
Abstract
Objectives
To investigate the influence of orthodontic materials, field of view (FOV), and artifact reduction (AR) on the assessment of approximal caries using cone beam computed tomography.
Materials and methods
Forty non-cavitated and restoration-free human premolars and molars ranging from sound to various grades of lesions without cavitations were assigned to 13 groups with different combination of fix appliance equipment. CBCT (cone beam computed tomography) (Planmeca ProMax 3D Mid, Helsinki, Finland) images were obtained using combinations of three orthodontic bracket materials and two orthodontic archwire with small and large FOVs and with and without AR activation. Receiver operating characteristic (ROC) analysis was used to calculate the area under the ROC curve (AUC).
Results
Interobserver agreement ranged from 0.44 to 0.92 and intraobserver agreement ranged from 0.50 to 0.99. Teeth lacking orthodontic materials had the highest Az values at 0.84. FOV and AR activation did not significantly affect AUC values (P > 0.05). The AUC data were significantly reduced by the addition of stainless steel wire, NT wire, or a combination of a stainless steel bracket with stainless steel wire (P < 0.05).
Conclusions
The addition of stainless steel wire, NT wire, or a stainless steel bracket with stainless steel wire combination prevented the diagnosis of non-cavitated interproximal tooth caries by CBCT. With and without AR modes and different FOVs did not influence the diagnosis of interproximal caries lesions with different types of orthodontic equipment.
Clinical relevance
A wide variety of brackets and wire combinations are used in the clinic; however, the extent to which these combinations impact the diagnosis of caries by CBCT as the effects of FOV and AR algorithms are unknown.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fixed orthodontic equipment increases plaque accumulation and complicates oral care. Such factors increase the progression of existing caries, and decalcification, which itself leads to cavities and causes cosmetic problems. Thus, the early diagnosis of decalcification and caries are necessary for adequate treatment. Traditional radiographic methods including bitewing, periapical, and panoramic views are routinely used; however, cone beam computed tomography (CBCT) is also used to evaluate orthodontic treatments for multiple reasons. Thus, knowledge of caries’ diagnosis using CBCT, and the effects of both bracket systems and CBCT modalities on images, is essential for dentists.
Studies of the effectiveness of CBCT have found that it is similar to that of traditional methods with regard to identifying interproximal caries without cavitations [1,2,3]. However, beam hardening occurs with metallic restorations; thus, such factors must be considered [4]. Few studies have examined the effects of bracket systems on the diagnosis of caries [5]. Sanders et al. [5] examined artifacts formed by acryl, stainless steel, porcelain, and titanium brackets on CBCT images; they found that stainless steel and titanium brackets increased the numbers of artifacts. Notably, previous studies have not evaluated archwire, brackets, or wire combinations, which are used in the clinic. However, different methods have been recommended for artifact reduction (AR) in CBCT, which may provide better images [6]. Investigations of the effects of AR algorithms on the accuracy of caries diagnosis using different orthodontic material combinations will inform clinicians in this regard. Another factor that affects image quality is the field of view (FOV). Previous studies have shown that FOV has a significant effect on mean gray values in images [7]. With regard to diagnosis of artificial implant defects, Pinheiro et al. reported that the most successful results were obtained with a small FOV [8].
A wide variety of brackets and wire combinations are used in the clinic; however, the extent to which these combinations impact the diagnosis of caries by CBCT is unknown, as are the effects of FOV and AR algorithms. In addition, the overall effect of these combinations on the diagnosis of caries using CBCT has not been determined. The selection criteria of the materials used in the study was determined due to the most commonly usage of orthodontic materials chosen in orthodontic practice.
Thus, this study examined the effects of different bracket types, wires, and combinations with and without AR algorithms using small and large FOVs.
Materials and methods
This study was approved by the Gaziantep University Faculty of Medicine Ethic Committee Presidency (Protocol code: 407).
A total of 40 permanent human molars and premolars that were extracted for orthodontic and periodontal reasons were included in the study. Sample size was determined by a power analysis with 70% power and 95% confidence. The selection criteria for teeth were no cracks and restorations, no developmental anomalies or hypo-plastic structures, ranging from sound teeth to teeth containing various grades of lesions without cavitations. Two premolars and two molars were embedded into silicon blocks (Zetaplus, Zhermack, Italy) and 10 silicon molds were obtained from the 40 teeth.
