
Abstract
Introduction
Postoperative wound events following ventral hernia repair are an important outcome measure. While efforts have been made by hernia surgeons to identify and address risk factors for postoperative wound events following VHR, the definition of these events lacks standardization. Therefore, the purpose of our study was to detail the variability of wound event definitions in recent ventral hernia literature and to propose standardized definitions for postoperative wound events following VHR.
Methods
The top 50 cited ventral hernia, peer-reviewed publications from 1995 through 2015 were identified using the search engine Google Scholar. The definition of wound event used and the incidence of postoperative wound events was recorded for each article. The number of articles that used a standardized definition for surgical site infection (SSI), surgical site occurrence (SSO), or surgical site occurrence requiring procedural intervention (SSOPI) was also identified.
Results
Of the 50 papers evaluated, only nine (18%) used a standardized definition for SSI, SSO, or SSOPI. The papers that used standardized definitions had a smaller variability in the incidence of wound events when compared to one another and their reported rates were more consistent with recently published ventral hernia repair literature.
Conclusion
Postoperative wound events following VHR are intimately associated with patient quality of life and long-term hernia repair durability. Standardization of the definition of postoperative wound events to include SSI, SSO, and SSOPI following VHR will improve the ability of hernia surgeons to make evidence-based decisions regarding the management of ventral hernias.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Over 350,000 ventral hernias are repaired annually in the United States [1,2,3]. Historically, the two most important outcome measures following ventral hernia repair (VHR) are the incidence of postoperative wound events and long-term hernia recurrence [2]. Interestingly, the rate of wound events following VHR varies significantly in the literature, ranging anywhere from 4 to 23% and is higher than the 2% wound event rate following other clean procedures [2, 4,5,6]. This variability in the incidence of wound events following VHR is likely related to the heterogeneity of the underlying disease process and surgical techniques available for repair. Wound events following VHR are intimately associated with an increased risk of ventral hernia recurrence [2, 4, 7]. In fact, in a randomized controlled trial by Luijendijk et al., they found that patients who experienced a postoperative wound event had a greater than 80% risk of experiencing a ventral hernia recurrence [8].
In addition to an increased risk of ventral hernia recurrence, postoperative wound events following VHR negatively impact patient quality of life and are associated with a significant financial burden due to the need for long-term antibiotics, serial debridements, mesh removal, and repair of hernia recurrences [9, 10]. For example, in a recent study by Cox et al., they found that postoperative wound events following VHR were associated with an additional $16,000 of inpatient hospital costs [9]. Furthermore, in another study by Colavita et al., they found that postoperative wound events are associated with an additional $63,000 in healthcare costs over the first postoperative year compared to $1000 for routine follow-up care following VHR in the absence postoperative wound events [10].
As demonstrated above, there is a high variability among current ventral hernia literature regarding the true rate of postoperative wound events. Similar to surgical approaches to ventral hernia repair, the definition of a postoperative wound event following ventral hernia repair lacks standardization [1, 3, 11]. Nevertheless, because postoperative wound events following VHR have a significant impact on patient quality of life, hernia repair durability, and on the healthcare economy, it is imperative that hernia surgeons use the same terminology when discussing these events. Therefore, the purpose of this study is to detail the variability of wound event definitions among recent ventral hernia repair literature and to propose standardized definitions of reporting wound events following VHR.
Methods
Following Institutional Review Board (IRB) exemption, the top 50 cited ventral hernia repair peer-reviewed publications from 1995 through 2015 were identified using the Google Scholar search engine using the terms “ventral hernia repair” and “wound event.” Google Scholar is a free website that allows consumers to gauge the visibility and influence of published articles by providing them with the number of other articles that have referenced the specific article searched, a feature that is not available on other commonly used search engines [12]. We chose to use only one search engine as it provided a comprehensive approach for all of the fields we were analyzing, including the year of publication and the number of citations. For each article identified, the definition of wound event used in the paper and the reported wound event incidence was recorded. The definition of wound events was divided into three main categories including: (1) the standardized definitions (SD) group, which included any paper that used the definitions put forth by the Centers for Disease Control and Prevention (CDC), the Ventral Hernia Working Group (VHWG), the American College of Surgeons National Surgery Quality Improvement Program (ACS-NSQIP) database, or the Clavien-Dindo Classification System, (2) the study-specific definitions (SS) group, which included any paper that used its own definition for postoperative wound events, and (3) the no definition (ND) group, which either listed wound event terms, such as cellulitis, hematoma, and seroma, or did not define what was considered a postoperative wound event. In addition to the wound event definitions used in each paper, the number of papers that went on to report the number of wound events that required any procedural intervention and the type of intervention was also recorded.
