
Abstract
Topographical disorientation (TD) refers to navigational impairment as an effect of aging or brain damage. Decreases in navigational performance with aging are more due to deficits in the ability to mentally represent space in an object-centered (allocentric) than in a self-centered (egocentric) format. Familiarity/remoteness of spatial memory traces can represent a protective factor for TD in aging. Conversely, using newly learned information for assessment may lead to overestimating TD severity as it combines two contributing factors: heading (allocentric) disorientation and anterograde agnosia. A supplementary evaluation of TD with aging according to ecological spatial tasks is recommended. The core tasks should focus on landmark positioning, both on a blind map (allocentric) and along a route (egocentric) of the hometown so as to disentangle spatial memory for familiar/remote information from decline due to recent encoding of information.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Navigation and spatial mental representation decline in aging: topographical disorientation
An extensive description of spatial cognition in humans includes encoding, consolidating, and mentally representing information that supports navigating the environment, communicating information about objects and the environment to others, and mentally manipulating spatial information and related objects [1]. In particular, spatial memory involves: remembering the location of objects in the environment, remembering the spatial context of a given memory trace, and recalling the topographical information related to a given environment, such as the presence of beacon (i.e., local) and compass (i.e., distant), landmarks, or environmental geometry (e.g., the layout of an enclosure) [2].
All the aforementioned components of spatial memory subserve two relevant functions of navigation, that is, wayfinding—a route is followed to reach a familiar location—and route learning—acquiring a new route [3]. The ensemble of these functions enables individuals to be topographically oriented.
The other side of the coin is topographical disorientation (TD). It refers to a syndrome characterized by the impairment of spatial and navigational abilities in real-world environments and is associated with a variety of brain disorders, such as dementia, traumatic brain injuries, stroke, epilepsy, and developmental disorders. In their seminal work, Aguirre and D’Esposito [4] proposed a four-category taxonomy of topographical disorientation: egocentric disorientation, heading (allocentric) disorientation, landmark agnosia, and anterograde disorientation.
Egocentric disorientation entails a severe deficit in representing the relative location of objects with respect to the self. In severe forms of the syndrome, patients are equally impaired in both familiar and in unfamiliar environment way-finding tasks. Data on human and animal brain lesions have shown that egocentric disorientation is associated with the posterior parietal lobe.
Heading disorientation consists in failing to derive directional information from landmarks. Patients suffering from heading disorientation also show great impairment in map drawing tasks. This could also be identified as allocentric disorientation, since patients form unreliable object-centered mental representations of an environment. The cerebral area associated with this category of the syndrome is the right retrosplenial cortex (i.e., posterior cingulate).
The third category is called landmark agnosia. It is an inability to recognize salient environment features and familiar landmarks, and has implications for navigation. The lesion sites responsible for landmark agnosia are situated in the medial part of the occipital lobe, involving the fusiform and lingual gyri and sometimes the parahippocampal gyrus.
Finally, the fourth category is labeled anterograde disorientation, in which the topographical impairment is primarily confined to novel environments. All the patients included in this category preserve way-finding skills in known environments but encounter great difficulties in encoding spatial information in novel environments, and all of them have lesions located in the medial temporal lobe, specifically in the parahippocampal cortex.
The egocentric and heading (allocentric) components, in the original taxonomy, refer to previously learned information (retrospective traces), while the anterograde disorientation component refers to spatial information to be acquired. To our knowledge, studies on retrograde disorientation are sparse. Therefore, the aims of this study are (1) to describe the most relevant literature on normal and pathological aging associated with orientation disorders involving topographical tasks (e.g., route learning, map completion, real navigation), with a particular focus on the role of familiarity in preserving spatial memory and (2) to propose a guide for the construction of two ecological spatial tasks suitable for detecting the retrograde components of TD. The general aim is not to identify new tasks for early detection of cognitive disorders, since these kinds of tasks are already available and are appropriately based on newly learned information, but rather to gather information on a more complete assessment framework for TD as described by Aguirre and D’ Esposito [4]. Indeed, if it is no longer possible to teach new spatial information in the most advanced stages of cognitive deterioration, remote information may nevertheless be spared, and thus represent an important clue to residual cognitive efficiency.
Topographical disorientation in Alzheimer’s disease
The aforementioned taxonomy is compatible with the assessment of TD as a consequence of cognitive decline resulting from neurodegenerative syndromes, specifically Alzheimer’s Disease (AD, [5,6,7]). Referring to single case studies, Grossi and colleagues [8] described the impairments of a patient with a progressive TD: while the patient only got lost in unfamiliar surroundings at the beginning of the observation period, getting lost episodes were later observed even in very familiar environments. Burgess and colleagues [9] described another case of a woman with probable early AD and severe TD but otherwise largely preserved cognitive skills. In navigational tests, she failed to remember object-locations when her viewpoint was shifted between the encoding and testing phases, but not when she was tested from the same viewpoint. The authors suggested that this person showed a selective deficit of allocentric spatial memory; by contrast, her egocentric spatial memory was spared. Pai and Hsiao [10] investigated emerging symptoms in a large sample of patients with AD and found that TD represented an early onset symptom in 7% of that sample. Pai and Jacobs [11] confirmed this decrease in orientation ability documenting the frequency of TD in a new large sample of early AD patients residing in a community in Taiwan. They found that almost 50% of patients presented TD. Functional imaging studies are in line with behavioral results: damage to several brain structures seems to be involved in TD (i.e., lingual gyrus, posterior parietal cortex, retrosplenial cortex, and parahippocampus/hippocampus), while early AD involves damage to the same areas (i.e., particularly the hippocampus and parietal structures). It is therefore reasonable to expect TD, together with spatial memory and navigation disorders, to be one of the early symptoms of AD, and not only as a consequence of general mental deterioration in the advanced stages of neurodegenerative processes [12, 13]. Moreover, in order to strengthen this hypothesis, some studies (e.g., [14, 15]) have argued that deficits in visual attentional dynamics and in visual perception, as well as in integration of spatial information, creation and storage of memory traces, and in the use of spatial information during navigational behavior, may account in large part for the occurrence of TD in AD. Guariglia and Nitrini [16] investigated the occurrence of TD in patients with mild to moderate dementia. They found that TD differentiated patients from control participants, even in early stages of AD. The spatial abilities which were most impaired even in mild AD were those related to landmark recognition, as well as egocentric, and allocentric orientation. Landmark recognition and route description impairments were more severely involved in moderate dementia, probably accounting for the worsening of TD usually seen in moderate compared to mild AD patients, while allocentric orientation appeared to be impaired relatively early in the course of the disease. More recently, Tu and colleagues [17] investigated spatial orientation in dementia patients and a group of healthy controls using a novel virtual task (i.e., a supermarket) as well as voxel-based morphometry. Results revealed significantly impaired spatial orientation in AD, compared to patients with other forms of dementia.
