
Abstract
To investigate the correlations of five angiogenesis-related miRNA (miR-126, miR-130a, miR-222, miR-218, and miR-185) expression levels with risk, severity, and inflammatory cytokines levels in acute ischemic stroke (AIS) patients. A total of 148 AIS patients and 148 age- and gender-matched controls were consecutively enrolled. Blood samples were collected from AIS patients and controls, and plasma was separated for miRNAs and cytokine level detection. Plasma levels of miRNAs were evaluated by real-time qPCR method, and inflammatory cytokine levels were detected using an enzyme-linked immunosorbent assay (ELISA). Plasma miR-126 and miR-130a expression levels in AIS patients were lower than those of controls, while the levels of miR-222, miR-218, and miR-185 were elevated in AIS patients compared with controls. After pooling the five miRNA expression levels together, the area under the curve (AUC) for predicting AIS risk was 0.840 (95% CI 0.795–0.885) with a sensitivity of 83.8% and a specificity of 69.6% at the best cut-off point. Plasma miR-126 (r = − 0.402, P < 0.001) and miR-130a (r = − 0.161, P = 0.050) levels were negatively correlated with NIHSS scores, while plasma miR-218 level was positively correlated with NIHSS scores (r = 0.471, P < 0.001). Most importantly, plasma miR-126 expression was negatively correlated with TNF-α (r = − 0.168, P = 0.041), IL-1β (r = − 0.246, P = 0.003), and IL-6 (r = − 0.147, P = 0.035) levels, while miR-130a expression was negatively correlated with TNF-α (r = − 0.287, P < 0.001), IL-1β (r = − 0.168, P = 0.041), and IL-6 (r = − 0.239, P = 0.003) expression levels and positively associated with IL-10 level (r = 0.261, P = 0.001). Circulating miR-126 and miR-130a levels correlate with lower disease risk, decreased disease severity, and reduced inflammatory cytokine levels in AIS patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stroke is the second leading cause of death and the third leading cause of disability worldwide [1]. Acute ischemic stroke (AIS), the most common type of stroke that accounting for approximately 60 to 80% of all strokes, is a neurological deficit caused by multiple types of cerebral artery blood flow disruption, focal cerebral ischemia, and hypoxia necrosis [2, 3]. Although enhanced computed tomography (CT) and magnetic resonance imaging (MRI) have been used to assist in the diagnosis of AIS in clinical practice, image interpretations can be inconsistent and the availability of such expensive machinery is limited, which often delays the diagnosis [4,5,6]. Therefore, understanding the molecular biology of ischemic stroke and identifying novel biomarkers with high feasibility for evaluating disease risk and monitoring disease progression are crucial to improve AIS patients’ outcomes.
MicroRNAs (miRNAs) are a class of small noncoding RNAs that interact with their target coding messenger RNAs to repress translation or degrade messenger RNA transcripts [7]. Numerous studies have demonstrated that miRNAs play crucial roles in various physiological processes and the pathogeneses of several diseases including cardiovascular and cerebrovascular diseases [8,9,10]. For example, miR-503 overexpression promotes angiotensin II-induced cardiac fibrosis in mice [11], while miRNA-34a-5p expression negatively correlates with AIS severity [12]. Our previous study identified 11 angiogenisis-related, differentially expressed miRNAs (DEMs) in an exploratory sample. The predictive values of the plasma expression levels of these 11 DEMs for risk and their correlations with severity of AIS were evaluated in a validating study that showed that miR-126, miR-130a, miR-222, miR-218, and miR-185 were independent predictive factors for AIS risk. This study also showed that pooling these five miRNAs’ plasma expression levels yields a valuable diagnostic potential for AIS. In addition, miR-126, miR-378, miR-101, miR-222, miR-218, and miR-206 were associated with NIHSS score [13]. However, the underlying mechanism of how these miRNAs participate in the development and progression of AIS is still unclear. AIS is a neurological deficit characterized by high intracranial vascular inflammation; we thus hypothesized that these miRNAs might be involved in AIS pathogenesis via inflammation regulation.
This study aimed to investigate the correlations of these five miRNA (miR-126, miR-130a, miR-222, miR-218, and miR-185) expression levels with disease risk, disease severity with risk, disease severity, and inflammatory cytokine levels in AIS patients.