The standardized definition for SSI as defined by the Centers for Disease Control and Prevention (CDC) is an infection that occurs in the part of the body where the surgery took place and includes superficial, deep, and organ space SSIs [13, 14]. The standardized definition for SSO as defined by the VHWG includes any SSI as well as wound cellulitis, non-healing incisional wound, fascial disruption, skin or soft tissue ischemia, skin or soft tissue necrosis, wound serous or purulent drainage, stitch abscess, seroma, hematoma, infected or exposed mesh, or development of an enterocutaneous fistula [1, 15]. The ACS-NSQIP database uses the CDC definition of SSI and also further categorizes these events into superficial, deep, and organ space SSIs [16]. The Clavien–Dindo Classification System divides postoperative events into five grades [17]. Grade I is any deviation from the expected postoperative course, Grade II is any deviation that requires medical treatment, Grade III is any deviation that requires a procedural intervention, Grade IV is a life-threatening complication such as single or multi-organ failure which requires treatment in the Intensive Care Unit, and Grade V is postoperative mortality [17].
Results
Of the top 50 cited articles reporting wound events following VHR within Google Scholar, the most cited article had 1430 citations while the least cited article had 51 citations (Table 1). The incidence of wound events among the articles ranged from 0.7 to 63.3%. Nine (18%) papers used at least one of the standardized definitions, 14 (28%) used study-specific definitions or generic wound event terms, and 27 (54%) papers listed wound event types but did not include a definition for postoperative wound events.
Of the nine papers in the standardized definitions group, one used the standardized SSI definition, two used the standardized definitions for both SSI and SSO, three used the standardized ACS-NSQIP definitions, two used the Clavien-Dindo Classification System, and one used both the ACS-NSQIP and Clavien-Dindo Classification System. Five (55.6%) of these papers went on to describe the interventions required for management of the postoperative wound events, including percutaneous seroma aspiration and mesh debridement. The highest cited article within the group that reported standardized wound event rates ranked 25th for total citations among the papers included in this analysis with 167 citations and the least cited article within the standard definitions group ranked 49th among the papers included in this analysis with 51 citations.
Of the 14 papers that used study-specific definitions for postoperative wound events, 10 (71.4%) described the interventions required for management of the reported postoperative wound events. These articles used definitions such as discharge of pus from the wound up to one month postoperatively, any infection requiring hospital readmission or debridement, any event that required reopening of the wound, and drainage of pus, isolation of bacteria, or clear signs of local inflammation or infection. Articles in this group ranged from the top cited article with 1430 citations to the 48th article with 54 citations.
Finally, of the 27 papers that simply listed the type of postoperative wound event with no definition, 15 (55.6%) described the interventions required for management of the reported postoperative wound events. The highest cited article within this group ranked 3rd among the papers included in this analysis with 929 citations and the least cited article within this group ranked 50th among the papers included in this analysis with 50 citations.
Discussion
Ventral hernia repair is one of the most commonly performed general surgery operations [2, 10]. Despite the prevalence of ventral hernias, there is a lack of standardization in ventral hernia staging, surgical approach to VHR, and the reporting of outcomes following VHR [2, 10, 11]. This lack of standardization limits comparison across articles currently available in the literature that report outcomes following VHR, as demonstrated by our study. Indeed, our findings demonstrate that 82% of the most cited articles regarding outcomes following VHR do not use a common language to define postoperative wound events. Furthermore, only 50% of peer-reviewed, scientific papers included in our study even defined what a postoperative wound event was. Interestingly, the papers that did use currently established standardized definitions were also within the bottom half of the top cited articles. Finally, the variability in the incidence of wound events among the included articles ranged from 0.7 to 63.3%, which is significantly higher than the previously reported 4–23% [1, 3]. This is likely related to the fact that ventral hernias range from simple to complex and postoperative wound events following VHR occur along a spectrum, from minor to life-threatening events, with some authors reporting all events and some authors only reporting the more severe events. Nevertheless, all these findings support the notion that there is an absence of a common language among hernia surgeons.
The absence of a common language among hernia surgeons has negatively impacted the ability of such surgeons to make accurate comparisons among findings within the literature, to have meaningful conversations at scientific meetings, and can negatively impact surgeon and hospital quality measures [10, 18, 19]. While the findings within each of the identified articles may indeed be accurate for the specific population of interest, the cumulative group of articles has limited capability to provide hernia surgeons information regarding the important perioperative considerations that may impact wound events and leaves the surgeon little ability to reasonably quote surgical site outcomes for individual patients when counseling them on their risks of various hernia procedures. Furthermore, postoperative wound events are a component of hospital and surgeon quality measures [18, 19]. Without standardized definitions for wound events, quality improvement with respect to perioperative management of these patients and surgeon and hospital performance will remain nebulous.
