
Abstract
Objectives
This study evaluated the effect of milk supplemented with Lactobacillus rhamnosus SP1 on the occurrence of caries and the salivary concentration of human β-defensin-3 (hβD-3) in preschool children with high caries risk.
Materials and methods
A sample of 42 children was randomly assigned to two groups; children in the intervention group were given 150 mL of milk supplemented with 107 CFU/mL of Lactobacillus rhamnosus SP1, while children in the control group were given standard milk, for 10 months. The occurrence of dental caries was assessed using the International Caries Detection and Assessment System (ICDAS), and the concentration of hβD-3 was measured in unstimulated saliva using an ELISA test at baseline and after the intervention.
Results
There was an increase in the number of teeth with carious lesions (dICDAS2-6 mft) in the control group, and this increase was statistically significant (p = 0.0489). The concentration of hβD-3 in saliva from the intervention group decreased from 597.91 to 126.29 pg/mL (p = 0.0061), unlike in the control group, where no change in hβD-3 salivary concentration was found.
Conclusions
These findings showed that regular intake of probiotic-supplemented milk in preschool children with high caries risk decreased the occurrence of caries and the salivary levels of hβD-3.
Clinical relevance
Our results suggest the need for developing and implementing probiotic supplementation, as adjuvants to the conventional treatments for caries and allow to considerate the salivary levels of hβD-3 as markers of oral tissue homeostasis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dental caries is a chronic, multifactorial disease that generally progresses slowly and has a high prevalence worldwide [1, 2]. According to the “Ecological Plaque Hypothesis”, dental caries is a result of changes in the environment due to acid production from the fermentation of dietary carbohydrates, which finally selects during biofilm formation, and acidogenic and acid-tolerating species such as mutans streptococci and lactobacilli [3, 4].
There are several preventive strategies for dental caries, including some mechanisms that modify the biofilm and reduce the cariogenic challenge, like the probiotic bacteria [5]. The World Health Organization (WHO) defines probiotics as live microorganisms, mainly bacteria, that are safe for human consumption and have beneficial effects on human health when ingested in sufficient quantities [6]. Now, probiotics also must have “defined contents, appropriate viable count at the end of shelf life, and suitable evidence for health benefits”, and further stated that all probiotics must be “safe for their intended use” [7, 8]. Several clinical trials have reported on the use of different probiotic strains such as Lactobacillus rhamnosus GG, L. casei, L. reuteri, L. plantarum, L. brevis CD2, and Bifidobacterium spp. for the prevention of caries [9,10,11,12,13,14]. Among the genus Lactobacillus, L. rhamnosus SP1, also known as L. rhamnosus GG, has become one of the most studied probiotic bacteria in the world with decades of safe use that supports its efficacy and either health benefits [15,16,17]. Specifically, in the oral health field, Lactobacillus rhamnosus SP1 have been well studied, showing beneficial effects in dental caries or periodontal diseases [18, 19]. Although the multiple mechanisms of action of probiotics are not fully understood, it has been proposed that probiotics may work through systemic and local effects involving adherence, co-aggregation, competitive inhibition, organic acid production, bacteriocin-like compound production, and immune response modulation [20], or by stimulating non-specific and specific immune responses [21].
It is known that saliva and its components play an essential role in homeostasis and the prevention of caries. Salivary defense mechanisms are numerous and include local and systemic production of immunoglobulins, lysozymes, mucins, and antimicrobial peptides [22]. Antimicrobial peptides are natural antibiotics that deliver a first-line defense against a broad spectrum of pathogens, including Gram+ and Gram− bacteria, viruses, and fungi [23, 24]. There are 3 leading families of antimicrobial peptides, which are defined by their amino acid composition and three-dimensional structure: cathelicidins or LL-37, histatins, and defensins [25]. In humans, three β-defensins (BD) are predominantly expressed in the mucosal epithelium (hβD-1, 2, and 3) [26]. hβD-3 stands out among BD because it has the most powerful antibacterial action, and it is widely distributed in the oral epithelia in the gums, tongue, salivary glands, and oral mucosa [27, 28]. In epithelial cell line derived from colorectal adenocarcinoma (Caco-2), BD expression or secretion is induced by several Lactobacillus species [29]. Indeed, probiotic consumption modulates innate intestinal immunity, stimulating the synthesis of hβD-2 [29,30,31,32]. Recently, Kobayashi et al. [33] showed that gastric administration of LG2055 could control the oral inflammation and bone resorption caused by P. gingivalis infection by producing BD in the oral cavity. However, there is no evidence about whether the expression of hβD-3 is affected by the consumption of probiotic strains. Therefore, the present study examined whether the use of milk supplemented with L. rhamnosus SP1 for 10 months affects the salivary concentration of hβD-3 and caries scores.