Settings
To test the artifact behavior, four different bracket materials were applied to all premolars in the following order: stainless steel, ceramic, and plastic meanwhile molar teeth had molar tubes. In addition, molar tubes were applied to molar teeth, whereas premolar control teeth had no material added. Each combination was applied to all silicon molds in order. At the first stage, no archwire was added, to analyze the effect of bracket material alone and CBCT images were recorded.
At the second stage, stainless-steel archwire material was applied to each type of bracket material in the following order: stainless steel, ceramic, and plastic. Following the CBCT analyses, NITI archwire materials were applied to each type of bracket material in the following order to analyze combinations: stainless steel, ceramic, and plastic. As a control group, all teeth were scanned with no material added. At the end, 13 working groups had been created. As an adhesive, 3 M Transbond XT orthodontic adhesive was used The characteristics of the included materials are shown in Table 1.
After sample preparation, teeth were scanned with a CBCT system with small and large FOVS, with and without AR option.
Tomography scans were performed using a CBCT device (Planmeca ProMax 3D Mid, Helsinki, Finland); all images were obtained using conditions of 90 kVp and 12 mA. For small FOV (SFOV), 0.15 mm voxel and (Ø40 × 50 mm) was used. Large FOV (LFOV) was obtained using 0.20 mm voxel and the (Ø160 × 90 mm) standard. All combinations of orthodontic materials with small and large FOVs were imaged with and without application of the AR option (Romexis software, Planmeca) in high mode. To mimic the soft tissue, blocks containing teeth were also imaged inside a 1 mm thick plastic container with water. A total of 520 CBCT images were recorded, and 3120 surfaces were evaluated.
Caries were scored independently by two examiners (Öİ, AMA), with a total of 80 mesial and distal surfaces being evaluated.
For each approximal surface, the observers scored caries using a 5-step confidence scale as follows: 0, radiolucency absent; 1, radiolucency in 1/2 of the enamel; 2, radiolucency in all of the enamel; 3, radiolucency up to 1/2 of the dentin; 4, radiolucency to the pulpal dentin. To assess intraobserver reliability, assays were repeated again after 2 weeks.
Histologic validation
Teeth were cut in half at the deepest point of the caries using an Isomet (Buehler, Lake Bluff, IL, USA). Then images of the divided teeth were obtained using a stereo microscope (Leica, Wetzlar, Germany) at a 25x magnification. Images were analyzed using the Leica Application Suite software. The evaluation criteria for the histological findings were as follows: 0, demineralization absence; 1, demineralization including 1/2 of the enamel; 2, demineralization including all of the enamel; 3, demineralization including up to 1/2 of the dentin; 4, demineralization to the pulpal dentin.
Three separate thresholds were used to evaluate the diagnosis of enamel and dentin caries as.
T1 threshold (adopted score 0 as sound), T2 threshold (adopted scores 1 and 2 as enamel caries), and T3 threshold (adopted scores 3 and 4 as dentin caries).
. All of the statistical calculations were performed in the Statistics Department of Gaziantep University using Statistical Package for the Social Sciences (SPSS v16.0 IBM, Chicago, IL, USA) and MedCalc programs (version 18.11 Ostend, Belgium. To examine the interobserver and intraobserver agreement, an intraclass correlation (ICC) was used. Area under the ROC curve values were compared using MedCalc. Paired sample t tests were used to compare the effects of AR and FOV. A P value < 0.05 was considered statistically significant.
Results
Histological scores for 80 surfaces were evaluated separately. A total of 32 surfaces had a score of 0 (no demineralization), 11 had a score of 1 (demineralization including 1/2 of the enamel), 9 had a score of 2 (demineralization including the entire enamel surface), 23 had a score of 3 (demineralization to 1/2 of the dentine), and 5 had a score of 4 (demineralization to the pulpal dentine). Intraobserver and interobserver agreements are shown in Table 2.
The highest level of intraobserver agreement was obtained for the plastic bracket, porcelain bracket, and steel wire group (ICC 0.99), whereas the lowest was obtained in the NITI wire group (ICC 0.50). The level of agreement between observers was highest in the plastic bracket group (ICC 0.92), whereas it was lowest in the steel bracket group (ICC 0.44).
