
Abstract
Objective
To evaluate the prevalence of signs and symptoms related to temporomandibular disorders (TMD) and orofacial pain in patients with indication for orthognathic surgery.
Methods
The search was carried out in seven electronic databases and gray literature. Studies that evaluated the frequency of signs and symptoms related to TMD and orofacial pain were included. The risk of bias was assessed using the Joanna Briggs Critical Appraisal tool. A meta-analysis of proportions with a random effect model was performed and the GRADE tool judged the certainty of evidence.
Results
After searching the databases, 1859 references were retrieved, 18 of which were selected for synthesis. The prevalence of individuals with at least one TMD symptom was 51% [CI95% = 44–58%], and 44% of the subjects had temporomandibular joint click/crepitus [CI95% = 37–52%]. Additionally, 28% exhibited symptoms related to muscle disorders [CI95% = 22–35%], 34% had disc displacement with or without reduction [CI95% = 25–44%], and 24% had inflammatory joint disorders [CI95% = 13–36%]. The prevalence of headache was 26% [CI95% = 8–51%]. The certainty of evidence was considered very low.
Conclusion
Approximately 1 in 2 patients with dentofacial deformity presents some sign and symptom related to TMD. Myofascial pain and headache may be present in approximately a quarter of patients with dentofacial deformity.
Clinical relevance
A multidisciplinary treatment is necessary for these patients, involving a professional with expertise in the management of TMD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Temporomandibular disorder (TMD) is established as the multiplicity of signs and symptoms related to the temporomandibular joint (TMJ) [1]. The most common signs of TMD are pain, headache, chewing difficulty, trismus, crepitus, and TMJ clicking. Several patients can develop TMD, as it affects people from adolescence to adulthood, including patients with indication for orthognathic surgery [2].
Estimates show that TMD affects approximately 5 to 12% of the entire adult population, with middle-aged women being the population group with the highest prevalence of signs and symptoms, thus becoming a public health problem [3]. The main indications for orthodontic and orthognathic surgical treatment in patients with dentofacial deformities and temporomandibular joint disorders are related to the improvement of masticatory and aesthetic function [4]. Patients with dentofacial deformity may have higher rates of depression and pain when compared to individuals without dentofacial deformity [5], and the correction of this abnormality can generate improvement in quality of life, joint pain and chronic pain, self-esteem and depression [6,7,8].
Only one review was found in the literature addressing the association between the existence of dentofacial deformity and the presence of TMD, and it observed a higher prevalence of this event when compared to a control population [1]. However, no reviews were found with a specific focus on surveying the prevalence of TMD in patients with dentofacial deformity. In this way, a new updated review is justified with a comprehensive search strategy on the subject.
Thus, the objective of this study is to perform a systematic review on the prevalence of signs and symptoms related to TMD and orofacial pain in patients with indication for orthognathic surgery.
Methods
This systematic review was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [9].
Eligibility criteria
To consider the eligibility of studies to be included/excluded from this review, the acronym “PECOS” was used:
-
Population (P): Individuals > 18 years of age
-
Exposition (E): Presence of dentofacial deformity with indication for orthognathic surgery;
-
Comparison (C): Not applicable;
-
Outcomes (O): Prevalence of signs and symptoms of TMD and orofacial pain;
-
Studies design (S): Cross-sectional studies, or longitudinal studies where pre-intervention data were available;
Inclusion criteria
Studies were included where the sample consisted of adult patients (> 18 years of age) with dentofacial deformity and indication for orthognathic surgery. Studies must have evaluated the presence or absence of signs and symptoms of TMD or orofacial pain in the population of interest. Only studies that used the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) or the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) tool to assess TMD were included. Visual-analog scales were accepted for the assessment of orofacial pain. Observational, cross-sectional or longitudinal studies with available data in relation to the preoperative period were included. There were no exclusions of studies based on ethnicity, sex, age, language, or year of publication.
Exclusion criteria
The following exclusion criteria were applied:
-
1.
Sample composed of children, adolescents or elderly people;
-
2.
Patients with no indication for orthognathic surgery, patients with cleft lip and palate or with any associated syndrome;
-
3.
