
Abstract
To evaluate the early absolute CD64/CD15/CD45 neutrophil count as a marker of prognosis of sepsis outcome the absolute CD64/CD15/CD45 count was measured by flow cytometry in 65 patients with confirmed or suspected Gram-negative sepsis and organ dysfunction. Serum interleukin(IL)-8 and interferon-gamma (IFNγ) were measured by an enzyme immunoassay. An absolute count lower than 2500 cells/mm3 could early discriminate non-survivors with sensitivity 82.9% (OR 3.46, 95%CIs 1.10–10.95, p 0.042). After forward step-wise Cox- regression analysis, it was found that acute coagulopathy, acute renal injury, and an early absolute CD64/CD15/CD45 count lower than 2500/mm3 were independently associated with unfavorable outcome. The OR for death among patients with an absolute CD64/CD15/CD45 neutrophil count greater than 2500/mm3 and circulating IL-8 greater than 95 pg/ml was 0.44; this was significantly increased to 7.44 among patients with an absolute CD64/CD15/CD45 neutrophil count lower than 2500/mm3 (p 0.045 by the Breslow-Day’s test; p 0.046 by the Tarone’s test). An absolute CD64/CD15/CD45 count below 2500/mm3 can be a useful prognosticator of sepsis outcome and a probable indicator of sepsis immunosuppression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The potential of the host for efficient phagocytosis is one of major dysregulated item of the host response in sepsis. This seems to be related with the modulation of the expression of the CD64 molecule on the cell membrane of neutrophils [1]. The CD64 antigen is a high-affinity receptor for the Fc gamma part of the IgG heavy chain and can bind monomeric IgG1 and IgG3 as well as aggregated IgG. A high expression of this receptor is found on monocytes and a low on resting neutrophils at a normal state. Upregulation of the receptor expression on neutrophils is conducted a few hours after activation by pro-inflammatory cytokines like interferon-gamma (IFNγ). This upregulation represents a physiological process promoting neutrophils to act as phagocytes. When the stimulus is decreased, CD64 expression returns to its basal levels within a few days [2].
Although the expression of CD64 on neutrophils has been proposed as diagnostic tool in sepsis [3], available studies are focusing on the percentage of circulating neutrophils that express this receptor and not on their absolute number. It is highly plausible that the real important knowledge may rely not on the percentage of expression but on the absolute count of neutrophils expressing CD64. The aim of the present study was to investigate whether the absolute counts of CD64-expressing neutrophils are related to outcome.
Patients and methods
Study design
This study is a sub-study conducted within a prospective, randomized clinical trial investigating the role of intravenous administration of clarithromycin for the management of patients with proven or suspected infection by Gram-negative bacteria [4] (www.clinicaltrials.gov registration NCT01223690). It was approved by the Ethics Committee of the ATTIKON University hospital (266/27-07-09). The sub-study was designed to investigate how surface expression the Fc gamma receptor on neutrophils is related to final outcome. Patients were enrolled after written informed provided by themselves or by first-degree relatives in case of patients unable to consent. The inclusion criteria were (a) age more than or equal to 18 years, b) severe sepsis or septic shock defined by the sepsis-2 definitions since the study was designed before the introduction of the sepsis-3 definitions, and (c) blood sampling within 24 h from the first organ failure. The exclusion criteria were (a) infection by the human immunodeficiency virus HIV-1, (b) neutropenia defined as less than 1.000 neutrophils/mm3, (c) intake of chemotherapy, and (d) chronic corticosteroid intake defined as more than 0.4 mg/kg equivalent prednisone daily for more than 15 consecutive days. Eight milliliters of whole blood was collected from each participant under sterile conditions by vein puncture of one forearm vein before randomization into blind treatment; 5 ml was transferred in one EDTA-coated tube for flow cytometry, and another 3 ml into one pyrogen-free tube for serum separation (Becton Dickinson, Cockeysville, MD, USA).
Survival was recorded for 28 days after start of blind treatment. Since 28-day mortality did not differ between patients allocated to each treatment arm, patients randomized to both arms were analyzed for the needs of this study together. Demographic and clinical data of age, gender, APACHE II score, SOFA score, presence of chronic comorbidities, type of infection, and microbiology were also recorded.