Materials and methods
Study design
This experimental study enrolled forty-two children aged 2 to 3 years old, with an allocation ratio of 1:1. The participants were recruited from 16 nursery schools from the Integra Foundation located in the northwestern area of Metropolitan Region, Santiago, Chile. Informed consent was requested from parents and guardians. The inclusion criteria were healthy children without milk intolerance or food allergies. This project was guided by the principles of the Declaration of Helsinki, and was approved by the ethics committee of the Faculty of Dentistry at the University of Chile (certificate no. 2011/14).
Intervention
During their afternoon break, children were given 150 mL of 2% milk, which was prepared by the nursery school staff by adding 500gm of powdered milk (Macro Food, Santiago, Chile) to 5 L of previously boiled water at 40 °C. After stirring the preparation, a sachet of probiotics was added to the milk to attain a final concentration of 107-CFU/mL L. rhamnosus SP1 (Sacco, Cadorago, Italy) for the probiotic group. The placebo sachet for the control group only contained medium-fat milk. The probiotic-supplemented milk and the placebo milk were prepared and given to the children only on weekdays. During the intervention period, samples of milk were taken, and microbiological tests were performed to assess the presence of probiotic bacteria. The children were exposed to the intervention for a total of 10 months. The school staff filled in a logbook every day with information regarding the attendance of each child or his or her absence due to sickness or any other circumstances.
Clinical examination
Clinical dental examinations were performed at baseline and at the end of the intervention after 10 months. All children were examined by two qualified dentists (trained specifically for the study examination) at the nursery schools with an artificial light, a mouth mirror, and WHO periodontal probe. The examiners were trained in the clinical setting and using literature related to International Caries Detection and Assessment System (ICDAS). The assessment of intra- and inter-examiner reliability values resulted in a kappa value of 0.71, respectively. Visual and tactile detection of dental caries followed the ICDAS to describe lesion severity.
Salivary samples
The salivary samples were taken at baseline and the end of the intervention in the morning session at each nursery school. The procedure was performed by the same operator and always under the same conditions. Unstimulated saliva samples were taken as reported in Naše et al. [34]. Using a sterile pipette, a 1.5-mL sample of saliva was collected and deposited in a sterile, plastic microcentrifuge tube. The samples were taken and refrigerated (4 °C) in the Laboratory of Cellular and Molecular Biology, Faculty of Dentistry, University of Chile, and later stored at − 80 °C before biochemical analysis. At the time of analysis, the samples were thawed at room temperature (RT) and cleared by centrifugation at 10,000 rpm at 4 °C for 10 min.
hβD-3 analysis
The levels of hβD-3 in the saliva samples were determined using an enzyme-linked immunosorbent assay (ELISA) (US Biological®, USA) according to the manufacturer’s instructions. The concentration of each saliva sample was expressed in pg/mL. In brief, undiluted saliva samples were applied to a plate pre-coated with the specific primary antibody to hβD-3 in triplicate and incubated for 1 h at room temperature (RT). After washing four times with a wash solution, each well was incubated with biotinylated antibody for 1 h at RT. After another four washings with a wash solution, streptavidin-peroxidase (HRP) conjugate was added and incubated for 1 h. After five washings with a wash solution, 3,3′,5,5′-tetramethylbenzidine (TMB) was added for 15 min in the dark, and the reaction was then stopped by the addition of 1% H2SO4. The concentrations of hβD-3 in the saliva samples were calculated from a standard curve established by known concentrations of an hβD-3 standard.
Statistical analysis
Differences between groups were analyzed for statistical significance using the Pearson χ2 test for categorized/dichotomized variables, and differences between groups at baseline and at the end of the study were analyzed for statistical significance using the Student t test. p < 0.05 was considered statically significant. The data were GraphPad software (GraphPad software Inc, La Jolla, CA USA).
Results
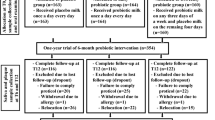
During the 10-month intervention, no adverse reactions to the daily consumption of milk supplemented with probiotic L. rhamnosus SP1 were detected. The number of children who participated is illustrated in the flowchart (Fig. 1). The baseline characteristics of the children in the intervention group and the control group are presented in Table 1. There were no statistically significant differences between the groups in terms of sex. At baseline condition, the mean salivary concentration of hβD-3 for ICDAS 2-6 individuals was 627.64 pg/mL (SD 41.92), and for caries-free individuals (ICDAS 2-6) is 353.23 pg/mL (SD 510.79). Individuals with cavitated caries lesions (ICDAS 5-6) have a salivary concentration of hβD-3 of 750.81 pg/mL (SD 966.61).

