
Abstract
Introduction
Incisional hernia repair (IHR) carries a high risk of wound complications. Thirty-day outcomes are frequently used in comparative-effectiveness research, but may miss a substantial number of surgical site occurrences (SSO) including surgical site infection (SSI). The objective of this study was to determine an optimal length of follow-up to detect SSI after IHR.
Methods
All adult patients undergoing open IHR at a single academic center over a 3 year period were reviewed. SSIs, non-infectious SSOs, and wound-related readmissions were recorded up to 180 days. The primary outcome was the proportion of SSIs detected at end-points of 30, 60, and 90 days of follow-up. Time-to-event analysis was performed for all outcomes at 30, 60, 90, and 180 days. Logistic regression was used estimate the relative risk of SSI for relevant risk factors.
Results
A total of 234 patients underwent open IHR. Median follow-up time of 102 days. Overall incidence of SSI was 15.8% with median time to occurrence of 23 days. Incidence of non-infectious SSO was 33.2%, and SSO-related readmission was 12.8%. At 30, 60, and 90 days sensitivity was 81.6%, 89.5%, and 92.1 for SSI, and 46.7%, 76.7%, and 83.3% for readmission. In regression analysis, body mass index (RR 1.08, 95% CI 1.00, 1.15, p = 0.04) anterior component separation (RR 4.21, 95% CI 2.09, 6.34, p = 0.003), and emergency surgery (RR 3.25, 95% CI 1.47, 5.02, p = 0.01), were independently associated with SSI after adjusting for age, sex, contamination class, and procedure duration.
Conclusion
A considerable proportion of SSIs occurred beyond 30 days, but 90-day follow-up detected 92% of SSIs. Follow-up to 90 days captured only 83% of SSO-related readmissions. These results have implications for the design of trials evaluating wound complication after open IHR, as early endpoints may miss clinically relevant outcomes and underestimate the number needed to treat. Where possible, we recommend a minimum follow-up of 90 days to estimate wound complications following open IHR.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Incisional hernia repair (IHR) is associated with a high incidence of wound complications [1, 2]. These complications, which include surgical site infection (SSI) and other surgical site occurrences (SSO) can be costly, often requiring protracted wound care or additional interventions, can increase the risk of hernia recurrence, and negatively impact patients’ quality of life [3,4,5,6]. To evaluate interventions designed to prevent these complications, comparative-effectiveness studies rely on accurate classification of wound outcomes. When ascertainment and detection bias threaten the validity of these outcomes, comparative studies tend to overestimate the size of effect [7].
Thirty-day outcomes have frequently been used in the development of risk scores, in surgical quality surveillance, and in studies evaluating novel wound management strategies to reduce the incidence of SSI and other SSO after IHR [8,9,10]. However, cohort studies have reported that a substantial number of deep SSIs and other SSOs occur beyond 30 days [11, 12], suggesting that this time-frame may be inadequate to capture the breadth of clinically relevant outcomes in this population. Although inadequate length follow-up may underestimate the true incidence of wound complications, it may also lead to biased estimates of effect size for interventions in comparative studies.
The objective of this study was to evaluate the validity of 30, 60, and 90 days wound outcomes to identify an appropriate endpoint for follow-up after IHR.
Methods
Design and study population
We performed a retrospective cohort analysis of all open IHRs performed at single university hospital from January 2016 to December 2019. The study was approved by the institution’s Research Ethics Committee, with permission to access patient charts in lieu of individual informed consent. This study received no outside support or industry funding. STROBE reporting guidelines for cohort studies were followed during the study’s conception. With a focus on primarily closed wounds after high-risk repairs, we limited our study to open IHRs, which are associated with a greater incidence of wound complications than laparoscopic hernia repairs [2, 13, 14] or primary ventral hernia repairs [15]. To capture the range of clinical scenarios and SSI risk, we included both emergency and elective cases, as well as contaminated and dirty cases. Duration of follow-up was defined as the time from surgery until the last documented follow-up, up to 180 days.
Surgical technique
Most procedures were performed by one of five surgeons with a practice interest in hernia surgery; however, certain emergency cases were also performed by general surgeons on call. Operative approach and other surgical details (including the use of mesh, component separation, drains, tissue flaps) were at the discretion the operating surgeon. Skin was most often closed with skin clips and abdominal dressings were placed immediately after closure. A sterile dry dressing was applied in most cases, however, a VAC® dressing or a PREVENA™ device (KCI, San Antonio, TX) was applied to primarily closed incisions in select patients at the surgeon’s discretion.