Laboratory investigation
Whole blood was incubated with the monoclonal antibodies anti-CD15 at the fluorochrome fluorescein isothiocyanate (FITC, emission 525 nm, Immunotech, Marseille, France), anti-CD64 at the phycoerythrin (PE, emission 575 nm CYTO-STAT, Miami, Florida, US), and anti-CD45 at the fluorochrome phycoerythrin-Cy5 (PC5, emission 650 nm, Immunotech). Red blood cells were lysed using VersaLyse Lysing Solution (Beckman Coulter, Immunotech, Marseille, France). White blood cells were analyzed after running through the Cytomics FC-500 flow cytometer with gating for granulocytes based on their characteristic SS/CD45 expression. Granulocytes expressing the surface marker CD15 were considered neutrophils. Fluorospheres (Immunotech) were used for the determination of absolute counts. IgG isotypic controls at the fluorochromes FITC and PE (Immunotech) were analyzed before the start of the analysis for every patient.
Serum was collected from each patient and stored at -70 °C until assay. Concentrations of interleukin-8 (IL-8) and IFNγ were measured in duplicate by enzyme immunoassay (Affymetrix, Santa Clara, CA, USA). The lower detection limits was 7.8 pg/ml for IL-8 and 19.5 pg/ml for IFNγ.
Power of the study
It was hypothesized that after receiver operator characteristic (ROC) curve analysis of the absolute counts of CD64-expressing neutrophils, a cut off associated with sensitivity more than 80% for prediction of unfavorable outcome could be found. In order to achieve this with power more than 80% at a level of significance of 10%, it was calculated that 60 patients should be enrolled.
Statistical analysis
Patients were divided into 28-day survivors and non-survivors. Comparisons of baseline demographics were done by the chi-square test for qualitative variables and by the Mann-Whitney U test for quantitative variables. Receiver operator characteristics (ROC) curve analysis was done to identify a cut-off of the absolute count of CD64-expressing neutrophils upon enrollment that could discriminate between survivors and non-survivors. Odds ratio (ORs) and 95% confidence intervals (CIs) for unfavorable outcome based on a cut-off with more than 80% sensitivity were determined according to Mantel-Haenszel statistics. ORs were compared by the Breslow-Day’s and the Tarone’s tests. Comparative survival analysis was done by the log-rank test. Forward Cox-regression analysis of variables associated with unfavorable outcome was done; statistically significant variables entered the analysis as independent variables. Serum IL-8 and IFNγ were compared by the Mann-Whitney U test. Any value of p below 0.05 was considered statistically significant.
Results
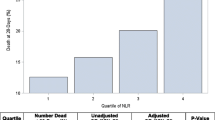
From the total number of enrolled patients in the clinical trial, 65 patients participated in this sub-study. Baseline demographics and clinical characteristics of survivors and non-survivors are shown in Table 1. As shown in the table, the absolute counts of CD64/CD15/CD45 neutrophils were significantly decreased in non-survivors compared to survivors. Based on this observation, a ROC curve was designed to discriminate between survivors and non-survivors based on the absolute counts of CD64/CD15/CD45 neutrophils on the first day of sepsis. The area under the ROC curve was significant (0.69, 95%CIs: 055–0.83, p 0.024) (data not shown). A cut-off point of 2500 cells/mm3 of CD64/CD15/CD45 neutrophils could early discriminate non-survivors with sensitivity 82.9% (OR 3.46, 95%CIs 1.10–10.95, p 0.042) (Fig. 1a). Results were also confirmed by survival analysis (Fig. 1b).

a Prognostic performance of the early absolute CD64/CD15/CD45 neutrophil count of the prediction of final outcome. b survival analysis according to the early absolute CD64/CD15/CD45 neutrophil count
Abbreviations: NPV: negative predictive value; PPV: positive predictive value; Sens: sensitivity; Spec: specificity.
From the total enrolled patients, sepsis was microbiologically confirmed in 35 patients and not confirmed in 30 patients; 13 (37.1%) and 11 (36.7%) patients respectively had at baseline lower than 2500/mm3 CD64/CD15/CD45 neutrophils (p: 1.00).
Forward step-wise Cox- regression analysis was performed to associate the independent association of the eight variables different between survivors and non-survivors (shown in Table 1) with final outcome. After three steps of analysis, it was found that acute coagulopathy, acute renal injury, and an early absolute CD64/CD15/CD45 count lower than 2500/mm3 were independently associated with unfavorable outcome (Table 2).
In order to provide some mechanistic explanation of the observation, circulating IL-8 and IFNγ were compared between survivors and non-survivors according to their absolute CD64/CD15/CD45 count. The only difference was found for IL-8 being greater in non-survivors with CD64/CD15/CD45 count lower than 2500/mm3 (Fig. 2). We next asked the question if increased circulating IL-8 was independent from or it was associated with the low absolute CD64/CD15/CD45 neutrophil count. Using ROC analysis, we found that IL-8 greater than 95 pg/ml was associated with sensitivity greater than 80% with unfavorable 28-day outcome (data not shown). The OR for death among patients with an absolute CD64/CD15/CD45 neutrophil count greater than 2500/mm3 and circulating IL-8 greater than 95 pg/ml was 0.44 (95%CIs: 0.04–5.01); this was significantly increased to 7.44 (95%CIs 1.44–38.41) among patients with an absolute CD64/CD15/CD45 neutrophil count lower than 2500/mm3 (p 0.045 by the Breslow-Day’s test; p 0.046 by the Tarone’s test).