The high variability in the incidence of surgical outcomes is not specific to ventral hernia repair. In fact, in 2005, the International Study Group of Pancreatic Fistula (ISGPF) was created in order to standardize the definition and clinical impact of postoperative pancreatic fistulas with the goal to facilitate a common language amongst pancreatic surgeons, within the literature, and at scientific meetings [20, 21]. Since that time, the classification of postoperative pancreatic fistulas as proposed by the ISGPF has been widely adopted by pancreatic surgeons. While the incidence of postoperative pancreatic fistula remains variable within the literature, two important events have occurred as result of the ISGPF meeting in 2005, including (1) the definitions proposed by the ISGPF have been validated in several follow-up studies and (2) the definitions proposed by the ISGPF have recently been revised to ensure that the stratification of postoperative pancreatic fistulas identifies clinically relevant fistulas only as a means to decrease the variability in the incidence in postoperative pancreatic fistulas [21]. It is our hope that the definitions for postoperative wound events following ventral hernia repair proposed within this manuscript will promote a similar common language and quality improvement process for these definitions amongst hernia surgeons.
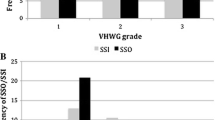
Currently, the CDC definition for SSI, the VHWG definition for SSO, the definitions within the ACS-NSQIP database, and the Clavien–Dindo Classification System have provided some clarity as to the type and severity of postoperative wound events following VHR. Among the nine articles that used the standardized definitions for postoperative wound events, the rate of SSI ranged from 0.8 to 6.6% and the rate of SSO ranged from 45 to 56.3% [22,23,24,25,26,27,28,29,30]. This observation is important for two reasons. First, the range of variability for each outcome is smaller than that for the entire cohort of papers included in this analysis, which may allow for a more clinically meaningful interpretation of these studies. Second, almost half of the articles used the ACS-NSQIP database, which uses the CDC definition for SSI [16]. The ACS-NSQIP database currently includes 885,502 cases from 603 participating institutions and several publications per years are released from this database [16]. The observation that nearly half of the papers that used the standardized definitions for postoperative wound events used the ACS-NSQIP database is reassuring that a call for standardization of wound events following VHR will not impact the current practices of large, national datasets.
Twenty-five (50%) of the articles included in this analysis at least partially describe interventions performed for postoperative wound events following VHR. The description of surgical site occurrences requiring procedural intervention (SSOPI) helps to capture the more clinically significant surgical site occurrences and surgical site infections. In other words, while the Clavien–Dindo Classification System can be used to determine the severity of deviation from a routine postoperative course for all types of surgical procedures, the term SSOPI is more hernia-specific and can be used by hernia surgeons to compare the outcomes of different surgical approaches and prosthetic materials as they relate to the durability of ventral hernia repairs. This notion is supported by a recent study by Yamamoto et al. that determined that significant differences exist between the Clavien–Dindo Classification System and the CDC definition for SSI, which had clinical implications on the type and duration of treatment for postoperative wound events following radical cystectomy [31]. Herein, we propose three standardized terms to define postoperative wound events following VHR: SSI, SSO, and SSOPI. Surgical site infection is a commonly accepted definition amongst surgical specialties, which facilitates easy adoption and interpretation of reported SSI rates. However, SSI is limited in scope, which is why SSO and SSOPI are also proposed- SSO to capture all wound events and SSOPI to identify the clinically relevant surgical site occurrences. The standardized definitions for postoperative wound event reporting following VHR are proposed as follows (Table 2):
-
1.
Surgical Site Infection (SSI)—an infection that occurs in the part of the body where the surgery took place and is further defined as superficial, deep, and organ space SSIs [13, 14].
-
2.
Surgical Site Occurrence (SSO)—any SSI as well as wound cellulitis, non-healing incisional wound, fascial disruption, skin or soft tissue ischemia, skin or soft tissue necrosis, wound serous drainage, seroma, hematoma, or development of an enterocutaneous fistula [1, 15].
-
3.
Surgical Site Occurrence Requiring Procedural Intervention (SSOPI)—any SSO that requires opening of the wound, wound debridement, suture excision, percutaneous drainage, or partial or complete mesh removal [15].