Studies that did not assess the presence of signs and symptoms of TMD at the pre-surgical moment, or when this assessment was not performed by DC/TMD or RDC/TMD;
-
4.
Reviews, letters, books, conference abstracts, case reports, case series, opinion articles, technical articles, and guidelines;
-
5.
Studies with incomplete data;
Information sources and search strategy
Appropriate word combinations and truncations were adapted to seven electronic databases selected as sources of information: Cochrane Library, EMBASE, Latin American and Caribbean Health Sciences Literature (LILACS), LIVIVO, PubMed/Medline, Scopus and Web of Science. In addition, gray literature was also used as a source of information through Google Scholar, MedRxiv and ProQuest Dissertation and Thesis (Supplementary material 1). Manual searches of references were performed in all included studies and experts were consulted in order to improve the search results. All searches were performed in a single day and Endnote® X7 software (EndNote® X7 Thomson Reuters, Philadelphia, PA) was used to manage and remove duplicate references.
An expert in the field, with publications related to the topic, was consulted via e-mail to verify suggestions of references relevant to the topic, which could be evaluated regarding the inclusion/exclusion of this review.
Selection process
The selection of articles was carried out in two phases. In the first phase, two reviewers (M.R.G and A.X.F) independently reviewed the titles and abstracts of all references. All articles that did not meet the eligibility criteria previously established were excluded at this stage. In the second phase, the same reviewers read the full text of the articles selected in the first phase, also independently. In the presence of disagreement, persisting even after discussion between the first two reviewers, a third reviewer (C.M.A) was involved for the final decision making. The Rayyan® website (http://rayyan.qcri.org) was used to allow independent reading between the two reviewers, blinding reviewers and all phases. A third member of the team acted as moderator.
Prior to beginning the selection of articles, a calibration was performed to assess the level of agreement between the reviewers. For this, the Kappa concordance coefficient was calculated, based on the application of eligibility criteria in a partial literature search. The selection of articles in phase 1 and phase 2 only started after obtaining Kappa values > 0.7.
Data collection process
Data of interest were collected by two reviewers (M.R.G and A.X.F) also independently. All information of interest was collected from the included studies, and discussed with a third team member with expertise in the topic (B.L.C.L). The characteristics of the included study, sample characterization, Angle’s classification of malocclusion, and prevalence of outcomes of interest were extracted from all included studies. In the presence of missing or incomplete data in the article, three attempts were made to contact the authors (first and last author, and corresponding author), with an interval of one week, to obtain information. In the absence of a response, the article was excluded.
Data items
The number of events related to TMD or orofacial pain was extracted from the included studies. To calculate the individual prevalence of each study, and the respective 95% confidence intervals (CI95%), the total sample evaluated for each outcome was also extracted.
Study risk of bias assessment
To assess the methodological quality and risk of bias of the included studies, the JBI Critical Appraisal Checklist for Analytical Cross Sectional Studies tool was used [10]. Two reviewers (M.R.G and A.X.F) judged the included articles independently according to the following evaluation criteria: “yes,” “no,” “uncertain,” and “not applicable.” The risk of bias was classified as follows: as high when the study reaches 49% “Yes”; moderate when the study reaches 50 to 69% “Yes”; and low when the study reaches more than 70% “Yes.” Disagreements were resolved through discussion and, in the presence of a lack of consensus, a third reviewer was involved.
Effect measures
Data related to the prevalence of signs and symptoms of temporomandibular disorders and orofacial pain were calculated and reported as prevalence (PV), with the respective 95% CI.
Synthesis methods
The meta-analysis was performed only when a minimum number of three articles were included, containing the frequency data of the evaluation of interest, for each evaluated outcome. Thus, a meta-analysis of proportions was performed with a random effect model, with the Tau2 value estimated by the DerSimonian and Laird method. The assessment of heterogeneity was performed using the inconsistency index (I2). For the data to follow an approximately normal distribution, the Freeman-Tukey double Arcsine transformation method was used. The weight of each study in the analysis was estimated using the inverse variance method, and the respective 95% CI were presented.