Flowchart of the randomization of participants throughout the 10-month intervention period
Effect on dental caries
The caries data at baseline and at the end of the study are shown in Table 2. The mean numbers of caries lesions in the children in the intervention group and the control group were equal at baseline in terms of both cavitated (dICDAS5-6 mft) (p = 0.45) and all carious lesions (dICDAS2-6 mft) (p = 0.474). The difference between the means of the number of caries lesions at the start and end of the intervention (dICDAS5-6 mft) was 0.76 ± 1.22 and 1.24 ± 1.92 for the probiotic group and the control group, respectively, and no statistically significant difference was found (p = 0.12) (Table 2). When examined at the all carious lesion level (dICDAS 2-6 mft) after the 10-month intervention period, the difference between the means of the number of caries lesions in the probiotic group was 1.29 ± 1.85, and in the control group was 2.38 ± 3.11. There was an increase in the number of teeth with carious lesions in the control group, and this increase was statistically significant (p = 0.0489) (Table 2).
Effect of probiotic consumption on the salivary concentration of hβD-3
At baseline, there were no statistically significant differences in salivary concentration between the intervention and control groups (p = 0.27) (Table 2). After the intervention, the salivary level of hβD-3 in the control group showed no statistically significant changes between baseline and after 10 months (p = 0.9815) (Fig. 2), which is different from the probiotic group, where the level decreased from 597.91 ± 743.28 to 126.29 ± 69.3 pg/mL (p = 0.0061) (Fig. 2). Similarly, a statistically significant difference (p = 0.0140) was found between both groups at 10 months (Table 2). In addition, the probiotic group had a wide range of hβD-3 saliva concentrations, with a large standard deviation before the initiation of the intervention (m = 0). After 10 months of probiotic consumption (m = 10), the salivary concentration of the peptide and the standard deviation in the group decreased. In the control group, the intragroup variability was maintained over time, as shown in the high standard deviation values.

Salivary concentration of hβD-3, expressed as pg/mL, of the groups at baseline (m = 0) and the end of the intervention (m = 10). The probiotic group showed a significant decrease in salivary concentration of hβD-3 (p = 0.0061) and a decrease in variability once the probiotic was consumed. No changes were observed in the control group
Discussion
Probiotic use offers a current strategy to fight oral disease, including the development of caries [9, 10, 12,13,14, 35,36,37]. In our study, after 10 months of an intervention with a probiotic, the number of teeth with carious lesions (dICDAS 2-6 mft) in the group treated with probiotic was lower than in the control group. This result confirmed that milk supplemented with probiotic L. rhamnosus SP1 will reduce the caries prevalence in this group of children with high caries risk, as shown in previous studies [11, 34, 38, 39]. In our study, the control and experimental groups were well balanced at baseline for dICDAS 2-6 mft caries lesions, 2.33 (SD 2.98), and 2.38 (SD 2.97). Although dICDAS 2-6 mft is an extensive range, we observed that dICDAS 5-6 mft caries lesions were well balanced too, 0.81 (SD 1.6) and 0.86 (SD 1.52).
Probiotics have multiple mechanisms of action that affect pathogenic bacteria in different aspects, such as metabolic activity [40], co-aggregation [37], microbial growth inhibition [35], and bacteriocins production [41]. In addition, probiotics can modulate the immune response [42]. On this subject, it has been reported that the use of Lactobacilli as a probiotic supplement increased salivary human neutrophil peptide 1–3 (HNP1-3) and was negatively related to the development of pit and fissure caries [43]. Since beta-defensin (BD) family members hβD-2 and hβD-3 are also associated with an oral immune response [44], we hypothesized that, similar to other antimicrobial peptides [43], probiotic supplementation might help prevent dental caries by augmenting basal production of hβD-3. Unexpectedly, we observed that regular consumption of milk enriched with L. rhamnosus SP1 caused a decrease in the salivary concentration of hβD-3 when compared with individuals who did not consume the probiotic.
This study compared groups with similar state of health related to dental caries. The hβD-3 levels indicated no statistical difference between the two groups at baseline and are in accordance with levels previously reported (0–6.21 μg/mL) [45].
Since microbial pathogens stimulate hβD-3 expression in oral epithelial cells [28, 46, 47] and hβD-3 function as a direct antibiotic agent to maintain homeostasis of microbes in the oral cavity, we think that the effect of probiotics on hβD-3 levels is probably associated with decreased caries prevalence and the re-establishment of a healthy oral microbiome. In periodontal disease, it has been observed that reducing the microbial burden decreases the inflammation of localized oral epithelial cells and supports disease resolution [48]. Although we [49,50,51,52] did not perform microbiota analyses, several clinical studies show that regular consumption of probiotics decreases the number of cariogenic Streptococci in bacterial plaques and in saliva [9,10,11,12, 34, 53, 54]. Besides, hβD-3 expression is also induced in epithelial cells by pro-inflammatory cytokines, such as (IL)-1β, tumor necrosis factor (TNF)-α, and IL-17 [55]; previous studies have shown high salivary levels of IL-6 and TNF-α in children with caries compared with healthy children [49,50,51,52]. Then, the suppression of inflammatory cytokines production in oral tissues by the consumption of L. rhamnosus SP1 might correlate with the hβD-3 levels observed at the end of the study. For instance, L. rhamnosus GG has proven to be immunostimulatory [56] showing several anti-inflammatory effects through the modulation of the gut microbiota and the downregulation of pro-inflammatory molecules in model of infection and cancer [57, 58]. Furthermore, probiotics have shown improving clinical symptoms in patients with immune dysregulation and autoimmune diseases, such as rheumatoid arthritis [59], systemic sclerosis [60], inflammatory bowel disease [61], and multiple sclerosis [62].
