obtained from patients with bloodstream infection (BSI) due to this pathogen. Risk factors associated with 30-day mortality were also assessed. We conducted a retrospective cohort study of patients diagnosed with Candida BSI at a Japanese university hospital from 2013 to 2021. The change in the distribution pattern of the Candida spp. isolated was examined by considering three successive sub-periods of 3 years each. Risk factors for 30-day mortality were determined using Cox regression analysis. In the entire study period, Candida albicans was the most frequent species (46.7%), followed by Candida glabrata (21.5%) and Candida parapsilosis (18.7%). There was no change in Candida species distribution comparing the three sub-periods analyzed. All isolates were susceptible to micafungin, and most were susceptible to fluconazole, except for C. glabrata. No isolates were resistant to amphotericin B or voriconazole. The overall 30-day mortality was 40.2%. Univariate analysis revealed an association between 30-day mortality and central venous catheter (CVC) removal at any time, high Pitt bacteremia score (PBS), and high Charlson comorbidity index (CCI). Multivariate Cox analysis found that high PBS was the only independent predictor of 30-day mortality; subsequent multivariate Cox regression demonstrated that early CVC removal significantly reduced 30-day mortality. Candida species distribution and antifungal susceptibility profile in our hospital remained similar from 2013 to 2021. Early CVC removal may improve candidemia outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Candida spp. are among the most important causative agents of bloodstream infections (BSIs) in hospitalized patients, resulting in an extremely high mortality rate [1,2,3,4]. A multicenter survey found that candidemia could reach up to 22% of healthcare-associated BSIs [5]. Despite the increased awareness of Candida spp. significance in healthcare-associated BSIs and considerable advances in treatment guidelines, which greatly rely on improved antifungal agents and more comprehensive knowledge of risk factors, the mortality rate of BSIs caused by Candida spp. remains high [6].
Early diagnosis and treatment are critical for BSIs caused by Candida spp. Although Candida spp. are common commensal organisms frequently found in the skin and gut microbiota [7, 8], eventual disruptions of the gastrointestinal barrier may result in disseminated lesions in the gastrointestinal tract. The use of central vascular catheters, recent surgical procedures (mainly abdominal surgery with anastomotic leakages), invasive procedures including mechanical ventilation, and broad-spectrum antibiotic therapy are major risk factors for invasive candidiasis. The skin may also act as an entry point for Candida spp. into circulation. Further dissemination to the lungs, kidneys, liver, spleen, and heart may occur [9]; chorioretinitis and intraocular inflammation due to Candida infection have also been documented [10].
Even when more than 15 Candida species have been identified as human pathogens, five of them—Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei—were found to be the most prevalent species [11]. Typically, C. albicans accounts for approximately 50% of candidemia cases; the remaining cases are caused by other species grouped as Candida non-albicans.
Epidemiological data, such as species distribution and drug susceptibility of local isolates, may be useful for optimizing antifungal drug therapies. Therefore, large-scale epidemiological surveys representing Japanese inpatient settings are necessary to support medical decisions based on local studies instead of overseas reports. However, it must be recognized that few hospitals in Japan are currently equipped to perform reliable mycological testing.
Recent studies carried out in different countries have documented a significant shift in the incidence of BSIs caused by Candida isolates from Candida albicans to non-albicans species [6, 11, 12]. However, regional differences have also been reported [13, 14]. Therefore, continuous epidemiological surveillance in each geographical region is needed to detect current trends and guide appropriate therapy for patients with BSIs caused by Candida.
This study aimed to characterize the clinical isolates of Candida spp. responsible for BSIs in patients admitted to a Japanese university hospital from 2013 to 2021. The change in species distribution over time, isolate susceptibility to antifungal drugs, and critical data for the rapid and appropriate management of Candida BSIs were analyzed. In addition, the clinical features of Candida BSIs and risk factors associated with 30-day mortality were assessed.
Methods
Study design and subjects
We conducted a single-center, retrospective cohort study of patients diagnosed with Candida BSI between January 2013 and December 2021 at the University of Fukui Hospital, a 600-bed university hospital that provides healthcare services to secondary and tertiary care areas.
The change in the distribution pattern of isolated Candida spp. over time was examined considering three successive sub-periods of 3 years each: 2013–2015 (sub-period I), 2016–2018 (sub-period II), and 2019–2021 (sub-period III).
This study was approved by the Institutional Review Board of the Faculty of Medical Sciences, University of Fukui.
