
Abstract
Objectives
Obstructive sleep apnea syndrome (OSAS) becomes increasingly important. For diagnosis and surgery, computed tomography (CT), and cone beam computed tomography (CB-CT) are used equally, although in most of cases, patient positioning differs between supine positioning (CT) and upright seating positioning (CB-CT). We measured volumetric and anatomical changes in the posterior airway space (PAS) between upright and supine positioning in a three-dimensional set up.
Materials and methods
Coherent CT and CB-CT scans of 55 patients were included in the study. Using Brainlab ENT 3.0, image data was superimposed, and three-dimensional models were segmented. PAS height, cross-sectional area, vertical and horizontal position of the mandible and hyoid, and volumetric analyses of the three-dimensional models were measured.
Results
PAS height and cross-sectional area were significantly higher in CB-CT compared to CT scans (p < 0.001). In the vertical dimension, the mandible and hyoid were localized more caudally in CB-CT in contrast to CT scans (p < 0.04; p < 0.001). Three-dimensional evaluation showed a greater volume of the PAS in CB-CT (p < 0.0001). Pearson correlation coefficient showed a correlation between vertical positioning of the mandible and hyoid compared to the positioning of the patient.
Conclusions
Patient positioning during CT and CB-CT has an effect on the location of anatomical structures like the mandible and hyoid and changes the dimensions and volume of the posterior airway space significantly.
Clinical relevance
The radiological technique used and the positioning of the patient should be taken into account when considering further surgical therapy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Untreated obstructive sleep apnea syndrome (OSAS) leads to cardiopulmonary complications such as hypertension, unstable heart frequency, and economic damage due to fatigue [1, 2]. In 1993, Young et al. stated that up to 2–4% of the US population suffer from sleep-disordered breathing [3]. Recent studies from Western-Europe even assume a prevalence of 23.4 and up to 49% regarding OSAS [4].
In contrast to central sleep apnea syndrome, OSAS is characterized as an obstruction of the posterior airway space (PAS) leading to apnea with a drop of oxygen saturation resulting in an awakening. Direct effects are sleepiness and lack of concentration during the day. Major implications are hypertension, cardiovascular diseases, and even diabetes mellitus type 2 [5].
Besides the STOP-BANG questionnaire as a screening method, OSAS is assessed by sleep polysomnography calculating the apnea-hypopnoea index (AHI). An AHI > 15 (events/h) or an AHI > 5 with typical clinical symptoms are considered as a manifest of OSAS [6].
One of the main risk factors of OSAS is obesity leading to a sixfold greater risk [7]. Besides smoking [8] and hormonal disorder [9], the anatomical structure of the PAS plays a central role in the occurrence of OSAS. Previous studies were able to show a correlation between OSAS occurrence and a small cross-sectional area of the PAS [10]. The significantly lower PAS in OSAS patients is not restricted to obese patients, as shown by Thapa et al. [11]. Especially adenoids, hypertrophic tonsils, an enlarged soft palate and the horizontal dimension of the maxilla contribute to a narrowing of the upper airway leading to a higher risk for obstruction [12, 13]. In the majority of OSAS patients, the obstruction of the PAS is located retropalatal and retrolingual because of a loose soft palate and tongue [14].
Obstructive sleep apnea syndrome therapy contains conservative and invasive approaches. The most common conservative therapy implies lifestyle change to achieve weight loss and continuous positive airway pressure (CPAP), which is poorly accepted by patients. Custom-fitted oral appliances for mandible protrusion serve as a second-line therapy in cases of CPAP failure [15].
In severe or therapy-resistant cases, surgical therapy is indicated. The surgical approaches like uvulopalatopharyngoplasty (UPPP) and mandibulo-maxillary-advancement (MMA) target the upper airway to reduce airflow resistance and obstruction [16, 17]. Different surgical approaches target variable sites of PAS obstruction. Mandibulo-maxillary-advancement for example leads to an enlargement of the retrolingual and retropalatal airway, whereas UPPP mainly addresses retropalatal obstructions [18].
Prior to the surgical therapy, such as MMA, preoperative radiological diagnostics like computed tomography (CT) or cone beam CT (CB-CT) scans are essential to visualize the individual anatomical structures [19, 20]. Both radiological techniques are able to evaluate the upper airway equally [21, 22]. Despite the different recording techniques and radiation exposures, the positioning of the patient varies. In contrast to a CT scan, in which the patient is in a supine position, most of the CB-CT scans are conducted in an upright seating position. Studies show differences in the upper airway morphology between the supine and upright positions, assuming an impact on the posterior airway space [23]. Differences in the upper airway morphology depending on the patient positioning may lead to misdiagnosis and false treatment regarding surgical intervention.
Whereas the PAS is defined as a volume, most of the available studies deal with two-dimensional evaluations [23] to only give an estimation of the changes in the PAS. Studies show differences in the upper airway morphology and position of bony structures like the hyoid, between the supine and upright positions, assuming an impact on the posterior airway space [23, 24].
This study was designed to evaluate volumetric and anatomical changes in the PAS between upright and supine positioning, depending on the recording technique, in a three-dimensional setup by creating virtual three-dimensional models of the PAS. Furthermore the influence of anatomical structures like the mandible and the hyoid on the PAS was investigated.
Patients and methods
The study was approved by the local ethics committee. After scanning the internal clinic database for patients with coherent CT and CB-CT scans, 55 patients were included in the study. All patients (29 women and 26 men; mean age 52 ± 19.6 years) received radiological diagnostics, CT and CB-CT scans. Mean time difference between CT and CB-CT scans was 275 ± 353 days. Investigations with insufficient image quality, trauma, or abscess-formation in the represented scans and intubated patients were excluded from the study.
Computed tomography was done with a “Somatom Definition Flash” (Siemens, Erlangen, Germany) and a slice thickness of 1 mm in a supine position. For the CB-CT scans, patients were in an upright position using Galileos (Sirona, Wals, Austria) with a voxel size of 0.3 × 0.3 × 0.3 mm.
Image registration
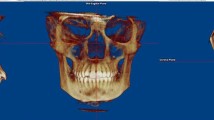
CT and CB-CT data were exported using Digital Imaging and Communications in Medicine (DICOM) format and imported into Brainlab ENT 3.0 (Brainlab, Munich, Germany). Using the implemented “Autofusion” option, the corresponding CT and CB-CT were superimposed. Beforehand, the maxilla, zygoma, and palate were, due to their immobility, selected as a “regions of interest” for the registration process (Fig. 1).