The ingested probiotics produce a change in the gut microbiota and promote health through various mechanisms, including the maintenance of the intestinal barrier function and the modulation of the host’s immune system [63,64,65]. These studies related to the human intestine suggest that defensins are critical regulators of bacterial diversity and tissue homeostasis [66]. In our study, we observed hβD-3 in saliva, which is a remote place from the intestine; it may suggest that intestinal cells sensitized with L. rhamnosus SP1 could migrate and act on oral cavity tissues, and regulate hβD-3 production locally. In this context, there are subsets of migrating intestinal lymph dendritic cells (DCs) that play immunogenic or tolerogenic roles according to the microenvironment [67]. Kobayashi et al. [33] showed in a mice model of periodontal disease that gastric administration of L. gasseri STB2055 increased the DCs number among gingival mononuclear cells; however, the exact phenotype of DCs subset and its function was not studied. Further studies are required regarding to elucidate the exact mechanisms underlying the communication between intestine and mouth.
The findings of this study have to be seen in light of some limitations. We were focusing on hβD-3 because of the higher specificity and activity for streptococci, and salt-tolerant activity [68, 69]. However, there are other salivary proteins involved in host defense in the mouth with overlapping functions in addition to defensins such as histatins [70] and cathelicidins [71]. Although the role of cathelicidins in protection against caries is inconclusive [69, 72], naturally occurring histatins in AEP have a crucial role to acid injury [73] and derivatives of histatins appears to have improved activity against several potential pathogens, including S. mutans [74]. Up to now, there are no studies that relate probiotics defensins with other antimicrobial proteins which will be interesting to consider in future studies.
Finally, our results suggest the need for developing and implementing different oral health strategies, such as probiotic supplementation, as adjuvants to the conventional treatments for caries. However, additional studies are required to fully elucidate the influence of probiotic consumption on the oral immune response.
References
Fejerskov O (2004) Changing paradigms in concepts on dental caries: consequences for oral health care. http://www.ncbi.nlm.nih.gov/pubmed/15153687. Accessed 28 July 2020
Selwitz RH, Ismail AI, Pitts NB (2007) Dental caries. http://www.ncbi.nlm.nih.gov/pubmed/17208642. Accessed 28 July 2020
Marsh PD (2010) Microbiology of dental plaque biofilms and their role in oral health and caries. http://www.ncbi.nlm.nih.gov/pubmed/20630188. Accessed 28 July 2020
Takahashi N, Nyvad B (2011) The role of bacteria in the caries process: ecological perspectives. http://www.ncbi.nlm.nih.gov/pubmed/20924061. Accessed 28 July 2020
Longbottom C, Ekstrand K, Zero D. Kambara M (2009) Novel preventive treatment options. http://www.ncbi.nlm.nih.gov/pubmed/19494683. Accessed 28 July 2020
Meurman JH, Stamatova I (2007) Probiotics: contributions to oral health. http://www.ncbi.nlm.nih.gov/pubmed/17714346. Accessed 28 July 2020
Hill CP, Yee J, Selsted ME, Eisenberg D (1991) Crystal structure of defensin HNP-3, an amphiphilic dimer: mechanisms of membrane permeabilization. http://www.ncbi.nlm.nih.gov/pubmed/2006422. Accessed 28 July 2020
ISAPP (2018) Minimum criteria for probiotics https://isappscience.org/minimum-criteria-probiotics/. Accessed 28 July 2020
Chuang LC, Huang CS, Ou-Yang LW, Lin SY (2011) Probiotic Lactobacillus paracasei effect on cariogenic bacterial flora. http://www.ncbi.nlm.nih.gov/pubmed/20502929. Accessed 28 July 2020
Petersson LG, Magnusson K, Hakestam U, Baigi A. Twetman S (2011) Reversal of primary root caries lesions after daily intake of milk supplemented with fluoride and probiotic lactobacilli in older adults. http://www.ncbi.nlm.nih.gov/pubmed/21563871. Accessed 28 July 2020