Methods
Study design
In our previous study, we observed that circulating miR-126, miR-130a, miR-222, miR-218, and miR-185 levels could be served as promising independent biomarkers for risk of AIS. In our present study, we validated our previous findings in a larger sample size and further investigated the associations of those miRNA (miR-126, miR-130a, miR-222, miR-218, and miR-185) expression levels with disease severity as assessed by the National Institutes Health Stroke Scale (NIHSS) and by levels of inflammatory cytokines in AIS patients.
Patients
A total of 148 AIS patients admitted to the Department of Emergency in Cangzhou Central Hospital from Oct 2013 to Jun 2017 were consecutively enrolled in the present study. The inclusion criteria were as follows: (1) diagnosed as AIS according to patient’s history, laboratory and neurological examination, computed tomography (CT) scan, magnetic resonance imaging (MRI), and/or magnetic resonance angiography (MRA) within 24 h following the onset of symptoms; and (2) age above 18 years. Patients were excluded if they had uncontrollable infection, renal or hepatic failure, hematological malignancies or solid tumors, or had undergone immunosuppressive therapy or thrombolytic therapy. During the same time frame, 148 age- and gender-matched controls with vascular risk factors in Cangzhou Central hospital were enrolled. Controls with history of stroke, myocardial infarction or peripheral vascular disease, severe infection, renal or hepatic dysfunction, non-specific dizziness, or non-organic headaches were excluded from this study.
Ethics
This study was approved by the Ethics Committee of Cangzhou Central Hospital, and all participants or direct family members provided signed informed consents.
Samples
Within 24 h following onset of symptoms, 5-ml blood samples were collected from AIS patients, which was centrifuged at 3000 rpm for 20 min at room temperature. A centrifugation of 12,000 rpm for 10 min at 4 °C was then performed to separate plasma, which was subsequently stored at − 80 °C for miRNA expression assessment and the detections of inflammatory cytokines. In addition, blood samples were also collected from controls when they were enrolled in this study, and the plasma was separated using the same method described above for miRNA assessments.
MiRNAs detection
Total RNA was extracted from plasma using TRIzol solution (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s protocol. Subsequently, RNA was reverse transcribed by transcript first-strand cDNA synthesis SuperMix (TransGen Biotech, Beijing, China). Real-time qPCR was performed using the SYBR Premix Ex Taq kit (Takara, Dalian, China) to assess the relative quantity of miRNAs, and U6 was used as internal reference for normalization of miRNA relative quantity. Then, the results were calculated using the 2−ΔΔt formula. Primer sequence information is shown in Table 1.
Inflammatory cytokine detection
Plasma levels of tumor necrosis factor alpha (TNF-α), IL (interleukin)-1β, IL-6, IL-8, and IL-10 were detected by enzyme-linked immunosorbent assay (ELISA) using commercial ELISA kits (Abcam, USA) according to the manufacturer’s instructions. Results were read by microplate reader at 450 nm (Biotek, USA).
Statistics
Statistical analysis was performed using SPSS 21.0 (SPSS, USA) and GraphPad Prism software 6.01 (GraphPad, USA). Data were mainly presented as mean ± standard deviation, median (1/4–3/4 quartiles) or count (percentage). Comparison between two groups was determined by t test, Wilcoxon rank sum test, or chi-square test. Receiver operating characteristic (ROC) curve analysis was performed to determine whether miRNAs could be used to distinguish AIS patients from controls. Spearman test was used to assess the associations of the expression levels of the five miRNAs with NIHSS scores and inflammatory cytokine levels. P < 0.05 was considered significant.
Results
Characteristics of AIS patients and controls
As presented in Table 2, no parameter differences between AIS patients and controls were discovered (all P > 0.05). In brief, 148 AIS patients with mean age of 61.5 ± 9.2 years and 148 controls with mean age of 59.8 ± 9.6 years were enrolled in this study. There were 92 male (62.2%) AIS patients and 84 male (56.8%) controls. The mean BMI values in AIS patients and controls were 23.1 ± 2.6 and 22.8 ± 2.8 kg/m2, respectively. Additionally, hypertension was found in 118 (79.7%) AIS patients and 112 (75.7%) controls, and the numbers of patients with hyperlipidemia in AIS patients and controls were 77 (52.0%) and 68 (45.9%), respectively. The other detailed clinical characteristics of AIS patients and controls are presented in Table 2.
