
Abstract
Introduction
Mild cognitive impairment (MCI) is common in Parkinson’s disease (PD), but the underlying pathological mechanism has not been fully understood. Voxel-based morphometry could be used to evaluate regional atrophy and its relationship with cognitive performances in early PD-MCI.
Patients and Methods
One hundred and six patients with PD were recruited from a larger cohort of patients, the Parkinson’s Disease Cognitive Impairment Study (PaCoS). Subject underwent a T1-3D MRI and a complete clinical and neuropsychological evaluation. Patients were divided into PD with normal cognition (PD-NC) and PD-MCI according to the MDS level II criteria–modified for PD-MCI. A subgroup of early patients with short disease duration (≤ 2 years) was also identified. VBM analysis between PD-NC and PD-MCI and between early PD-NC and PD-MCI was performed using two-sample t tests with whole-brain statistical threshold of p < 0.001 uncorrected in the entire PD group and p < 0.05 FWE inside ROIs, in the early PD.
Results
Forty patients were diagnosed with MCI and 66 were PD-NC. PD-MCI patients showed significant gray matter (GM) reduction in several brain regions, including frontal gyrus, precuneus, angular gyrus, temporal lobe, and cerebellum. Early PD-MCI showed reduction in GM density in superior frontal gyrus and cerebellum. Moreover, correlation analysis between neuropsychological performances and GM volume of early PD-MCI patients showed associations between performances of Raven and superior frontal gyrus volume, Stroop time and inferior frontal gyrus volume, accuracy of Barrage and volume of precuneus.
Conclusion
The detection of frontal and cerebellar atrophy, even at an early stage, could be used as an early marker of PD-related cognitive impairment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson’s disease (PD) is a common and complex neurodegenerative disorder clinically characterized by motor symptoms including tremor, rigidity, and bradykinesia and associated with numerous nonmotor symptoms, some of which precede motor dysfunction by more than a decade [1]. Cognitive impairment is one of the most common and relevant nonmotor symptoms involving a number of cognitive areas belonging to nonmemory and memory domains [2]. The full continuum of cognitive impairment can be observed in PD, ranging from subjective cognitive decline to mild cognitive impairment (MCI), and even PD dementia (PDD) [3]. The mean prevalence of PD-MCI has been estimated to be 26.7% [4], but it ranges from 20 to 69% depending on recruitment source, cognitive batteries used, and cutoff scores to define the impairment [5,6,7]. The underlying brain pathology leading to cognitive deficits in PD is still poorly understood. Interruption of the circuitry subserving the striatopallidothalamic network to the dorsolateral prefrontal cortex, due to striatal dopaminergic deficit, has been suggested to underlie the cognitive impairment occurring in PD [8]. Voxel-based morphometry (VBM) is a voxel-wise image processing method that allows investigating differences in brain anatomy typically starting from a T1-weighted volumetric MRI dataset. Several studies investigated and focused on neuroanatomical changes in patients with PD and cognitive impairment, showing widespread atrophy in frontal, parietal, and temporal lobes [9,10,11], but also subcortical structures [12, 13], and suggesting that the involvement of the frontal-limbic-temporal regions could be the main features of cognitive decline in PD [14]. Recently, authors described neuroanatomical findings considering also PD patients in early stage of disease [15,16,17,18,19].
The aim of this study was to investigate the different anatomical patterns of atrophy in a relatively large group of PD patients with and without MCI. Additionally, analysis was also restricted to PD patients with a short disease duration (≤ 2 years) in order to find a biological substratum underlying cognitive abnormalities and correlation with neuropsychological performances, occurring in the early stage of the disease. This study is part of the Parkinson’s Disease Cognitive Study (PaCoS), a multicenter study involving two centers located in Southern Italy (Sicily) aimed to evaluate frequency, clinical features, and biomarkers associated with MCI in a large hospital-based cohort of PD patients [20].