Topographical disorientation in mild cognitive impairment
The interest in TD for patients with mild cognitive impairment (MCI) is more recent [18]. MCI is known to be a transitional stage of cognitive impairment between normal aging and early dementia [19, 20]. The neural association between TD and MCI was investigated by Lim, Iaria, and Moon [21]. Results showed that the presence of TD in MCI patients was associated with loss of gray matter in the medial temporal regions, including hippocampus and parahippocampal cortex, fusiform gyrus, inferior occipital gyrus, amygdala, and cerebellum. These findings were consistent with those of DeIpolyi and colleagues [22], who compared the neural correlates of spatial abilities and navigation in 21 MCI and 13 AD patients with 24 healthy controls on a route-learning task that engaged various spatial processes. Results showed that both MCI and AD patients recognized landmarks as effectively as controls but could not find their locations on maps or recall the order in which they were encountered. Half of AD and one-quarter of MCI patients got lost on the route and showed lower right posterior hippocampal and parietal volumes than patients and controls who did not get lost. Hort and colleagues [23] documented the presence of spatial navigation disorders in amnestic MCI patients (aMCI). Results showed that AD patients and the amnestic MCI multiple domain (aMCImd) group were impaired in all subtests (i.e., egocentric, allocentric, egocentric/allocentric, and a delayed task, in both real and virtual versions). The amnestic MCI single domain (aMCIsd) group was significantly impaired on a subtest focused on allocentric orientation (e.g., [24, 25]). From a neuroanatomic point of view, the hippocampus was involved in the spatial impairment. The hippocampal size was reduced in patients affected by aMCI [26].
Similarly, Laczo and colleagues [27] tested AD, non-amnestic MCI (naMCI), and aMCI patients, as well as control participants using a real-world version of the Morris water maze. Overall, AD and MCI groups performed worse than controls in all subtests; the MCI group with a hippocampal impairment performed worse than the MCI group without hippocampal impairment especially in the allocentric subtest. Weniger and colleagues [28] compared patients with aMCI and healthy controls on two virtual reality navigation tasks assessing allocentric and egocentric spatial memory. Behavioral results showed that aMCI patients were significantly more impaired than controls in both allocentric and egocentric tasks. Caffò and colleagues [29, 30] investigated categorical spatial memory deficits using a virtual navigation-based reorientation task. MCI patients with the amnesic form of the disease were compared to healthy elderly controls on the performance of a virtual reorientation test (i.e., VReoT). The reorientation performance of participants with amnesic MCI was significantly worse than that of controls, specifically in the subtest characterized by directional landmarks, showing that they were most impaired in tasks requiring allocentric abilities. Benke and colleagues [31] investigated neuropsychological and demographical predictors of route learning impairment in aged normal controls and patients with MCI and AD. An ecological assessment procedure for route learning (RL) was employed, as well as the evaluation of landmark learning and navigational abilities. Results showed that almost all AD patients and most subjects with MCI misidentified landmarks and made navigational errors when following the route without assistance. Moreover, a small subgroup of normal controls also had problems with RL. Poor RL performance was best predicted by impairments in memory and executive functions [32]. Rusconi and colleagues [33] submitted healthy participants and two groups of MCI patients (aMCI and naMCI) to a neuropsychological battery and to a new spatial navigation test of reproducing an ideal city. They found that aMCI patients performed worse in learning a new route, in replacing landmarks in the city, and in drawing a map of the city, while naMCI patients’ performance was not different from that observed in healthy subjects, except that they required more time for route forward learning. Serino and colleagues [34] compared the performances of participants suffering from aMCI, patients with AD, and a control group, using a virtual reality-based procedure to assess abilities for encoding, storing, and syncing different spatial representations. The authors found that aMCI patients showed a deficit in the ability to encode and store an allocentric viewpoint independent representation. On the other hand, AD patients had a specific impairment in storing an allocentric viewpoint independent representation and then syncing it with the allocentric viewpoint dependent representation. Results in the aforementioned areas of research need to be better harmonized; nonetheless, it seems clear that an allocentric format for spatial tasks is more demanding than an egocentric one. More recently, Boccia and colleagues [35] assessed the neural correlates of the decline of topographical memory in patients with aMCI and healthy controls by means of an intensive learning paradigm. Participants had to encode one path from an egocentric perspective and one path from an allocentric perspective and after the learning period, they were asked to retrieve each of these paths using an allocentric or egocentric frame of reference. Results showed that aMCI patients had a specific deficit in storing new topographical memories from an allocentric perspective and retrieving stored information to perform the egocentric task, with respect to healthy controls. These deficits were correlated with hypoactivation of the brain areas generally involved in spatial navigation.