Rodriguez G, Ruiz B, Faleiros S, Vistoso A, Marro ML, Sanchez J, Urzua I, Cabello R (2016) Probiotic compared with standard milk for high-caries children: a cluster randomized trial. http://www.ncbi.nlm.nih.gov/pubmed/26747421. Accessed 28 July 2020
Singh RP, Damle SG. Chawla A (2011) Salivary mutans streptococci and lactobacilli modulations in young children on consumption of probiotic ice-cream containing Bifidobacterium lactis Bb12 and Lactobacillus acidophilus La5. http://www.ncbi.nlm.nih.gov/pubmed/21466258. Accessed 28 July 2020
Taipale T, Pienihakkinen K, Alanen P, Jokela J, Soderling E (2013) Administration of Bifidobacterium animalis subsp. lactis BB-12 in early childhood: a post-trial effect on caries occurrence at four years of age. http://www.ncbi.nlm.nih.gov/pubmed/23571819. Accessed 28 July 2020
Taipale T, Pienihakkinen K, Salminen S, Jokela J. Soderling E (2012) Bifidobacterium animalis subsp. lactis BB-12 administration in early childhood: a randomized clinical trial of effects on oral colonization by mutans streptococci and the probiotic. http://www.ncbi.nlm.nih.gov/pubmed/22327347. Accessed 28 July 2020
Banna GL, Torino F, Marletta F, Santagati M, Salemi R, Cannarozzo E, Falzone L, Ferrau F, Libra M (2017) Lactobacillus rhamnosus GG: an overview to explore the rationale of its use in cancer. http://www.ncbi.nlm.nih.gov/pubmed/28919861. Accessed 28 July 2020
Pace F, Pace M, Quartarone G (2015) Probiotics in digestive diseases: focus on Lactobacillus GG. http://www.ncbi.nlm.nih.gov/pubmed/26657927. Accessed 28 July 2020
Vandenplas Y, Huys G, Daube G (2015) Probiotics: an update. http://www.ncbi.nlm.nih.gov/pubmed/25458874. Accessed 28 July 2020
Matsubara VH, Bandara HM, Ishikawa KH, Mayer MP, Samaranayake LP (2016) The role of probiotic bacteria in managing periodontal disease: a systematic review. http://www.ncbi.nlm.nih.gov/pubmed/27224284. Accessed 28 July 2020
Sivamaruthi BS, Kesika P, Chaiyasut C (2020) A review of the role of probiotic supplementation in dental caries. http://www.ncbi.nlm.nih.gov/pubmed/32307660. Accessed 28 July 2020
Teughels W, Loozen G, Quirynen M (2011) Do probiotics offer opportunities to manipulate the periodontal oral microbiota? http://www.ncbi.nlm.nih.gov/pubmed/21323712. Accessed 28 July 2020
Bonifait L, Chandad F, Grenier D (2009) Probiotics for oral health: myth or reality? http://www.ncbi.nlm.nih.gov/pubmed/19840501. Accessed 28 July 2020
de Almeida PEV, Grégio AM, Machado MA, de Lima AA, Azevedo LR (2008) Saliva composition and functions: a comprehensive review. http://www.ncbi.nlm.nih.gov/pubmed/18335122. Accessed 28 July 2020
Ganz T (2004) Defensins: antimicrobial peptides of vertebrates. http://www.ncbi.nlm.nih.gov/pubmed/15330253. Accessed 28 July 2020
Zasloff M (2002) Antimicrobial peptides of multicellular organisms. http://www.ncbi.nlm.nih.gov/pubmed/11807545. Accessed 28 July 2020
Abiko Y, Saitoh M (2007) Salivary defensins and their importance in oral health and disease. http://www.ncbi.nlm.nih.gov/pubmed/17979749. Accessed 28 July 2020
Duits LA, Ravensbergen B, Rademaker M, Hiemstra PS, Nibbering PH (2002) Expression of beta-defensin 1 and 2 mRNA by human monocytes, macrophages and dendritic cells. http://www.ncbi.nlm.nih.gov/pubmed/12153515. Accessed 28 July 2020
Harder J, Bartels J, Christophers E, Schroder JM (2001) Isolation and characterization of human beta -defensin-3, a novel human inducible peptide antibiotic. http://www.ncbi.nlm.nih.gov/pubmed/11085990. Accessed 28 July 2020
Dhople V, Krukemeyer A, Ramamoorthy A (2006) The human beta-defensin-3, an antibacterial peptide with multiple biological functions. http://www.ncbi.nlm.nih.gov/pubmed/16978580. Accessed 28 July 2020
Schlee M, Harder J, Koten B, Stange EF, Wehkamp J, Fellermann K (2008) Probiotic lactobacilli and VSL#3 induce enterocyte beta-defensin 2. http://www.ncbi.nlm.nih.gov/pubmed/18190603. Accessed 28 July 2020