Methods
Subjects
The study subjects with PD belong to the PaCoS cohort, a large multicenter, prospective study regarding risk factors for PD-MCI and predictors for its evolution to PD dementia [20]. Patients affected by PD diagnosed according to the Brain Bank criteria [21], who underwent a comprehensive neuropsychological assessment and a routine MRI protocol acquired at the same time, were enrolled in the present study. They were evaluated at the Neurologic Unit of the University Hospital “Policlinico Vittorio Emanuele” in Catania, and the Memory and Parkinson’s Disease Center of the “Policlinico Paolo Giaccone” in Palermo, during a 4-year period (2014–2017). One hundred and six PD patients were recruited and a subgroup of early patients with a short disease duration (≤ 2 years, 62 patients) was also identified. Patients with morphological abnormalities and vascular and/or intracranial lesions as well as presence of an MRI pattern suggestive for normal pressure hydrocephalus were excluded.
Clinical and neuropsychological assessment
Patients underwent a comprehensive neurological examination performed by movement disorder specialists. Demographic, clinical, and pharmacological data were recorded. PD severity was evaluated with the Unified Parkinson Disease Rating Scale–Motor Examination (UPDRS-ME) and the Hoehn-Yahr (HY) scale [22, 23]. Cumulative daily dosage of dopaminergic drugs was converted using the levodopa equivalent dosage [24]. All patients were evaluated in practical “off” motor state after an overnight fast. Mild cognitive impairment was diagnosed according to the Movement Disorder Society (MDS) task force, level II criteria [25], slightly modified, because not all patients had been tested in the language domain. The following cognitive domains with at least two tests were assessed: episodic memory (Rey’s Auditory Verbal Learning Test and prose recall test with a delayed recall condition); attention (Stroop color-word test, Barrage and Trail Making Test part A); executive functioning (Verbal fluency letter test, Frontal Assessment Battery, and Colored Raven’s Progressive Matrices); visuospatial functioning (clock drawing test and copy of figures). Neuropsychological performance was considered as impaired when subjects scored two standard deviations below normality cutoff values. All PD subjects underwent neuropsychological assessment after a 12-h washout of hypnotic sedatives or other medications that may affect cognitive performances. For the current analysis, subjects were divided into PD with normal cognition (PD-NC) and PD with MCI (PD-MCI). Additionally, MCI subtypes were identified as follows based on the number of altered cognitive domains and the involvement of the memory domain: amnestic MCI single domain (aMCIsd), nonamnestic MCI single domain (naMCIsd), amnestic MCI multidomain (aMCImd), and nonamnestic MCI multiple domain (naMCImd) [25].
MRI data acquisition
Brain MRI was performed according to our routine protocol with a 1.5-T unit (Signa HDxt, GE Medical Systems, Milwaukee, WI, USA), the same scan model for the two participating centers. A 3D T1-weighted high-resolution spoiled gradient echo (SPGR) sequence with a 1.2-mm slice thickness and an isotropic in-plane resolution of 0.98 mm was acquired with the following parameters: repetition time 14.8 ms, echo time 6.4 ms, flip angle 25°, 115 slices, matrix size 256 × 256, and a field of view of 24 cm. Additionally, all subjects underwent a T2-weighted and FLAIR images in order to exclude morphological abnormalities, intracranial lesions, or the presence of an MRI pattern suggestive of normal pressure hydrocephalus (considering the identification of a “DESH” pattern and Evans’ index > 0.3). Patients with high vascular lesion load were excluded according to the visual rating scale proposed by Wahlund and coll [26], considering the presence of hemispheric white matter confluent lesions or more than one focal lesion in basal ganglia.
Voxel-based morphometry
We performed a voxel-based analysis investigating GM volume changes. Data were processed using the SPM8 software (http://www.fil.ion.ucl.ac.uk/spm), where we applied VBM implemented in the VBM8 toolbox (http://dbm.neuro.uni-jena.de/vbm.html) and incorporated the DARTEL toolbox that was used to obtain a high-dimensional image registration and normalization. Images were bias-corrected, tissue classified, and images were registered using linear (12-parameter affine) and nonlinear transformations, within a unified model. Subsequently, the warped GM segments were affine transformed into MNI-152 space and were scaled by the Jacobian determinants of the deformations (modulation). Finally, the modulated volumes were smoothed with a Gaussian kernel of 8-mm full width at half maximum (FWHM).