Data collection
The following data were collected from the electronic medical records of each patient: age; sex; weight; underlying diseases; intensive care unit stay at BSI onset (yes/no); neutropenia (defined as an absolute neutrophil count < 500/mm3) at BSI onset (yes/no); presence or absence of central venous catheter (CVC); total parenteral nutrition (TPN); and peripheral parenteral nutrition (PPN) at BSI onset; surgical history (within 30 days before BSI onset); use of immunosuppressants, corticosteroids, antineoplastic chemotherapy, antibiotics, and antifungals (within 30 days before BSI onset); source of BSI; time to blood culture positivity (TTP) [15]; time to use of appropriate antifungal therapy; days to CVC removal; and 7-, 14-, and 30-day survival or mortality after BSI onset. The severity at BSI onset was evaluated by calculating the Charlson comorbidity index (CCI) and Pitt bacteremia score (PBS).
Definitions
Candida BSI was defined as the isolation of Candida species from at least one blood culture in patients with symptoms or signs of a systemic infection. The day the blood sample that yielded the first positive result was collected was considered the day of BSI onset. Only the initial episode was considered in this analysis for patients with multiple positive blood culture results.
Catheter-associated BSI was defined based on the isolation of the same species from blood and catheter tip cultures. Other secondary BSIs were defined based on clinical, imaging, and microbiological evidence using CDC criteria. Patients with an unknown source of infection were considered to have primary BSI. Antifungal drug therapy was considered appropriate if it included at least one antifungal agent with in vitro activity, dosage, and administration route that followed the published guidelines.
Microbiological procedures and Candida antifungal susceptibility testing
The microbiological procedures were performed at the clinical microbiology laboratory of our hospital. Bacterial and fungal isolates were obtained from patients’ blood cultures using BacT/Alert 3D (bioMerieux, Marcy l’Etoile, France) or BACTEC FX (BD, Franklin Lakes, NJ, USA) systems. Species were identified using the API ID 32C kit (bioMérieux, Marcy l’Etoile, France) or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS; Microflex LT, Bruker Daltonics, Bremen, Germany). Antifungal susceptibility testing was performed using the Dry Plate Eiken system (Eiken Chemical, Tokyo, Japan) according to the manufacturer’s recommendations. Susceptibility to fluconazole (FLCZ), voriconazole (VRCZ), and micafungin (MCFG) was evaluated according to the clinical breakpoints of the Clinical Laboratory Standards Institute M27-S4 [16]. The susceptibility to amphotericin B (AMPH-B) was evaluated according to the clinical breakpoint of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) Antifungal Clinical Breakpoint Table v. 9.0 [17].
Statistical analysis
Continuous variables are expressed as the median and interquartile range (IQR); categorical variables are expressed as the number (n) of subjects/isolates and percentage (%). The normal distribution of continuous variables was evaluated using the Kolmogorov–Smirnov test. Continuous variables were compared using Student’s t test or Mann–Whitney U-test, depending on the normality of the distribution. Categorical variables were analyzed using the chi-square test or two-tailed Fisher’s exact test. Comparisons of continuous variables between different Candida spp. were performed using the Kruskal–Wallis test with post hoc analysis.
The relationship between CVC indwelling time after BSI onset and the mortality rate was evaluated using the Cochran-Armitage trend test. Multivariate Cox regression analysis was performed to identify predictors of 30-day mortality. Variables with P < 0.1 after univariate analysis were included in the multivariate analysis. The hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. All P values were two-tailed, and results with P < 0.05 were considered statistically significant.
All analyses were performed using the EZR software version 1.53 (Saitama Medical Center, Jichi Medical University, Japan).
Results
Change in species distribution over time
During the entire survey period (2013 to 2021), 107 Candida isolates were obtained from 101 patients with Candida BSI. The incidence of Candida BSI calculated in terms of episodes per 1000 admissions and 1000 patient-days was 0.86 and 0.06, respectively. These incidence rates did not change across sub-periods, reaching 0.80, 0.89, and 0.84 episodes/1000 admissions for the sub-periods I (2013–2015), II (2016–1018), and III (2019–2021), respectively. The number of episodes/1000 patient-days for these sub-periods was 0.05, 0.06, and 0.06, respectively.
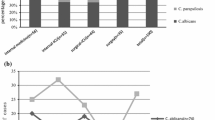
During all three sub-periods, the most commonly isolated Candida species was C. albicans, accounting for 46.7% of all isolates (Fig. 1). Comparing the three sub-periods analyzed, there was no change in the proportion of C. albicans isolates (sub-period I: 46.9%, sub-period II: 50.0%, sub-period III: 43.3%, P = 0.619). After C. albicans, the most commonly isolated species was C. glabrata (21.5%), followed by C. parapsilosis (18.7%), C. tropicalis (4.7%), Candida guilliermondii (4.7%), Candida famata (1.9%), C. krusei (0.9%), and Candida kefyr (0.9%). The proportion of C. glabrata isolates in sub-period III was 8.2% higher than that in the sub-period I and 8.6% higher than that in the sub-period II, but there was no significant change in species distribution over time (P = 0.954) (Fig. 1).

