
Abstract
To investigate the predictors and burden of hospital readmission with recurrent Clostridioides difficile infection (rCDI) in a large European healthcare system with a low prevalence of hyper-virulent C. difficile clones. We conducted an inception cohort study based on an exhaustive health insurance database and including all survivors of a first hospital stay with CDI over a one-year period (2015) in France. Readmissions with rCDI were defined as a novel hospital stay with CDI within 12 weeks following discharge of the index hospitalization. Risk factors for readmission with rCDI were investigated through multivariate logistic regression analyses. Among the 14,739 survivors of the index hospital stay (females, 57.3%; median age, 74 [58–84] years), 2135 (14.5%) required at least one readmission with rCDI. Independent predictors of readmission were age ≥ 65 years (adjusted odds ratio (aOR), 1.34, 95% confidence interval (CI), 1.21–1.49, P < 0.0001), immunosuppression (aOR, 1.27, 95% CI, 1.15–1.41, P < 0.0001), chronic renal failure (aOR, 1.29, 95% CI, 1.14–1.46, P < 0.0001), and a previous history of CDI (aOR, 2.05, 95% CI, 1.55–2.71, P < 0.0001). The cumulative number of risk factors was independently associated with the hazard of readmission. Mean acute care costs attributable to rCDI were 5619 ± 3594 Euros for readmissions with rCDI as primary diagnosis (mean length of stay, 11.3 ± 10.2 days) and 4851 ± 445 Euros for those with rCDI as secondary diagnosis (mean length of stay, 16.8 ± 18.2 days), for an estimated annual nation-wide cost of 14,946,632 Euros. Hospital readmissions with rCDI are common after an index episode and drive major healthcare expenditures with substantial bed occupancy, strengthening the need for efficient secondary prevention strategies in high-risk patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The growing burden of Clostridioides difficile infections (CDI, formerly Clostridium difficile infections) stands as a global public health threat [1]. Indeed, C. difficile is the main pathogen responsible for hospital-acquired diarrhea—with a marked cross-transmissibility resulting in epidemics in hospitals and long-term care facilities—while the incidence of community-acquired CDI is rising steadily [2, 3]. At the individual level, the occurrence of CDI translates into worsened morbidity and discomfort, extended length of hospital stay (LOS), and a substantial mortality attributable to both severe presentations (e.g., pseudomembranous colitis, toxic megacolon, and related organ failures) and the frailty of at-risk patient populations [4, 5]. At the hospital scale, CDI account for major expenditures and organizational challenges ensuing from additional healthcare resources utilization and the implementation of barrier precautions to prevent dissemination [6, 7].
CDI is characterized by a recurrence rate ranging from 15 to 25% that dramatically amplifies the global burden of the disease [1]. Age over 65 years, immunosuppression, severe comorbidities, a previous history of CDI, an index CDI episode meeting the criteria for severe complicated disease or involving a hyper-virulent C. difficile strain, the continuation of drugs that impair the normal gut microbiome (i.e., antimicrobial agents or proton-pump inhibitors), and the use of metronidazole rather than vancomycin or fidaxomicin as first-line regimen may predispose to recurrent CDI (rCDI) [8, 9].
Yet, predictors of hospital readmission with rCDI after an index episode and its impact on healthcare costs and bed occupancy remain scarcely investigated in large epidemiological studies. Of note, most of available data on these issues originate from the USA [10,11,12] and may not be directly transposable to other ecological and medico-economic environments. Further, defining patient subgroups with the higher hazard of readmission with rCDI could help better targeting the implementation of secondary prevention strategies [13].
The objectives of this study were to investigate the predictors and nation-wide burden of hospital readmission with rCDI after an index CDI episode using an exhaustive administrative database over a one-year period in France.