Covariates and outcomes
Routine demographics and comorbidities as per the Charlson comorbidity index (CCI) were collected. Established risk factors for wound complication after ventral hernia repair were also recorded, including smoking exposure, obesity, diabetes mellitus, chronic obstructive pulmonary disease (COPD), immunosuppression (organ-transplant recipients, recent chemotherapy, or steroids), prior hernia repairs, history of wound infection, and stoma [2, 16,17,18]. Patients undergoing elective hernia repair at our institution are counseled regarding smoking cessation. Smoking exposure was defined as a documented history of smoking in the year prior to surgery. Active smokers were documented as still smoking at the time of their preoperative medical evaluation or at the time of surgery. Surgical details included procedure duration, intraoperative complications, blood loss, use of mesh, mesh material, technique of component separation, use of closed suction drains, undermining of subcutaneous tissue (creation of skin flaps), and the use of rotational myocutaneous flaps for tissue coverage (tissue flaps). Mesh position was classified as per consensus classification by Parker et al. [19]. Wound contamination was classified as per definitions by the Centers for Disease Control [20].
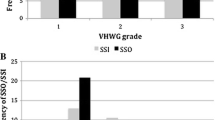
Hernias were labeled as “complex” as per consensus based definition by Slater et al. [21]. Cases were classified using the 3-level modified hernia grading scale (MHGS) proposed by Kanter et al. [17]. The MHGS was adapted from the 4-level Ventral Hernia Working Group (VHWG) grading scale and uses patient-level risk factors and surgical contamination to classify open hernia repairs into three risk grades: grade 1 (low risk); grade 2 (co-morbid patients); and grade 3 (contaminated cases) [22]. The Ventral Hernia Risk Scores (VHRS) for SSI and SSO developed by Berger et al. [18] were also calculated for each case. The VHRS for SSI is a prospectively validated risk score that uses a point system ranging from 0 to 16 to categorize cases into 5 risk strata. The VHRS is calculated based on 6 risk factors (use of a mesh implant, concomitant hernia repair, creation of skin flaps, American Anesthesiologist (ASA) class 3 or greater, body mass index (BMI) 40 or greater, and wound class 4).
The primary outcome was the sensitivity of 30-, 60-, and 90-day endpoints in the detection SSI after open IHR. A total of 180 days of follow-up was used to determine the true incidence of SSI in the cohort, and subsequently used to calculate the sensitivity for the outcome at each end point. The definition of incisional SSI was based on the Centers for Disease Control (CDC) reporting guidelines [20, 23]. These included wound infections diagnosed by the surgical team or wound events involving the deep or superficial tissues of the incision with (1) the presence of purulent drainage, (2) a positive culture in the context of localized or systemic signs or symptoms of wound infection, or (3) abscess or infectious signs identified on imaging.
Secondary outcomes included hospital readmission, non-infectious SSOs, and SSOs requiring procedural intervention (SSOPIs). SSO and SSOPI were reported as per recommendations by Haskins et al. [24]. Non-infectious SSOs included cellulitis, serous drainage from the wound, skin or tissue necrosis, wound dehiscence requiring wound packing or VAC placement, seroma, hematoma, and enterocutaneous fistula. SSOs that occurred as an immediate consequence of an SSI or its treatment were excluded from the definition of non-infectious SSO. SSOPI were recorded as any SSI or SSO necessitating a procedural interventions (reoperation, percutaneous drainage, or other therapeutic procedures) but not antimicrobial therapy alone. Late wound outcomes were defined as events occurring beyond 30 days postoperatively [25].
Data analysis
Statistical analysis was performed in R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria). Time-to-event analysis was performed for outcomes at 30, 60, and 90 days using the Kaplan–Meier method. A subset of established risk factors and risk scores for wound complication after ventral hernia repair were selected a priori and evaluated using multivariate logistic regression for the outcomes of SSI, SSO, SSOPI, and unplanned hospital readmission. Relative risks were computed indirectly using the delta method. The selected variables were age, sex, obesity, contaminated or dirty wound class, technique of component separation, procedure duration, and emergency surgery.
