
Abstract
Purpose
It has been estimated in the UK that 27 % of men and 3 % of women will undergo an inguinal hernia repair (IHR) during their lifetimes. However, no epidemiologic study investigating IHR has been performed to date in an Asian population. The present study explored the incidence and recurrence of IHR in an Asian population using a nation-wide population-based dataset in Taiwan.
Methods
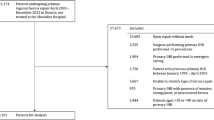
Based on the National Health Insurance Database, we identified 5806 patients who underwent an IHR between 2000 and 2010 and followed them until they had a recurrence, died during hospitalization, left the program, or the study ended. We calculated the age-stratified recurrence rates and used Cox proportional hazards to explore the influence of demographic and clinical factors on recurrence. We also plotted IHR occurrence over the study period.
Results
Among the 5806 sampled subjects who had an IHR, 565 (9.73 %) had an IHR recurrence yielding an overall incidence of 18.23 per 1000 person-years. The hazard ratios for recurrence increased with age, and were greater among men and blue collar workers. The incidence of IHR decreased from 168.21 to 92.10 per 100,000 person-years over the study period. Surgical complication rates ranged between 0.16 and 2.57 %.
Conclusions
On account of the increased risk of recurrence with age, young hernia patients may not want to delay surgery. This study detected a decreasing trend in initial IHR rates, confirming similar trends reported in Western countries. However, the incidence of initial IHR is lower in Taiwan than it is in the West.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia has been reported to have a lifetime prevalence of 27 % among men and 3 % among women in the UK [1], making inguinal hernia repair (IHR) the most frequently performed operation in general surgery [2–5]. While a common operation, IHR is noted to carry a substantial risk for recurrence. In one study assessing hernia recurrence in eight Swedish hospitals it was found that among 4879 hernia operations performed over 3 years, 16 % were done for recurrences [6]. A follow-up investigation, also conducted in Sweden, reported similar results with recurrence rates ranging between 10 and 15 % 3 years after operation depending on the definition of recurrence and completeness of the physical examination [7]. Thus, the possibility of recurrence, and therefore the sheer number of patients suffering a recurrence, is quite high.
Studies conducted using Scandinavian hernia registries have also identified several factors to be risk factors for recurrence, such as BMI [8], operating time [9], and method of hernia repair [10]. The same datasets have been used to identify age as a risk factor for primary hernia [11]. However, no study to date has been performed assessing the age-stratified risk of hernia recurrence [1, 2, 12–16].
There is substantial geographic variation in the incidence of IHR in the literature. The average incidence between 1989 and 2008 in Olmsted County, MN, has been reported to be 200.1 per 100,000 person-years, but during a similar time frame rates as high as 340 per 100,000 person-years were reported in Italy [16], and rates as low as 160.69 per 100,000 person-years have been detected in Denmark [15]. Additionally, the study conducted in Olmsted County, MN, also detected substantial decreases in the incidence of both initial and recurrent IHR over the course of their study [2]. Despite the geographic variation of IHR in the literature, and the changing epidemiology reported by the study conducted in Olmsted County, no study to date has explored IHR in an Asian population. Moreover, as IHR has been suggested to be used as an indicator of surgical quality [16], the results of studies assessing IHR in Asian populations could also be used to gauge the surgical quality of those countries’ medical systems.
Therefore, in order to quantify age as a risk factor for recurrence and explore the clinical epidemiology of IHR in an Asian population, this study set out to characterize IHR incidence over time, as well as provide age-stratified risk estimates for its recurrence utilizing a nation-wide population-based dataset in Taiwan.
Materials and methods
Data source
The National Health Insurance Research Database (NHIRD) contains all the outpatient and inpatient claims in Taiwan accrued between 1996 and 2010. This database was derived from the Taiwan National Health Insurance Program and is maintained by the National Health Research Institute. This insurance program included over 96 % of Taiwan population in 2000. Our study used a Longitudinal Health Insurance Database (LHID2000), a part of the NHIRD, containing one million beneficiaries randomly selected from the Registry for beneficiaries in 1996–2000. On account of the Personal Information Protection Act, the identification numbers of the beneficiaries were re-coded prior to release to researchers. This study was approved by the Institutional Review Board of the China Medical University Hospital, Taiwan. The diseases and conditions studied in this investigation were identified in the NHIRD based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
Study subjects and outcome
We sourced all the adult patients (age ≥18 years of age) who received an IHR between 2000 and 2010 from the LHID2000 and used this value (numerator) along with the total number of people at risk for IHR in the LHID2000 (denominator) to calculate the incidence of IHR in the adult population of Taiwan. As the LHID2000 was randomly sampled from the overall population of Taiwan and contains one million beneficiaries, the incidence should be a stable estimate of the overall incidence in Taiwan. The date of the IHR was defined as the index date. All the study subjects were followed from the index date to the recurrence of hernia (ICD-9-CM: 550.X1 and 550.X3) or recurrence of IHR. If patients did not suffer a recurrence, they were followed to the end of 2010, hospitalized death, or loss from the program, whichever came first.