From a neuroanatomical point of view, all of the above statements are supported by theories of hippocampal function [36]. In this regard, Byrne, Becker, and Burgess [37] proposed a computational model of the neural structures subserving spatial memory: the BBB Model. According to the BBB Model, the role of the hippocampus is crucial. It specifies that most spatial activities require translation between egocentric and allocentric representations, based on the assumption that allocentric and egocentric representations are often combined. The allocentric parahippocampal representation is transformed into an egocentric medial parietal representation by processing in the posterior parietal cortex and the retrosplenial cortex/parieto–occipital sulcus. Even if the BBB Model is useful for a reconstruction of mental spatial representations, gradually, the memory traces become more and more consolidated and independent from the medial temporal lobe structures.
Another key point is that most of the research investigates newly learned environments. Less is known about the effects of aging on orientation in familiar environments. The next section is devoted to this topic.
Topographical disorientation in aging. Why familiarity with the environment matters
As stated above, most research on aging participants has studied egocentric-allocentric memory in tasks involving recently encoded information. By contrast, only a few studies have investigated remote egocentric-allocentric memory likely acquired due to repeated occurrences of navigation, such as in participants’ hometowns.
Evans and Pezdek [38] introduced the term familiar with reference to spatial information from the everyday world. Their intention was to improve our knowledge of how people process spatial information derived from familiar (i.e., direct experience with the University Campus of San Bernardino) as contrasted with unfamiliar environments (i.e., map study of the same setting). Results showed that when the environment was primarily learned through direct experience, spatial information was processed from many viewpoints; by contrast, map study produced orientation-dependent representations. Thorndyke and Hayes-Roth [39] compared two groups of participants, one with a direct experience of the environment (familiar group) and the other who learned the same setting through map study. The familiar group performed better in tasks related to route estimation and pointing out objects than the unfamiliar group.
Kirasic [40] evaluated memory for the configural representation of newly-learned and familiar supermarkets in young and elderly women through their ability to judge distances between objects with route and map placement tasks. The difference in performance for the young and elderly was smaller for familiar than for newly learned environments. More recently, Iachini and colleagues [41] reported results showing that allocentric representations are available if participants have had extensive experience with an environment. If the extensive experience is lacking, then the egocentric format is the most likely frame of reference available for the participants.
Shifting our attention to aging studies, Rosenbaum and colleagues [42] showed that elderly people performed as well as the young on judgment of direction tasks regarding consolidated spatial information. Meneghetti and colleagues [43] confirmed that older people performed with the same level of accuracy as young people on judgment of direction tasks regarding their hometown. Moreover, Campbell and colleagues [44] investigated topographical memory processes for autobiographical, topographical, and semantic memories in participants with memory impairments. The results showed that age and gender had an impact on heading orientation while aging had no impact on memory for a familiar environment. Again, Muffato and colleagues [45] investigated age-related differences in spatial mental representation for familiar and unfamiliar environments, showing that the elderly performed as well as the young in pointing tasks. Finally, Merriman and colleagues [46] showed that familiarity with the environment protects the elderly from spatial memory impairment. Familiarity facilitated the elderly in tasks based on memory for objects and direction.
In a nutshell, behavioral studies seem to be converging on the protective role of familiarity for elderly people, in particular, if they are required to perform allocentric tasks. The results of neuroscience research have provided good support for these behavioral studies. Since O’Keefe and Nadel’s work [47], it has been recognized that the hippocampal area is widely engaged in acquiring spatial memory for navigation [48]. According to Maguire [49], an experienced London taxi driver with selective hippocampal atrophy was able to rely on an over learned schematic representation of the environment acquired before the damage. It has been demonstrated that patients with bilateral damage to the hippocampus and medial temporal lobe are able to retrieve remote spatial memories but not to learn recent spatial information [48, 50,51,52,53]. Accordingly, the Multiple Trace Theory (MTT) (e.g., [54]) suggested that both recent and remote memories seem to depend on the hippocampus. Notwithstanding, each time a remote memory is retrieved, a new hippocampal-mediated trace is formed, so that older memories are more represented than new ones. MTT argues that these well consolidated memories are also represented in extrahippocampal structures and are less prone to be impaired or lost than recent memories [54,55,56].
Moreover, Boccia and colleagues [57] supported the claim that few studies investigated the relationship between old and recent memory from a functional point of view. The authors underlined the presence of different networks designed to navigate in a well-learned, familiar environment and a recently learned environment. The middle frontal gyrus, posterior cingulate cortex, and superior temporal gyrus seemed to be involved in processing familiar environments. By contrast, the inferior parietal lobule, precuneus, cuneus, lingual gyrus, and parahippocampal gyrus seemed to be involved in processing newly learned environments.
Considering all of the above, it is possible that the documented difficulties that older people face in making use of allocentric information is not entirely independent of the fact that most studies on spatial memory examine recently learned information which has not yet had sufficient time to be consolidated, transformed, and transferred to brain structures other than the hippocampus. Compatibly, the corpus of research on the recovery of weakly consolidated information has probably contributed to producing an overestimation bias for decreased performance of allocentric tasks.