Results
Among 270 patients undergoing ventral hernia repair (VHR) during the study period, 234 patients underwent open IHR (Fig. 1). Among these, 168 (72%) were complex hernia repairs. Median follow-up time was 102 days (IQR 37–264 days). Demographics data and risk factors for SSI are presented in Table 1 and surgical details are presented in Table 2. MHGS and VHRS for SSI and SSO are summarized in Table 3.

Flow chart of participant selection
Wound-related outcomes up to 180 days are presented in Table 4. The incidence of incisional SSI was 15.8% (n = 37) with a median time to SSI of 23 days (IQR 12–30). Most SSIs were superficial (n = 25, 10.7%) or deep (17, 7.3%). Among all SSIs, seven occurred beyond 30 days (18.9% of SSIs) and 21% (n = 8) progressed from a prior SSO occurring within 30 days. All late SSIs involved comorbid patients who underwent complex IHR and only two late SSIs (28.6%) progressed from a prior SSO.
The incidence of any wound complication including SSI was 40.6% (n = 95). Non-infectious SSO was 33.2% (n = 77) with a median time of 22 days (IQR 12–34). Seroma (n = 59, 25.1%) and wound dehiscence (n = 18, 7.7%) were the most common. Of all non-infectious SSOs, 33.7% (n = 26) occurred beyond 30 days. The incidence of SSOPI was 15.8% (n = 37) with a median time of 25 days (IQR 13–47). Opening of the wound was performed in 19 patients, percutaneous drainage in 18 patients, and 11 patients required operative debridement. Among 198 patients undergoing open IHR with permanent synthetic or slowly resorbing mesh, 7 patients (4%) had the mesh removed due to wound complication.
The sensitivity for outcomes as follow-up was extended from 30 to 60 and 90 days are presented in Table 5. Among 37 SSIs at 180 days, 81.6% (n = 30) were diagnosed at 30 days, 89.5% (n = 33) at 60 days, and 92.1% (n = 35) at 90 days. Among patients experiencing any SSO, 31.6% (n = 30) were readmitted within 180 days and follow-up beyond 120 days was required to detect at least 90% of these readmissions. The Kaplan–Meier Curves for these outcomes is shown in Fig. 2.

Kaplan–Meier curves for SSI, SSO, SSOPI, readmission. Kaplan–Meier curves showing cumulative probability of follow-up up to 90 days without, a surgical site infection (SSI), b surgical site occurrence (SSO), c surgical site occurrence requiring procedural intervention (SSOPI), and d hospital readmission for SSO-related complications
In multivariate regression analysis, BMI [RR 1.08, 95% CI (1.00, 1.15), p = 0.04], emergency surgery [RR 3.25, 95% CI (1.47, 5.02), p = 0.01], and anterior component separation [RR 4.21, 95% CI (2.09, 6.34), p = 0.003] were independently associated with SSI after adjusting for age, sex, obesity, wound contamination, procedure duration, and emergency surgery. No associations were found for non-infectious SSOs. BMI [RR 1.17, 95% CI (1.07, 1.27), p = 0.001], anterior component separation [RR 3.62, 95% CI (1.83. 5.41), p = 0.004], and procedure duration [RR 1.29, 95% CI (1.43, 1.53), p = 0.02] were independently associated with SSOPI. BMI [RR 1.12, 95% CI (1.02, 1.22), p = 0.02], and anterior component separation [RR 5.15, 95% CI (2.14, 8.16), p = 0.007] were independently associated with wound-related readmissions. The adjusted relative risks estimated from logistic regression models for all outcomes are presented in Table 6.
Discussion
Clinical-effectiveness studies rely on accurate outcome ascertainment in the evaluation of new interventions. In this analysis of wound outcomes in 234 patients undergoing open IHRs, a considerable proportion of SSIs and SSOs occurred beyond 30 days. Only 81% of SSIs and 66% of non-infectious SSOs occurring within the first 6 months after surgery were detected at 30 days. However, with follow-up extended to 90 days, 92% of SSIs and 97% of other SSOs were detected. Only 83% of SSO-related hospital readmissions were detected at 90 days, and follow-up beyond 120 days was required to detect at least 90% of these readmissions. This information has important implications for the design of future studies comparing the effectiveness of interventions to prevent SSI and SSO after open IHR, as the traditional 30-day endpoint will likely underestimate these outcomes.