Candida spp. frequency distribution over time. A total of 107 Candida isolates were obtained from 101 patients diagnosed with bloodstream infection from January 2013 to December 2021 at the University of Fukui Hospital
Antifungal susceptibility profiles
Table 1 shows the results of the antifungal susceptibility testing performed on 104 Candida isolates obtained from 92 patients diagnosed with BSI. Isolates identified as C. famata (n = 2) and C. kefyr (n = 1) were excluded from this analysis because of the lack of specific clinical breakpoints. Susceptibility to FLCZ was good, and no C. albicans isolates were FLCZ resistant. In contrast, one C. parapsilosis isolate (5.0%) and one C. tropicalis isolate (20.0%) were susceptible to FLCZ in a dose-dependent manner (SDD/I). One C. glabrata isolate (5.3%) and one C. krusei isolate (100%) were FLCZ resistant. Susceptibility to VRCZ was also good, although one C. albicans isolate (2.0%) showed SDD/I for VRCZ. The C. parapsilosis and C. tropicalis isolates that were SDD/I for FLCZ were also SDD/I for VRCZ. Nearly all isolates were susceptible to MCFG; only one C. glabrata isolate (4.2%) showed intermediate susceptibility (4.3%), and three C. glabrata isolates (13.0%) were MCFG-resistant. No AMPH-B-resistant isolates were detected during the survey period. There was no increase in the resistance of the isolates to any antifungal drug assessed over time.
Clinical features of patients with BSI
Of the 101 patients diagnosed with BSI due to Candida spp. during the entire survey period, nine were excluded: two Candida spp. were detected in six of them, and bacteria plus Candida were detected in the other three patients. Therefore, a total of 92 patients were included in the analysis.
Among these 92 subjects, the most common Candida species was C. albicans, isolated from 42 patients (45.7%), followed by C. parapsilosis in 20 patients (21.7%), C. glabrata in 19 patients (20.7%), and other Candida spp. in 11 patients (12.0%). The median age of all patients was 74.5 years (IQR: 66–81), of whom 48 (52.2%) were male and 64 (69.6%) had malignancies (solid tumor, 55 patients; hematological malignancy, 9 patients). At the onset of BSI, 66 patients (71.7%) had indwelling CVC and 62 (67.4%) had TPN. In addition, 78 patients (84.8%) had antibiotic treatment within the previous month. The most common source of infection was primary BSI (34 patients, 37.0%), followed by catheter-associated infections (31 patients, 33.7%), and urinary tract infections (11 patients, 12.0%). Fundus examination was performed on 69 subjects (75.0%), among whom 10 (14.5%) were diagnosed with ocular candidiasis. The overall mortality rates at 7, 14, and 30 days were 14.1, 20.7, and 40.2%, respectively (Table 2).
From the clinical history analysis, it was deduced that patients with C. parapsilosis were more likely to have diabetes mellitus than those with C. albicans or C. glabrata. In addition, the TTP for C. glabrata was significantly longer than that for the other species.
Among the antifungal agents administered as initial treatment, MCFG was the most common (77%). Less than 20% of patients received FLCZ as initial therapy, and very few received liposomal-AMPH. One patient (non-survivor) did not receive any antifungal therapy. There was no significant difference in the mortality rate of individuals affected by different Candida species 7, 14, or 30 days after BSI onset.
Of the 10 patients who developed ocular candidiasis, 9 (90.0%) were infected with C. albicans and one (10.0%) with C. parapsilosis. In 34 out of 42 patients (81.0%) with BSI due to C. albicans, fundus examination was performed, and 26.5% (9/34) of them were diagnosed with ocular candidiasis (Table 2).
Analysis of 30-day mortality predictors
Overall, 37 patients (40.2%) died within 30 days after BSI onset, and several variables were compared between survivors and non-survivors (Table 3). Univariate analysis revealed an association between mortality and high PBS (P < 0.001), CCI (P = 0.009), and CVC removal (at any time) (P < 0.001). Multivariate Cox hazard regression analysis considering patient age and risk factors with P < 0.1 in the univariate analysis revealed that PBS (HR 1.32, 95% CI: 1.10–1.59, P = 0.004) was the only independent risk factor for 30-day mortality (Table 4).
Examining the relationship between 30-day mortality and CVC indwelling time after BSI onset revealed a trend toward increased mortality with longer indwelling times (P = 0.0014) (Fig. 2). The mortality rate reached 64.5% among those who maintained the CVC for 3 days or more after BSI onset and 27.9% in patients with CVC indwelling times of less than 2 days. Based on this finding, multivariate Cox regression analysis was again performed considering early CVC removal (≤ 2 days), a variable that was found to significantly reduce 30-day mortality (P = 0.036), with an HR of 0.44 and a 95% CI of 0.21–0.95 (Table 5).