Patients and methods
Study design and data source
This retrospective inception cohort study was conducted by exploiting the French Health Insurance database (Programme de Médicalisation des Systèmes d’Information - PMSI). This exhaustive database includes all hospital stays in public and private care facilities with prospectively collected data on patient demographics, hospitalization unit (i.e., medical or surgical wards, intensive care unit (ICU), and rehabilitation or long-term care facilities), main and secondary diagnoses of the hospital stay using the 10th revision of the International Classification of Diseases (ICD-10), PMSI codes for resource utilization (including radiological, surgical, and invasive medical procedures), LOS, and vital status at discharge. A personal identification number is attributed to each single patient, enabling the search for iterative hospital admissions over a given period. Of note, information on deaths occurring outside the French hospital system is not available in the database. In compliance with French law on electronic data sources, this database is registered at the Commission Nationale de l’Informatique et des Libertés (registration number, 2019044). The protocol of this observational study was not submitted to an ethical committee since all data were fully anonymized at baseline. Results are reported according to the STROBE guidelines (www.strobe-statement.org). The study sponsor was not involved in data acquisition, statistical analyses, or interpretation of the results.
Patient selection and definitions
We first identified all patients with at least one hospital admission with the ICD-10 code for CDI (i.e., A04.7) as main or secondary diagnosis between January 1 and December 31, 2015, without age restriction. The index episode of CDI was defined as the first hospital stay with CDI and was considered as cured at hospital discharge. Hospital readmission with rCDI was defined as a new stay with CDI as main or secondary diagnosis within 12 weeks following discharge of the index hospital stay. This extended period when compared with the 8-week timeframe established by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines [9] to define rCDI was chosen to fit with recent randomized controlled trials (RCT) focused on rCDI prevention, and in whom recurrence was defined as a new episode occurring up to 12 weeks following the index case [14,15,16]. A 12-week rolling period was applied to distinguish index episodes and recurrences—that is, back to October 1, 2014, for patients enrolled on January 1, 2015, and until April 1, 2016, for patient enrolled on December 31, 2015. Survivors of the index hospital stay with CDI were included in the study cohort. Only the first index CDI was considered for patients with two or three index episodes (i.e., more than 12 weeks apart) over the study period.
Variables presented in the tables were extracted from the database. Age ≥ 65 years, chronic renal failure, immunosuppression, a history of previous CDI between 24 and 12 weeks before the index episode (i.e., not defining a recurrence), and a severe complicated index episode of CDI were considered as risk factors for rCDI, in accordance with the ESCMID guidelines [9]. A severe complicated episode of CDI was defined by the occurrence of at least one complication among acute renal failure, paralytic ileus, septic shock, ICU admission, and need for unscheduled colectomy during the same hospital stay, as adapted from the ESCMID definition [9]. The ICD-10 and PMSI code lists used for these definitions were elaborated by author consensus (Table S1 in the electronic supplementary data—ESD).
Burden of rCDI
The financial burden of rCDI was appraised using the DRG (diagnosis-related groups of patients) and MEG (medico-economic groups of patients) administrative tools which are uniformly applied in France for activity-based funding of acute care hospitals and rehabilitation or long-term care facilities, respectively. For patients with rCDI as the primary diagnosis, we measured the global cost of the hospital stay. For patients with rCDI as secondary diagnosis, we performed a case-control study by matching these patients (1:1 ratio) on age, sex, main diagnosis of the index hospital stay, and the need for ICU admission with non-CDI patients randomly selected in the database over the same 1-year period. Incremental costs related to CDI were then calculated as the cost difference between the two groups of patients using the DRG and MEG nomenclatures, as appropriate. The same methodology was applied for index hospital stays. The annual financial burden of CDI was estimated as the sum of costs attributable to CDI for both index hospital stays and readmissions. Additional information on cost measurement is provided with Table S2 in the ESD. Recurrences occurring during the index hospital stay and those managed in the outpatient setting were not considered.
Statistical analyses
Categorical variables are expressed as number (percentage) and continuous variables as mean ± standard deviations (SD) or median (25th–75th percentile, IQR). Patients with and without hospital readmission with rCDI were compared using the Student t test for continuous variables and the χ2 test or the Fisher exact test for categorical variables. The Wilcoxon or Kruskal–Wallis non-parametric tests were used when appropriate.