Other studies have evaluated the follow-up and natural history of wound complications after open VHR. In a retrospective evaluation of long-term wound outcomes following 632 clean hernia repairs, Baucom et al. reported that 30% of all SSOs occurred after thirty days in their cohort [26]. In a review of 1635 primary and IHRs—including emergent, and contaminated or dirty cases—Holihan et al. reported that 7.2% of cases developed SSI, of which 17.1% percent occurred beyond thirty days [11]. Notably, no risk factors were predictive of late vs. early SSI, with late infections developing even after simple repairs of primary hernias, and in patients without significant comorbidities or risk factors. In contrast, late SSIs in our cohort occurred only among comorbid patients undergoing complex open IHR. While approximately 20% of all SSIs progressed from a prior SSO, only two patients with SSIs beyond 30 days (SSI diagnosed on day 63 and 96) had developed an SSO within the first 30 days of follow-up (SSO diagnosed on day 28 and 21, respectively), suggesting that the absence of SSO in the early follow-up period does not definitively rule out the occurrence of a late SSI.
In 2013, the CDC and NHSN updated the surveillance protocols for deep surgical site infection, modifying the reporting period to 90 days for selected procedures, including herniorrhaphy [20, 27]. Superficial incisional SSIs continue to be reported up to 30 days as per CDC definitions. The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) collects outcomes up to 30 days, including SSIs [28]. Many hernia-specific registries, including the European Registry of Abdominal Wall Hernias (EuraHS) and the Americas Hernia Society Quality Collaborative (AHSQC) require the reporting of 30-day “early” outcomes, but also include non-clinical follow-up to detect outcomes beyond 30 days [29,30,31]. Similarly, the European Hernia Society encourages the reporting of early and late wound outcomes, distinguishing late outcomes as those occurring after 30 days. Our results support the use of late outcomes in the design of comparative-effectiveness studies evaluating interventions to prevent SSO and SSI after open IHR.
These findings have implications for studies designed to investigate interventions to improve outcomes of VHR. The use of incisional negative pressure wound therapy (iNPWT) in high-risk patients undergoing VHR has been the focus of several retrospective and non-randomized prospective cohort studies [8, 32,33,34]. We recently reported results of a retrospective matched cohort study favoring an effect of iNPWT in the prevention of deep and superficial SSI after complex IHR at 30 days [35]. The estimated effect was consistent with prior studies of iNPWT in this high-risk population; however, the effect was no longer significant with follow-up up to 180 days. To our knowledge, only a single randomized controlled trial has since been published evaluating iNPWT after VHR [36]. This RCT supported an effect of iNPWT in reducing SSI, but only reported outcomes up to 30 days and was at risk of bias because outcome assessors were not blinded to the treatment status of the participants. At least another two prospective randomized trials are registered or underway [37, 38]. These include a study with 30-day wound outcomes, and a study with 3-month wound outcomes, quality of life, and cost outcomes. Based on the results of the present study, as well as the others mentioned above [11, 26], the appropriate follow-up duration should be at least 90 days, and it would be interesting for these trials to report effectiveness at the different follow-up timepoints to evaluate for differential detection bias due to early end-points. Appropriate follow-up for wound-related hospital readmission may be longer still, perhaps beyond 120 days, which was required to capture 90% of wound-related readmissions in our cohort.
Our study is limited by its retrospective design and lack of prospective and systematic follow-up beyond routine clinical care. Although best practices to prevent SSIs—including the administration of perioperative antibiotics, antiseptic technique, prevention hypothermia, and maintenance of euglycemia—are routinely followed at our institution, adherence to these practices were not routinely measured. These and other unmeasured confounders may have influenced the results. Patients are routinely followed-up within 4–6 weeks after surgery. If no complications are noted, many patients are followed on an as-needed basis or for symptomatic recurrence, with significant variability between surgeons. Variability in follow-up may introduce bias, in that patients who do not experience a wound complication may have less documented follow-up. Our institution also services a large geographical area, and there may be patients whose SSOs were diagnosed outside our center. However, given the practice patterns in our clinical context, these patients would have likely been transferred to our institution for definitive management. Our study is limited by sample size and number of events. With limited statistical power, we could only include a subset of clinically relevant variables in the multivariate regression analysis. Certain variables such as diabetes, smoking, immunosuppression, prior wound infection, the use of closed suction drains, mesh position, mesh material, and the creation of skin flaps were not directly adjusted for in regression analysis. However, these factors did not behave as predictors or confounders when included individually in multivariate regression (not reported). We also noted a change in clinical practices during the study period, with a growing preference for transversus abdominis release versus anterior component separation, which was not accounted for.