The sensitivity and specificity of groups are shown in Table 3. Paired t test analyses demonstrated statistically significant differences for scores of some groups: the steel bracket group between SFOVAR and LFOV, the SFOV-LFOV steel wire group between SFOVAR and LFOV, LFOV-LFOVAR, NITI wire between SFOVAR and LFOVAR, SFOVAR-LFOV and molar tubes between SFOV-LFOVAR, and SFOVAR-LFOVAR (Table 4). The highest area under the curve (AUC) value (0.84) was obtained from the without bracket group at T1, with LFOV but without artifact reduction. The lowest AUC value belonged to molar tubes at T3 (0.555) with LFOV and artifact reduction, then to the stainless steel wire group at T1 (0.575) (LFOV without AR). When comparing all of the groups’ AUC values, T1, T2, and T3 did not show statistically significant differences in the diagnosis of caries (P > 0.05). However, a decrease in the AUC values was observed at T1 and T2 for the control group (without brackets) compared to the steel wire (T2 LFOV without AR) (P = 0.03), NITI wire (T1 SFOV with AR) (P = 0.04), and steel bracket and steel wire (T1 LFOV without AR) (P = 0.03) groups. Conversely, no significant differences in AUC values were observed at T3 (P > 0.05). FOV and AR activation did not significantly affect AUC values (P > 0.05). Figure 1 shows the effects of FOV and AR on CBCT images.

CBCT images of NITI wire group. a Small field of view without artifact reduction, b small field of view with artifact reduction, c large field of view without artifact reduction, and d large field of view with artifact reduction.
Discussion
Orthodontists frequently use CBCT for orthognathic surgery, airway measurements, and the evaluation of root resorption. Although CBCT is not the gold standard approach for caries diagnosis in routine clinical dental practice, images obtained for other reasons can be examined for the detection of any existing pathology [9]. The incidence of caries increases, particularly when orthodontic equipment has been used [10, 11].
Thus, it is important for dentists to carefully diagnose caries early to maintain oral health, to plan preventive procedures, and to avoid economic losses.
To obtain high diagnostic success, it is necessary to combine high sensitivity and high specificity detection methods. In this study, when sensitivity and specificity were evaluated separately, it was noted that sensitivity increases as specificity decreases particularly when metallic equipment was used (Table 3). For example, the T1 (SFOV with AR) stainless steel wire teeth had a sensitivity of 97.82% and a specificity of 18.82%. Conversely, T1 (LFOV without AR) bracket-free teeth had a sensitivity of 83.48% and a specificity of 84.51%. In addition, similar results were obtained for different groups during the study. These data are similar to those of Kuzczy et al., [9] who found that metal equipment reduced the success of detecting caries by CBCT. However, in contrast to published data [9, 12, 13], the present study showed higher ranges for sensitivity and lower ranges for specificity in the control group (WB). In a study by Kulczyk et al., the number of histologically confirmed carious dentin lesions was small: only 12 of 68 and 13 of 68 in surfaces next to fillings and surfaces distal to fillings [9], respectively. In a study by Haiter-Neto et al., microscopy showed that approximal surfaces were 63% sound and 37% carious [13]. However, in the present study, 32 surfaces were histologically scored as sound and 48 were scored as carious. This differentiation between ratios of carious dentin surfaces to sound surfaces may affect statistical outcomes.
In a study by Haiter-Neto et al., the sensitivity values were determined to be significantly affected for approximal caries detection when CBCT devices from different manufacturers were used [13]. Previous studies used CBCT devices from different manufacturers, as well as different FOVs and voxels [9, 12, 13]. These differences in sample width and statistical power may have affected the statistical outcomes.
Schwendicke et al. [12] also demonstrated limited sensitivity and high specificity for initial approximal carious lesions. However, they presented a meta-analysis with intraoral radiography (i.e., bitewing or periapical radiographs); their study did not differentiate between the radiographic techniques used [12] . In contrast, the present study focused only CBCT-based caries detection. Outcomes may differ based on the study design, imaging technique, degree of knowledge, and number of observers. In the investigation by Schwendicke et al., carious lesions under clinical and in-vitro conditions were investigated; comparison between in-vitro and in-vivo conditions suggested that observers may overestimate sensitivity and underestimate specificity [12] . This phenomenon should be considered when interpreting the reported heterogeneity between studies.
X-rays are absorbed by teeth containing metal with limited light from the space behind the material reaching the detector. Thus, such occurrences may cause artifacts (i.e., disappearance artifact) [14] that are interpreted as caries. While this condition increases sensitivity it may cause caries to be misinterpreted (Fig. 2). In this study, high sensitivity and low specificity values were observed in groups that contained steel and NITI, as well as in groups that contained acryl and porcelain. Although the lowest sensitivity and highest specificity were observed in dentin caries, AUC values did not significantly vary among T1, T2, and T3. Thus, the successful diagnosis of caries was not affected by the level of caries in each bracket and wire combination.