Moro-García MA, Alonso-Arias R, Baltadjieva M, Fernández Benítez C, Fernández Barrial MA, Díaz Ruisánchez E, Alonso Santos R, Alvarez Sánchez M, Saavedra Miján J, López-Larrea C (2013) Oral supplementation with Lactobacillus delbrueckii subsp. bulgaricus 8481 enhances systemic immunity in elderly subjects. http://www.ncbi.nlm.nih.gov/pubmed/22645023. Accessed 28 July 2020
Schlee M, Wehkamp J, Altenhoefer A, Oelschlaeger TA, Stange EF, Fellermann K (2007) Induction of human beta-defensin 2 by the probiotic Escherichia coli Nissle 1917 is mediated through flagellin. http://www.ncbi.nlm.nih.gov/pubmed/17283097. Accessed 28 July 2020
Wehkamp J, Harder J, Wehkamp K, Wehkamp-von Meissner B, Schlee M, Enders C, Sonnenborn U, Nuding S, Bengmark S, Fellermann K, Schröder JM, Stange EF (2004) NF-kappaB- and AP-1-mediated induction of human beta defensin-2 in intestinal epithelial cells by Escherichia coli Nissle 1917: a novel effect of a probiotic bacterium. http://www.ncbi.nlm.nih.gov/pubmed/15385474. Accessed 28 July 2020
Kobayashi R, Kobayashi T, Sakai F, Hosoya T, Yamamoto M, Kurita-Ochiai T (2017) Oral administration of Lactobacillus gasseri SBT2055 is effective in preventing Porphyromonas gingivalis-accelerated periodontal disease. http://www.ncbi.nlm.nih.gov/pubmed/28373699. Accessed 28 July 2020
Näse L, Hatakka K, Savilahti E, Saxelin M, Pönkä A, Poussa T, Korpela R, Meurman JH (2001) Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. http://www.ncbi.nlm.nih.gov/pubmed/11799281. Accessed 28 July 2020
Keller MK, Hasslöf P, Stecksén-Blicks C, Twetman S (2011) Co-aggregation and growth inhibition of probiotic lactobacilli and clinical isolates of mutans streptococci: an in vitro study. http://www.ncbi.nlm.nih.gov/pubmed/21306197. Accessed 28 July 2020
Keller MK, Larsen IN, Karlsson L, Twetman S (2014) Effect of tablets containing probiotic bacteria (Lactobacillus reuteri) on early caries lesions in adolescents: a pilot study. http://www.ncbi.nlm.nih.gov/pubmed/24889893. Accessed 28 July 2020
Twetman L, Larsen U, Fiehn NE, Stecksén-Blicks C, Twetman S (2009) Coaggregation between probiotic bacteria and caries-associated strains: an in vitro study. http://www.ncbi.nlm.nih.gov/pubmed/19479452. Accessed 28 July 2020
Angarita-Diaz MP, Forero-Escobar D, Ceron-Bastidas XA, Cisneros-Hidalgo CA, Davila-Narvaez F, Bedoya-Correa CM, Freitas SC, Cabrera-Arango CL, Melo-Colina R (2020) Effects of a functional food supplemented with probiotics on biological factors related to dental caries in children: a pilot study. http://www.ncbi.nlm.nih.gov/pubmed/31388942. Accessed 28 July 2020
Cortes-Dorantes N, Ruiz-Rodriguez MS, Karakowsky-Kleiman L, Garrocho-Rangel JA, Sanchez-Vargas LO, Pozos-Guillen AJ (2015) Probiotics and their effect on oral bacteria count in children: a pilot study. http://www.ncbi.nlm.nih.gov/pubmed/25793955. Accessed 28 July 2020
Hedberg M, Hasslöf P, Sjöström I, Twetman S, Stecksén-Blicks C (2008) Sugar fermentation in probiotic bacteria--an in vitro study. http://www.ncbi.nlm.nih.gov/pubmed/18954354. Accessed 28 July 2020
Teughels W, Van Essche M, Sliepen I, Quirynen M (2008) Probiotics and oral healthcare. http://www.ncbi.nlm.nih.gov/pubmed/18715361. Accessed 28 July 2020
Maldonado Galdeano C, Cazorla SI, Lemme Dumit JM, Velez E, Perdigon G (2019) Beneficial Effects of Probiotic Consumption on the Immune System. http://www.ncbi.nlm.nih.gov/pubmed/30673668. Accessed 28 July 2020
Wattanarat O, Makeudom A, Sastraruji T, Piwat S, Tianviwat S, Teanpaisan R, Krisanaprakornkit S (2015) Enhancement of salivary human neutrophil peptide 1-3 levels by probiotic supplementation. http://www.ncbi.nlm.nih.gov/pubmed/25884192. Accessed 28 July 2020
Joly S, Maze C, McCray PB Jr, Guthmiller JM (2004) Human beta-defensins 2 and 3 demonstrate strain-selective activity against oral microorganisms. http://www.ncbi.nlm.nih.gov/pubmed/15004048. Accessed 28 July 2020
Tao R, Jurevic RJ, Coulton KK, Tsutsui MT, Roberts MC, Kimball JR, Wells N, Berndt J, Dale BA (2005) Salivary antimicrobial peptide expression and dental caries experience in children. http://www.ncbi.nlm.nih.gov/pubmed/16127066. Accessed 28 July 2020