Comparison of miR-126, miR-130a, miR-222, miR-218, and miR-185 plasma expression levels between AIS patients and controls
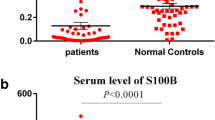
As presented in Fig. 1, miR-126 (Fig. 1a, P < 0.001) and miR-130a expression levels (Fig. 1b, P < 0.001) in AIS patients were lower than those in controls, while the levels of miR-222 (Fig. 1c, P < 0.001), miR-218 (Fig. 1d, P < 0.001), and miR-185 (Fig. 1e, P < 0.001) were elevated in AIS patients compared with controls.

Relative expression levels of miR-126, miR-130a, miR-222, miR-218, and miR-185 in AIS patients and controls. Relative expression levels of miR-126 (a) and miR-130a (b) were reduced in AIS patients compared with controls; however, the miR-222 (c), miR-218 (d), and miR-185 (e) relative expression levels were increased in CAD patients compared with controls. Comparison between the two groups was determined by Wilcoxon rank sum test. P < 0.05 was considered significant. AIS acute ischemic stroke
Predictive value of miR-126, miR-130a, miR-222, miR-218, and miR-185 plasma expression levels for AIS risk
ROC analyses were conducted to evaluate the predictive value of the five miRNAs for risk of AIS. The area under the curve (AUC) of miR-126, miR-130a, miR-222, miR-218, and miR-185 for predicting AIS risk were 0.665 (95% CI 0.602–0.728), 0.619 (95% CI 0.556–0.683), 0.629 (95% CI 0.566–0.692), 0.685 (95% CI 0.625–0.746), and 0.633 (95% CI 0.570–0.696), respectively. When pooling the five miRNA expression levels together, the AUC was 0.840 (95% CI 0.795–0.885) with sensitivity of 83.8% and specificity of 69.6% at best cut-off point, which was defined as the point with the maximum value of specificity plus sensitivity (Fig. 2). These findings suggest that the measurement of the five pooled miRNAs’ expression levels could be served as a promising biomarker for AIS risk.

The predictive values of miR-126, miR-130a, miR-222, miR-218, and miR-185 expression levels for AIS risk. ROC curve showed that pooling the miR-126, miR-130a, miR-222, miR-218, and miR-185 expression levels yielded a higher AUC than the value of each individual miRNA. The analysis was performed by ROC curve. ROC receiver operating characteristic, AUC area under curve
Correlations between miR-126, miR-130a, miR-222, miR-218, and miR-185 plasma expression levels and NIHSS score
The plasma levels of miR-126 (r = − 0.402, P < 0.001) (Fig. 3a) and miR-130a (r = − 0.161, P = 0.050) (Fig. 3b) were negatively correlated with NIHSS scores, while miR-218 expression (r = 0.471, P < 0.001) (Fig. 3d) was positively correlated with NIHSS scores. However, no correlation between miR-222 (r = − 0.062, P = 0.454) (Fig. 3c) or miR-185 (r = 0.129, P = 0.117) (Fig. 3e) expression levels and NIHSS scores was found (Fig. 3).

Correlations of plasma miR-126, miR-130a, miR-222, miR-218, and miR-185 expression levels with NIHSS score. The levels of miR-126 (a) and miR-130a (b) were both negatively correlated with NINHSS score, while miR-218 (d) expression was positively correlated with NIHSS score, but miR-222 (c) and miR-185 (e) were not correlated with NIHSS score. The Spearman test was used to assess the correlations of five miRNA levels with NIHSS score. P < 0.05 was considered significant. NIHSS National Institutes Health Stroke Scale
Correlations between miR-126, miR-130a, miR-222, miR-218, and miR-185 plasma expression levels and inflammatory cytokine levels
As presented in Fig. 4, miR-126 expression was negatively correlated with TNF-α (r = − 0.168, P = 0.041) (Fig. 4a), IL-1β (r = − 0.246, P = 0.003) (Fig. 4b), and IL-6 levels (r = − 0.147, P = 0.035) (Fig. 4c), but no correlation of miR-126 expression with IL-8 expression (r = − 0.140, P = 0.089) (Fig. 4d) or IL-10 expression (r = 0.149, P = 0.071) (Fig. 4e) was found. miR-130a expression was negatively correlated with TNF-α (r = − 0.287, P < 0.001) (Fig. 4f), IL-1β (r = − 0.168, P = 0.041) (Fig. 4g) and IL-6 (r = − 0.239, P = 0.003) (Fig. 4h) levels, but was positively correlated with IL-10 expression (r = 0.261, P = 0.001) (Fig. 4j). There was no correlation between miR-130a and IL-8 level (r = − 0.102, P = 0.261) (Fig. 4i).