Reporting on bias assessment
The existence of publication bias was assessed by a funnel plot analysis and by the Egger test, considering a significance level of 5%. In addition, to reduce the probability of occurrence of a publication bias, a broad search strategy in seven databases, and the inclusion of a non-English language database (LILACS), and gray literature, were carried out.
To ensure greater robustness in the estimates, a sensitivity analysis was performed, keeping only articles with a sample size with adequate statistical power. For this, a sample size calculation was performed based on the global estimate initially obtained, when all studies were included. The sample size calculation was performed for each meta-analysis performed, estimating the necessary sample size when considering a margin of error of 10%, inference for an infinite population, and 95% CI.
Certainty assessment
The level of certainty of evidence was assessed by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) tool [11]. This tool classifies the evidence generated as very low, low, moderate, and high, according to the level of certainty judged according to the following aspects: risk of bias, inconsistency, imprecision, indirect evidence, and publication bias.
Results
Study selection
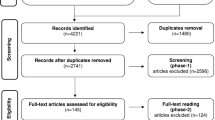
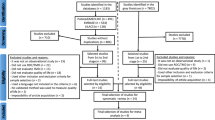
A total of 1859 references were retrieved through searches in the seven electronic databases, leaving the number of 988 after the removal of duplicate references. After reading the titles and abstracts (phase 1), a total of 86 articles were selected for full reading (phase 2). Of these, 68 articles were excluded (Supplementary material 2), resulting in 18 articles included for qualitative synthesis (Fig. 1). No articles from the gray literature, or by indication of an expert, were included.

Flowchart of the literature search and selection criteria
Study characteristics
The articles included originated from the following countries: Brazil, Bosnia and Herzegovina, Colombia, France, Hong Kong, India, Japan, Denmark, USA, Switzerland, Italy, and Sweden. Totaling five cross-sectional studies and thirteen cohort studies. The year of publication varied between 2005 and 2021. There was a higher prevalence of females in the included studies. Of the analyzed articles, 17 used the RDC/TMD for analysis, and one article used a visual analogue scale to assess orofacial pain. The characterization of the studies can be seen in Table 1.
Reporting biases
Regarding the risk of bias in the studies, eleven studies were considered as low risk [12,13,14,15,16,17,18,19,20,21], six as moderate risk [4, 22,23,24,25,26] and one was considered as high risk [27] (Supplementary material 3). The domains that showed the highest prevalence of deficient reports were related to the lack of detail in the inclusion and exclusion criteria items, in addition to the presence and lack of control of confounding factors.
Results of individual studies
TMD and orofacial pain
Joint pain, joint sounds (click/crepitus), headache and myofascial pain were more prevalent when the dentofacial deformity had not yet been corrected. [4, 14, 19, 24]. Muscle disorders were more prevalent in females [4, 18, 27]. Myofascial pain negatively impacted the quality of life of patients with dentofacial deformity [20]. In the study carried out by Farela et al., the patients did not present spontaneous muscle pain, however, they presented sensitivity in at least one facial muscle, when palpated [14]. Luo et al., found that preoperatively patients had pain located in the mandible, which continued even after surgery in 21.4% of patients. The pain threshold for the masseter was significantly lower postoperatively [15].
Arthralgia, arthrosis and arthritis
When considering arthralgia, there was disagreement in the literature, with studies noting less (15) or no difference, and greater arthralgia in individuals with dentofacial deformity [17]. Abrahamsson et al., analyzed patients according to the RDC/TMD compared to the control group, and observed a higher prevalence of myofascial pain without opening limitation, arthralgia and disc displacement with reduction in this population [22]. In addition, there was also disagreement regarding the prevalence of arthrosis and arthritis in these patients, with a greater [17] or no difference in prevalence being described in patients with dentofacial deformity, controlled for patients without deformity [16].
Disc displacement
There was no difference for disc displacement in patients with dentofacial deformity when compared to patients with facial harmony [16]. However, Chung et al., observed a higher prevalence of disc displacement with a reduction in patients with dentofacial deformity associated with asymmetries, when compared to patients with symmetrical deformities. [13].