Superimposition of CT (blue) and CB-CT (orange) scans using Brainlab ENT 3.0 showing PAS model margins (CT: purple/blue; CB-CT: orange/yellow)
Segmentation and cropping of posterior airway space
Following the segmentation procedure of the PAS, the three-dimensional models were cropped. The palatal plane from the spina nasalis anterior to spina nasalis posterior represented the cranial margin of the PAS. The caudal border was defined as a parallel plane through the tip of the epiglottis.
Consecutively, all PAS models were divided into an upper and lower part by a parallel plane through the tip of the soft palate (Fig. 2a).

a PAS model gets divided into an upper and lower part, b vertical position of the mandible, c horizontal position of the mandible, d angle of inclination of the dens axis
The final cropped three-dimensional models of the PAS were saved and exported in STL format.
Distance and positioning measurements
Measurements were conducted in Brainlab ENT in the midsagittal plane.
The vertical position of the mandible was determined as the rectangular distance between the palatal plane and the most anterior point of the mandible (Fig. 2b). A plump from the palatal plane and spina nasalis posterior was used to measure the horizontal distance to the mandible (Fig. 2c). Additionally, the angle between the palatal plane, spina nasalis posterior, and the mandible was registered.
Vertical and horizontal positions of the hyoid were registered in line with the measurements of the mandible.
To evaluate changes in the upper spine in supine and upright positioning, the angle of inclination of the dens axis was recorded (Fig. 2d). Therefore, the angle between the palatal plane and a constructed line through the midpoint and tip of the dens axis has been measured.
The height of the upper (palatal plane—tip of the soft palate) and lower (tip of the soft palate—tip of the epiglottis) PAS was assessed in the midsagittal plane likewise (Fig. 3).