Statistical analysis
Data were analyzed using STATA 12.1 software packages (StataCorp, College Station, TX, USA). Data cleaning was performed before the data analysis considering both range and consistence checks. Quantitative variables were described using mean and standard deviation. Differences between means and proportions were evaluated by the t test and the chi-squared test respectively. In case of not a normal distribution, appropriate nonparametric tests were performed.
Image analysis
Two-sample t tests were used to compare the GM density between PD-NC and PD-MCI, and between early PD-NC and early PD-MCI. The statistical threshold was set at p < 0.001 uncorrected for multiple comparisons, at whole-brain level, in order to avoid a priori assumption. A p < 0.05 with a familywise error (FWE) correction inside ROIs was used for VBM analysis in early PD patients. We considered as ROIs the regions that showed the most significant GM changes in the comparisons between PD-NC and PD-MCI. Age, education, and total intracranial volume (ICV) were included in the model as covariates of no-interest. Moreover, to evaluate a possible association between GM volume changes and neuropsychological data of early PD-MCI, a correlation analysis using the multiple regression function of SPM8 was performed. Whole-brain correlation analyses were performed employing a statistical threshold of p < 0.05 FWE at cluster level.
Results
Demographic and clinical characteristics
One hundred six nondemented patients from the PaCoS cohort were selected in the present study, among those who had a complete assessment including MRI and neuropsychological evaluation. Of 106 enrolled patients, 40 patients (37.7%) were diagnosed with MCI and 66 (62.3%) were PD-NC; among PD-MCI patients, the most common subtype was aMCImd (42.5%), followed by naMCImd (35%) and naMCIsd (17.5%), while aMCIsd was found in only 2 patients (5%). Table 1 shows the demographics and clinical characteristics of the PD groups. No significant differences were found, except for PD-MCI who had a significantly lower education and took more antipsychotic drugs and less antidepressant treatment in comparison to PD-NC. Thirty-seven PD-NC and 25 PD-MCI with short disease duration (≤ 2 years) were identified. There were no significant differences for the main clinical features between the early PD groups. Supplementary Table 1 shows neuropsychological performances of early PD patients.
GM abnormalities in patients with PD without and with MCI
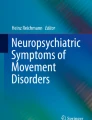
There was no difference in total GM, WM, and CSF between PD-NC and PD-MCI. VBM analysis between PD-NC and PD-MCI showed no significant differences using a whole-brain threshold of p < 0.05 FWE; on the other hand, there were significant differences in several brain regions at p < 0.001, uncorrected for multiple comparisons (Table 2). Patients with PD-MCI showed reduction in GM density in left superior frontal gyrus, left precuneus, right superior parietal lobe (angular gyrus), bilateral temporal lobe, left cerebellum (lobules IV–V), and right cerebellum (lobule III) (Fig. 1).

Reduced GM volume in PD-MCI compared with PD-NC patients. Significant clusters are shown. a Superior frontal gyrus, b angular gyrus, c precuneus, d temporal lobe, e cerebellum. PD-NC Parkinson’s disease with normal cognition, PD-MCI Parkinson’s disease with mild cognitive impairment, GM gray matter
Interestingly, considering as ROIs the regions that showed the most significant GM changes in the comparisons between PD-NC and PD-MCI, VBM analysis between early PD-NC and early PD-MCI showed GM density decrease only in three clusters involving superior frontal gyrus (medial) and cerebellum (left lobules IV–V and right lobule III) (p < 0.05 FWE, inside ROIs) (Table 2 and Fig. 2). No significant findings were detected considering voxels outside the selected ROIs.