Topographical disorientation: Evaluation supplement with hometown orientation tasks
Two main kinds of task have been developed to assess the encoding and the retrieval of egocentric and allocentric information: the laboratory-based psychometric tasks based on mental rotation, spatial updating, pointing errors, reorientation paradigms, and learning paradigms, (see for a review, [30, 58,58,60]) and more ecological tasks such as direction finding and studying maps [61,62,63]. They were based on three different learning settings: real environments (e.g., [64]), simulated, virtual environments (e.g., [65, 66]), and maps (e.g., [67, 68]). For the present review, our interest is in the more ecological tasks such as pointing, sketching (completion of a) map, and wayfinding [40, 61, 62].
The aforementioned ecological tasks can be listed as follows:
-
landmark name recall or recognition: to tag the correct names for landmarks or to select the correct name from a list of distractors;
-
landmark map localization (position): to pinpoint the correct positions of the landmarks on a map;
-
route recall: to pinpoint the correct positions of the landmarks along a path;
-
spatial judgment: to estimate Euclidean distances between landmarks or to make a categorical evaluation of landmark positions (i.e., “A is on the left/right or west/east of B”);
-
heading orientation (perspective and compass direction): to provide a compass direction of the landmarks using a given perspective.
In accordance with the idea that solving spatial tasks based on egocentric and allocentric frames of reference is the core ability for individuals since such tasks include landmark recall/recognition, spatial judgment and heading orientation [44, 46], two general hometown spatial tasks as well as criteria for scoring them are introduced here. Both tasks are focused on landmark positioning: on a blind map (allocentric format) or along a route (egocentric format) of the hometown. Furthermore, a detailed description of the test materials is given to make the mapping task freely available.
The initial question that needs to be considered is: what are the criteria for a good spatial task? Starting from Lynch’s theory of urban form [69] and the importance of interactions between observer and environment in building a cognitive map, Imageability determines the visual quality of the environment. Namely, “it is the quality in a physical object which gives it a higher probability of evoking a strong image in any given observer.” The quality of an object depends upon its location (real location, spatial relationships, prominence, and scope), appearance (shape, color, age, size, and construction materials), meaning (economic, political, social, historical, or religious functions), and associations (familiarity, atmosphere, and affinity) [70]. A vividly imagined environment would have a good form, a strong identity, and would be recognizable to citizens. People can create a mental map that constitutes a mental representation of what the city contains, namely landmarks. The landmarks are unique elements and external features that act as reference points for an individual [69]. Landmarks vary with an individual’s personal experience, and they are very important cues in the way-finding process. Landmarks are characterized by physical and identity features. They are distinguishable by their physical structures or geographic features and singularity, prominence, accessibility, content, prototypicality, stability, and function. Moreover, landmarks can be distant (like a sign indicating the direction toward a target) or local (like a beacon, near the target). Therefore, the first step in evaluating a map or a path is to define a finite set of landmarks that constitutes the target environment.
Landmark positioning on a map (LPM, [71])
A LPM task of the hometown can be used to assess allocentric spatial memory. Three steps have to be followed to arrange a suitable task in order to collect an allocentric representation of hometown landmarks for the patient/participant:
-
(1)
To select ten salient landmarks from the geographical map of the intended town. Going beyond the classical contribution of Linch [69], the topic of the salience of landmarks for navigation and, in turn, for spatial mental representations has recently garnered significant attention (e.g., [72,73,74,75]) and suggests different methods for deriving physical as well as cognitive characteristics of the elements within an environment from maps, or from verbal descriptions given from the point of view of the observer. Moreover, in our knowledge, there are no empirical data regarding differences with respect to landmark positioning depending on whether the boundaries of the town are available or not available. In our opinion, giving the boundary of the town on the sheet will facilitate the task of the participants by anchoring their work to a given, canonical direction (e.g., North). The boundary is roughly inscribed in a circumference (not visible on the participant’s sheet) of 6.5 in. in diameter (see Fig. 1).
-
(2)
Two of the landmarks are fixed on the map as reference points: one in the center of the invisible circumference and the other on the boundary. The latter serves as a second anchor either in terms of direction or for estimating distances. Using a web mapping service (Google Maps®), that offers a satellite bird’s eye view image, and selecting the area/place/location of interest, it is possible to pinpoint landmarks manually by clicking the marker icon and placing it directly on the map, or to search for locations using the search box at the top of the screen (see Fig. 2).
-
(3)
At the beginning of the testing phase, it is necessary to ensure that the landmarks have been successfully recognized (ten landmarks previously shown in photographs). In the event that the participant fails to recognize certain landmarks, they should not be included in the analysis. During the test phase, participants have a blind map of their hometown, the list of the to-be-placed landmarks, a pencil, and a rubber, so they can modify their work until they are fully satisfied. No time limits have been specified. The execution of the task lasts about 15 min. The participants are instructed to pinpoint all the landmarks, keeping in mind the metric (i.e., relative distances) as well as categorical (“A is above/below and left/right of B”) spatial relationships between landmarks. The distance between the participant’s positioning and the true location of each landmark in an xy-Cartesian coordinate system provides the error score. In order to further simplify the scoring procedure, this coordinate information can be transformed into a discrete number of correct answers. In particular, a Cartesian coordinate system allows for the detection of position and direction in space in order to encode the landmark position (above and below x-Cartesian coordinate) and the landmark side (right and left y-Cartesian coordinate). Consequently, for every correct landmark placement compared to the other objects, namely the real landmark position in relation to the geocentric coordinates of any other object, the participants receive one point. The highest possible number of correct answers for the LPM task is 56 points (28 on the North-South, y; and 28 on the East-West, x; axes), (see Fig. 3).