Measurement of the PAS height
Cross-sectional and volumetric measurements
STL files of the cropped three-dimensional models of the PAS were imported into the software Geomagic Studio 2014 (3D Systems, Rockhill, SC, USA).
The cross-sectional analysis was performed at the upper, middle, and lower cutting surface of the three-dimensional PAS models. After marking the corresponding cutting surface, Geomagic Studio calculated the exact cross-sectional area.
Additionally, the volume of the imported three-dimensional PAS models (upper and lower PAS) was computed fully automated (Fig. 4).

Three-dimensional model of the PAS with marked cross-sectional area (red)
Statistical analysis
Student’s t test and Pearson correlation coefficient were used for statistical analysis. The level of significance was set at p ≤ 0.05. All data are expressed as mean values ± standard deviation. Statistical calculations were performed under StatPlus:mac (AnalystSoft Inc., Walnut, CA, USA) running on a MacOS 10.12 computer.
Results
The registered mean total height of the PAS in the CT scans (48.04 ± 8.34 mm) was significantly lower compared to the CB-CT scans (53.33 ± 8.39 mm; p < 0.0001) (Fig. 5).

Total and upper PAS height
In contrast to the lower part of the PAS (palatal plane—epiglottal plane), which showed no significant deviation between both recording techniques (CT, 16.07 ± 7.38 mm; CB-CT, 17.71 ± 6.55 mm; p = 0.095), the upper part of the PAS was significantly shorter in the CT scans (31.97 ± 4.66 mm) in relation to the CB-CT scans (35.62 ± 5.54 mm; p < 0.0001) (Fig. 5).
In addition, the vertical position of the mandible was located significantly more cranially in the CT scans (58.6 ± 6.73 mm) compared to the CB-CT scans (59.89 ± 7.19 mm; p = 0.04) (Fig. 6). No effect in the horizontal position of the mandible was recorded (CT, 41.79 ± 8.57 mm; CB-CT, 42.28 ± 8.64 mm; p = 0.49).

Vertical position of the mandible and hyoid
In line with the mandible, the vertical position of the hyoid in the CT scans was significantly higher (64.72 ± 8.52 mm) in contrast to the CB-CT scans (67.34 ± 8.34 mm; p < 0.0001) (Fig. 6). The horizontal position of the hyoid did not differ between either recording technique (CT, − 3.16 ± 9.63 mm; CB-CT, − 4.28 ± 10.06 mm; p = 0.31).
Furthermore, the angle of inclination of the dens axis was significantly larger in the CT scans (93.76° ± 8.71°) compared to the CB-CT scans (91.42° ± 8.6°; p = 0.026) (Fig. 7).

Angle of inclination of the dens axis
When comparing the cross sections between CT and CB-CT scans, only the upper cross section showed a significant deviation (CT, 523.58 ± 272.51 mm2; CB-CT, 611.23 ± 251.01 mm2; p = 0.001) (Fig. 8).

Upper cross-sectional area of the PAS
The measured total volume of the three-dimensional models in the CT scans was significantly lower (11.91 ± 7.4 cm3) in relation to the CB-CT scans (15.59 ± 8.11 cm3; p = 0.0001) (Fig. 9). The upper volume of the PAS showed the same distribution (CT, 7.25 ± 3.91 cm3; CB-CT, 10.74 ± 6.37 cm3; p < 0.0001) (Fig. 9); whereas, the lower volume did not differ between either techniques (CT, 4.66 ± 4.63 cm3; CB-CT, 4.84 ± 2.73 cm3; p = 0.76). Measurements are summarized in Table 1.