Variables of interest
The risk factors adjusted for in this study included patient, hospital, and physician characteristics. The patients’ demographic characteristics included age (18–29, 30–39, 40–49, 50–59, and ≥60 years), gender, occupation (white collar, blue collar, and others), treatment for hernia (open with or without mesh), and length of stay for hernia. Patient occupation was classified into three types based on working place: indoor workers were defined as white collar; outdoor workers were defined as blue collar; and low income earners and clergy were defined as others. Hospital characteristics included the level of the hospital (medical center, regional hospital, district hospital/clinic). These institutions are classified according to their departments and what services they offer. To reduce the burden of larger medical centers, patients are encouraged to first attend clinics and district hospitals before working their way up to the more specialized care available at regional hospitals and medical centers. Physicians’ characteristics included age, gender, time of clinical practice, and number of hernia operations per year. While the cutoff point for number of hernia operations per year was 1.5, this figure reflects how many times a surgeon performed an operation on this pool of patients. As this pool of patients was drawn from 1,000,000 randomly sampled Taiwanese, and the current population is about 23,000,000, this figure should be about 1/23rd of the actual number of cases performed by that surgeon, or approximately 34.5 cases.
Statistical analysis
All statistical analyses were performed using SAS 9.3 software for windows (SAS Institute, Cary, NC, USA). The significance level was set at 0.05 in this study. We used Cox proportional hazards regressions to estimate the risk of IHR and its associated factors.
Results
The average age of subjects was 55.4 years (standard deviation, SD = 18.5). The majority were men (89.4 %), with the greatest proportion holding white collar jobs (45.0 %). Open repair with mesh was the major mode of treatment (95.6 %) and the median length of stay was 2 days (interquartile range 1.00). Most patients with hernia were diagnosed in clinics (39.9 %). The average age and practice time of the diagnosing physician was 46.3 and 12.1 years (SD = 8.18 and 5.35) (Table 1).
During the 11-year study period, a total of 565 patients with hernia had a reoccurrence (9.73 %) with an incidence of 18.23 per 1000 person-years. The incidence of recurrence increased with age from 7.11 per 1000 person-years between the ages of 18 and 29 years to 24.61 per 1000 person-years among those aged over 60 years (Table 2).
Table 3 includes the hazard ratios (HRs) for hernia recurrence among the sampled patients. Compared with the youngest patients (18–29 years old), the HR for recurrence increased with age. After adjusting for the demographic characteristics, and hospital and physician characteristics significant in the univariate analysis, patients aged 30–39 years were found to be at 1.68 (95 % CI 1.07–2.65) times the risk of the youngest age group to suffer a recurrence, while patients aged over 60 years were 2.76 (95 % CI 1.90–3.99) times more likely than the youngest age group to suffer a recurrence.
Figure 1 plots the incidence and prevalence of hernia over the study period (2000–2010). The prevalence decreased from 250.17 to 210.14 per 100,000 person-years, and the incidence decreased from 168.21 to 92.10 per 100,000 person-years. The average incidence over the study period was 124.86 per 100,000 person-years.

Incidence and prevalence for inguinal hernia repair in Taiwan between 2000 and 2010
Discussion
This population-based study exploring IHR in Taiwan detected greater risks for recurrence with increasing age. We also detected a decreasing trend in the occurrence of IHR in Taiwan, with IHR seeming to be performed much less frequently in Taiwan than in most of the Western countries whose data was reported the literature.
Many patients with hernia may delay treatment until it becomes a necessity on account of the risk of recurrence IHR has been demonstrated to carry [17–21]. While small-scaled studies have been conducted to ascertain the safety of the “Watchful Waiting” strategy for IHR [17], hernias do not heal spontaneously and are prone to grow larger over time. Therefore, it is possible that “Watchful Waiting” is simply delaying the inevitable. But, in contrast to the numerous studies in the literature assessing many of the epidemiological facets of hernia in Western populations [1–5, 8–11, 15, 16], the literature boasts little in the way of population-based evidence assessing the risk for hernia recurrence [6, 7], with no such studies having been conducted on IHR or hernia in an Asian population.
Furthermore, while age is a known risk factor for hernia recurrence [22], no population-based studies have provided age-specific risk estimates, leaving patients with hernia unsure of the risk of recurrence they may face should they choose to undergo an operation. We feel that the results of this population-based study demonstrating substantial increases in the adjusted risk of recurrence with age may encourage young patients suffering from hernia to avoid delays and receive surgical treatment while their risk of recurrence is at its lowest.