Conclusion
A considerable proportion of SSIs occurred beyond 30 days after open IHR. A 30 days SSI outcome detected only 81% of SSIs occurring within 6 months of open IHR; however, sensitivity improved to 92% by 90 days of follow-up. Early endpoints may miss clinically relevant outcomes after open IHR and studies without longer follow-up should be interpreted with this limitation in mind. These results have implications for the design of trials evaluating interventions to prevent SSI and SSO after open IHR. We recommend at least 90 days of follow-up for these outcomes after open IHR.
References
Helgstrand F, Rosenberg J, Kehlet H, Jorgensen LN, Bisgaard T (2013) Nationwide prospective study of outcomes after elective incisional hernia repair. J Am Coll Surg 216:217–228
Kaoutzanis C, Leichtle SW, Mouawad NJ, Welch KB, Lampman RM, Wahl WL, Cleary RK (2015) Risk factors for postoperative wound infections and prolonged hospitalization after ventral/incisional hernia repair. Hernia 19:113–123
van Ramshorst GH, Eker HH, Hop WCJ, Jeekel J, Lange JF (2012) Impact of incisional hernia on health-related quality of life and body image: a prospective cohort study. Am J Surg 204:144–150
Plymale MA, Davenport DL, Walsh-Blackmore S, Hess J, Griffiths WS, Plymale MC, Totten CF, Roth JS (2020) Costs and complications associated with infected mesh for ventral hernia repair. Surg Infect 21:344–349
Cox TC, Blair LJ, Huntington CR, Colavita PD, Prasad T, Lincourt AE, Heniford BT, Augenstein VA (2016) The cost of preventable comorbidities on wound complications in open ventral hernia repair. J Surg Res 206:214–222
Lauren Paton B, Novitsky YW, Zerey M, Sing RF, Kercher KW, Todd Heniford B (2007) Management of infections of polytetrafluoroethylene-based mesh. Surg Infect 8:337–342
Miller JN, Colditz GA, Mosteller F (1989) How study design affects outcomes in comparisons of therapy. II: surgical. Stat Med 8:455–466
Poruk KE, Hicks CW, Trent Magruder J, Rodriguez-Unda N, Burce KK, Azoury SC, Cornell P, Cooney CM, Eckhauser FE (2017) Creation of a novel risk score for surgical site infection and occurrence after ventral hernia repair. Hernia 21:261–269
Burkhart RA, Javed AA, Ronnekleiv-Kelly S, Wright MJ, Poruk KE, Eckhauser F, Makary MA, Cameron JL, Wolfgang CL, He J, Weiss MJ (2017) The use of negative pressure wound therapy to prevent post-operative surgical site infections following pancreaticoduodenectomy. HPB 19:825–831
Pauli EM, Krpata DM, Novitsky YW, Rosen MJ (2013) Negative pressure therapy for high-risk abdominal wall reconstruction incisions. Surg Infect 14:270–274
Holihan JL, Flores-Gonzalez JR, Mo J, Ko TC, Kao LS, Liang MK (2017) How long is long enough to identify a surgical site infection? Surg Infect 18:419–423
Lankiewicz JD, Yokoe DS, Olsen MA, Onufrak F, Fraser VJ, Stevenson K, Khan Y, Hooper D, Platt R, Huang SS (2012) Beyond 30 days: does limiting the duration of surgical site infection follow-up limit detection? Infect Control Hosp Epidemiol 33:202–204
Kroese LF, Kleinrensink G-J, Lange JF, Gillion J-F, Ain J-F, Beck M, Barrat C, Berney C, Berrod J-L, Binot D, Boudet M-J, Bousquet J, Blazquez D, Bonan A, Cas O, Champault-Fezais A, Chastan P, Cardin J-L, Chollet J-M, Cossa J-P, Dabrowski A, Démaret S, Drissi F, Durou J, Dugue T, Faure J-P, Framery D, Fromont G, Gainant A, Gauduchon L, Genser L, Gillion J-F, Guillaud A, Jacquin C, Jurczak F, Khalil H, Lacroix A, Ledaguenel P, Lepère M, Lépront D, Letoux N, Loriau J, Magne E, Ngo P, Oberlin O, Paterne D, Pavisd’Escurac X, Potiron L, Renard Y, Soler M, Rignier P, Roos S, Thillois J-M, Tiry P, Verhaeghe R, Vu P, Zaranis C (2018) External validation of the European hernia society classification for postoperative complications after incisional hernia repair: a cohort study of 2,191 patients. J Am Coll Surg 226:223–229