Significant cluster of GM atrophy in early PD-MCI compared with early PD-NC patients. a Superior frontal gyrus (medial), b cerebellum (left lobules IV–V), c cerebellum (right lobule III). PD-NC Parkinson’s disease with normal cognition, PD-MCI Parkinson’s disease with mild cognitive impairment, GM gray matter
Correlation analysis
Regression analysis performed between neuropsychological performances and GM volume of PD-MCI with short disease duration showed the involvement of salient brain areas related to specific cognitive domains (Table 3). Specifically, performances obtained on the Raven’s Colored Progressive Matrices were associated with volume of superior frontal gyrus (p < 0.05 FWE, r = 0.74); Stroop performances (time) were negatively correlated with volume of inferior frontal gyrus (p < 0.05 FWE, r = − 0.86). Finally, performances related to the Barrage accuracy were negatively associated with volume of precuneus (p < 0.05 FWE r = − 0.76) (Fig. 3).

Correlation analysis between neuropsychological performances of early PD patients and global maxima of GM volume clusters. The regression line and r value are shown. GM gray matter
Discussion
In this study, we examined GM volume changes in a relatively large group of PD patients with and without MCI using a whole-brain structural MRI approach. Although at an uncorrected threshold, patients with PD-MCI showed GM atrophy in different brain regions, involving the frontal, temporal, and parietal lobes and cerebellar lobules. More interestingly, a subgroup of PD-MCI with short disease duration showed GM density decrease in frontal lobe, and cerebellum considering correction for multiple comparisons.
Structural MRI techniques have been previously applied to evaluate cognitive impairment in PD patients. Different studies showed heterogeneous patterns of GM atrophy correlated with cognitive functions suggesting a gradient of atrophy from normal cognition to PDD [27,28,29]. In line with our findings, MCI in PD seemed to be related to widespread GM reduction involving the temporal, parietal, and frontal areas [9, 11,12,13, 16, 28]. Noh and colleagues [30] showed a significant decreased GM volume in the precuneus, frontal and temporal cortices, and cingulate gyrus in PD-MCI compared with PD-NC, also finding a correlation with cognitive status and particularly with verbal memory impairment. The authors suggest that progression of cognitive impairment could reflect the progression of cortical atrophy from posterior to anterior areas [30]. The involvement of frontal areas has been showed by other studies, underlying the importance of frontoparietal networks in working memory and executive function [9, 31]. On the other hand, Segura and colleagues [10] showed significant cortical thinning in right precuneus in PD-MCI, highlighting the presence of a posterior atrophy pattern involving also visuospatial and visuoperceptual domains.
Resting-state functional MRI (rs-fMRI) studies showed an abnormal connectivity in default-mode network (including temporoparietal and cingulate cortices) and frontoparietal network in absence of structural changes in PD-MCI compared with PD-NC, suggesting a functional disconnection underlying the cognitive impairment; these authors also suggested that functional abnormalities could anticipate the presence of detectable structural changes [32, 33]. Furthermore, Anderkova and colleagues [34] showed decreased connectivity in the precuneus which negatively correlated with memory performance, suggesting the role of a posterior cortical hub of this brain region tightly interconnected with the hippocampus and striatum Recently, Chen and colleagues [13] used the combination of rs-fMRI and VBM techniques, showing functional and structural differences in the prefrontal cortex, temporal gyrus, and medial temporal lobe, as well as the striatum and cerebellum areas and suggesting that multimodal approach could be useful for detecting subtle changes in PD-MCI patients.
An interesting finding of our study is the detection of a significant frontal GM density reduction also in a group of PD-MCI patients with short disease duration. Previous studies examined brain morphometry in early-stage PD-MCI patients. Pereira and colleagues [16] assessed cortical thickness in a cohort of drug-naive patients with early (≤ 1 year) PD with and without MCI showing a widespread pattern of cortical atrophy associated with MCI; they suggested that the neurodegenerative process could be already present at the time of diagnosis of MCI. Other studies showed regional atrophy in frontotemporoparietal areas in de novo PD patients [15, 17, 18, 30], suggesting that even in the early stages of PD, there is evidence of cortical brain atrophy.
Moreover, we showed the involvement of the cerebellum in PD-MCI at earlier stage. Cerebellar structures have been mainly showed in relation to working memory tasks [35], but it may contribute also to other cognitive functions [36]. Indeed, in patients with PD, a significant impairment in attention and visuospatial functions together with the presence of freezing of gait has been associated with atrophy of the cerebellum [37]. Additionally, a recent fMRI study showed that the cerebellum might play a role in dual-tasking deficiency evidenced in PD, suggesting an abnormal connectivity of the cerebellum itself with cognitive areas, including precuneus and prefrontal cortex [38].