To clarify, any SSI should be included in the total count for surgical site occurrences. However, an SSI or SSO should only be included in the total count for surgical site occurrences requiring procedural intervention if the wound event required some procedural intervention. Following publication of this manuscript, we believe that additional terms that have been used to describe postoperative wounds events following VHR should be replaced by the three aforementioned definitions.
Despite our results, our study does have some limitations. This study used a search engine to identify the top 50 cited ventral hernia repair articles. While this site is commonly used by physicians, it is possible that the number of citations captured within this site is different than other sites that capture the same information, such as Elsevier’s Scopus. Nevertheless, we believe that regardless of the search engine used, there would still be a significant amount of variability amongst the articles with respect to the definitions and incidence of postoperative wound events. Similarly, our search included only the terms “ventral hernia repair” and “wound event” which may have limited our results. However, we felt that these two terms were the most encompassing of the hernia repair cases we were trying to identify. Despite this, if we had used terms such as incisional hernia repair, or abdominal wall hernia repair it is possible that we would have obtained alternative studies. Furthermore, while we attempted to demonstrate consistency amongst articles that use standardized definitions for SSI, SSO, and SSOPI, only a small number of articles currently use this terminology. This may be at least partially explained by the fact that SSOPI is a relatively new definition. Therefore, future studies are needed to expand on the clinical utility of standardized wound event definitions. Finally, while we propose standardized definitions for reporting postoperative wound events following VHR, ultimately the decision to classify a wound event and to intervene on such an event is surgeon dependent, which cannot be accounted for by this study.
Conclusion
Postoperative wound events following VHR are intimately associated with patient quality of life and long-term durability of the hernia repair. Our study demonstrates a significant variability among the definition and incidence of postoperative wound events following ventral hernia repair within the literature. In order for surgeons to be able to make evidence-based decisions regarding ventral hernia management that minimize the risk of postoperative wound events, standardized definitions of SSI, SSO, and SSOPI must be used within the literature. Therefore, we recommend that all future papers that discuss the incidence of postoperative wound events following VHR use the standardized definitions put forth within this article.
References
Poulose BK, Shelton J, Phillips S et al (2012) Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia 16(2):179–183
Ventral Hernia Working Group, Breuing K, Butler CE et al (2010) Incisional ventral hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery 148(3):544–558
Haskins IN, Amdur RL, Lin PP et al (2016) The use of mesh in emergent ventral hernia repair: effects on early patient morbidity and mortality. J Gastrointest Surg 20(11):1899–1903
Baucom RB, Ousley J, Oyefule OO et al (2016) evaluation of long-term surgical site occurrences in ventral hernia repair: implications of preoperative site independent MRSA infection. Hernia 20(5):701–710
Krpata DM, Blatnik JA, Novitsky YW et al (2013) Evaluation of high-risk, comorbid patients undergoing open ventral hernia repair with synthetic mesh. Surgery 153(1):120–125
Fischer JP, Wink JD, Nelson JA et al (2015) wound risk assessment in ventral hernia repair: generation and internal validation of risk stratification system using the ACS-NSQIP. Hernia 19(1):103–111
Finan KR, Cick CC, Kiefe CI et al (2005) Predictors of wound infection in ventral hernia repair. Am J Surg 190(5):676–681
Luijendijk RW, Hop WC, van den Tol MP et al (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343(6):392–398
Cox TC, Blair LJ, Huntington CR et al (2016) The cost of preventable comorbidities on wound complications in open ventral hernia repair. J Surg Res 206(1):214–222
Frangou C (2014) Study reveals staggering costs of ventral hernia repair complication. General Surgery News. http://www.generalsurgerynews.com/In-the-News/Article/01-14/Study-Reveals-Staggering-Costs-of-Ventral-Hernia-Repair-Complication/24813/ses=ogst. Accessed 26 April 2017
Petro CC, O’Rourke CP, Posielski NM et al (2016) Designing a ventral hernia staging system. Hernia 20(1):111–117
Google scholar overview. https://scholar.google.com/intl/en/scholar/metrics.html#metrics. Accessed 19 May 2017
Surgical Site Infection (SSI) (2010) https://www.cdc.gov/hai/ssi/ssi.html. Accessed 26 April 2017
Surgical Site Infection (SSI) (2016) Event. http://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed 26 April 2017