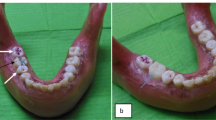
a Microscopic image of a section of premolar and molar teeth. b Corresponding CBCT scans of teeth without any orthodontic material, c corresponding CBCT scans of teeth with stainless steel wire. Note that CBCT examinations of teeth with stainless steel wire suggests more severe demineralization relative to bracket-free, and histological views.
ROC analyses were used in this study; these analyses evaluate sensitivity and specificity, and are recommended for diagnostic purposes in medicine and dentistry [15]. AUC values indicated that caries diagnosis was most successful (0.84) in the bracket-free group at T1 (LFOV without AR)The least successful group (0.55) (LFOV with AR) was the molar tube group at T3, followed by the stainless steel wire group (0.575) at T1 (LFOV without AR). In a study by et al. [16], the area under the ROC curve for teeth that did not include restorative materials was 0.568. In similar studies, Zhang et al. [2] observed an AUC of 0.528, while Kalathingal et al. [17] observed an AUC of 0.82 when CBCT was used. Thus, AUC values vary in accordance with observers’ attention and experience. In addition, caries and the number of healthy teeth should also be considered when determining sensitivity, specificity, and AUC values [18].
Although the CBCT image quality of teeth without restorations and brackets is generally good, many patients have additional materials, including implants, amalgams, and brackets, which cause artifacts [5, 9] . Sanders et al. [5] examined teeth with interproximal defects containing steel, titanium, plastic, and ceramic brackets and found that metal and titanium brackets significantly affected interpretation.
Kulczyk et al. [9] investigated the effects of amalgam restorations on the diagnosis of interproximal caries using CBCT and found that diagnosis was insufficient due to low specificity. Moreover, Neto et al. [19] examined the Hausdorff Distance units for CBCT images with bracket-free, steel bracketed, and steel wire on steel bracketed teeth where they found that image quality was satisfactory despite the presence of orthodontic equipment. Consistent with this, the current study found that when bracket and wire combinations were compared to the bracket-free, groups, no significant difference between AUC values among T2 and T3 groups were observed. However, when caries smaller than ½ of the enamel were included, steel wire, NITI wire, and steel bracket and steel wire groups had significantly lower AUC values, compared to the bracket-free, d groups. Thus, when steel and NT equipment is used during caries diagnosis with CBCT, small caries go undiagnosed. In this case, it was difficult to determine enamel lesions with metallic orthodontic equipment, which delayed treatment.
Hence, alternative methods are needed for artifact reduction without increasing the exposure dose. AR was examined in this study as a possible approach for achieving this objective with regard to orthodontic equipment. Bechara et al. [6] used AR for the diagnosis of artificial root fractures; they reported that the highest accuracy values were obtained without the use of AR [20] . Candemil et al. evaluated the effectiveness of AR in CBCT artifacts arising from metallic objects in the exomass, and concluded that AR was not effective in improving CBCT artifacts from the two different CBCT units used [21].
Kamburoğlu et al. compared peri-implant defects and obtained similar results with and without different AR modes [22] . De Rezende Barbosa et al. evaluated the diagnostic success of AR in cases with metallic posts and reported better results using AR [23] . Queiroz et al. investigated the efficacy of AR in CBCT for different dental materials and concluded that the use of AR significantly reduced image noise around the dental amalgam and Cu–Al alloy cylinders [24] .
In the present study, however, the paired test results were affected by changing AR, in a manner similar to that reported by Kamburoğlu et al. [22] AR did not significantly affect the accuracy of caries diagnosis. These different outcomes in the literature might be a result of the examination of different types of lesions, examination of different dental materials, and the observers’ subjective interpretations.
FOV may affect mean gray values, interpretation, and success of diagnosis [7, 8]. Pinheiro et al. evaluated peri-implant defects and noted that most successful diagnoses were obtained with SFOV (4 cm × 4 cm) [8] .
Da Silveira et al. measured the artificial internal root resorption at LFOV (voxel size 0.200, 0.250) and SFOV (voxel size 0.076, 0.1000); they noted that the voxel size changed resolution, but did not cause significant differences in the results [25] . Shokri et al. evaluated metal artifacts of dental implants by using large (6 × 8 cm2) and small (4 × 6 cm2) FOVs and stated that a smaller FOV significantly reduced metal artifacts around implants [26] .