Correlations of plasma miR-126 and miR-130a relative expressions with inflammatory cytokine levels. MiR-126 relative expression was negatively correlated with the levels of TNF-α (a), IL-1β (b), and IL-6 (c), but no correlation of miR-126 level with IL-8 (d) or IL-10 (e) was found. Furthermore, miR-130a expression level was negatively correlated with TNF-α (f), IL-1β (g), and IL-6 (h) levels, but was positively correlated with IL-10 (j) expression. No correlation of miR-130a expression with IL-8 (i) level was found. The Spearman test was used to assess the correlations of inflammatory cytokines with miRNA levels. P < 0.05 was considered significant. TNF-α tumor necrosis factor alpha, IL-1β interleukin-1β, IL-6 interleukin 6, IL-8 interleukin 8, IL-10 interleukin 10
As for miR-222, miR-218, and miR-185 expression levels, as shown in Supplementary Fig. S1, their expression levels were not correlated with any inflammatory cytokine levels, including TNF-α, IL-1β, IL-6, IL-8, and IL-10 (all P > 0.05) (Supplementary Fig. S1 A-O).
Logistic regression model analysis of miR-126, miR-130a, miR-222, miR-218, and miR-185 expression levels in predicting AIS risk
As listed in Supplementary Table S1, the univariate logistic regression illustrated that low expression levels of miR-126 (P < 0.001) and miR-130a (P < 0.001), and high expression levels of miR-222 (P < 0.001), miR-218 (P < 0.001), and miR-185 (P < 0.001), were associated with increased AIS risk. Additionally, multivariate logistic regression showed that low expression levels of miR-126 (P < 0.001) and miR-130a (P = 0.001) and high expression levels of miR-222 (P = 0.001), miR-218 (P < 0.001), and miR-185 (P < 0.001) were independent factors for predicting elevated AIS risk.
Discussion
In this study, we evaluated plasma expression levels of five miRNAs to investigate their associations with disease risk, disease severity, and inflammatory cytokines in AIS patients. Our data showed that (1) plasma levels of miR-126 and miR-130a were repressed, while plasma levels of miR-222, miR-218, and miR-185 were upregulated in AIS patients relative to controls. ROC analysis revealed that pooling miR-126, miR-130a, miR-222, miR-218, and miR-185 expression levels yields a useful predictive metric for AIS risk; (2) miR-126 and miR-130a expression levels were negatively correlated with NIHSS scores, while the miR-218 expression level was positively correlated with NIHSS scores; (3) miR-126 and miR-130a expression levels are both negatively correlated with levels of TNF-α, IL-1β, and IL-6, while miR-130a expression levels are positively correlated with IL-10 level.
Many reports have demonstrated that the five miRNAs explored in the present study, including miR-126, miR-130a, miR-222, miR-218, and miR-185, are involved in the regulation of angiogenesis [14,15,16,17,18,19,20,21]. Specifically, miR-126 is found to be highly expressed in human endothelial cells and exhibits a protective role in intracerebrally hemorrhaging mice through angiogenesis regulation [14, 15]; miR-130a regulates the homeobox A5 (HOXA5) homeobox gene GAS, a growth arrest-specific homeobox, thereby promoting the production of vascular endothelial cells angiogenic phenotype [16]; miR-222 has been shown to target stem cell factor (SCF) and cKit and thus obstruct endothelial cell migration, proliferation, and function as anti-angiogenic miRNA in vitro [17, 18]; miR-218 has been shown to repress tumor angiogenesis by targeting the mTOR component RICTOR in prostate cancer cells and inhibits retinal neovascularization by reducing the expression of loop 1 in oxygen-induced retinopathy mice [19, 20]; miR-185 levels have been shown to change in endothelial cells under hypoxia, and miR-185 has been shown to negatively regulate angiogenesis in human microvascular endothelial cells by directly interacting with stromal interaction molecule1 [21]. This collective evidence suggests that miR-126, miR-130a, miR-222, miR-218, and miR-185 play critical roles in modulating angiogenesis in various diseases; however, their associations with AIS susceptibility are seldom reported. Our previous study showed that miR-126, miR-130a, miR-222, miR-218, and miR-185 are independent predicting factors for AIS risk. Pooling the expression levels of these five miRNAs yields a useful diagnostic metric for AIS risk with an AUC 0.767 (95% CI 0.705–0.829) [13]. In this study, we verified these results in a larger sample size of patients and were able to show that miR-126 and miR-130a expression levels were reduced in AIS patients, while miR-222, miR-218, and miR-185 expression levels were increased in AIS patients compared with controls. Pooling of these five miRNA levels yielded a metric that could be used to distinguish AIS patients from controls with AUC 0.840 (95% CI 0.795–0.885). A possible explanation for these results is that these five miRNAs regulate vascular epithelial cell functions by targeting angiogenetic genes or related pathways, and some of them such as miR-126 and miR-130a also modulate inflammation, as illuminated in our subsequent experiments. As a result, AIS patients display dysregulated expression levels of these five miRNAs.