In addition to age, we also found occupation to also play a role in the recurrence of hernia. In this study, blue collar workers were at 1.24 times the risk of white collar workers for recurrence. Blue collar workers may be more economically disadvantaged, and therefore may be more likely to return to work prior to properly recuperating from surgery. Blue collar workers also engage in more strenuous physical activity, which is not advised to avoid recurrence, and although controversial [12, 23] has been suggested to be a risk factor for initial hernia [24].
While we feel confident that our results demonstrate high internal validity, these findings may not hold for other populations which seem to have substantially different incidence rates. Between 2000 and 2010, the average annual incidence rate of IHR in Taiwan was 124.86 per 100,000 persons. However, a population-based study conducted in Olmstead county, MN, USA, reported an overall incidence rate among adults of 200.1 per 100,000 person-years over the course of their study (1989–2008) [2]. A study performed in the Emilia-Romagna region of Italy captured all the IHR conducted in both public and private hospitals among patients older than 14 years of age between 2000 and 2009 and reported an average of 340 IHR per 100,000 person-years [16]. The lowest reported IHR incidence rate reported in a Western population was detected in Denmark. That study utilized data from the Civil Registration System covering all Danish citizens. During their 5-year study, 45,315 of 5,639,885 Danes underwent an IHR, yielding an incidence rate of 160.69 per 100,000 person-years [15].
Interestingly, while the incidence of IHR varied substantially between this study and those conducted in Western populations, the decreasing trend observed in Olmstead County, MN, by Zendejas et al. [2] was also noted in this investigation. In Taiwan, there was a substantial decline in the incidence of IHR over the study period, with the incidence decreasing from 168.21 to 92.10 per 100,000 person-years between 2000 and 2010. In Olmstead county, the incidence rate in adult men decreased from 474.1 per 100,000 person-years in 1989 to 372.5 person-years in 2008 [2].
Zendejas et al. proposed that there are likely several factors contributing to the decreasing incidence of hernia in Olmsted County which are also likely to support this trend in Taiwan. One is a rise in the proportion of individuals that are obese or overweight. The obesity rate in Taiwan has been increasing [25, 26], and obese people have been shown to have a lower incidence of IHR [17, 27]. However, they have also been demonstrated to have a greater risk of recurrence [8]. Another factor is the recent decrease in smoking in Taiwan [28, 29], which although controversial [12, 24] has been suggested to be a risk factor for hernia and hernia recurrence [11, 30]. However, the effects of an aging population in both Olmstead County and Taiwan [2, 29, 31] should work to increase the incidence of hernia.
The results of this study need to be seen in light of several limitations. First, all the data analyzed in this study was acquired from an administrative database and may not be as accurate as data collected prospectively according to standardized procedures. For example, as patients were followed until the date that a recurrent hernia became present or a recurrence necessitated an operation, only symptomatic recurrent hernias would have been assessed in this study while asymptomatic hernia recurrences would not have been included in the health insurance database or this analysis.
Second, the limitations of this administrative dataset also precluded us from investigating the effects of some factors on the individual level. These included BMI and smoking status, whose respective increase and decrease may have contributed to the decreasing trend in IHR observed in this study [17, 25, 26].
Third, as we had no measure for the severity or size of the hernias among the subjects in this study, we were also unable to consider how hernia size influences the risk of recurrence and complications.