Furthermore, we identified significant associations between neuropsychological performance of PD-MCI with short disease duration and peculiar areas of GM atrophy linked with specific cognitive domains. In particular, the Raven’s Colored Progressive Matrices [39], which explores executive functioning, was associated with atrophy in superior frontal gyrus. Pereira and colleagues [40] found a disruption in network connectivity in PD-MCI, mainly in the frontal areas, thus suggesting that the disconnection of these areas from others could be associated with the dysexecutive syndrome typically described in PD patients with cognitive decline.
GM reduction of the inferior frontal gyrus was significantly associated with performances in the Stroop test, evaluating the ability to inhibit cognitive interference [41]. It is well known the role of inferior frontal cortex in inhibition response [42] and similar results were reported by previous studies, which showed a significant correlation between attention and frontotemporal areas in PD-MCI [9], even at an early stage of the disease and in drug-naive patients [16].
Finally, the accuracy in the Barrage test, assessing attention and visuospatial domain, was negatively correlated with GM density in the precuneus. The involvement of the latter area in visuospatial functioning has been shown in different rs-fMRI connectivity studies showing that the dorsal precuneus had greater connectivity with occipital and posterior parietal cortices and was also connected with areas involved in attention and visuospatial functioning [43].
In conclusion, our findings suggest that the neurodegenerative process leading to atrophy of peculiar cortical areas underlies the cognitive abnormalities in PD-MCI, and these changes are present even at very early stages of the disease.
References
Kalia LV, Lang AE (2016) Parkinson disease in 2015: evolving basic, pathological and clinical concepts in PD. Nat Rev Neurol 12(2):65–66
Aarsland D, Kurz MW (2010) The epidemiology of dementia associated with Parkinson disease. J Neurol Sci 289(1–2):18–22
Baschi R, Nicoletti A, Restivo V, Recca D, Zappia M, Monastero R (2018) Frequency and correlates of subjective memory complaints in Parkinson’s disease with and without mild cognitive impairment: data from the Parkinson’s disease cognitive impairment study. J Alzheimer’s dis. J Alzheimers Dis 63(3):1015–1024
Litvan I, Aarsland D, Adler CH et al (2011) MDS task force on mild cognitive impairment in Parkinson’s disease: critical review of PD-MCI. Mov Disord 15(10):1814–1824
Pedersen KF, Larsen JP, Tysnes OB, Alves G (2013) Prognosis of mild cognitive impairment in early Parkinson disease: the Norwegian ParkWest study. JAMA Neurol 70(5):580–586
Yarnall AJ, Breen DP, Duncan GW, ICICLE-PD Study Group (2014) Characterizing mild cognitive impairment in incident Parkinson disease: the ICICLE-PD study. Neurology 82(4):308–316
Domellöf ME, Ekman U, Forsgren L, Elgh E (2015) Cognitive function in the early phase of Parkinson’s disease, a five-year follow-up. Acta Neurol Scand 132(2):79–88
Emre M (2003) What causes mental dysfunction in Parkinson’s disease? Mov Disord 8(Suppl 6):S63–S71
Mak E, Zhou J, Tan LC et al (2014) Cognitive deficits in mild Parkinson’s disease are associated with distinct areas of grey matter atrophy. J Neurol Neurosurg Psychiatry 85(5):576–580
Segura B, Baggio HC, Marti MJ, Valldeoriola F, Compta Y, Garcia-Diaz AI, Vendrell P, Bargallo N, Tolosa E, Junque C (2014) Cortical thinning associated with mild cognitive impairment in Parkinson’s disease. Mov Disord 29(12):1495–1503