Landmark positioning on a map (LPM): example of circumference

Landmark positioning on a map (LPM): sheet for the participant

Landmark positioning on a map (LPM): sheet for the scoring
Landmark positioning along a route (LPR, [71])
The participant is required to imagine walking along a path, positioning a series of landmarks along a given route on the correct side of the street. The LPR task is used to assess egocentric spatial memory.
-
(1)
As in the LPM task, ten salient landmarks (different from those used in the LPM task) are selected.
-
(2)
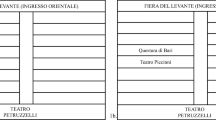
Two of the landmarks are fixed as reference points on the hometown path: one as the starting point and the other as the end point (see Fig. 4). After the research assistant has orally described the path, mentioning only the street names and turns, participants have to identify the correct landmark positions and pinpoint the remaining eight on the same path (e.g., “What would the first landmark be? On which side is it? What about the next one?”).
-
(3)
At the beginning of the testing phase, the landmark recognition task is performed. During the test phase participants have got a blind path of their hometown (see Fig. 5), the list of the to-be-placed landmarks, a pencil, and a rubber, since they can modify their work until they are fully satisfied. Time limits have not been specified. The execution of the task lasts about 15 min. Participants have to identify the correct landmark positions and pinpoint them on the path. The score for the items consists in a single measure between correct positions (28, the sum of the number of correct comparisons between each landmark and all the others along the route) and correct side (8 right and left orthogonal to the path).

Landmark positioning along a route (LPR): sheet for the participant

Landmark positioning along a route (LPR): sheet for the scoring
Conclusion
The present short critical review permits us to draw some brief concluding remarks: (a) spatial cognition domains undergo decline as an effect of aging-related functional and structural brain modifications [58], (b) TD is a prominent feature of AD and its prodromic stages, at least for newly learned spatial information, and can be used to monitor disease progression [18], (c) familiarity plays a decisive role in protecting elderly people from failures in orientation tasks in real environments, and can also, in specific circumstances, provide protection for allocentric tasks [46], and (d) the aforementioned monitoring (see point b of the present list) cannot be confined to the standardized neuropsychological, psychometric tasks typically based on newly-learned, virtual, fictitious environments. In such tasks, there is a risk of overestimating TD because different deficits are combined: in particular, heading (allocentric) disorientation is compounded with anterograde agnosia and in general with well-documented difficulties in learning new material. The important message for researchers is that they should without delay devise new ecological tasks for spatial orientation based on standardized and shared strategies of construction that relate to the daily living environment of every elderly individual requiring an assessment. In this way, the progression of any impairment or the preservation of health can be monitored in a fair and suitable way. This will require the involvement of a large number of primary care centers and memory clinics that can develop tasks appropriate for the local areas in which they operate, and a series of large multicenter studies that can collect data, to validate a large series of hometown-based tasks and, in turn, to disentangle allocentric ability from the ability to learn new spatial information [71].
The present critical review encompasses the point of view widely supported by the World Health Organization and by the EU Framework Programme for Research and Innovation (i.e., Horizon 2020) which aim to implement policies that increase the promotion of health, and wellness and “active aging” according to a deeper understanding of the causes of neurodegenerative conditions and the search for appropriate and fair assessments, treatments, rehabilitative interventions (e.g., [76]), and care strategies.
References
Klencklen G, Després O, Dufour A (2012) What do we know about aging and spatial cognition? Reviews and perspectives. Ageing Res Rev 11(1):123–135. https://doi.org/10.1016/j.arr.2011.10.001
Postma A, van der Ham I J M (2016) Neuropsychology of space: spatial functions of the human brain. Academic Press
Moffat SD (2009) Aging and spatial navigation: what do we know and where do we go? Neuropsychol Rev 19(4):478–489. https://doi.org/10.1007/s11065-009-9120-3
Aguirre GK, D'Esposito M (1999) Topographical disorientation: a synthesis and taxonomy. Brain 122(9):1613–1628. https://doi.org/10.1093/brain/122.9.1613
Giovagnoli AR, Manfredi V, Parente A, Schifano L, Oliveri S, Avanzini G (2017) Cognitive training in Alzheimer’s disease: a controlled randomized study. Neurol Sci 38(8):1485–1493. https://doi.org/10.1007/s10072-017-3003-9
Ferrari C, Nacmias B, Sorbi S (2018) The diagnosis of dementias: a practical tool not to miss rare causes. Neurol Sci 39(4):615–627. https://doi.org/10.1007/s10072-017-3206-0
Stanzani Maserati M, D’Onofrio R, Matacena C, Sambati L, Oppi F, Poda R, Capellari S (2018) Human figure drawing distinguishes Alzheimer’s patients: a cognitive screening test study. Neurol Sci 39:1–5. https://doi.org/10.1007/s10072-018-3288-3
Grossi D, Fasanaro AM, Cecere R, Salzano S, Trojano L (2007) Progressive topographical disorientation: a case of focal Alzheimer’s disease. Neurol Sci 28(2):107–110. https://doi.org/10.1007/s10072-007-0797-x
Burgess N, Trinkler I, King J, Kennedy A, Cipolotti L (2006) Impaired allocentric spatial memory underlying topographical disorientation. Rev Neurosci 17(1–2):239–251. https://doi.org/10.1515/REVNEURO.2006.17.1-2.239.