As for disease severity, we observed that miR-126 and miR-130a were negatively correlated with NIHSS score, while miR-218 was positively correlated with NIHSS score. These results might be because miR-126 and miR-130a act as pro-angiogenetic genes that prevent disease progression, while miR-218 is considered as anti-angiogenetic genes that promote disease progression in multiple cerebrovascular and cardiovascular diseases [14,15,16, 19, 20]. In addition, the inverse correlation of miR-126 and miR-130a with patients’ NIHSS scores might also result from these miRNAs’ anti-inflammation effects, which were verified in our following experiment.
Immune response to acute cerebral ischemia and subsequent inflammation are proposed to be major factors in AIS pathobiology, and corresponding anti-inflammation approaches contribute to decreasing the risk of AIS development and progression [22, 23]. Meanwhile, many recent studies have revealed that the interplay between the expression levels of several miRNAs and the effects of inflammatory cells or cytokines increases patients’ AIS susceptibility and severity [24, 25]. In the present study, we further analyzed the correlation between five miRNA expression levels and inflammatory cytokine levels in AIS patients, which illustrated that miR-126 and miR-130a acted as anti-inflammatory genes that negatively correlated with pro-inflammatory cytokines including TNF-α, IL-1β, and IL-6 levels. MiR-126 was discovered to inhibit secretion of TNF-α and IL-6 in human gingival fibroblasts under high glucose via targeting TNF receptor associated factor (TRAF) 6 and to protect human cardiac microvascular endothelial cells (HCMECs) from hypoxia/reoxygenation-induced injury and inflammatory response (IL-6, IL-10, and TNF-α) by activating the PI3K/Akt/eNOS signaling pathway [26]. MiR-130a was observed to decrease the expression of TNF-α, to inhibit inflammation in chondrocytes, and to reduce TNF-α and Sp1 via regulating NF-κB pathway in primary hepatocytes [27, 28]. Therefore, a possible explanation for our results might be the following: In AIS, these miRNAs might reduce the secretion of inflammatory cytokines through multiple pathways, such as targeting TRAF 6, activating the PI3K/Akt/eNOS signaling pathway and regulating the NF-κB pathway, thereby reducing AIS inflammation. In light of our aforementioned results, we considered that miR-126 and miR-130a are important factors involved in etiology of AIS not only because of their pro-angiogenetic effects but also because of their anti-inflammatory roles, as inflammation also plays a critical role in AIS etiology [26,27,28].
There were several limitations in this study: (1) As a case-control study, AIS patients were not followed up; thus, the values of studied miRNAs in prognosis of AIS patients were not explored. (2) The detailed mechanisms of studied miRNAs in regulating the development of AIS were not evaluated in our study. Therefore, in vivo and in vitro experiments investigating the detailed mechanism of these miRNAs in AIS need to be performed in the future. (3) As a case-control study, which has no follow-ups, the levels of miRNAs and inflammatory cytokines in patients with AIS were assessed only once (within 24 h post the onset of AIS); thus, the miRNAs and inflammatory cytokine levels after 24 h following the onset of AIS and after treatments were not assessed in our study.
In conclusion, plasma levels of circulating miR-126 and miR-130a correlate with lower disease risk, decreased disease severity, and reduced inflammatory cytokines in AIS patients, which indicates that miR-126 and miR-130a could be served as biomarkers for disease risk prediction and disease monitoring in clinical practice.