Zhang J, Zhang YT, Hu WD, Li L, Liu GY, Bai YP (2015) Gray matter atrophy in patients with Parkinson’s disease and those with mild cognitive impairment: a voxel-based morphometry study. Int J Clin Exp Med 8(9):15383–15392
Lee JE, Cho KH, Song SK, Kim HJ, Lee HS, Sohn YH, Lee PH (2014) Exploratory analysis of neuropsychological and neuroanatomical correlates of progressive mild cognitive impairment in Parkinson’s disease. J Neurol Neurosurg Psychiatry 85(1):7–16
Chen B, Wang S, Sun W, Shang X, Liu H, Liu G, Gao J, Fan G (2017) Functional and structural changes in gray matter of Parkinson’s disease patients with mild cognitive impairment. Eur J Radiol 93:16–23
Xu Y, Yang J, Hu X, Shang H (2016) Voxel-based meta-analysis of gray matter volume reductions associated with cognitive impairment in Parkinson’s disease. J Neurol 263(6):1178–1187
Danti S, Toschi N, Diciotti S, Tessa C, Poletti M, del Dotto P, Lucetti C (2015) Cortical thickness in de novo patients with Parkinson disease and mild cognitive impairment with consideration of clinical phenotype and motor laterality. Eur J Neurol 22(12):1564–1572
Pereira JB, Svenningson P, Weintraub D et al (2014) Initial cognitive decline is associated with cortical thinning in early Parkinson disease. Neurology 82(22):2017–2025
Uribe C, Segura B, Baggio HC, Abos A, Garcia-Diaz AI, Campabadal A, Marti MJ, Valldeoriola F, Compta Y, Tolosa E, Junque C (2018) Cortical atrophy patterns in early Parkinson’s disease patients using hierarchical cluster analysis. Parkinsonism Relat Disord 50:3–9
Jia X, Wang Z, Yang T, Li Y, Gao S, Wu G, Jiang T, Liang P (2019) Entorhinal cortex atrophy in early, drug-naive Parkinson’s disease with mild cognitive impairment. Aging Dis 10(6):1221–1232
Klein JC, Rolinski M, Griffanti L, Szewczyk-Krolikowski K, Baig F, Ruffmann C, Groves AR, Menke RAL, Hu MT, Mackay C (2018) Cortical structural involvement and cognitive dysfunction in early Parkinson’s disease. NMR Biomed 31(4):e3900
Monastero R, Cicero CE, Baschi R, Davì M, Luca A, Restivo V, Zangara C, Fierro B, Zappia M, Nicoletti A (2018) Mild cognitive impairment in Parkinson’s disease: the Parkinson’s Disease Cognitive Study (PACOS). J Neurol 265(5):1050–1058
Gibb WR, Lees AJ (1989) The significance of the Lewy body in the diagnosis of idiopathic Parkinson’s disease. Neuropathol Appl Neurobiol 15:27–44
Fahn, S., Elton, R. and Members of the UPDRS Development Committee. The Unified Parkinson’s Disease Rating Scale. In: Fahn, S., Marsden, C.D., Calne, D.B. and Goldstein, M., Eds., 1987 Recent Developments in Parkinson’s Disease, Vol. 2, McMellam Health Care Information, Florham Park, 153–163
Hoehn MM, Yahr MD (1967) Parkinsonism: onset, progression and mortality. Neurology 17(5):427–442
Tomlinson CL, Stowe R, Patel S et al (2010) Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord 2010 25(15):2649–2653
Litvan I, Goldman JC, Tröster AI et al (2012) Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force Guidelines. Mov Disord 27(3):349–356
Wahlund LO, Barkhof F, Fazekas F, Bronge L, Augustin M, Sjögren M, Wallin A, Ader H, Leys D, Pantoni L, Pasquier F, Erkinjuntti T, Scheltens P, European Task Force on Age-Related White Matter Changes (2001) A new rating scale for age-related white matter changes applicable to MRI and CT. Stroke 32(6):1318–1322
Song SK, Lee JE, Park HJ, Sohn YH, Lee JD, Lee PH (2011) The pattern of cortical atrophy in patients with Parkinson’s disease according to cognitive status. Mov Disord 26(2):289–296
Melzer TR, Watts R, MacAskill MR et al (2012) Grey matter atrophy in cognitively impaired Parkinson’s disease. J Neurol Neurosurg Psychiatry 83(2):188–194