Total and upper PAS volume
The Pearson correlation coefficient was used to evaluate a dependency between the total height and the total volume of the PAS and the position of the mandible and hyoid.
The total height of the PAS showed a weak correlation to the vertical position of the mandible (r = 0.36; p < 0.0001) and a very strong correlation to the vertical position of the hyoid (r = 0.86; p < 0.0001). In line with the height of the PAS, the volume of the PAS showed a weak correlation to the vertical position of the hyoid (r = 0.35; p < 0.0003), whereas the vertical position of the mandible did not (r = 0.07; p = 0.49).
Discussion
Obstructive sleep apnea syndrome is linked to cardiopulmonary diseases and has a significant economic impact due to fatigue and nonproductive time [1, 2].
The only chance for recovery from failing conservative first-line therapy, like weight loss, CPAP, and oral appliances, is surgical therapy [15]. Therefore, preoperative radiological evaluation is essential to find the anatomical cause for airway obstruction. Based on anatomical variations, the surgical method has to be adapted individually. A widely used technique for three-dimensional visualization is CT [25]. Nowadays, CT scans are available in almost every hospital. One disadvantage is the comparatively high dose of radiation [26].
Using modern CB-CT scanners, the level of radiation can be reduced to one fifth with equivalent quality [22]. Due to lower levels of radiation and almost ubiquitous availability, the use of CB-CT scanners has become popular. Besides the recording technique, one of the main differences between CT and CB-CT is the positioning of the patient during the scanning process. During CT scans, the patient is usually in a supine position, whereby most of the CB-CT scans are being conducted in an upright seating position.
The differences in patient positioning might have a crucial effect on the location of anatomical structures like the mandible or the hyoid, especially in patients suffering from OSAS where the position of anatomical structures influences the PAS fundamentally. Therefore, radiological diagnostics should reflect the exact conditions to minimize misdiagnosis.
Studies already showed a significant difference in PAS cross sections between CT and CB-CT scans, even before the three-dimensional aspect was implemented [23].
Camacho et al. were able to highlight a significant difference in PAS volume in a group of five OSAS patients only, receiving CT and CB-CT scans [27].
In line with previous data, we showed a significant difference in PAS height comparing the supine position of patients in CT scans and the upright seating position in CB-CT scans. Comparing the height of the upper to the lower part of the PAS, it becomes obvious that only the upper part significantly contributes to the changes in height. This supports the thesis that the anatomical location of the soft palate, as the lower border of the upper PAS part, is highly movable especially while switching between supine and upright positioning of the patient.
Schwab et al. stated that airway narrowing predominantly occurs retropalatal and mainly affects the lateral dimension of the airway [12]. Supporting these findings, we were able to show that the upper cross section is significantly larger in an upright seating position. The supine position leads to a narrowing of the PAS, which is linked to a higher upper airway resistance thereby increasing the risk of an OSAS [28]. These findings may have an impact on misdiagnosis of position-dependent OSAS patients too. The usually narrower PAS while sleeping in a supine position is masked by the upright patient positioning during image recording.
The three-dimensional and the two-dimensional data reflect the changes in PAS in different positions. The overall volume of the PAS increases significantly while moving from a supine position to an upright seating position. In line with the PAS height, the change in volume is predominantly located in the upper part of the PAS.
Besides the changes in the PAS height and volume, we showed significant changes in the localization of anatomical structures. The two bony anatomical structures, which might influence the PAS, are the mandible and hyoid.
Common surgical therapy for OSAS is mandibular advancement [29]. In our findings, supine positioning has no influence on the horizontal (anterior–posterior) position of the mandible and hyoid in contrast to the vertical (occipital–caudal) position. In an upright position, the mandible, as well as the hyoid, are located more caudally compared to supine positioning of the patient. The results can be simply explained by gravity, which affects the localization of the mandible and hyoid.