To identify risk factors for hospital readmission with rCDI, we first performed bivariate analyses to compare survivors of the index hospital stay with at least one readmission to those not readmitted. Analyses were restrained to the first readmission in patients with multiple readmissions with rCDI. Variables yielding P value < 0.2 were then entered into a backward multivariate logistic regression model for the calculation of adjusted odds ratio (aOR) and corresponding 95% confidence interval (CI), handling readmission with rCDI as the primary outcome. This model was applied on both the whole cohort and a sub-cohort excluding the patients who died during another hospital stay without rCDI within the 12-week timeframe. Another multivariate logistic regression model was built to appraise whether the cumulative number of risk factors for rCDI—rather than risk factors separately—may impact the hazard of readmission with rCDI. No variable was forced into these models. Kaplan–Meier curves of readmission-free survival according to the number of risk factors were compared using the log-rank test. Only deaths occurring during a new hospital stay without rCDI were considered for these analyses. All tests were two-sided, and P values < 0.05 were considered statistically significant. Analyses were carried out using the SAS® version 9.3 (SAS Institute, Cary, NC, USA).
Results
Study cohort
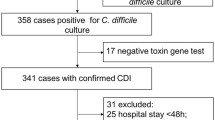
A total of 16,794 patients experienced an index hospital stay with CDI over the year 2015 in France and 2055 (12.2%) died during this first hospitalization (Fig. 1 and Table S3). The remaining 14,739 patients (females, 57.3%; age, 74 [58–84] years) were included in the study (Table 1). Among them, 9638 (65.4%) were aged 65 years or older, 2081 (14.1%) suffered from chronic renal failure, 3828 (26.0%) were immunocompromised (mostly solid neoplasms and hematological malignancies), 1628 (11.0%) met the criteria for a severe complicated index episode of CDI, and only 267 (1.8%) had a previous history of CDI before the index episode. Overall, 11,790 survivors (80.0%) had at least one risk factor for rCDI (one factor, 58.1%; two factors, 19.5%; three or four factors, 2.4%; five factors, none).

Study flowchart. CDI, Clostridioides difficile infection; rCDI, recurrent CDI
Predictors of hospital readmission with rCDI
Among the 14,739 survivors of the index hospital stay, 2135 (14.5%) required at least one readmission with rCDI within 12 weeks following discharge (mean interval between discharge and readmission, 18 ± 20 days). More than 80% of readmission with rCDI occurred within 8 weeks, whichever the number of risk factors for rCDI (Fig. 2). Survivors with and without readmission are compared in Table 1.

Kaplan–Meier curves of survival without hospital readmission with recurrent Clostridioides difficile infection (rCDI) according to the number of risk factors for rCDI. CDI, Clostridioides difficile infection. Risk factors for recurrent CDI: age older than 65 years, chronic renal failure, immunosuppression, severe complicated index episode of CDI, and a previous history of CDI before the index episode. Only deaths occurring during a new hospital stay without rCDI were considered since information on deaths occurring outside the French hospital system was not available in the database
By multivariate analysis, independent risk factors for hospital readmission with rCDI were age ≥ 65 years (aOR 1.34, 95% CI 1.21 to 1.49, P < 0.0001), immunosuppression (aOR 1.27, 95% CI 1.15 to 1.41, P < 0.0001), chronic renal failure (aOR 1.29, 95% CI 1.14 to 1.46, P < 0.0001), and an history of CDI (aOR 2.05, 95% CI 1.55 to 2.71, P < 0.0001) (Table 2). Conversely, cerebrovascular diseases (aOR 0.73, 95% CI 0.58 to 0.91, P = 0.004) and dementia (aOR 0.73, 95% CI 0.61 to 0.88, P = 0.001) were protective (Table 2). Of note, a severe complicated index episode of CDI was slightly more common in patients with readmission than in those without (12.6% versus 10.8%, respectively, P < 0.0001); however, this feature had no independent impact on the hazard of readmission with rCDI after adjustment on potential confounders. Similar results were obtained in a second multivariate model excluding the 969 patients (6.6%) who died during another hospital stay without rCDI within the 12-week timeframe (Table S4).