Relationship between 30-day mortality and central venous catheter (CVC) indwelling time after bloodstream infection onset. Overall data for patients diagnosed with BSI from January 2013 to December 2021 at the University of Fukui Hospital
Discussion
This study surveyed the distribution of isolated Candida spp. responsible for BSIs in patients assisted at the University of Fukui Hospital from 2013 to 2021. To allow the detection of possible shifts in Candida sp. distribution along this period, three successive 3-year intervals were considered.
C. albicans accounted for 43.2% of isolated species in the sub-period III (2019–2021), with no substantial change compared to the sub-period I (2013–2015). However, an 8.2% increase in C. glabrata frequency between the sub-periods I and III was observed in this study. In a Japanese surveillance program that collected 533 Candida sp. blood isolates over a 1-year period from 2001 to 2002, C. albicans accounted for 40.7% of isolates, C. parapsilosis for 23.0%, C. glabrata for 17.9%, and C. tropicalis for 11.6% [18]. A similar trend was reported in a more extended surveillance program (2003–2014), which included data on 1921 Candida sp. blood isolates obtained at 10 Japanese university hospitals: C. albicans accounted for 39.5% of the isolates, C. parapsilosis for 23.0%, C. glabrata for 13.2%, and C. tropicalis for 7.1% [19].
Given that the present study revealed similar proportions of patients with BSI caused by C. albicans in our successive cohorts, no major shifts to non-albicans species seem to have occurred since 2001. In contrast, the proportion of patients with C. glabrata infection increased slightly, accounting for 47.6% (10/21) of all non-albicans species in the sub-period III. C. glabrata has been reported frequently in the elderly [14], and the fact that this study mainly included relatively old persons (median age: 74.5 years) may have influenced the results. Data from the SENTRY Antifungal Surveillance Program have also shown an increase in C. glabrata frequency from 2006 to 2016 [11]. C. tropicalis is considered a common isolate in the Asia–Pacific region [11, 20]; however, in our hospital, the proportion of patients with C. tropicalis was low (5.4% in the sub-period III). Data about C. guilliermondi and C. famata may not be exact given the lack of accuracy of the commercial kit used (API ID 32C) to differentiate among these rare species.
The use of the commercial Frozen Dry Plate Eiken system to evaluate the antifungal susceptibility of Candida isolates is very extended in Japan, and some previous reports [21, 22] have demonstrated that this kit provides reproducible and reliable results comparable to those obtained using the broth dilution reference method established in CLSI M27-A2; therefore, the CLSI breakpoints were considered suitable (except for amphotericin B).
Regarding the antifungal susceptibility profiles of Candida spp., the SENTRY study [11] showed regional differences. According to data from 2006 to 2016, FLCZ resistance did not increase over time, with resistance rates ranging from 0.3 to 8.1%. Interestingly, the Chinese CHIF-NET study [23] reported higher FLCZ resistance rates than those reported for the Asia–Pacific region in the SENTRY study of isolates collected from 2015 to 2017: 2.5% for C. albicans, 3.7% for C. parapsilosis, and 10.3% for C. glabrata.
We observed good susceptibility rates to FLCZ among all isolates collected, with values of 73.7% for all Candida spp. (73/99), 100% for C. albicans, and 95% for C. parapsilosis. Except for C. krusei, which is naturally FLCZ resistant, only one C. glabrata isolate was FLCZ resistant, with an overall resistance rate of 1.0% (1/98).
The VCRZ susceptibility rate was also high at 96.1% (73/76), and no VCRZ-resistant isolates were detected during the survey period. Cross-resistance between VRCZ and FLCZ has been reported [11]. In this study, one C. parapsilosis isolate and one C. tropicalis isolate were considered SDD/I for FLCZ and VRCZ, respectively. Therefore, when FLCZ resistance is observed, VRCZ is unlikely to be the optimal drug of choice.
Although Candida resistance to echinocandins is rare, the emergence of resistant strains has been reported in C. glabrata and C. tropicalis [11, 24, 25]. In this study, a high susceptibility rate to MCFG was detected (96.2%, 100/104), but one MCFG-I isolate and three MCFG-resistant isolates were found, and these four isolates corresponded to the species C. glabrata. The incidence of MCFG resistance among our C. glabrata isolates (13%) was higher than that documented in previous reports [11, 20, 23]. Nevertheless, we did not observe a tendency for higher resistance rates over time in this study, with one MCFG-resistant strain isolated in each sub-period. Given that the Infectious Diseases Society of America (IDSA) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines [26, 27] both recommend echinocandins as a first-line treatment for invasive candidiasis, trends in susceptibility profiles must be monitored continuously to avoid inappropriate treatments.