Diamond G, Beckloff N, Weinberg A, Kisich KO (2009) The roles of antimicrobial peptides in innate host defense. http://www.ncbi.nlm.nih.gov/pubmed/19601838. Accessed 28 July 2020
Diamond G, Ryan L (2011) Beta-defensins: what are they really doing in the oral cavity? http://www.ncbi.nlm.nih.gov/pubmed/21332602. Accessed 28 July 2020
Zaura E, Twetman S (2019) Critical appraisal of oral pre- and probiotics for caries prevention and care. http://www.ncbi.nlm.nih.gov/pubmed/30947169. Accessed 28 July 2020
Lima GQT, Brondani MA, Silva A, Carmo C, Silva RAD, Ribeiro CCC (2018) Serum levels of proinflammatory cytokines are high in early childhood caries. http://www.ncbi.nlm.nih.gov/pubmed/29895395. Accessed 28 July 2020
Ribeiro CCC, Pacheco CJB, Costa EL, Ladeira LLC, Costa JF, da Silva RA, Carmo CDS (2018) Proinflammatory cytokines in early childhood caries: salivary analysis in the mother/children pair. http://www.ncbi.nlm.nih.gov/pubmed/29246654. Accessed 28 July 2020
Ribeiro TR, Dria KJ, de Carvalho CB, Monteiro AJ, Fonteles MC, de Moraes Carvalho K, Fonteles CS (2013) Salivary peptide profile and its association with early childhood caries. http://www.ncbi.nlm.nih.gov/pubmed/22892037. Accessed 28 July 2020
Sharma V, Gupta N, Srivastava N, Rana V, Chandna P, Yadav S, Sharma A (2017) Diagnostic potential of inflammatory biomarkers in early childhood caries - a case control study. http://www.ncbi.nlm.nih.gov/pubmed/28579141. Accessed 28 July 2020
Lin TH, Lin CH, Pan TM (2018) The implication of probiotics in the prevention of dental caries. http://www.ncbi.nlm.nih.gov/pubmed/29192351. Accessed 28 July 2020
Stecksén-Blicks C, Sjöström I, Twetman S (2009) Effect of long-term consumption of milk supplemented with probiotic lactobacilli and fluoride on dental caries and general health in preschool children: a cluster-randomized study. http://www.ncbi.nlm.nih.gov/pubmed/19690413. Accessed 28 July 2020
Diamond G, Beckloff N, Ryan LK (2008) Host defense peptides in the oral cavity and the lung: similarities and differences. http://www.ncbi.nlm.nih.gov/pubmed/18809744. Accessed 28 July 2020
Mileti E, Matteoli G, Iliev ID, Rescigno M (2009) Comparison of the immunomodulatory properties of three probiotic strains of Lactobacilli using complex culture systems: prediction for in vivo efficacy. http://www.ncbi.nlm.nih.gov/pubmed/19756155. Accessed 28 July 2020
Gamallat Y, Meyiah A, Kuugbee ED, Hago AM, Chiwala G, Awadasseid A, Bamba D, Zhang X, Shang X, Luo F, Xin Y (2016) Lactobacillus rhamnosus induced epithelial cell apoptosis, ameliorates inflammation and prevents colon cancer development in an animal model. http://www.ncbi.nlm.nih.gov/pubmed/27447122. Accessed 28 July 2020
Khailova L, Baird CH, Rush AA, Barnes C, Wischmeyer PE (2017) Lactobacillus rhamnosus GG treatment improves intestinal permeability and modulates inflammatory response and homeostasis of spleen and colon in experimental model of Pseudomonas aeruginosa pneumonia. http://www.ncbi.nlm.nih.gov/pubmed/27745813. Accessed 28 July 2020
Alipour B, Homayouni-Rad A, Vaghef-Mehrabany E, Sharif SK, Vaghef-Mehrabany L, Asghari-Jafarabadi M, Nakhjavani MR, Mohtadi-Nia J (2014) Effects of Lactobacillus casei supplementation on disease activity and inflammatory cytokines in rheumatoid arthritis patients: a randomized double-blind clinical trial. http://www.ncbi.nlm.nih.gov/pubmed/24673738. Accessed 28 July 2020
Frech TM, Khanna D, Maranian P, Frech EJ, Sawitzke AD, Murtaugh MA (2011) Probiotics for the treatment of systemic sclerosis-associated gastrointestinal bloating/ distention. http://www.ncbi.nlm.nih.gov/pubmed/21586214. Accessed 28 July 2020
Ganji-Arjenaki M, Rafieian-Kopaei M (2018) Probiotics are a good choice in remission of inflammatory bowel diseases: a meta analysis and systematic review. http://www.ncbi.nlm.nih.gov/pubmed/28294322. Accessed 28 July 2020
Kouchaki E, Tamtaji OR, Salami M, Bahmani F, Daneshvar Kakhaki R, Akbari E, Tajabadi-Ebrahimi M, Jafari P, Asemi Z (2017) Clinical and metabolic response to probiotic supplementation in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled trial. http://www.ncbi.nlm.nih.gov/pubmed/27669638. Accessed 28 July 2020