Pagonabarraga J, Corcuera-Solano I, Vives-Gilabert Y, Llebaria G, García-Sánchez C, Pascual-Sedano B, Delfino M, Kulisevsky J, Gómez-Ansón B (2013) Pattern of regional cortical thinning associated with cognitive deterioration in Parkinson’s disease. PLoS One 8(1):e54980
Noh SW, Han YH, Mun CW, Chung EJ, Kim EG, Ji KH, Seo JH, Kim SJ (2014) Analysis among cognitive profiles and gray matter volume in newly diagnosed Parkinson’s disease with mild cognitive impairment. J Neurol Sci 347(1–2):210–213
Biundo R, Calabrese M, Weis L, Facchini S, Ricchieri G, Gallo P, Antonini A (2013) Anatomical correlates of cognitive functions in early Parkinson’s disease patients. PLoS One 8(5):e64222
Amboni M, Tessitore A, Esposito F, Santangelo G, Picillo M, Vitale C, Giordano A, Erro R, de Micco R, Corbo D, Tedeschi G, Barone P (2015) Resting-state functional connectivity associated with mild cognitive impairment in Parkinson’s disease. J Neurol 262(2):425–434
Baggio HC, Segura B, Sala-Llonch R, Marti MJ, Valldeoriola F, Compta Y, Tolosa E, Junqué C (2015) Cognitive impairment and resting-state network connectivity in Parkinson’s disease. Hum Brain Mapp 36(1):199–212
Anderkova L, Barton M, Rektorova I (2017) Striato-cortical connections in Parkinson’s and Alzheimer’s disease: relation to cognition. Mov Disord 32(6):917–922
Nee DE, Brown JW, Askren MK, Berman MG, Demiralp E, Krawitz A, Jonides J (2013) A meta-analysis of executive components of working memory. Cereb Cortex 23(2):264–282
Stoodley CJ, Schmahmann JD (2009) Functional topography in the human cerebellum: a meta-analysis of neuroimaging studies. Neuroimage 44(2):489–501
Jha M, Jhunjhunwala K, Sankara B et al (2015) Neuropsychological and imaging profile of patients with Parkinson’s disease and freezing of gait. Parkinsonism Relat Disord 21(10):1184–1190
Gao L, Zhang J, Hou Y et al (2017) The cerebellum in dual-task performance in Parkinson’s disease. Sci rep 30:7–45662
Carlesimo GA, Caltagirone C, Gainotti G (1996) The mental deterioration battery: normative data, diagnostic reliability and qualitative analyses of cognitive impairment. The group for the standardization of the mental deterioration battery. Eur Neurol 36(6):378–384
Pereira JB, Aarsland D, Ginestet CE, Lebedev AV, Wahlund LO, Simmons A, Volpe G, Westman E (2015) Aberrant cerebral network topology and mild cognitive impairment in early Parkinson’s disease. Hum Brain Mapp 36(8):2980–2995
Uttl B, Graf P (1997) Color-Word Stroop test performance across the adult life span. J Clin Exp Neuropsychol 19(3):405–420
Aron AR, Fletcher PC, Bullmore ET et al (2003). Stop-signal inhibition disrupted by damage to right inferior frontal gyrus in humans. Nat Neurosci 6(2):115-116. Erratum in: Nat Neurosci 6(12):1329
Zhang S, Li CS (2012) Functional connectivity mapping of the human precuneus by resting state fMRI. Neuroimage 59(4):3548–3562
Funding
This research was funded by the Department of Medical and Surgical Sciences and Advanced Technologies “G.F. Ingrassia,” University of Catania, Italy (Piano Triennale di Sviluppo delle Attività di Ricerca Scientifica del Dipartimento 2016-18).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOC 35 kb)
Rights and permissions
About this article

Cite this article
Donzuso, G., Monastero, R., Cicero, C.E. et al. Neuroanatomical changes in early Parkinson’s disease with mild cognitive impairment: a VBM study; the Parkinson’s Disease Cognitive Impairment Study (PaCoS). Neurol Sci 42, 3723–3731 (2021). https://doi.org/10.1007/s10072-020-05034-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-020-05034-9