Pai MC, Hsiao S (2002) Incipient symptoms of alzheimer’s disease and effect of education on the onset age: a study of 155 taiwanese patients. Acta Neurol Taiwanica 11(2):66–69
Pai MC, Jacobs WJ (2004) Topographical disorientation in community-residing patients with Alzheimer’s disease. Int J Geriatr Psychiatry 19:250–255. https://doi.org/10.1002/gps.1081
Iachini T, Iavarone A, Senese VP, Ruotolo F, Ruggiero G (2009) Visuospatial memory in healthy elderly, AD and MCI: a review. Curr Aging Sci 2(1):43–59. https://doi.org/10.2174/1874609810902010043
Wolbers T, Dudchenko PA, Wood ER (2014) Spatial memory—a unique window into healthy and pathological aging. Front Aging Neurosci 6(MAR). https://doi.org/10.3389/fnagi.2014.00035.
Mandal PK, Joshi J, Saharan S (2012) Visuospatial perception: an emerging biomarker for alzheimer’s disease. J Alzheimers Dis 31(SUPPL. 3):S117–S135. https://doi.org/10.3233/JAD-2012-120901.
Lester AW, Moffat SD, Wiener JM, Barnes CA, Wolbers T (2017) The aging navigational system. Neuron 95(5):1019–1035. https://doi.org/10.1016/j.neuron.2017.06.037
Guariglia CC, Nitrini R (2009) Topographical disorientation in alzheimer’s disease. Arq Neuropsiquiatr 67(4):967–972. https://doi.org/10.1590/S0004-282X2009000600001
Tu S, Wong S, Hodges JR, Irish M, Piguet O, Hornberger M (2015) Lost in spatial translation—a novel tool to objectively assess spatial disorientation in Alzheimer’s disease and frontotemporal dementia. Cortex 67:83–94. https://doi.org/10.1016/j.cortex.2015.03.016
Lithfous S, Dufour A, Després O (2013) Spatial navigation in normal aging and the prodromal stage of alzheimer’s disease: insights from imaging and behavioral studies. Ageing Res Rev 12(1):201–213. https://doi.org/10.1016/j.arr.2012.04.007
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Phelps CH (2011) The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the national institute on aging-alzheimer’s association workgroups on diagnostic guidelines for alzheimer’s disease. Alzheimers Dement 7(3):270–279. https://doi.org/10.1016/j.jalz.2011.03.008
Park S, Lee J, Lee K, Kim J (2018) Comparison of odor identification among amnestic and non-amnestic mild cognitive impairment, subjective cognitive decline, and early Alzheimer’s dementia. Neurol Sci 39(3):557–564. https://doi.org/10.1007/s10072-018-3261-1
Lim TS, Iaria G, Moo SY (2010) Topographical disorientation in mild cognitive impairment: a voxel-based morphometry study. J Clin Neurol 6(4):204–211. https://doi.org/10.3988/jcn.2010.6.4.204
DeIpolyi AR, Rankin KP, Mucke L, Miller BL, Gorno-Tempini ML (2007) Spatial cognition and the human navigation network in AD and MCI. Neurology 69(10):986–997. https://doi.org/10.1212/01.wnl.0000271376.19515.c6
Hort J, Laczó J, Vyhnálek M, Bojar M, Bureš J, Vlček K (2007) Spatial navigation deficit in amnestic mild cognitive impairment. Proc Natl Acad Sci U S A 104(10):4042–4047. https://doi.org/10.1073/pnas.0611314104
Iachini T, Ruggiero G, Ruotolo F (2009) The effect of age on egocentric and allocentric spatial frames of reference. Cogn Process 10(2):222–224. https://doi.org/10.1007/s10339-009-0276-9
Weniger G, Ruhleder M, Wolf S, Lange C, Irle E (2009) Egocentric memory impaired and allocentric memory intact as assessed by virtual reality in subjects with unilateral parietal cortex lesions. Neuropsychologia 47(1):59–69. https://doi.org/10.1016/j.neuropsychologia.2008.08.018
Wolf H, Jelic V, Gertz HJ, Nordberg A, Julin P, Wahlund LO (2003) A critical discussion of the role of neuroimaging in mild cognitive impairment. Acta Neurol Scand 107(Suppl. 179):52–76. https://doi.org/10.1034/j.1600-0404.107.s179.10.x.
Laczo J, Vlcek K, Vyhnalek M, Vajnerova O, Ort M, Holmerova I, Tolar M, Andel R, Bojar M, Hort J (2009) Spatial navigation testing discriminates two types of amnestic mild cognitive impairment. Behav Brain Res 202(2):252–259. https://doi.org/10.1016/j.bbr.2009.03.041
Weniger G, Ruhleder M, Lange C, Wolf S, Irle E (2011) Egocentric and allocentric memory as assessed by virtual reality in individuals with amnestic mild cognitive impairment. Neuropsychologia 49(3):518–527. https://doi.org/10.1016/j.neuropsychologia.2010.12.031
Caffò AO, De Caro MF, Picucci L, Notarnicola A, Settanni A, Livrea P, Lancioni GE, Bosco A (2012) Reorientation deficits are associated with amnestic mild cognitive impairment. Am J Alzheimers Dis Other Demen 27(5):321–330. https://doi.org/10.1177/1533317512452035
Caffò A O, Lopez A, Spano G, Serino S, Cipresso P, Stasolla F, … Bosco A (2017) Spatial reorientation decline in aging: the combination of geometry and landmarks. Aging Ment Health 1-12. doi:https://doi.org/10.1080/13607863.2017.1354973
Benke T, Karner E, Petermichl S, Prantner V, Kemmler G (2014) Neuropsychological deficits associated with route learning in alzheimer disease, MCI, and normal aging. Alzheimer Dis Assoc Disord 28(2):162–167. https://doi.org/10.1097/WAD.0000000000000009
Rusconi ML, Suardi A, Zanetti M, Rozzini L (2015) Spatial navigation in elderly healthy subjects, amnestic and non amnestic MCI patients. J Neurol Sci 359(1–2):430–437. https://doi.org/10.1016/j.jns.2015.10.010
Chipi E, Frattini G, Eusebi P, Mollica A, D’Andrea K, Russo M, Parnetti L (2018) The Italian version of cognitive function instrument (CFI): reliability and validity in a cohort of healthy elderly. Neurol Sci 39(1):111–118. https://doi.org/10.1007/s10072-017-3150-z
Serino S, Morganti F, Di Stefano F, Riva G (2015) Detecting early egocentric and allocentric impairments deficits in Alzheimer’s disease: an experimental study with virtual reality. Front Aging Neurosci 7. doi:https://doi.org/10.3389/fnagi.2015.00088.