Kokotovic D, Bisgaard T, Helgstrand F (2016) Long-term recurrence and complications associated with elective incisional hernia repair. JAMA 316:1575–1582
Holihan JL, Alawadi Z, Martindale RG, Roth JS, Wray CJ, Ko TC, Kao LS, Liang MK (2015) Adverse events after ventral hernia repair: the vicious cycle of complications. J Am Coll Surg 221:478–485
Fischer JP, Wink JD, Nelson JA, Kovach SJ 3rd (2014) Among 1,706 cases of abdominal wall reconstruction, what factors influence the occurrence of major operative complications? Surgery 155:311–319
Kanters AE, Krpata DM, Blatnik JA, Novitsky YM, Rosen MJ (2012) Modified hernia grading scale to stratify surgical site occurrence after open ventral hernia repairs. J Am Coll Surg 215:787–793
Berger RL, Li LT, Hicks SC, Davila JA, Kao LS, Liang MK (2013) Development and validation of a risk-stratification score for surgical site occurrence and surgical site infection after open ventral hernia repair. J Am Coll Surg 217:974–982
Parker SG, Halligan S, Liang MK, Muysoms FE, Adrales GL, Boutall A, de Beaux AC, Dietz UA, Divino CM, Hawn MT, Heniford TB, Hong JP, Ibrahim N, Itani KMF, Jorgensen LN, Montgomery A, Morales-Conde S, Renard Y, Sanders DL, Smart NJ, Torkington JJ, Windsor ACJ (2020) International classification of abdominal wall planes (ICAP) to describe mesh insertion for ventral hernia repair. Br J Surg 107:209–217
Centers for Disease Control (2019) National Healthcare Safety Network Surveillance (NHSN) patient safety component manual 2019. Centers for Disease Control, Atlanda
Slater NJ, Montgomery A, Berrevoet F, Carbonell AM, Chang A, Franklin M, Kercher KW, Lammers BJ, Parra-Davilla E, Roll S, Towfigh S, van Geffen E, Conze J, van Goor H (2014) Criteria for definition of a complex abdominal wall hernia. Hernia 18:7–17
Ventral Hernia Working Group, Breuing K, Butler CE, Ferzoco S, Franz M, Hultman CS, Kilbridge JF, Rosen M, Silverman RP, Vargo D (2010) Incisional ventral hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery 148:544–558
Berríos-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, Reinke CE, Morgan S, Solomkin JS, Mazuski JE, Dellinger EP, Itani KMF, Berbari EF, Segreti J, Parvizi J, Blanchard J, Allen G, Kluytmans JAJW, Donlan R, Schecter WP, Committee HICPA (2017) Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg 152:784–791
Haskins IN, Horne CM, Krpata DM, Prabhu AS, Tastaldi L, Perez AJ, Rosenblatt S, Poulose BK, Rosen MJ (2018) A call for standardization of wound events reporting following ventral hernia repair. Hernia 22:729–736
Muysoms FE, Deerenberg EB, Peeters E, Agresta F, Berrevoet F, Campanelli G, Ceelen W, Champault GG, Corcione F, Cuccurullo D, DeBeaux AC, Dietz UA, Fitzgibbons RJ Jr, Gillion JF, Hilgers R-D, Jeekel J, Kyle-Leinhase I, Köckerling F, Mandala V, Montgomery A, Morales-Conde S, Simmermacher RKJ, Schumpelick V, Smietański M, Walgenbach M, Miserez M (2013) Recommendations for reporting outcome results in abdominal wall repair: results of a consensus meeting in Palermo, Italy, 28–30 June 2012. Hernia 17:423–433
Baucom RB, Ousley J, Oyefule OO, Stewart MK, Phillips SE, Browman KK, Sharp KW, Holzman MD, Poulose BK (2016) Evaluation of long-term surgical site occurrences in ventral hernia repair: implications of preoperative site independent MRSA infection. Hernia 20:701–710