Results of syntheses
Fifteen studies were included in the meta-analysis, and it was possible to meta-analyze data related to the prevalence of at least one TMD sign/symptom, joint clicks/crepitus, disc displacement, arthralgia, arthritis or arthrosis, headache, and myofascial pain. Since the articles did not report the prevalence for each subgroup, such as sex, age group, type of surgery performed, or initial malocclusion, it was not possible to estimate the prevalence for these subgroups.
When considering the prevalence of temporomandibular disorders, approximately 1 in every two patients had TMD (PV = 51%; CI95% = 44–58%; I2 = 59%) (Fig. 2). Similarly, when considering the prevalence of joint clicks/crepitus, a prevalence of 44% was observed (CI95% = 37–52%; I2 = 63%) (Fig. 3). A smaller proportion of patients had disc displacement, being seen in approximately 1 in 3 patients (PV = 34%; CI95% = 25–44%; I2 = 88%) (Fig. 4). A prevalence of 24% of patients who had arthralgia, arthritis or arthrosis was also observed. (CI95% = 13–36%; I2 = 86%) (Fig. 5).

Forest plot of the meta‐analysis of prevalence of TMD, displaying the risk of bias judgments for each study included

Forest plot of the meta‐analysis of prevalence of joint clicks, displaying the risk of bias judgments for each study included

Forest plot of the meta‐analysis of prevalence of disc displacement, displaying the risk of bias judgments for each study included

Forest plot of the meta‐analysis of prevalence of arthralgia, arthritis or arthrosis, displaying the risk of bias judgments for each study included
The analysis that showed the greatest heterogeneity, and the greatest width of the confidence interval, was when the prevalence of headache was evaluated, with an estimated average prevalence of 26% (CI95% = 8–51%; I2 97%) (Fig. 6). A prevalence of 28% of individuals diagnosed with myofascial pain was estimated (CI95% = 22–35%; I2 = 76%) (Fig. 7).

Forest plot of the meta‐analysis of prevalence of headache, displaying the risk of bias judgments for each study included

Forest plot of the meta‐analysis of prevalence of myofascial pain, displaying the risk of bias judgments for each study included
Considering only studies with samples of Class III patients, the prevalence remains close to the estimated values when including all studies. The observed prevalence rates were as follows: 54% for at least one TMD sign/symptom (CI95% = 42–66%; I2 = 38%), 41% for clicks/crepitus (CI95% = 27–56%; I2 = 55%), 30% for joint disc displacement (CI95% = 22–38%; I2 = 0%), 18% for arthralgia, arthritis, or arthrosis (CI95% = 4–36%; I2 = 74%), and 20% for myofascial pain (CI95% = 1–51%; I2 = 87%).
Reporting biases
The existence of publication bias was not identified when evaluating the symmetry of the funnel plot and the Egger test (p > 0.05), for all analyses performed. When considering only studies with an adequate sample size by de sensitivity analysis, considering a margin of error of 10%, the estimates of all evaluated outcomes decreased, in addition, there was a ≥ 20% reduction in the observed heterogeneity for three of the six outcomes (Table 2).
Certainty of evidence
The level of certainty of evidence was considered very low for all outcomes evaluated, due to the existence of studies with a moderate risk of bias, and inconsistency due to the high heterogeneity in the analyses, even after sensitivity analysis (Table 3).
Discussion
Patients with dentofacial deformity treated with orthognathic surgery may have a decrease in TMD-related signs and symptoms [18], however, in the preoperative period, when the deformity is still present, there may be a higher prevalence of myogenic complaints, depression, and chronic pain [7]. The survey of prevalence of signs and symptoms related to TMD and orofacial pain in these patients can support management strategies in this population. Thus, the aim of the present study was to evaluate the prevalence of signs and symptoms related to temporomandibular disorders and orofacial pain in patients with indication for orthognathic surgery, through systematic review and meta-analysis. Evidence suggests a high prevalence of signs and symptoms related to the temporomandibular joint, and the existence of painful symptoms in the orofacial region, related to myofascial pain and headache.