Circulating cytokines according to 28-day outcome and early absolute CD64/CD15/CD45 neutrophil count a interleukin (IL)-8 and b interferon-gamma (IFNγ). P values refer to comparisons between survivors and non-survivors
Discussion
In this study, it was shown that an early absolute CD64/CD15/CD45 neutrophil count lower than 2500/mm3 was an independent variable associated with 28-day mortality. Although at first glance APACHE II and SOFA score seem to provide better predictive capacity of the final outcome than the early absolute CD64/CD15/CD45 neutrophil count, it needs to be outlined that the validity of the early absolute CD64/CD15/CD45 neutrophil count as an independent prognosticator of final outcome is coming from forward step-wise logistic regression analysis of all different variables at baseline between survivors and non-survivors where SOFA and APACHE II were included. This low neutrophil count acted synergistically with high circulating IL-8 to further predict unfavorable outcome.
Over the last decade, CD64-expression on neutrophils has been proposed as a biomarker for sepsis diagnosis superior to serum pro-inflammatory cytokines and to clinical scores like APACHE II and SOFA [5,6,7,8]. In these studies, the methods of measuring CD64 were not similar and comprised mean fluorescence intensity (MFI), percentage expression, CD64-index, and quantification of the receptor’s molecule numbers. A rapid increase of CD64 MFI was found in patients admitted in an intensive care unit before the development of infection; this was significantly higher than patients without infection [9]. In this study, we introduce for the first time the need to measure the early (i.e., the first 24 h) absolute CD64/CD15/CD45 neutrophil count. Measuring an absolute count can always provide more reproducible results since it provides information on the total cell population and not a relative expression of a receptor.
Although all the above-mentioned approaches of measurement of the expression of CD64 on neutrophils provide similar qualitative results, they have ended to standardized thresholds for universal application. For example, MFI measurements cannot be compared between different flow cytometry devices due to functional differentiations in manufacturers’ settings [9]. The use of an absolute count may surpass this limitation. The setting of our study cannot allow the investigation of the early absolute CD64/CD15/CD45 count for sepsis diagnosis since only patients with overt organ dysfunction were enrolled. Further investigation among patients admitted with suspicion of sepsis at the emergencies is probably most warranted.
The main question is the functional implication of this observation. It has been suggested that the MFI of CD64 of neutrophils is associated with the phagocytic activity of the neutrophils. More precisely, the MFI of CD64 neutrophils differed between sepsis survivors and non-survivors but not between non-survivors and healthy volunteers [1]. The MFI of neutrophilic CD64 was also decreased among non-survivors from septic shock. The authors considered that this could reflect a non-responsive state or a functional downregulation of the immune activity prior to the resolution of the infection [10]. It is well known that IL-8 is a potent chemokine priming neutrophil maturation and chemotaxis. Its increased circulatory levels among non-survivors with low CD64/CD15/CD45 count may reflect a reciprocal host response to further stimulate neutrophilic responses that eventually end up with neutrophilic exhaustion and immunosuppression. This may become a diagnostic sign of immunoparalysis guiding immunostimulation therapy.
The present study has four main limitations: (i) the relative low number of enrolled patients, (ii) the use of measurements in one central laboratory, (iii) the lack of proof of mechanism beneath the association of low CD64/CD15/CD45 count and high circulatory IL-8, and (iv) the inclusion of so severe patient population making questionable whether the finding of the early absolute CD64/CD15/CD45 count as an outcome prognosticator independent from severity scores coming from the forward step-wise logistic regression analysis is generalizable. It should, however, be underscored that the studied population was homogeneous since all enrolled patients were suffering from organ dysfunction and sepsis of Gram-negative origin.
The present study showed that an absolute CD64/CD15/CD45 neutrophil count below 2500/mm3 can be a useful prognosticator of sepsis outcome. Since this is probably an indicator of sepsis immunosuppression, it could be used to build classification models for immune intervention in sepsis.