Centers for Disease Control and Prevention (2022) Procedure-associated Module: Surgical Site Infection. National Healthcare Safety Network. https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf
American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) (2018) User Guide for the 2017 ACS NSQIP Participant Use Data File (PUF). ACS NSQIP. https://www.facs.org/qualityprograms/acs-nsqip/participant-use
Sun BJ, Kamal RN, Lee GK, Nazerali RS (2018) Quality measures in ventral hernia repair: a systematic review. Hernia 22:1023–1032
Bernardi K, Liang MK (2019) Establishing a hernia program. In: Davis SS, Dakin G, Bates A (eds) The SAGES manual of hernia surgery. Springer, Cham, pp 595–610
Muysoms F, Campanelli G, Champault GG, DeBeaux AC, Dietz UA, Jeekel J, Klinge U, Köckerling F, Mandala V, Montgomery A, Morales Conde S, Puppe F, Simmermacher RKJ, Śmietański M, Miserez M (2012) EuraHS: the development of an international online platform for registration and outcome measurement of ventral abdominal wall hernia repair. Hernia 16:239–250
Hicks CW, Poruk KE, Baltodano PA, Soares KC, Azoury SC, Cooney CM, Cornell P, Eckhauser FE (2016) Long-term outcomes of sandwich ventral hernia repair paired with hybrid vacuum-assisted closure. J Surg Res 204:282–287
Soares KC, Baltodano PA, Hicks CW, Cooney CM, Olorundare IO, Cornell P, Burce K, Eckhauser FE (2015) Novel wound management system reduction of surgical site morbidity after ventral hernia repairs: a critical analysis. Am J Surg 209:324–332
Tran BNN, Johnson AR, Shen C, Lee BT, Lee ES (2019) Closed-incision negative-pressure therapy efficacy in abdominal wall reconstruction in high-risk patients: a meta-analysis. J Surg Res 241:63–71
Hopkins B, Eustache J, Ganescu O, Cipolla J, Kaneva P, Fried GM, Khwaja K, Vassiliou M, Fata P, Lee L, Feldman LS (2020) S116: Impact of incisional negative pressure wound therapy on surgical site infection after complex incisional hernia repair: a retrospective matched cohort study. Surg Endosc. https://doi.org/10.1007/s00464-020-07857-1
Bueno-Lledó J, Franco-Bernal A, Garcia-Voz-Mediano MT, Torregrosa-Gallud A, Bonafé S (2020) Prophylactic single-use negative pressure dressing in closed surgical wounds after incisional hernia repair: a randomized, controlled trial. Ann Surg. https://doi.org/10.1097/SLA.0000000000005271
Kajmolli A, Mcguirk M (2020) Assess the efficacy of prevena plus vs SOC to closed incision in Pts undergoing CAWR and other laparotomy procedures. Identifier NCT: 04539015. https://clinicaltrials.gov/ct2/show/NCT04539015. Accessed 10 Nov 2020
How NE, Blewett CE (2020) Negative pressure incisional wound therapy for high-risk ventral hernia repair. Identifier NCT04455724. https://clinicaltrials.gov/ct2/show/NCT04455724. Accessed 10 Nov 2020
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Feldman has received educational Grants from Merck. Dr. Lee has received an investigator-initiated research Grant from Johnson & Johnson. Drs. Hopkins, Eustaches, Fiore, Ganescu, and Cipolla have no conflict of interest or financial ties to disclose. Ms. Kaneva have no conflict of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hopkins, B., Eustache, J., Ganescu, O. et al. At least ninety days of follow-up are required to adequately detect wound outcomes after open incisional hernia repair. Surg Endosc 36, 8463–8471 (2022). https://doi.org/10.1007/s00464-022-09143-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09143-8