Collado MC, Isolauri E, Salminen S, Sanz Y (2009) The impact of probiotic on gut health. http://www.ncbi.nlm.nih.gov/pubmed/19149514. Accessed 28 July 2020
Plaza-Diaz J, Fernandez-Caballero JA, Chueca N, Garcia F, Gomez-Llorente C, Saez-Lara MJ, Fontana L, Gil A (2015) Pyrosequencing analysis reveals changes in intestinal microbiota of healthy adults who received a daily dose of immunomodulatory probiotic strains. http://www.ncbi.nlm.nih.gov/pubmed/26016655. Accessed 28 July 2020
Plaza-Diaz J, Gomez-Llorente C, Campana-Martin L, Matencio E, Ortuno I, Martinez-Silla R, Gomez-Gallego C, Periago MJ, Ros G, Chenoll E, Genoves S, Casinos B, Silva A, Corella D, Portoles O, Romero F, Ramon D, Perez de la Cruz A, Gil A, Fontana L (2013) Safety and immunomodulatory effects of three probiotic strains isolated from the feces of breast-fed infants in healthy adults: SETOPROB study. http://www.ncbi.nlm.nih.gov/pubmed/24205115. Accessed 28 July 2020
Menendez A, Ferreira RB, Finlay BB (2010) Defensins keep the peace too. http://www.ncbi.nlm.nih.gov/pubmed/20016512. Accessed 28 July 2020
Milling S, Yrlid U, Cerovic V, MacPherson G (2010) Subsets of migrating intestinal dendritic cells. http://www.ncbi.nlm.nih.gov/pubmed/20193024. Accessed 28 July 2020
Maisetta G, Batoni G, Esin S, Luperini F, Pardini M, Bottai D, Florio W, Giuca MR, Gabriele M, Campa M (2003) Activity of human beta-defensin 3 alone or combined with other antimicrobial agents against oral bacteria. http://www.ncbi.nlm.nih.gov/pubmed/14506056. Accessed 28 July 2020
Ouhara K, Komatsuzawa H, Yamada S, Shiba H, Fujiwara T, Ohara M, Sayama K, Hashimoto K, Kurihara H, Sugai M (2005) Susceptibilities of periodontopathogenic and cariogenic bacteria to antibacterial peptides, {beta}-defensins and LL37, produced by human epithelial cells. http://www.ncbi.nlm.nih.gov/pubmed/15886266. Accessed 28 July 2020
Oppenheim FG, Xu T, McMillian FM, Levitz SM, Diamond RD, Offner GD, Troxler RF (1988) Histatins, a novel family of histidine-rich proteins in human parotid secretion. Isolation, characterization, primary structure, and fungistatic effects on Candida albicans. http://www.ncbi.nlm.nih.gov/pubmed/3286634. Accessed 28 July 2020
Durr UH, Sudheendra US, Ramamoorthy A (2006) LL-37, the only human member of the cathelicidin family of antimicrobial peptides. http://www.ncbi.nlm.nih.gov/pubmed/16716248. Accessed 28 July 2020
Altman H, Steinberg D, Porat Y, Mor A, Fridman D, Friedman M, Bachrach G (2006) In vitro assessment of antimicrobial peptides as potential agents against several oral bacteria. http://www.ncbi.nlm.nih.gov/pubmed/16687459. Accessed 28 July 2020
Siqueira WL, Margolis HC, Helmerhorst EJ, Mendes FM, Oppenheim FG (2010) Evidence of intact histatins in the in vivo acquired enamel pellicle. http://www.ncbi.nlm.nih.gov/pubmed/20351356. Accessed 28 July 2020
Groenink J, Ruissen AL, Lowies D, van ‘t Hof W, Veerman EC, Nieuw Amerongen AV (2003) Degradation of antimicrobial histatin-variant peptides in Staphylococcus aureus and Streptococcus mutans. http://www.ncbi.nlm.nih.gov/pubmed/12939363. Accessed 28 July 2020
Funding
The work was supported by the Grant FIOUCH 17/011 from Dirección de Investigación, Facultad de Odontología, Universidad de Chile.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the ethics committee of the Faculty of Dentistry at the University of Chile (certificate no. 2011/14) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained in writing from the children’s parents or legal guardian.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sandoval, F., Faleiros, S., Cabello, R. et al. The consumption of milk supplemented with probiotics decreases the occurrence of caries and the salivary concentration of hβD-3 in children. Clin Oral Invest 25, 3823–3830 (2021). https://doi.org/10.1007/s00784-020-03712-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-020-03712-8