The potential effect of the cumulative number of pre-specified risk factors for rCDI was appraised in a third multivariate model (Table S5). Patients with two (aOR 1.77, 95% CI 1.51 to 2.07, P < 0.0001) or three to four (aOR 1.67, 95% CI 1.23 to 2.26, P = 0.001) risk factors were at higher hazard of readmission with rCDI than those with only one (aOR 1.50, 95% CI 1.31 to 1.71, P < 0.0001) or no (reference, aOR = 1) risk factor.
Burden of hospital readmission with rCDI
Average hospital LOS for readmissions with rCDI as primary or secondary diagnosis were 11.3 ± 10.2 and 16.8 ± 18.2 days, respectively (Table 3). The mean inclusive cost of readmissions with rCDI as primary diagnosis (n = 1392) was evaluated as 5619 ± 3594 Euros versus 5276 ± 3929 Euros for index hospital stays (Table 3). Mean extra-costs attributable to rCDI for readmissions with rCDI as secondary diagnosis (n = 1378) were evaluated as 4851 ± 445 Euros versus 8535 ± 242 Euros for index hospital stays. Additional costs are detailed in Table 3. Overall annual costs attributable to rCDI were estimated as 14,946,632 Euros—that is, 10.5% of the nation-wide financial burden of CDI (estimation, 142,619,422 Euros for the year 2015).
Outcome of hospital readmission with rCDI
The overall in-hospital mortality rate in patients with a first readmission for rCDI was 12.6% (n = 270). Among the 1865 patients who survived to this first readmission, 422 (22.6%) required one or more additional readmissions for rCDI (second readmission, n = 296; third readmission and beyond, n = 126).
Discussion
Predictors of hospital readmission with rCDI and associated costs remain under-investigated in large European hospital systems. In this study including 14,739 inpatients discharged alive after an index episode of CDI over a one-year period in France, age ≥ 65 years, immunosuppression, chronic renal failure, and a previous history of CDI were independently linked with a higher hazard of readmission (overall rate, 14.5%), this association strengthening as the cumulative number of risk factors increased. The annual cost burden of readmission with rCDI was estimated as almost 15 million Euros.
Previous studies reported an 8–11% rate of hospital readmission with rCDI after an index episode [6, 12, 17,18,19,20]. However, most of these works were conducted in referral hospitals where the management of index cases may differ from practices implemented in non-specialized healthcare settings. In addition, available data on readmission with rCDI mainly comes from North America, a region where the hyper-virulent BI/NAP-1/027 strain of C. difficile has successfully disseminated. The prevalence of this ribotype independently associated with rCDI has declined markedly over the recent years in Europe, especially in France where the overall prevalence of hyper-virulent C. difficile clones remains currently limited. [21, 22] The 14.5% rate of readmission that we observed in this nation-wide cohort highlights the need for sustained efforts to prevent rCDI even in healthcare systems with low endemicity of such hyper-virulent strains.
Older age, immunosuppression, chronic renal failure, and a history of CDI have been identified as independent risk factors for rCDI [23,24,25,26]. Still, whether these factors may predict hospital readmission with rCDI had not been precisely appraised. Here, we demonstrated that patients exhibiting these baseline characteristics were at higher risk of being readmitted. This appears especially meaningful as the proportion of at-risk inpatients—notably those aged and/or immunocompromised—are expected to increase in the years to come. Strikingly, cerebrovascular diseases and dementia exerted an apparent protective effect, a finding that possibly reflects physicians’ decision not to re-hospitalize institutionalized patients with poor performance status or extra-hospital mortality ensuing from severe underlying conditions and not colligated in the PMSI database.