The clinical features of patients who underwent Candida BSI at our hospital were investigated to identify the risk factors and mortality predictors. Approximately 70% of the patients included in this study had a malignant neoplasm; however, very few had neutropenia (6 patients, 6.5%). Common clinical features among patients were indwelling CVC, TPN, and prior use of antibiotics (of which 76.9% [60/78] were broad-spectrum antibiotics), all of which have been identified as risk factors for Candida BSI in previous studies [26, 28].
Our analysis revealed that TTP was significantly longer in C. glabrata than in the other species. This finding agrees with the data reported by Lai et al. [15], who suggested that TTP could be used as a criterion to differentiate C. glabrata from other Candida spp.
Ocular candidiasis has been reported in around 20% of patients with Candida BSI [29, 30]. In the present study, the incidence of ocular candidiasis was slightly lower (14.5%). Given that only 75% (69/92) of the patients in this study underwent fundus examination, some cases of ocular candidiasis may have been missed. Of the patients with ocular candidiasis, 90% were infected with C. albicans. This result is consistent with previous reports and provides additional support to the IDSA treatment guidelines, which strongly recommend ophthalmic examination to detect intraocular inflammation in all patients with candidiasis [26].
Univariate analysis revealed that high PBS, high CCI, and CVC removal (at any time) were factors that affected 30-day mortality. However, multivariate analysis identified only PBS as an independent predictor of 30-day mortality and ruled out CVC removal (at any time) as an independent predictor of 30-day mortality. In addition, we found that 30-day mortality tended to increase with increasing CVC indwelling time; hence, the analysis was performed again, considering early CVC removal (within 2 days after BSI onset) as a factor impacting 30-day mortality. Multivariate analysis identified PBS and early CVC removal as independent predictors of 30-day mortality.
Current IDSA [26] and ESCMID [27] guidelines strongly recommend the removal of CVCs as early as possible. However, there is controversy regarding this recommendation and, in particular, early CVC removal as a therapeutic strategy for Candida BSI [31,32,33,34]. Lee et al. [35] noted that early CVC removal may improve the survival of patients with Candida BSI; however, this improvement was not observed in patients with CCI ≥ 4. In this study, 40 patients had CCI ≥ 4 (43.4%) (data not shown). Nucci et al. [36] investigated the impact of both CVC removal (at any time) and early CVC removal in patients with Candida BSI and found that CVC removal (at any time) had a positive effect, but early CVC removal had no impact; therefore, it was considered to have no clinical benefit. The results reported by these authors contrast with the outcome of this study, in which CVC indwelling periods ≥ 3 days after BSI onset resulted in higher 30-day mortality rates. However, a major difference in the “early CVC removal” definition exists between these two studies. In the study by Nucci et al., “early CVC removal” was defined as removal within 48 h from Candida BSI diagnosis (that is, 48 h since the day at which a blood culture was found to contain Candida sp.); in this study, “early CVC removal” was defined as removal within 48 h from BSI onset (that is, 2 days after the collection of the blood sample that gave a positive result). Thus, considering that the median TTP for Candida is 41 h, the definition of early CVC removal by Nucci et al. is equivalent to removal within 4 days according to our study. Early CVC removal has been defined by considering various starting points: when a positive blood culture sample was collected [33], when a positive blood culture was revealed (at diagnosis) [37], and at the start of treatment [32].
A systematic review of the Cochrane Database, which included studies involving CVC removal in patients with Candida BSI [38], found a lack of randomized controlled trials and highlighted that conclusions could not be drawn based on observational studies. In addition, the impact of CVC removal on 30-day mortality may be influenced by differences in analytical methods and definitions of early CVC removal, as already indicated. Given the considerable time required to detect Candida in blood cultures, postponing CVC removal until Candida is detected may be unadvisable. Therefore, alternative test methods and biomarkers should be developed to enable a faster diagnosis of Candida BSIs and appropriate antifungal therapy [39].
This study has some limitations. First, given its retrospective nature, some data could have been misinterpreted, and unknown confounders may have been omitted. Second, this was a single-center study with a small number of patients and limited information. Third, most patients were relatively old (median age: 74.5 years); thus, the data may not be generalizable to other age groups. However, our findings offer valuable information for managing patients with candidemia and improving therapeutic outcomes.
Data availability
Our institution does not mandate archiving datasets generated during retrospective analyses, but they will be available on reasonable request.