In the current study, however, paired test results were affected by changing FOV, similar to the findings Da Silveira et al. [25]; notably, the difference between SFOV and LFOV was not significant for AUC values. The present study was performed to diagnose caries lesions, and did not focus on mean gray values. Therefore, differences in methodology may have affected the interpretation and results.
Although working conditions were standardized during scoring, their perspectives and interpretations may have differed. While the agreement between observers ranged from fair to strong, intraobserver agreement ranged from moderate to strong. Thus, this coherent variability may affect the interpretation. In addition, the study was performed in vitro, and therefore did not account for true clinical conditions such as soft tissue imaging and movement artifacts. Therefore, future studies are anticipated to provide more detailed information regarding caries diagnosis using CBCT.
Conclusion
Fixed appliance equipment, such as steel wire, NITI wire, and steel brackets, increased the sensitivity ranges for the diagnosis of interproximal lesions, compared with the bracket-free control group. Conversely, the specificity ranges decreased in samples with appliance equipment. Because of these material artifacts, we suggest the use of caution when interpreting images from teeth containing fixed appliances.
All CBCT images obtained with and without AR modes and different FOVs showed no difference in the diagnosis of interproximal caries lesions with different types of orthodontic equipment.
References
Tsuchida R, Araki K, Okano T (2007) Evaluation of a limited cone-beam volumetric imaging system: comparison with film radiography in detecting incipient proximal caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104:412–416. https://doi.org/10.1016/j.tripleo.2007.02.028
Zhang ZL, Qu XM, Li G, Zhang ZY, Ma XC (2011) The detection accuracies for proximal caries by cone-beam computerized tomography, film, and phosphor plates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 111:103–108. https://doi.org/10.1016/j.tripleo.2010.06.025
Qu X, Li G, Zhang Z, Ma X (2011) Detection accuracy of in vitro approximal caries by cone beam computed tomography images. Eur J Radiol 79:e24–e27. https://doi.org/10.1016/j.ejrad.2009.05.063
Aglarci OS, Bilgin MS, Erdem A, Ertas ET (2015) Is it possible to diagnose caries under fixed partial dentures with cone beam computed tomography? Oral Surg Oral Med Oral Pathol Oral Radiol 119:579–583. https://doi.org/10.1016/j.oooo.2015.02.004
Sanders MA, Hoyjberg C, Chu CB, Leggitt VL, Kim JS (2007) Common orthodontic appliances cause artifacts that degrade the diagnostic quality of CBCT images. J Calif Dent Assoc 35:850–857
Bechara BB, Moore WS, McMahan CA, Noujeim M (2012) Metal artefact reduction with cone beam CT: an in vitro study. Dentomaxillofac Radiol 41:248–253. https://doi.org/10.1259/dmfr/80899839
Rodrigues AF, Campos MJ, Chaoubah A, Fraga MR, Farinazzo Vitral RW (2015) Use of gray values in CBCT and MSCT images for determination of density: influence of variation of FOV size. Implant Dent 24:155–159. https://doi.org/10.1097/ID.0000000000000179
Pinheiro LR, Scarfe WC, Augusto de Oliveira Sales M, Gaia BF, Cortes AR, Cavalcanti MG (2015) Effect of cone-beam computed tomography field of view and acquisition frame on the detection of chemically simulated peri-implant bone loss in vitro. J Periodontol 86:1159–1165. https://doi.org/10.1902/jop.2015.150223
Kulczyk T, Dyszkiewicz Konwinska M, Owecka M, Krzyzostaniak J, Surdacka A (2014) The influence of amalgam fillings on the detection of approximal caries by cone beam CT: in vitro study. Dentomaxillofac Radiol 43:20130342. https://doi.org/10.1259/dmfr.20130342
Gorelick L, Geiger AM, Gwinnett AJ (1982) Incidence of white spot formation after bonding and banding. Am J Orthod 81:93–98
Mizrahi E (1982) Enamel demineralization following orthodontic treatment. Am J Orthod 82:62–67
Schwendicke F, Tzschoppe M, Paris S (2015) Radiographic caries detection: a systematic review and meta-analysis. J Dent 43:924–933. https://doi.org/10.1016/j.jdent.2015.02.009