Overall, 80% of patients presented at least one risk factor for rCDI; therefore, identifying those with the higher hazard of readmission remains challenging. Considering the cumulative number of risks factors could be a rational approach when discussing the indication of expensive secondary prevention strategies after an index hospital stay with CDI. Vancomycin and fidaxomicin are currently the recommended drugs for a first episode, especially when risk factors for rCDI are present [9, 27]. The cost-effectiveness of fidaxomicin to prevent a first recurrence remains equivocal when compared to vancomycin [28] yet might improve when extended-pulsed regimens are prescribed. [29] Model-based analyses suggest that bezlotoxumab—a monoclonal antibody directed against C. difficile toxin B—is cost-effective for rCDI prevention when combined to standards of care for index CDI cases [30]. Of note, a post-hoc analysis of the MODIFY-I/II RCTs suggests that bezlotoxumab has the greatest preventive effect in patients with three or more risk factors, while no relevant impact was observed in those with no risk factor [31]. The potential role of fecal microbiota transplantation as a first-line treatment for CDI is currently evaluated [32].
Studies conducted in tertiary care hospitals in the USA and Europe estimated the extra-costs attributable to rCDI in inpatients as ranging from 8488 to 9960 Euros [6, 11, 20, 33]. Our estimations based on the French Health Insurance invoicing algorithms are slightly below these values as a likely result of more heterogeneous case-mix and patient management. Nevertheless, the nation-wide annual cost of hospital readmission with rCDI—that is, roughly 15 million Euros or 10.5% of overall annual CDI-related costs—was consistent with a previous estimation from 12 French acute care hospitals [6] and underlines the burden of rCDI on the healthcare system. However, our study was conducted on a cohort of patients hospitalized with CDI in 2015. Hence, we cannot firmly exclude that this amount decreased over the more recent years owing to improved management of patients at high risk for rCDI.
Strengths of this study include the large number of enrolled patients, the exploitation of an exhaustive nation-wide database that ensures external validity, and the accurate appraisal of readmission-related costs using standardized administrative tools. Yet, several limitations inherent to claims data analysis should be underlined. First, definitions for CDI episodes, severity criteria, and comorbidities were based on ICD-10 coding, without further medical chart review, which could have led to a degree of patient misclassification owing to reporting omission. Next, the impact of certain well-established risk factors for rCDI could not be evaluated since they were not available in the database—this especially applies for antibiotic exposure [9], the pharmacological management of index episodes [34], and serum levels of anti-toxin B antibodies [35]. Third, certain risk factors for rCDI (i.e., older ages, immunosuppression, and chronic renal failure) exert an independent impact on the hazard of short-term death in survivors of a first hospital stay with CDI. Since out-of-hospital deaths were not mentioned in the database, the competing risk of death could not be taken into account when appraising the incidence and predictors of readmission with rCDI. Lastly, analyses were restrained to the first readmission with rCDI, which could have underestimated total healthcare costs. However, only 3% of included patients experienced more than one readmission over the study period.
In conclusion, readmissions with rCDI are commonly required in French patients discharged after an index episode and are responsible for a significant part of the global burden of CDI. Secondary prevention strategies—along with the use of vancomycin or fidaxomicin—should be discussed upon the index episode in patients cumulating two or more risk factors for readmission.