The most common TMD findings are pain, TMJ clicking, crepitus, headache, chewing difficulty and trismus, and it can affect people from adolescence to adulthood, including patients with dentofacial deformity [2]. In the present study, it was estimated that approximately 1 in 2 people with dentofacial deformity may have TMD and joint clicking, and many have more than one associated sign or symptom. In addition, joint changes, such as disc displacement, arthritis, arthrosis or arthralgia may be present in 34% and 24% of these patients, respectively. In the study by Al Warawreh et al., of the 100 patients analyzed, 35% had one or more TMD symptoms, followed by clicking, pain and crepitus, respectively [2]. On the other hand, Mladenović et al., observed that the prevalence of TMD in this population is similar to patients with malocclusion, but without dentofacial deformity [16]. When considering the general population, excluding patients with skeletal deformities, Valesan et al. estimated, through a meta-analysis, that approximately 1 in 3 adult/elderly individuals had TMD (31%), which is lower than the prevalence found in the present study [3]. In view of this, the high prevalence observed in the present study cannot be inferred from the cause-effect aspect, since prevalence meta-analyses are not intended to infer causality or association.
Some of the included studies report a decrease in TMD-related signs and symptoms in patients with dentofacial deformity when treated by orthodontic-surgical treatment, through orthognathic surgery. [18, 19, 23, 25, 26, 28]. There is still disagreement in the literature on this aspect, with authors reporting on the contrary, an increase in TMD signs in this population when treated [22]. Studies with adequate samples, with statistical power and sample representativeness, should be performed, for a better inference on this outcome. Another point that must be taken into account is the evaluation of this outcome by uncontrolled studies, which favor the occurrence of the Hawthorne effect, with the chance of signs and symptoms decreasing are not related to the intervention, but to the change in behavior due to the fact of the patient’s follow up [29].
Class III patients requiring surgical orthodontic treatment may have a higher prevalence of myofascial pain and chronic pain, associated with higher depression scores, when compared to controls without dentofacial deformity [23]. There is a higher prevalence of headache in patients with dentofacial deformity when compared to patients already treated by orthognathic surgery [24]. Myofascial pain is often associated with persistent localized pain, shoulder pain, orofacial pain, and when this is maintained even after removing the initial triggering factors, it can contribute to the occurrence of sporadic headaches in persistent ones [30]. In the present study, it was estimated that myofascial pain and headache may be present in approximately one quarter of patients with dentofacial deformity, with an approximate prevalence of each other.
Some limitations should be pointed out, prevalence meta-analyses are important for the assessment of the population distribution of the outcome of interest, however, as they do not make inferences comparing them to a control group, they do not allow associative or causality analyses. Most of the included studies did not provide estimates for each subgroup, such as gender, age group, initial malocclusion, and type of surgery performed, making it impossible to meta-analyze these data. Furthermore, due to the nature of this measure, the longitudinal assessment of the outcome is not taken into account, making it impossible to assess behavior over time. The certainty of evidence was considered very low, due to the existence of uncontrolled confounding factors, which may influence the generated estimates. On the other hand, the epidemiological survey of distribution of signs and symptoms in this population can help the surgeon and orthodontist to provide a multidisciplinary treatment to the patient, involving a professional with expertise in the management of temporomandibular disorders. New studies should be carried out, with the appropriate epidemiological design for assessing prevalence (prevalence as the primary outcome), and with an adequate sample size to allow a reduction in the margin of error, as it was observed in the present study that the inclusion of smaller studies in the analysis overestimated the global prevalence.
Conclusion
Approximately 1 in 2 patients with dentofacial deformity present some sign and symptom related to TMD, and many of these patients may present more than one symptomatology. Myofascial pain and headache may be present in approximately a quarter of patients with dentofacial deformity. The evidence still presents uncertainty for these outcomes.
Other information
The protocol was registered on the PROSPERO website (Prospective International Register of Systematic Review – York University Center for Commentary and Dissemination) – under number CRD42022287174.
Data availability
The datasets used and/or analyses during the current study are available from the corresponding author on reasonable request.