References
Primatesta P, Goldacre MJ (1996) Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol 25:835–839
Zendejas B, Ramirez T, Jones T et al (2013) Incidence of inguinal hernia repairs in Olmsted County, MN: a population-based study. Ann Surg 257:520–526
Pokorny H, Klingler A, Schmid T et al (2008) Recurrence and complications after laparoscopic versus open inguinal hernia repair: results of a prospective randomized multicenter trial. Hernia 12:385–389
Phillips W, Goldman M (2004) Groin Hernia. Health care needs assessment, the epidemiologically based needs assessment reviews. First series, vol 1, 2nd edn. Radcliffe Publishing UK
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362:1561–1571
Nilsson E, Kald A, Anderberg B et al (1997) Hernia surgery in a defined population: a prospective 3 year audit. Eur J Surg 163:823–829
Haapaniemi S, Nilsson E (2002) Recurrence and pain 3 years after groin hernia repair. Validation of postal questionnaire and selective physical examination as a method of follow-up. Eur J Surg 168:22–28
Rosemar A, Angerås U, Rosengren A, Nordin P (2010) Effect of body mass index on groin hernia surgery. Ann Surg 252:397–401
van der Linden W, Warg A, Nordin P (2011) National register study of operating time and outcome in hernia repair. Arch Surg 146:1198–1203
Magnusson N, Nordin P, Hedberg M, Gunnarsson U, Sandblom G (2010) The time profile of groin hernia recurrences. Hernia 14:341–344
Sorensen LT, Hemmingsen UB, Kirkeby LT, Kallehave F, Jorgensen LN (2005) Smoking is a risk factor for incisional hernia. Arch Surg 140:119–123
Ruhl CE, Everhart JE (2007) Risk factors for inguinal hernia among adults in the US population. Am J Epidemiol 165:1154–1161
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am 83:1045–1051
Abramson JH, Gofin J, Hopp C et al (1978) The epidemiology of inguinal hernia. A survey in western Jerusalem. J Epidemiol Community Health 32:59–67
Burcharth J, Pedersen M, Bisgaard T et al (2013) Nationwide prevalence of groin hernia repair. PLoS One 8:e54367
Ansaloni L, Coccolini F, Fortuna D et al (2014) Assessment of 126,913 inguinal hernia repairs in the Emilia-Romagna region of Italy: analysis of 10 years. Hernia 18:261–267
Fitzgibbons RJ Jr, Giobbie-Hurder A, Gibbs JO et al (2006) Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA 295:285–292
Oberlin P, Boudet MJ, Vyrieres M et al (1995) French Associations for Surgical Research. Recurrence after inguinal hernia repair: prognostic facts in a prospective study of 1706 hernias. Br J Surg 82(suppl 1):65
Neumayer L, Giobbie-Hurder A, Jonasson O et al (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350:1819–1827
Bay-Nielsen M, Thomsen H, Andersen FH et al (2004) Convalescence after inguinal herniorrhaphy. Br J Surg 91:362–367
Cunningham J, Temple WJ, Mitchell P et al (1996) Cooperative Hernia Study. Pain in the postrepair patient. Ann Surg 224:598–602
Ho CH, Tsai YC (2012) Old age is a risk factor for recurrence after laparoscopic inguinal hernia repair with porcine small intestine submucosa mesh. Am Surg 78:497
Lau H, Fang C, Yuen WK et al (2007) Risk factors for inguinal hernia in adult males: a case-control study. Surgery 141:262–266
Carbonell JF, Sanchez JL, Peris RT et al (1993) Risk factors associated with inguinal hernias: a case control study. Eur J Surg 159:481–486
Yeh CJ, Chang HY, Pan WH (2011) Time trend of obesity, the metabolic syndrome and related dietary pattern in Taiwan: from NAHSIT 1993–1996 to NAHSIT 2005–2008. Asia Pac J Clin Nutr 20:292–300
Percentage distribution of Body Mass Index (BMI). Health Promotion Administration, Ministry of Health and Welfare Web. 14 Nov. 2013. https://olap.bhp.doh.gov.tw/Search/search2.aspx?menu=1&mode=3&TarId=157&year=99&NL=1&sel=0#QuerySetting
Aufenacker TJ, de Lange DH, Burg MD et al (2005) Hernia surgery changes in the Amsterdam region 1994–2001: decrease in operations for recurrent hernia. Hernia 9:46–50
Cheng TY, Wen CP, Tsai MC et al (2003) The current status of smoking behavior in Taiwan: data analysis from National Health Interview Survey in 2001. (in Chinese). Taiwan J Public Health 22:453–464
Percentage reported being a smoker. Health Promotion Administration, Ministry of Health and Welfare Web. 14 Nov.2013. https://olap.bhp.doh.gov.tw/Search/search2.aspx?menu=1&mode=1&TarId=154&year=98&NL=1&sel=0#QuerySetting
Cannon DJ, Read RC (1981) Metastatic emphysema: a mechanism for acquiring inguinal herniation. Ann Surg 194:270–278
Health and Vital Statistic (2) (1994) Vital Statistic Department of Health. Taiwan: Executive Yuan, R.O.C
Acknowledgments
This study was supported in part by grants from the Clinical Trial and Research Center of Excellence (DOH 100-TD-B-111-004), the Cancer Research Center of Excellence (DOH 100-TD-C-111-005), and Academia Sinica Taiwan Biobank.
Conflict of interest
None declared.
Author information
Authors and Affiliations
Corresponding authors
Additional information
J. J. Keller and C.-H. Muo contributed equally to this manuscript.
Rights and permissions
About this article

Cite this article
Keller, J.J., Muo, CH., Lan, YC. et al. A nation-wide population-based study of inguinal hernia repair incidence and age-stratified recurrence in an Asian population. Hernia 19, 735–740 (2015). https://doi.org/10.1007/s10029-015-1359-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-015-1359-4