Abbreviations
- APACHE:
-
Acute physiology and chronic health evaluation
- SOFA:
-
Sequential organ failure assessment
References
Danikas DD, Karakantza M, Theodorou GL, Sakellaropoulos GC, Gogos CA (2008) Prognostic value of phagocytic activity of neutrophils and monocytes in sepsis. Correlation to CD64 and CD14 antigen expression. Clin Exp Immunol 154:87–97
Gámez-Díaz LY, Enriquez LE, Matute JD, Velásquez S, Gómez ID, Toro F, Ospina S, Bedoya V, Arango CM, Valencia ML, De La Rosa G, Gómez CI, García A, Patiño PJ, Jaimes FA (2011) Diagnostic accuracy of HMGB-1, sTREM-1, and CD64 as markers of sepsis in patients recently admitted to the emergency department. Acad Emerg Med 18:807–815
Liu Y, Hou J, Li Q, Chen K, Wang S, Wang J (2016) Biomarkers for diagnosis of sepsis in patients with systemic inflammatory response syndrome: a systematic review and meta-analysis. SpringerPlus 5:2091
Giamarellos-Bourboulis E, Mylona V, Antonopoulou A, Tsangaris I, Koutelidakis I, Marioli A, Raftogiannis M, Kopterides P, Lymberopoulou K, Mouktaroudi M, Papageorgiou C, Papaziogas B, Georgopoulou AP, Tsaganos T, Papadomichelakis E, Gogos C, Ladas M, Savva A, Pelekanou A, Baziaka F, Koutoukas P, Kanni T, Spyridaki A, Maniatis N, Pelekanos N, Kotsaki A, Vaki I, Douzinas EE, Koratzanis G, Armaganidis A (2014) Effect of clarithromycin in patients with suspected gram-negative sepsis: results of a randomized controlled trial. J Antimicrob Chemother 69:1111–1118
Livaditi O, Kotanidou A, Psarra A, Dimopoulou I, Sotiropoulou C, Augustatou K, Papasteriades C, Armaganidis A, Roussos C, Orfanos SE, Douzinas EE (2006) Neutrophil CD64 expression and serum IL-8: sensitive early markers of severity and outcome in sepsis. Cytokine 36:283–290
Cid J, García-Pardo G, Aguinaco R, Sánchez R, Llorente A (2011) Neutrophil CD64: diagnostic accuracy and prognostic value in patients presenting to the emergency department. Eur J Clin Microbiol Infect Dis 30:845–852
Chen Q, Shi J, Fei A, Wang F, Pan S, Wang W (2014) Neutrophil CD64 expression is a predictor of mortality for patients in the intensive care unit. Int J Clin Exp Pathol 7:7806–7813
Papadimitriou-Olivgeris M, Lekka K, Zisimopoulos K, Spiliopoulou I, Logothetis D, Theodorou G, Anastassiou ED, Fligou F, Karakantza M, Marangos M (2015) Role of CD64 expression on neutrophils in the diagnosis of sepsis and the prediction of mortality in adult critically ill patients. Diagn Microbiol Infect Dis 82:234–239
Dimoula A, Pradier O, Kassengera Z, Dalcomune D, Turkan H, Vincent J (2014) Serial determinations of neutrophil CD64 expression for the diagnosis and monitoring of sepsis in critically ill patients. Clin Infect Dis 58:820–829
Fischer G, Schneider E, Moldawer LL, Karcher C, Barth E, Suger-Wiedeck H, Georgieff M, Weiss M (2001) CD64 surface expression on neutrophils is transiently upregulated in patients with septic shock. Intensive Care Med 27:1848–1852
Funding
The study was funded by the Hellenic Institute for the Study of Sepsis. The funders did not have any role in the study design, analysis, and interpretation of data and drafting the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
EJ Giamarellos-Bourboulis has received honoraria (paid to the University of Athens) from AbbVie USA, Abbott CH, Biotest Germany, Brahms GmbH, InflaRx GmbH, the Medicines Company; MSD Greece and XBiotech Inc. He has received independent educational grants from AbbVie, Abbott, Astellas Pharma, AxisShield, bioMérieux Inc., InflaRx GmbH, the Medicines Company and XBiotech Inc. He has received funding from the FrameWork 7 program HemoSpec and from the Horizon2020 Marie-Curie project European Sepsis Academy (granted to the National and Kapodistrian University of Athens).
The other authors declare no conflict of interest.
Ethical approval
This study was approved by the Ethics Committee of the ATTIKON University hospital (266/27-07-09).
Informed consent
Patients were enrolled after written informed provided by themselves or by first-degree relatives in case of patients unable to consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xini, A., Pistiki, A., Lada, M. et al. Association of the early absolute CD64-expressing neutrophil count and sepsis outcome. Eur J Clin Microbiol Infect Dis 38, 1123–1128 (2019). https://doi.org/10.1007/s10096-019-03507-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-019-03507-0