References
Al-Moraissi EA, Perez D, Ellis E 3rd (2017) Do patients with malocclusion have a higher prevalence of temporomandibular disorders than controls both before and after orthognathic surgery? A systematic review and meta-analysis. J Cranio-Maxillo-Facial Surg Off Publ Eur Assoc Cranio-Maxillo-Facial Surg 45:1716–1723. https://doi.org/10.1016/j.jcms.2017.07.015
AlWarawreh AM, AlTamimi ZH, Khraisat HM, Kretschmer W (2018) Prevalence of temporomandibular disorder symptoms among orthognathic patients in Southern Germany: retrospective study. Int J Dent 2018:. https://doi.org/10.1155/2018/4706487
Valesan LF, Da-Cas CD, Réus JC et al (2021) Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig 25:441–453. https://doi.org/10.1007/s00784-020-03710-w
Abrahamsson C, Henrikson T, Nilner M et al (2013) TMD before and after correction of dentofacial deformities by orthodontic and orthognathic treatment. Int J Oral Maxillofac Surg 42:752–758. https://doi.org/10.1016/j.ijom.2012.10.016
Sebastiani AM, Gerber JT, Bergamaschi IP et al (2021) Individuals requiring orthognathic surgery have more depression and pain than controls. Braz Oral Res 35:e091. https://doi.org/10.1590/1807-3107bor-2021.vol35.0091
De Araujo CM, Schroder AGD, De Araujo BMDM et al (2020) Impact of orthodontic-surgical treatment on quality of life: a meta-analysis. Eur J Orthod 42:281–289. https://doi.org/10.1093/ejo/cjz093
Bergamaschi IP, Cavalcante RC, Fanderuff M et al (2021) Orthognathic surgery in class II patients: a longitudinal study on quality of life, TMD, and psychological aspects. Clin Oral Investig 25:3801–3808. https://doi.org/10.1007/s00784-020-03709-3
Basso IB, Gonçalves FM, Martins AA et al (2022) Psychosocial changes in patients submitted to orthodontic surgery treatment: a systematic review and meta-analysis. Clin Oral Investig 26:2237–2251. https://doi.org/10.1007/s00784-021-04304-w
Page MJ, McKenzie JE, Bossuyt PM, et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:. https://doi.org/10.1136/bmj.n71
The Joanna Briggs Institute (2014) Joanna Briggs Institute Reviewers’ Manual
Guyatt GH, Oxman AD, Vist GE et al (2008) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336:924–926. https://doi.org/10.1136/bmj.39489.470347.AD
Abrahamsson C, Henrikson T, Bondemark L, Ekberg EC (2015) Masticatory function in patients with dentofacial deformities before and after orthognathic treatment - a prospective, longitudinal, and controlled study. Eur J Orthod 37:67–72. https://doi.org/10.1093/ejo/cju011
Chung K, Richards T, Nicot R et al (2017) ENPP1 and ESR1 genotypes associated with subclassifications of craniofacial asymmetry and severity of temporomandibular disorders. Am J Orthod Dentofac Orthop 152:631–645. https://doi.org/10.1016/j.ajodo.2017.03.024
Farella M, Michelotti A, Bocchino T et al (2007) Effects of orthognathic surgery for class III malocclusion on signs and symptoms of temporomandibular disorders and on pressure pain thresholds of the jaw muscles. Int J Oral Maxillofac Surg 36:583–587. https://doi.org/10.1016/j.ijom.2007.02.001
Luo Y, Svensson P, Jensen JD et al (2014) Quantitative sensory testing in patients with or without ongoing pain one year after orthognathic surgery. J Oral Facial Pain Headache 28:306–316. https://doi.org/10.11607/ofph.1275
Mladenović I, Dodić S, Stošić S et al (2014) TMD in class III patients referred for orthognathic surgery: Psychological and dentition-related aspects. J Cranio-Maxillofacial Surg 42:1604–1609. https://doi.org/10.1016/j.jcms.2014.04.029
de Oliveira Freitas Passos DCB, Conti PCR, Filho HN, Berretin-Felix G (2015) The occurrence of temporomandibular disorders in subjects presented with dentofacial deformities/ Ocorrencia de disfuncao temporomandibular em individuos com deformidade dentofacial. Rev CEFAC Atualizacao Cient em Fonoaudiol e Educ 17:1215+