Boccia M, Silveri MC, Sabatini U, Guariglia C, Nemmi F (2016) Neural underpinnings of the decline of topographical memory in mild cognitive impairment. Am J Alzheimers Dis Other Demen 31(8):618–630. https://doi.org/10.1177/1533317516654757
Ekstrom AD, Arnold AE, Iaria G (2014) A critical review of the allocentric spatial representation and its neural underpinnings: toward a network-based perspective. Front Hum Neurosci 8:803. https://doi.org/10.3389/fnhum.2014.00803
Bird CM, Burgess N (2008) The hippocampus and memory: insights from spatial processing. Nat Rev Neurosci 9(3):nrn2335. https://doi.org/10.1038/nrn2335
Evans GW, Pezdek K (1980) Cognitive mapping: knowledge of real-world distance and location information. J Exp Psychol Hum Learn 6(1):13–24. https://doi.org/10.1037/0278-7393.6.1.13
Thorndyke PW, Hayes-Roth B (1982) Differences in spatial knowledge acquired from maps and navigation. Cogn Psychol 14(4):560–589. https://doi.org/10.1016/0010-0285(82)90019-6
Kirasic KC (1991) Spatial cognition and behavior in young and elderly adults: implications for learning new environments. Psychol Aging 6(1):10–18. https://doi.org/10.1037/0882-7974.6.1.10
Iachini T, Borghi AM, Senese VP (2008) Categorization and sensorimotor interaction with objects. Brain Cogn 67(1):31–43. https://doi.org/10.1016/j.bandc.2007.11.002
Rosenbaum R S, Winocur G, Binns M A, Moscovitch M (2012) Remote spatial memory in aging: all is not lost. Front Aging Neurosci 4. doi: https://doi.org/10.3389/fnagi.2012.00025
Meneghetti C, Borella E, Fiore F, De Beni R (2013) The ability to point to well-known places in young and older adults. Aging Clin Exp Res 25(2):203–209. https://doi.org/10.1007/s40520-013-0027-8
Campbell JI, Hepner IJ, Miller LA (2014) The influence of age and sex on memory for a familiar environment. J Environ Psychol 40:1–8. https://doi.org/10.1016/j.jenvp.2014.04.007
Muffato V, Della Giustina M, Meneghetti C, De Beni R (2015) Age-related differences in pointing accuracy in familiar and unfamiliar environments. Cogn Process 16(1):313–317. https://doi.org/10.1007/s10339-015-0720-y
Merriman NA, Ondřej J, Roudaia E, O’Sullivan C, Newell FN (2016) Familiar environments enhance object and spatial memory in both younger and older adults. Exp Brain Res 234(6):1555–1574. https://doi.org/10.1007/s00221-016-4557-0
O'Keefe J, Nadel L (1978) The hippocampus as a cognitive map. Oxford: Clarendon Press
Burgess N, Maguire EA, O’Keefe J (2002) The human hippocampus and spatial and episodic memory. Neuron 35:625–641. https://doi.org/10.1016/S0896-6273(02)00830-9
Maguire EA, Woollett K, Spiers HJ (2006) London taxi drivers and bus drivers: a structural MRI and neuropsychological analysis. Hippocampus 16(12):1091–1101. https://doi.org/10.1002/hipo.20233
Rosenbaum RS, Priselac S, Köhler S, Black SE, Gao F, Nadel L, Moscovitch M (2000) Remote spatial memory in an amnesic person with extensive bilateral hippocampal lesions. Nat Neurosci 3(10):1044–1048. https://doi.org/10.1038/79867
Maguire EA, Vargha-Khadem F, Mishkin M (2001) The effects of bilateral hippocampal damage on fMRI regional activations and interactions during memory retrieval. Brain 124:1156–1170. https://doi.org/10.1093/brain/124.6.1156
Burgess N, Becker S, King JA, O'Keefe J (2001) Memory for events and their spatial context: models and experiments. Philos Trans R Soc B Biol Sci 356(1413):1493–1503. https://doi.org/10.1098/rstb.2001.0948
Rosenbaum RS, Gao F, Richards B, Black SE, Moscovitch M (2005) ‘Where to?’ Remote memory for spatial relations and landmark identity in former taxi drivers with Alzheimer’s disease and encephalitis. J Cogn Neurosci 17(3):446–462. https://doi.org/10.1162/0898929053279496
Moscovitch M, Rosenbaum RS, Addis DR, Westmacott R, Grady C, McAndrews MP, Levine B, Black S, Winocur G, Nadel L (2005) Functional neuroanatomy of remote episodic, semantic and spatial memory: a unified account based on multiple trace theory. J Anat 207(1):35–66. https://doi.org/10.1111/j.1469-7580.2005.00421.x
Winocur G, Moscovitch M, Sekeres M (2007) Memory consolidation or transformation: context manipulation and hippocampal representations of memory. Nat Neurosci 10(5):555–557. https://doi.org/10.1038/nn1880
Hirshhorn M, Newman L, Moscovitch M (2011) Detailed descriptions of routes traveled, but not map-like knowledge, correlates with tests of hippocampal function in older adults. Hippocampus 21(11):1147–1151. https://doi.org/10.3389/fnagi.2012.00025
Boccia M, Nemmi F, Guariglia C (2014) Neuropsychology of environmental navigation in humans: review and meta-analysis of FMRI studies in healthy participants. Neuropsychol Rev 24(2):236–251. https://doi.org/10.1007/s11065-014-9247-8
Serino S, Cipresso P, Morganti F, Riva G (2014) The role of egocentric and allocentric abilities in Alzheimer’s disease: a systematic review. Ageing Res Rev 16(1):32–44. https://doi.org/10.1016/j.arr.2014.04.004.