References
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB (2004) Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis 39:309–317. https://doi.org/10.1086/421946
Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA, Fridkin SK (2008) National Healthcare Safety Network Team; Participating National Healthcare Safety Network Facilities, NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect Control Hosp Epidemiol 29:996–1011. https://doi.org/10.1086/591861
Puig-Asensio M, Padilla B, Garnacho-Montero J, Zaragoza O, Aguado JM, Zaragoza R, Montejo M, Muñoz P, Ruiz-Camps I, Cuenca-Estrella M, Almirante B (2014) CANDIPOP Project; GEIH-GEMICOMED (SEIMC); REIPI, Epidemiology and predictive factors for early and late mortality in Candida bloodstream infections: a population-based surveillance in Spain. Clin Microbiol Infect 20:O245-254. https://doi.org/10.1111/1469-0691.12380
Nagao M (2013) A multicentre analysis of epidemiology of the nosocomial bloodstream infections in Japanese university hospitals. Clin Microbiol Infect 19:852–858. https://doi.org/10.1111/1469-0691.12083
Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, Lynfield R, Maloney M, McAllister-Hollod L, Nadle J, Ray SM, Thompson DL, Wilson LE, Fridkin SK (2014) Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team, Multistate point-prevalence survey of health care-associated infections. N Engl J Med 370:1198–1208. https://doi.org/10.1056/NEJMoa1306801
Koehler P, Stecher M, Cornely OA, Koehler D, Vehreschild MJGT, Bohlius J, Wisplinghoff H, Vehreschild JJ (2019) Morbidity and mortality of candidaemia in Europe: an epidemiologic meta-analysis. Clin Microbiol Infect 25:1200–1212. https://doi.org/10.1016/j.cmi.2019.04.024
Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ (2018) Invasive candidiasis. Nat Rev Dis Primers 4:1–20. https://doi.org/10.1038/nrdp.2018.26
Talapko J, Juzbašić M, Matijević T, Pustijanac E, Bekić S, Kotris I, Škrlec I (2021) Candida albicans—the virulence factors and clinical manifestations of infection. J Fungi (Basel) 7:79. https://doi.org/10.3390/jof7020079
Kullberg BJ, Arendrup MC (2015) Invasive candidiasis. N Engl J Med 373:1445–1456. https://doi.org/10.1056/NEJMra1315399
Son HJ, Kim MJ, Lee S, Choi S, Jung KH, Jung J, Chong YP, Kim SH, Choi SH, Kim YS, Woo JH, Lee JY, Lee SO (2019) Risk factors and outcomes of patients with ocular involvement of candidemia. PLoS ONE 14:e0222356. https://doi.org/10.1371/journal.pone.0222356
Pfaller MA, Diekema DJ, Turnidge JD, Castanheira M, Jones RN (2019) Twenty years of the SENTRY antifungal surveillance program: results for Candida species from 1997–2016. Open Forum Infect Dis 15(Suppl 1):S79–S94. https://doi.org/10.1093/ofid/ofy358
Bassetti M, Righi E, Costa A, Fasce R, Molinari MP, Rosso R, Bobbio Pallavicini F, Viscoli C (2006) Epidemiological trends in nosocomial candidemia in intensive care. BMC Infect Dis 6:21. https://doi.org/10.1186/1471-2334-6-21
Richardson MD (2005) Changing patterns and trends in systemic fungal infections. J Antimicrob Chemother 56(Suppl 1):i5–i11. https://doi.org/10.1093/jac/dki218
Guinea J (2014) Global trends in the distribution of Candida species causing candidemia. Clin Microbiol Infect 20(Suppl 6):5–10. https://doi.org/10.1111/1469-0691.12539
Lai CC, Wang CY, Liu WL, Huang YT, Hsueh PR (2012) Time to positivity of blood cultures of different Candida species causing fungaemia. J Med Microbiol 61:701–704. https://doi.org/10.1099/jmm.0.038166-0
Clinical and Laboratory Standards Institute (2012) Reference method for broth dilution antifungal susceptibility testing of yeasts; fourth informational supplement. CLSI document M27-S4 (ISBN 1-56238-863-0 [Print]; ISBN 1-56238-864-9 [Electronic]). Wayne, PA, USA
European Committee on Antimicrobial Susceptibility Testing (2018) Antifungal agents. Breakpoint tables for interpretation of MICs, Version 9.0, valid from 2018–02–12. https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/Antifungal_breakpoints_v_9.0_180212.pdf. Accessed 9 Mar 2022