References
Hankey GJ (2017) Stroke. Lancet 389(10069):641–654. https://doi.org/10.1016/S0140-6736(16)30962-X
Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson L, Truelsen T, O'Donnell M, Venketasubramanian N, Barker-Collo S, Lawes CM, Wang W, Shinohara Y, Witt E, Ezzati M, Naghavi M, Murray C, Global Burden of Diseases I, Risk Factors S, the GBDSEG (2014) Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet 383(9913):245–254
Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson LM, Truelsen T, O'Donnell M, Venketasubramanian N, Barker-Collo S, Lawes CM, Wang W, Shinohara Y, Witt E, Ezzati M, Naghavi M, Murray C, Global Burden of Diseases IRFS, Group GBDSE (2013) Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health 1(5):e259–e281. https://doi.org/10.1016/S2214-109X(13)70089-5
Kilburg C, Scott McNally J, de Havenon A, Taussky P, Kalani MY, Park MS (2017) Advanced imaging in acute ischemic stroke. Neurosurg Focus 42(4):E10. https://doi.org/10.3171/2017.1.FOCUS16503
Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors JJ, Culebras A, Elkind MS, George MG, Hamdan AD, Higashida RT, Hoh BL, Janis LS, Kase CS, Kleindorfer DO, Lee JM, Moseley ME, Peterson ED, Turan TN, Valderrama AL, Vinters HV, American Heart Association Stroke Council CoCS, Anesthesia, Council on Cardiovascular R, Intervention, Council on C, Stroke N, Council on E, Prevention, Council on Peripheral Vascular D, Council on Nutrition PA, Metabolism (2013) An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 44(7):2064–2089. https://doi.org/10.1161/STR.0b013e318296aeca
Fisher M, Albers GW (2013) Advanced imaging to extend the therapeutic time window of acute ischemic stroke. Ann Neurol 73(1):4–9. https://doi.org/10.1002/ana.23744
Dong H, Lei J, Ding L, Wen Y, Ju H, Zhang X (2013) MicroRNA: function, detection, and bioanalysis. Chem Rev 113(8):6207–6233. https://doi.org/10.1021/cr300362f
Maitrias P, Metzinger-Le Meuth V, Nader J, Reix T, Caus T, Metzinger L (2017) The involvement of miRNA in carotid-related stroke. Arterioscler Thromb Vasc Biol 37(9):1608–1617. https://doi.org/10.1161/ATVBAHA.117.309233
Che F, Du H, Zhang W, Cheng Z, Tong Y (2018) MicroRNA-132 modifies angiogenesis in patients with ischemic cerebrovascular disease by suppressing the NFkappaB and VEGF pathway. Mol Med Rep 17(2):2724–2730. https://doi.org/10.3892/mmr.2017.8138
Majdi A, Mahmoudi J, Sadigh-Eteghad S, Farhoudi M, Shotorbani SS (2016) The interplay of microRNAs and post-ischemic glutamate excitotoxicity: an emergent research field in stroke medicine. Neurol Sci 37(11):1765–1771. https://doi.org/10.1007/s10072-016-2643-5
Zhou Y, Deng L, Zhao D, Chen L, Yao Z, Guo X, Liu X, Lv L, Leng B, Xu W, Qiao G, Shan H (2016) MicroRNA-503 promotes angiotensin II-induced cardiac fibrosis by targeting Apelin-13. J Cell Mol Med 20(3):495–505. https://doi.org/10.1111/jcmm.12754
Liang TY, Lou JY (2016) Increased expression of mir-34a-5p and Clinical Association in Acute Ischemic Stroke Patients and in a rat model. Med Sci Monit 22:2950–2955
Jin F, Xing J (2017) Circulating pro-angiogenic and anti-angiogenic microRNA expressions in patients with acute ischemic stroke and their association with disease severity. Neurol Sci 38(11):2015–2023. https://doi.org/10.1007/s10072-017-3071-x
van Solingen C, Seghers L, Bijkerk R, Duijs JM, Roeten MK, van Oeveren-Rietdijk AM, Baelde HJ, Monge M, Vos JB, de Boer HC, Quax PH, Rabelink TJ, van Zonneveld AJ (2009) Antagomir-mediated silencing of endothelial cell specific microRNA-126 impairs ischemia-induced angiogenesis. J Cell Mol Med 13(8A):1577–1585. https://doi.org/10.1111/j.1582-4934.2008.00613.x