Ruggiero G, D’Errico O, Iachini T (2016) Development of egocentric and allocentric spatial representations from childhood to elderly age. Psychol Res 80(2):259–272. https://doi.org/10.1007/s00426-015-0658-9
Bosco A, Picucci L, Caffò AO, Lancioni GE, Gyselinck V (2008) Assessing human reorientation ability inside virtual reality environments: the effects of retention interval and landmark characteristics. Cogn Process 9(4):299–309. https://doi.org/10.1007/s10339-008-0210-6
Barrash J (1994) Age-related decline in route learning ability. Dev Neuropsychol 10(3):189–201. https://doi.org/10.1080/87565649409540578
Kirasic KC, Mathes EA (1990) Effects of different means for conveying environmental information on elderly adults’ spatial cognition and behavior. Environ Behav 22(5):591–607. https://doi.org/10.1177/0013916590225002
Boccia M, Vecchione F, Piccardi L, Guariglia C (2017) Effect of cognitive style on learning and retrieval of navigational environments. Front Pharmacol 8:496. https://doi.org/10.3389/fphar.2017.00496
Tlauka M (2006) Orientation dependent mental representations following real-world navigation. Scand J Psychol 47(3):171–176. https://doi.org/10.1111/j.1467-9450.2006.00504.x
Waller D (2005) The WALKABOUT: using virtual environments to assess large-scale spatial abilities. Comput Hum Behav 21(2):243–253. https://doi.org/10.1016/j.chb.2004.02.022
Picucci L, Caffo AO, Bosco A (2009) Age and sex differences in a virtual version of the reorientation task. Cogn Process 10(2):272–275. https://doi.org/10.1007/s10339-009-0321-8
Bosco A, Longoni AM, Vecchi T (2004) Gender effects in spatial orientation: cognitive profiles and mental strategies. Appl Cogn Psychol 18(5):519–532. https://doi.org/10.1002/acp.1000
Coluccia E, Bosco A, Brandimonte MA (2007) The role of visuo-spatial working memory in map learning: new findings from a map drawing paradigm. Psychol Res 71(3):359–372. https://doi.org/10.1007/s00426-006-0090-2
Lynch K (1960) The Image of the City. The MIT Press
Broadbent G, Bunt R, Jencks C (1980) Signs, symbols, and architecture. John Wiley & Sons
Lopez A, Caffò A O, Spano G, Bosco A (2019) The effect of aging on memory for recent and remote egocentric and allocentric information. Exp Aging Res in press
Caduff D, Timpf S (2008) On the assessment of landmark salience for human navigation. Cogn Process 9(4):249–267. https://doi.org/10.1007/s10339-007-0199-2
Götze J, Boye J (2016) Learning landmark salience models from users’ route instructions. J Locat Based Serv 10(1):47–63. https://doi.org/10.1080/17489725.2016.1172739
Röser F, Krumnack A, Hamburger K, Knauff M (2012) A four factor model of landmark salience—a new approach. In Proceedings of the 11th International Conference on Cognitive Modeling (ICCM) 82–87
Nemmi F, Piras F, Péran P, Incoccia C, Sabatini U, Guariglia C (2013) Landmark sequencing and route knowledge: an fMRI study. Cortex 49(2):507–519. https://doi.org/10.1016/j.cortex.2011.11.016
Caffò AO, Hoogeveen F, Groenendaal M, Perilli AV, Picucci L, Lancioni GE, Bosco A (2014) Intervention strategies for spatial orientation disorders in dementia: a selective review. Dev Neurorehabil 17(3):200–209. https://doi.org/10.3109/17518423.2012.749951
Funding
The second author (AOC) was supported by the project “Epidemiology of Topographical Disorientation and Mild Cognitive Impairment in a South Italian elderly population” - Action Co-founded by Cohesion and Development Fund 2007–2013 - APQ Research Puglia Region “Regional programme supporting smart specialization and social and environmental sustainability - FutureInResearch” (Grant Code CEY4SQ4). All the authors contributed to the conception, drafting and revising the work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Submission declaration
This is a review article that has not been published previously and is not under consideration for publication elsewhere. This work has been approved by all authors and explicitly by the responsible authorities where the work was carried out, and if accepted, will not be published elsewhere.
Rights and permissions
About this article

Cite this article
Lopez, A., Caffò, A.O. & Bosco, A. Topographical disorientation in aging. Familiarity with the environment does matter. Neurol Sci 39, 1519–1528 (2018). https://doi.org/10.1007/s10072-018-3464-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-018-3464-5