Sebastiani AM, Baratto-Filho F, Bonotto D et al (2016) Influence of orthognathic surgery for symptoms of temporomandibular dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol 121:119–125. https://doi.org/10.1016/j.oooo.2015.08.012
Sebastiani AM, de Lucas Corso PFC, Bonotto D et al (2018) Does orthognathic surgery improve myofacial pain in individuals with skeletal class III? One-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol 126:322–330. https://doi.org/10.1016/j.oooo.2018.03.020
Sebastiani AM, Dos Santos KM, Cavalcante RC et al (2020) Depression, temporomandibular disorders, and genetic polymorphisms in IL6 impact on oral health-related quality of life in patients requiring orthognathic surgery. Qual Life Res Int J Qual life Asp Treat Care Rehabil 29:3315–3323. https://doi.org/10.1007/s11136-020-02581-8
Roland-Billecart T, Raoul G, Kyheng M et al (2021) TMJ related short-term outcomes comparing two different osteosynthesis techniques for bilateral sagittal split osteotomy. J Stomatol Oral Maxillofac Surg 122:70–76. https://doi.org/10.1016/j.jormas.2020.03.018
Abrahamsson C, Ekberg E, Henrikson T et al (2009) TMD in consecutive patients referred for orthognathic surgery. Angle Orthod 79:621–627. https://doi.org/10.2319/060408-293.1
Di Paolo C, Pompa G, Arangio P et al (2017) Evaluation of temporomandibular disorders before and after orthognathic surgery: therapeutic considerations on a sample of 76 patients. J Int Soc Prev Community Dent 7:125–129. https://doi.org/10.4103/jispcd.JISPCD_443_16
Sahu GR, Kaur A, Rattan V et al (2022) Effect of orthognathic surgery on temporomandibular disorders: a prospective study. J Maxillofac Oral Surg 21:277–282. https://doi.org/10.1007/s12663-021-01644-8
Takahara N, Kabasawa Y, Sato M et al (2017) MRI changes in the temporomandibular joint following mandibular setback surgery using sagittal split ramus osteotomy with rigid fixation. Cranio - J Craniomandib Pract 35:38–45. https://doi.org/10.1080/08869634.2016.1143167
Toh AQJ, Leung YY (2022) The effect of orthognathic surgery on temporomandibular disorder. J Cranio-Maxillofacial Surg 50:218–224. https://doi.org/10.1016/j.jcms.2021.11.012
Jaramillo SP, Del Valle AF (2004) Signos y síntomas de desórdenes temporomandibulares antes y después de cirugía ortognática, comparación entre osteotomía sagital y osteotomía oblicua de rama. Rev Fac Odontol Univ Antioq 16(1):42–51
Catherine Z, Courvoisier DS, Scolozzi P (2016) Are condylar morphologic changes associated with temporomandibular disorders in patients with orthognathia? Oral Surg Oral Med Oral Pathol Oral Radiol 122:e44–e50. https://doi.org/10.1016/j.oooo.2016.03.006
Ho AMH, Phelan R, Mizubuti GB et al (2018) Bias in before-after studies: narrative overview for anesthesiologists. Anesth Analg 126:1755–1762. https://doi.org/10.1213/ANE.0000000000002705
Graff-Radford SB, Bassiur JP (2014) Temporomandibular disorders and headaches. Neurol Clin 32:525–537. https://doi.org/10.1016/j.ncl.2013.11.009
Author information
Authors and Affiliations
Contributions
M.R.G., R.D.S., A.X.F., carried out the article selection process, risk of bias analysis, and critical reading of the writing. F.M.G and W.V.N, carried out the construction of figures and tables, and critical reading of the writing. R.S.S., B.L.C.L., A.G.D.S., B.S.Z. performed the writing of the manuscript. C.M.A. coordinated the research, carried out the statistical analyzes and critical reading of the writing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Garcia, M.R., da Silva, R.D., Ferraz, A.X. et al. Prevalence of signs and symptoms related to temporomandibular disorders and orofacial pain in patients indicated for orthognathic surgery: a meta-analysis. Clin Oral Invest 27, 3307–3319 (2023). https://doi.org/10.1007/s00784-023-05110-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05110-2