References
Evans CT, Safdar N (2015) Current trends in the epidemiology and outcomes of Clostridium difficile infection. Clin Infect Dis 60(Suppl 2):S66–S71
Lessa FC, Winston LG, McDonald LC (2015) Burden of Clostridium difficile infection in the United States. N Engl J Med 372:2369–2370
Chitnis AS, Holzbauer SM, Belflower RM, Winston LG, Bamberg WM, Lyons C et al (2013) Epidemiology of community-associated Clostridium difficile infection, 2009 through 2011. JAMA Intern Med 173:1359–1367
Gao T, He B, Pan Y, Deng Q, Sun H, Liu X et al (2015) Association of Clostridium difficile infection in hospital mortality: a systematic review and meta-analysis. Am J Infect Control 43:1316–1320
Barbut F, Bouee S, Longepierre L, Goldberg M, Bensoussan C, Levy-Bachelot L (2018) Excess mortality between 2007 and 2014 among patients with Clostridium difficile infection: a French health insurance database analysis. J Hosp Infect 98:21–28
Le Monnier A, Duburcq A, Zahar JR, Corvec S, Guillard T, Cattoir V et al (2015) Hospital cost of Clostridium difficile infection including the contribution of recurrences in French acute-care hospitals. J Hosp Infect 91:117–122
Dubberke ER, Olsen MA (2012) Burden of Clostridium difficile on the healthcare system. Clin Infect Dis 55(Suppl 2):S88–S92
Ma GK, Brensinger CM, Wu Q, Lewis JD (2017) Increasing incidence of multiply recurrent Clostridium difficile infection in the United States: a cohort study. Ann Intern Med 167:152–158
Debast SB, Bauer MP, Kuijper EJ (2014) European society of clinical microbiology and infectious diseases: update of the treatment guidance document for Clostridium difficile infection. Clin Microbiol Infect 20(Suppl 2):1–26
Rodrigues R, Barber GE, Ananthakrishnan AN (2017) A comprehensive study of costs associated with recurrent Clostridium difficile infection. Infect Control Hosp Epidemiol 38:196–202
Dubberke ER, Schaefer E, Reske KA, Zilberberg M, Hollenbeak CS, Olsen MA (2014) Attributable inpatient costs of recurrent Clostridium difficile infections. Infect Control Hosp Epidemiol 35:1400–1407
Zhang D, Prabhu VS, Marcella SW (2018) Attributable healthcare resource utilization and costs for patients with primary and recurrent Clostridium difficile infection in the United States. Clin Infect Dis 66:1326–1332
Martin J, Wilcox M (2016) New and emerging therapies for Clostridium difficile infection. Curr Opin Infect Dis 29:546–554
van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG, de Vos WM et al (2013) Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 368:407–415
Wilcox MH, Gerding DN, Poxton IR, Kelly C, Nathan R, Birch T et al (2017) Bezlotoxumab for prevention of recurrent Clostridium difficile infection. N Engl J Med 376:305–317
Guery B, Menichetti F, Anttila VJ, Adomakoh N, Aguado JM, Bisnauthsing K et al (2018) Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis 18:296–307
Olsen MA, Yan Y, Reske KA, Zilberberg M, Dubberke ER (2015) Impact of Clostridium difficile recurrence on hospital readmissions. Am J Infect Control 43:318–322
Collins CE, Ayturk MD, Anderson FA Jr, Santry HP (2015) Predictors and outcomes of readmission for Clostridium difficile in a national sample of medicare beneficiaries. J Gastrointest Surg 19:88–99 discussion 99
Kurti Z, Lovasz BD, Mandel MD, Csima Z, Golovics PA, Csako BD et al (2015) Burden of Clostridium difficile infection between 2010 and 2013: trends and outcomes from an academic center in Eastern Europe. World J Gastroenterol 21:6728–6735
Zilberberg MD, Nathanson BH, Marcella S, Hawkshead JJ 3rd, Shorr AF (2018) Hospital readmission with Clostridium difficile infection as a secondary diagnosis is associated with worsened outcomes and greater revenue loss relative to principal diagnosis: a retrospective cohort study. Medicine (Baltimore) 97:e12212
Couturier J, Davies K, Gateau C, Barbut F (2018) Ribotypes and new virulent strains across Europe. Adv Exp Med Biol 1050:45–58
Davies KA, Ashwin H, Longshaw CM, Burns DA, Davis GL, Wilcox MH (2016) Diversity of Clostridium difficile PCR ribotypes in Europe: results from the European, multicentre, prospective, biannual, point-prevalence study of Clostridium difficile infection in hospitalised patients with diarrhoea (EUCLID), 2012 and 2013. Euro Surveill 21
Cornely OA, Crook DW, Esposito R, Poirier A, Somero MS, Weiss K et al (2012) Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 12:281–289