Americas Hernia Society Quality Collaborative (2016) Qualified clinical data registry physician quality reporting system measure specifications. https://www.ahsqc.org/images/uploads/general_images/AHSQC_QCDR_Posting_to_website_4.27.16.pdf. Accessed 26 April 2017
ACS NSQIP participant user file. https://www.facs.org/quality-programs/acs-nsqip/program-specifics/participant-use. Accessed 19 May 2017
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications. Ann Surg 240(2):205–213
Bruce J, Russell EM, Millison J et al (2001) The quality of measurement of surgical wound infection as the basis for monitoring: a systematic review. J Hosp Infect 49:99–108
Leaper D, Tanner J, Kiernan M (2013) Surveillance of surgical site infection: more accurate definitions and intensive recording needed. J Hosp Infect 83:83–86
Bassi C, Dervenis C, Butturini G et al (2005) Postoperative pancreatic fistula: an International Study Group (ISGPF) definition. Surgery 138(1):8–13
Bassi C, Marchegiani G, Dervenis C et al (2017) The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 161(3):584–591
Kim H, Bruen K, Vargo D (2006) Acellular dermal matrix in the management of high-risk abdominal wall defects. Am J Surg 192(6):705–709
Finan KR, Vick CC, Kiefe CI et al (2005) Predictors of wound infection in ventral hernia repair. Am J Surg 190(5):676–681
Itani KM, Hur K, Kim LT et al (2010) Comparisons of laparoscopic and open repair with mesh for the treatment of ventral incisional hernia: a randomized trial. Arch Surg 145(4):322–328
Perrone JM, Soper NJ, Eagon JC et al (2005) Perioperative outcomes and complications of laparoscopic ventral hernia repair. Surgery 138(4):708–715
Choi JJ, Palaniappa NC, Dallas KB et al (2012) Use of mesh during ventral hernia repair in clean-contaminated and contaminated cases: outcomes of 33,832 cases. Ann Surg 255(1):176–180
Stretmitzer S, Bachleitner-Hoffman T, Gradl B et al (2010) Mesh graft infection following abdominal hernia repair: risk factor evaluation and strategies of mesh graft preservation. a retrospective analysis of 476 operations. World J Surg 34(7):1702–1709
Mason RJ, Maozzez A, Sohn HJ et al (2011) Laparoscopic versus open anterior abdominal wall hernia repair: 30-day morbidity and mortality using the acs-nsqip database. Ann Surg 254(4):641–652
Berger RL, Li LT, Hicks SC et al (2013) Development and validation of a risk-stratification score for surgical site occurrence and surgical site infection after open ventral hernia repair. J Am Coll Surg 217(6):974–982
Rogmark P, Pertersson U, Bringman S et al (2013) Short-term outcomes for open and laparoscopic midline incisional hernia repair: a randomized multicenter controlled trial: the ProLOVE (prospective randomized trial of open versus laparoscopic operation of ventral eventrations) trial. Ann Surg 258(1):37–45
Yamamoto T, Takahashi S, Ichihara K et al (2015) How do we understand the disagreement in the frequency of surgical site infection between the CDC and Clavien-Dindo classifications? J Infect Chemother 21:130–133
Author information
Authors and Affiliations
Contributions
INH: study concept, data acquisition, data analysis, data interpretation, manuscript writing. CMH: data acquisition, data analysis, data interpretation, manuscript writing. DMK: study concept, data interpretation, final manuscript review. ASP: study concept, data interpretation, final manuscript review. LT: data interpretation, final manuscript review. AJP: data interpretation, final manuscript writing. SR: data interpretation, final manuscript review. BKP: study concept, data analysis, data interpretation, final manuscript review. MJR: study concept, data analysis, data interpretation, final manuscript review.
Corresponding author
Ethics declarations
Conflict of interest
INH has a Resident Research Grant with the Americas Hernia Society unrelated to this work. ASP has a grant with Intuitive Surgical, receives salary support from Cooper Surgical, Bard Davol, and MedTronic unrelated to this work. BKP has received grant funding from Bard Davol and receives salary support from Artiste Medical, Pfizer, and AHSQC unrelated to this work. MJR is the Medical Director of and receives salary support from the AHSQC and he receives consulting fees from Bard and Gore, and has received grant funding from Miromatrix and Intuitive Surgical, Inc. unrelated to this work. CMH, DMK, LT, AJP and SR declares that they have no conflict of interest.
Ethical approval
No listed author received funding for this study. This study received Institutional Review Board exemption.
Human and animal rights
This study does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Haskins, I.N., Horne, C.M., Krpata, D.M. et al. A call for standardization of wound events reporting following ventral hernia repair. Hernia 22, 729–736 (2018). https://doi.org/10.1007/s10029-018-1748-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-018-1748-6