Haiter-Neto F, Wenzel A, Gotfredsen E (2008) Diagnostic accuracy of cone beam computed tomography scans compared with intraoral image modalities for detection of caries lesions. Dentomaxillofac Radiol 37:18–22. https://doi.org/10.1259/dmfr/87103878
Prell D, Kyriakou Y, Struffert T, Dörfler A, Kalender W (2010) Metal artifact reduction for clipping and coiling in interventional C-arm CT. Am J Neuroradiol 31:634–639
Obuchowski NA (2003) Receiver operating characteristic curves and their use in radiology 1. Radiology 229:3–8
Valizadeh S, Tavakkoli MA, Karimi Vasigh H, Azizi Z, Zarrabian T (2012) Evaluation of cone beam computed tomography (CBCT) system: comparison with intraoral periapical radiography in proximal caries detection. J Dent Res Dent Clin Dent Prospects 6:1–5. https://doi.org/10.5681/joddd.2012.001
Kalathingal SM, Mol A, Tyndall DA, Caplan DJ (2007) In vitro assessment of cone beam local computed tomography for proximal caries detection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104:699–704. https://doi.org/10.1016/j.tripleo.2006.08.032
Hintze H, Frydenberg M, Wenzel A (2003) Influence of number of surfaces and observers on statistical power in a multiobserver ROC radiographic caries detection study. Caries Res 37:200–205. https://doi.org/10.1159/000070445
Rino Neto J, Silva FP, Chilvarquer I, Paiva JB, Hernandez AM (2012) Hausdorff distance evaluation of orthodontic accessories’ streaking artifacts in 3D model superimposition. Braz Oral Res 26:450–456
Bechara B, Alex McMahan C, Moore WS, Noujeim M, Teixeira FB, Geha H (2013) Cone beam CT scans with and without artefact reduction in root fracture detection of endodontically treated teeth. Dentomaxillofac Radiol 42:20120245. https://doi.org/10.1259/dmfr.20120245
Candemil AP, Salmon B, Freitas DQ, Ambrosano GMB, Haiter-Neto F, Oliveira ML (2019) Are metal artefact reduction algorithms effective to correct cone beam CT artefacts arising from the exomass? Dentomaxillofac Radiol 48:20180290. https://doi.org/10.1259/dmfr.20180290
Kamburoglu K, Kolsuz E, Murat S, Eren H, Yuksel S, Paksoy CS (2013) Assessment of buccal marginal alveolar peri-implant and periodontal defects using a cone beam CT system with and without the application of metal artefact reduction mode. Dentomaxillofac Radiol 42:20130176. https://doi.org/10.1259/dmfr.20130176
de Rezende Barbosa GL, Sousa Melo SL, Alencar PN, Nascimento MC, Almeida SM (2016) Performance of an artefact reduction algorithm in the diagnosis of in vitro vertical root fracture in four different root filling conditions on CBCT images. Int Endod J 49:500–508. https://doi.org/10.1111/iej.12477
Queiroz PM, Groppo FC, Oliveira ML, Haiter-Neto F, Freitas DQ (2017) Evaluation of the efficacy of a metal artifact reduction algorithm in different cone beam computed tomography scanning parameters. Oral Surg Oral Med Oral Pathol Oral Radiol 123:729–734. https://doi.org/10.1016/j.oooo.2017.02.015
Da Silveira PF, Fontana MP, Oliveira HW, Vizzotto MB, Montagner F, Silveira HL et al (2015) CBCT-based volume of simulated root resorption - influence of FOV and voxel size. Int Endod J 48:959–965. https://doi.org/10.1111/iej.12390
Shokri A, Jamalpour MR, Khavid A, Mohseni Z, Sadeghi M (2019) Effect of exposure parameters of cone beam computed tomography on metal artifact reduction around the dental implants in various bone densities. BMC Med Imaging 19:34. https://doi.org/10.1186/s12880-019-0334-4
Acknowledgments
The authors would like to thank Prof. Dr. Hasan Hüseyin Yılmaz for his contributions as a scientific advisor.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This study was approved by the Gaziantep University Faculty of Medicine Ethic Committee Presidency (Protocol code: 407).
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Isman, O., Aktan, A.M. & Ertas, E.T. Evaluating the effects of orthodontic materials, field of view, and artifact reduction mode on accuracy of CBCT-based caries detection. Clin Oral Invest 24, 2487–2496 (2020). https://doi.org/10.1007/s00784-019-03112-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03112-7