Takakura S, Fujihara N, Saito T, Kudo T, Iinuma Y, Ichiyama S (2003) National surveillance of species distribution in blood isolates of Candida species in Japan and their susceptibility to six antifungal agents including voriconazole and micafungin. J Antimicrob Chemother 53:283–289. https://doi.org/10.1093/jac/dkh053
Kakeya H, Yamada K, Kaneko Y, Yanagihara K, Tateda K, Maesaki S, Takesue Y, Tomono K, Kadota JI, Kaku M, Miyazaki Y, Kamei K, Shibuya K, Niki Y, Yoshida M, Sei Y (2018) National trends in the distribution of Candida species causing candidemia in Japan from 2003 to 2014. Med Mycol J 59:E19–E22. https://doi.org/10.3314/mmj.17-00014
Boonsilp S, Homkaew A, Phumisantiphong U, Nutalai D, Wongsuk T (2021) Species distribution, antifungal susceptibility, and molecular epidemiology of Candida species causing candidemia in a tertiary care hospital in Bangkok. Thailand J Fungi (Basel) 19:577. https://doi.org/10.3390/jof7070577
Makimura K, Suzuki T, Tamura T, Ikedo M, Hanazawa R, Takahashi Y, Yamada Y, Uchida K, Yamaguchi H (2004) Comparative evaluation of standard dilution method and commercial kit for frozen plate antifungal susceptibility testing of yeasts using 200 clinical isolates. Microbiol Immunol 48:747–753
Makimura K, Oguri T, Mikami Y, Kume H, Hanazawa R, Abe M, Ikeda R, Shinoda T (2005) Multicenter evaluation of commercial frozen plates for microdilution broth antifungal susceptibility testing of yeasts and comparison of MIC limits recommended in NCCLS M27–A2. Microbiol Immunol 49:97–106
Xiao M, Chen SCA, Kong F, Xu XL, Yan L, Kong HS, Fan X, Hou X, Cheng JW, Zhou ML, Li Y, Yu SY, Huang JJ, Zhang G, Yang Y, Zhang JJ, Duan SM, Kang W, Wang H, Xu YC (2020) Distribution and antifungal susceptibility of Candida species causing candidemia in China: an update from the CHIF-NET study. J Infect Dis 16:S139–S147. https://doi.org/10.1093/infdis/jiz573
Lindberg E, Hammarström H, Ataollahy N, Kondori N (2019) Species distribution and antifungal drug susceptibilities of yeasts isolated from the blood samples of patients with candidemia. Sci Rep 7:3838. https://doi.org/10.1038/s41598-019-40280-8
Yang ZH, Song YG, Li RY (2021) A ten-year retrospective study of invasive candidiasis in a tertiary hospital in Beijing. Biomed Environ Sci 34:773–788. https://doi.org/10.3967/bes2021.107
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, Reboli AC, Schuster MG, Vazquez JA, Walsh TJ, Zaoutis TE, Sobel JD (2015) Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis 62:e1-50. https://doi.org/10.1093/cid/civ933
Cornely OA, Bassetti M, Calandra T, Garbino J, Kullberg BJ, Lortholary O, Meersseman W, Akova M, Arendrup MC, Arikan-Akdagli S, Bille J, Castagnola E, Cuenca-Estrella M, Donnelly JP, Groll AH, Herbrecht R, Hope WW, Jensen HE, Lass-Flörl C, Petrikkos G, Richardson MD, Roilides E, Verweij PE, Viscoli C, Ullmann AJ (2012) ESCMID Fungal Infection Study Group, ESCMID* guideline for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clin Microbiol Infect 18(Suppl 7):19–37. https://doi.org/10.1111/1469-0691.12039
Das I, Nightingale P, Patel M, Jumaa P (2011) Epidemiology, clinical characteristics, and outcome of candidemia: experience in a tertiary referral center in the UK. Int J Infect Dis 15(11):e759-763. https://doi.org/10.1016/j.ijid.2011.06.006
Nagao M, Saito T, Doi S, Hotta G, Yamamoto M, Matsumura Y, Matsushima A, Ito Y, Takakura S, Ichiyama S (2012) Clinical characteristics and risk factors of ocular candidiasis. Diagn Microbiol Infect Dis 73:149–152. https://doi.org/10.1016/j.diagmicrobio.2012.03.006
Ueda T, Takesue Y, Tokimatsu I, Miyazaki T, Nakada-Motokawa N, Nagao M, Nakajima K, Mikamo H, Yamagishi Y, Kasahara K, Yoshihara S, Ukimura A, Yoshida K, Yoshinaga N, Izumi M, Kakeya H, Yamada K, Kawamura H, Endou K, Yamanaka K, Yoshioka M, Amino K, Ikeuchi H, Uchino M, Miyazaki Y (2019) The incidence of endophthalmitis or macular involvement and the necessity of a routine ophthalmic examination in patients with candidemia. PLoS ONE 14:e0216956. https://doi.org/10.1371/journal.pone.0216956