Eyre DW, Walker AS, Wyllie D, Dingle KE, Griffiths D, Finney J et al (2012) Predictors of first recurrence of Clostridium difficile infection: implications for initial management. Clin Infect Dis 55(Suppl 2):S77–S87
Garey KW, Sethi S, Yadav Y, DuPont HL (2008) Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect 70:298–304
D'Agostino RB Sr, Collins SH, Pencina KM, Kean Y, Gorbach S (2014) Risk estimation for recurrent Clostridium difficile infection based on clinical factors. Clin Infect Dis 58:1386–1393
McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE et al (2018) Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 66:987–994
Le P, Nghiem VT, Mullen PD, Deshpande A (2018) Cost-effectiveness of competing treatment strategies for Clostridium difficile infection: a systematic review. Infect Control Hosp Epidemiol 39:412–424
Cornely OA, Watt M, McCrea C, Goldenberg SD, De Nigris E (2018) Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients aged >/=60 years (EXTEND): analysis of cost-effectiveness. J Antimicrob Chemother 73:2529–2539
Prabhu VS, Dubberke ER, Dorr MB, Elbasha E, Cossrow N, Jiang Y et al (2018) Cost-effectiveness of bezlotoxumab compared with placebo for the prevention of recurrent Clostridium difficile infection. Clin Infect Dis 66:355–362
Gerding DN, Kelly CP, Rahav G, Lee C, Dubberke ER, Kumar PN et al (2018) Bezlotoxumab for prevention of recurrent Clostridium difficile infection in patients at increased risk for recurrence. Clin Infect Dis 67:649–656
Juul FE, Garborg K, Bretthauer M, Skudal H, Oines MN, Wiig H et al (2018) Fecal microbiota transplantation for primary Clostridium difficile infection. N Engl J Med 378:2535–2536
Wilcox MH, Ahir H, Coia JE, Dodgson A, Hopkins S, Llewelyn MJ et al (2017) Impact of recurrent Clostridium difficile infection: hospitalization and patient quality of life. J Antimicrob Chemother 72:2647–2656
Beinortas T, Burr NE, Wilcox MH, Subramanian V (2018) Comparative efficacy of treatments for Clostridium difficile infection: a systematic review and network meta-analysis. Lancet Infect Dis 18:1035–1044
Gupta SB, Mehta V, Dubberke ER, Zhao X, Dorr MB, Guris D et al (2016) Antibodies to toxin B are protective against Clostridium difficile infection recurrence. Clin Infect Dis 63:730–734
Funding
This study was supported by MSD.
Author information
Authors and Affiliations
Contributions
Concept and design: A. Dinh, S. Alimi., A. Duburcq and F. Barbier.
Acquisition of data: C. Emery, E. Torreton and A. Duburcq.
Statistical analysis: C. Emery, E. Torreton and A. Duburcq.
Interpretation of results: A. Dinh, A. Le Monnier, A. Duburcq and F. Barbier.
Writing of the manuscript: A. Dinh, A. Le Monnier and F. Barbier.
Critical revision of the manuscript for important intellectual content: all authors.
Corresponding author
Ethics declarations
The database exploited for this study is registered at the Commission Nationale de l’Informatique et des Libertés (registration number, 2019044), in compliance with French law on electronic data sources. The protocol of this retrospective observational study was not submitted to an ethical committee since all data were fully anonymized at baseline.
Conflict of interest
FB: MSD (conference and lecture fees, conference invitation), Pfizer (conference invitation), BioMérieux (conference fees).
AD: MSD (conference and lecture fees, conference invitation), Pfizer (conference invitation), InfectoPharm (conference and lecture fees), Sanofi-Pasteur (conference and lecture fees), Correvio (conference and lecture fees).
ALM: MSD (conference invitation), Astellas (conference and lecture fees, conference invitation), Pfizer (conference invitation), Cepheid (conference and lecture fees), bioMérieux (conference and lecture fees), Sanofi-Pasteur (conference and lecture fees).
Other authors: no conflict of interest to declare.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 30 kb)
Rights and permissions
About this article

Cite this article
Dinh, A., Le Monnier, A., Emery, C. et al. Predictors and burden of hospital readmission with recurrent Clostridioides difficile infection: a French nation-wide inception cohort study. Eur J Clin Microbiol Infect Dis 38, 1297–1305 (2019). https://doi.org/10.1007/s10096-019-03552-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-019-03552-9