Kong F, Zhou J, Zhou W, Guo Y, Li G, Yang L (2017) Protective role of microRNA-126 in intracerebral hemorrhage. Mol Med Rep 15(3):1419–1425. https://doi.org/10.3892/mmr.2017.6134
Chen Y, Gorski DH (2008) Regulation of angiogenesis through a microRNA (miR-130a) that down-regulates antiangiogenic homeobox genes GAX and HOXA5. Blood 111(3):1217–1226. https://doi.org/10.1182/blood-2007-07-104133
Poliseno L, Tuccoli A, Mariani L, Evangelista M, Citti L, Woods K, Mercatanti A, Hammond S, Rainaldi G (2006) MicroRNAs modulate the angiogenic properties of HUVECs. Blood 108(9):3068–3071. https://doi.org/10.1182/blood-2006-01-012369
Li Y, Song YH, Li F, Yang T, Lu YW, Geng YJ (2009) MicroRNA-221 regulates high glucose-induced endothelial dysfunction. Biochem Biophys Res Commun 381(1):81–83. https://doi.org/10.1016/j.bbrc.2009.02.013
Guan B, Wu K, Zeng J, Xu S, Mu L, Gao Y, Wang K, Ma Z, Tian J, Shi Q, Guo P, Wang X, He D, Du Y (2017) Tumor-suppressive microRNA-218 inhibits tumor angiogenesis via targeting the mTOR component RICTOR in prostate cancer. Oncotarget 8(5):8162–8172. https://doi.org/10.18632/oncotarget.14131
Han S, Kong YC, Sun B, Han QH, Chen Y, Wang YC (2016) microRNA-218 inhibits oxygen-induced retinal neovascularization via reducing the expression of roundabout 1. Chin Med J 129(6):709–715. https://doi.org/10.4103/0366-6999.178013
Hou J, Liu L, Zhu Q, Wu Y, Tian B, Cui L, Liu Y, Li X (2016) MicroRNA-185 inhibits angiogenesis in human microvascular endothelial cells through targeting stromal interaction molecule 1. Cell Biol Int 40(3):318–328. https://doi.org/10.1002/cbin.10572
Anrather J, Iadecola C (2016) Inflammation and stroke: an overview. Neurotherapeutics 13(4):661–670. https://doi.org/10.1007/s13311-016-0483-x
Esenwa CC, Elkind MS (2016) Inflammatory risk factors, biomarkers and associated therapy in ischaemic stroke. Nat Rev Neurol 12(10):594–604. https://doi.org/10.1038/nrneurol.2016.125
Khoshnam SE, Winlow W, Farzaneh M (2017) The interplay of MicroRNAs in the inflammatory mechanisms following ischemic stroke. J Neuropathol Exp Neurol 76(7):548–561. https://doi.org/10.1093/jnen/nlx036
Huang L, Ma Q, Li Y, Li B, Zhang L (2018) Inhibition of microRNA-210 suppresses pro-inflammatory response and reduces acute brain injury of ischemic stroke in mice. Exp Neurol 300:41–50. https://doi.org/10.1016/j.expneurol.2017.10.024
Yang HH, Chen Y, Gao CY, Cui ZT, Yao JM (2017) Protective effects of microRNA-126 on human cardiac microvascular endothelial cells against hypoxia/reoxygenation-induced injury and inflammatory response by activating PI3K/Akt/eNOS signaling pathway. Cell Physiol Biochem 42(2):506–518. https://doi.org/10.1159/000477597
Li ZC, Han N, Li X, Li G, Liu YZ, Sun GX, Wang Y, Chen GT, Li GF (2015) Decreased expression of microRNA-130a correlates with TNF-alpha in the development of osteoarthritis. Int J Clin Exp Pathol 8(3):2555–2564
Zheng H, Dong X, Liu N, Xia W, Zhou L, Chen X, Yang Z, Chen X (2016) Regulation and mechanism of mouse miR-130a/b in metabolism-related inflammation. Int J Biochem Cell Biol 74:72–83. https://doi.org/10.1016/j.biocel.2016.02.021
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
This study was approved by the Ethics Committee of Cangzhou Central Hospital, and all participants or direct family members signed the written informed consents.
Rights and permissions
About this article

Cite this article
Jin, F., Xing, J. Circulating miR-126 and miR-130a levels correlate with lower disease risk, disease severity, and reduced inflammatory cytokine levels in acute ischemic stroke patients. Neurol Sci 39, 1757–1765 (2018). https://doi.org/10.1007/s10072-018-3499-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-018-3499-7