Andes DR, Safdar N, Baddley JW, Playford G, Reboli AC, Rex JH, Sobel JD, Pappas PG, Kullberg BJ (2012) Mycoses Study Group, Impact of treatment strategy on outcomes in patients with candidemia and other forms of invasive candidiasis: a patient-level quantitative review of randomized trials. Clin Infect Dis 54:1110–1122. https://doi.org/10.1093/cid/cis021
Nucci M, Anaissie E, Betts RF, Dupont BF, Wu C, Buell DN, Kovanda L, Lortholary O (2010) Early removal of central venous catheter in patients with candidemia does not improve outcome: analysis of 842 patients from 2 randomized clinical trials. Clin Infect Dis 51:295–303. https://doi.org/10.1086/653935
Liu CY, Huang LJ, Wang WS, Chen TL, Yen CC, Yang MH, Hsiao LT, Liu CY, Chen PM, Chiou TJ (2009) Candidemia in cancer patients: impact of early removal of non-tunneled central venous catheters on outcome. J Infect 58:154–160. https://doi.org/10.1016/j.jinf.2008.12.008
Garnacho-Montero J, Díaz-Martín A, García-Cabrera E, Pérez R, de Pipaón M, Hernández-Caballero C, Lepe-Jiménez JA (2013) Impact on hospital mortality of catheter removal and adequate antifungal therapy in Candida spp. bloodstream infections. J Antimicrob Chemother 68:206–213. https://doi.org/10.1093/jac/dks347
Lee YM, Kim DY, Kim YJ, Park KH, Lee MS (2019) Clinical impacts of delayed central venous catheter removal according to the severity of comorbidities in patients with candidaemia. J Hosp Infect 103:420–427. https://doi.org/10.1016/j.jhin.2019.08.018
Nucci M, Rocha Braga P, Nouér SA, Anaissie E (2018) Time of catheter removal in candidemia and mortality. Braz J Infect Dis 22:455–461. https://doi.org/10.1016/j.bjid.2018.10.278
Kutlu M, Sayın-Kutlu S, Alp-Çavuş S, Öztürk ŞB, Taşbakan M, Özhak B, Kaya O, Kutsoylu OE, Şenol-Akar Ş, Turhan Ö, Mermut G, Ertuğrul B, Pullukcu H, Banu Çetin Ç, Avkan-Oğuz V, Yapar N, Yeşim-Metin D, Ergin Ç (2022) Mortality-associated factors of candidemia: a multi-center prospective cohort in Turkey. Eur J Clin Microbiol Infect Dis 41:597–607. https://doi.org/10.1007/s10096-021-04394-0
Janum S, Afshari A (2016) Central venous catheter (CVC) removal for patients of all ages with candidaemia. Cochrane Database Syst Rev 7:CD011195. https://doi.org/10.1002/14651858.CD011195.pub2
Clancy CJ, Nguyen MH (2013) Finding the “missing 50%” of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin Infect Dis 56:1284–1292. https://doi.org/10.1093/cid/cit006
Acknowledgements
Editorial support in the form of medical writing, assembling tables, and creating high-resolution images based on authors’ detailed directions, collating author comments, copyediting, fact checking, and referencing was provided by Editage, Cactus Communications.
Author information
Authors and Affiliations
Contributions
Conceptualization: Hitoshi Tsukamoto, Takashi Higashi, Takaaki Kodawara, Hiromichi Iwasaki, Nobuyuki Goto.
Data curation: Hitoshi Tsukamoto, Takashi Higashi.
Formal analysis: Hitoshi Tsukamoto, Takashi Higashi, Kyohei Watanabe, Nobuyuki Goto.
Investigation: Hitoshi Tsukamoto, Takashi Higashi, Takaaki Kodawara, Kyohei Watanabe, Yukio Hida.
Project administration: Hiromichi Iwasaki, Nobuyuki Goto.
Supervision: Hiromichi Iwasaki, Nobuyuki Goto.
Validation: Hitoshi Tsukamoto, Takashi Higashi, Takaaki Kodawara, Kyohei Watanabe, Yukio Hida.
Visualization: Hitoshi Tsukamoto.
Writing—original draft: Hitoshi Tsukamoto.
Writing—review and editing: Hitoshi Tsukamoto, Takashi Higashi, Takaaki Kodawara, Kyohei Watanabe, Yukio Hida, Hiromichi Iwasaki, and Nobuyuki Goto.
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the institutional review board of the Faculty of Medical Sciences, University of Fukui (approval number: 20120089). The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The requirement for informed consent was waived due to the retrospective nature of the study.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tsukamoto, H., Higashi, T., Kodawara, T. et al. A longitudinal study of Candida bloodstream infections in a Japanese university hospital: species distribution, drug susceptibility, clinical features, and mortality predictors. Eur J Clin Microbiol Infect Dis 41, 1315–1325 (2022). https://doi.org/10.1007/s10096-022-04499-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-022-04499-0