With the help of the Pearson correlation, we showed that the height and volume of the PAS are influenced by the vertical position of the mandible and the hyoid. A more caudal position of the mandible or the hyoid leads to an enhancement of PAS height and volume.
We are aware of the limitation due to the time difference between the CT and CB-CT scans. Furthermore, in our opinion, this is the only way to compare CT and CB-CT scans in such a large sample size and keeping the ethical standard.
The presented data show that radiological CT and CB-CT scans are able to record, process, and display anatomical structures of the PAS with equal image quality. Nonetheless, both recording methods differ in patient positioning leading to different results, especially in PAS diagnostics. The PAS as well as surrounding anatomical structures like the mandible and the hyoid is significantly influenced causing changes in shape and location.
These changes might have an impact on preoperative diagnostics for decision-making concerning surgical treatment of OSAS.
To guarantee valid and reproducible PAS evaluation in line with surgical interventions, it is necessary to pay attention to consistent radiographic recordings and patient positioning.
References
Kapur VK (2010) Obstructive sleep apnea: diagnosis, epidemiology, and economics. Respir Care 55:1155–1167
Ward KL, Hillman DR, James A, Bremner AP, Simpson L, Cooper MN, Palmer LJ, Fedson AC, Mukherjee S (2013) Excessive daytime sleepiness increases the risk of motor vehicle crash in obstructive sleep apnea. J Clin Sleep Med 9:1013–1021. https://doi.org/10.5664/jcsm.3072
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S (1993) The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 328:1230–1235. https://doi.org/10.1056/NEJM199304293281704
Garvey JF, Pengo MF, Drakatos P, Kent BD (2015) Epidemiological aspects of obstructive sleep apnea. J Thorac Dis 7:920–929. https://doi.org/10.3978/j.issn.2072-1439.2015.04.52
Friedman O, Logan AG (2009) The price of obstructive sleep apnea-hypopnea: hypertension and other ill effects. Am J Hypertens 22:474–483. https://doi.org/10.1038/ajh.2009.43
Sateia MJ (2014) International classification of sleep disorders-third edition. Chest 146:1387–1394. https://doi.org/10.1378/chest.14-0970
Peppard PE, Young T, Palta M, Dempsey J, Skatrud J (2000) Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA 284:3015–3021. https://doi.org/10.1001/jama.284.23.3015
Wetter DW, Young TB, Bidwell TR, Badr MS, Palta M (1994) Smoking as a risk factor for sleep-disordered breathing. Arch Intern Med 154:2219–2224. https://doi.org/10.1001/archinte.1994.00420190121014
Young T, Finn L, Austin D, Peterson A (2003) Menopausal status and sleep-disordered breathing in the Wisconsin Sleep Cohort Study. Am J Respir Crit Care Med 167:1181–1185. https://doi.org/10.1164/rccm.200209-1055OC
Chen H, Aarab G, de Ruiter MHT, de Lange J, Lobbezoo F, van der Stelt PF (2016) Three-dimensional imaging of the upper airway anatomy in obstructive sleep apnea: a systematic review. Sleep Med 21:19–27. https://doi.org/10.1016/j.sleep.2016.01.022
Thapa A, Jayan B, Nehra K, Agarwal SS, Patrikar S, Bhattacharya D (2015) Pharyngeal airway analysis in obese and non-obese patients with obstructive sleep apnea syndrome. Med J Armed Forces India 71:S369–S375. https://doi.org/10.1016/j.mjafi.2014.07.001
Schwab RJ, Gupta KB, Gefter WB, Metzger LJ, Hoffman EA, Pack AI (1995) Upper airway and soft tissue anatomy in normal subjects and patients with sleep-disordered breathing. Significance of the lateral pharyngeal walls. Am J Respir Crit Care Med 152:1673–1689. https://doi.org/10.1164/ajrccm.152.5.7582313
Dempsey JA, Skatrud JB, Jacques AJ, Ewanowski SJ, Woodson BT, Hanson PR, Goodman B (2002) Anatomic determinants of sleep-disordered breathing across the spectrum of clinical and nonclinical male subjects. Chest 122:840–851. https://doi.org/10.1378/chest.122.3.840
Koo SK, Choi JW, Myung NS, Lee HJ, Kim YJ, Kim YJ (2013) Analysis of obstruction site in obstructive sleep apnea syndrome patients by drug induced sleep endoscopy. Am J Otolaryngol 34:626–630. https://doi.org/10.1016/j.amjoto.2013.07.013
Carberry JC, Amatoury J, Eckert DJ (2017) Personalized management approach for obstructive sleep apnea. Chest 153:744–755. https://doi.org/10.1016/j.chest.2017.06.011
Schwartz AR, Schubert N, Rothman W, Godley F, Marsh B, Eisele D, Nadeau J, Permutt L, Gleadhill I, Smith PL (1992) Effect of uvulopalatopharyngoplasty on upper airway collapsibility in obstructive sleep apnea. Am Rev Respir Dis 145:527–532. https://doi.org/10.1164/ajrccm/145.3.527
MacKay SG, Chan L (2016) Surgical approaches to obstructive sleep apnea. Sleep Med Clin 11:331–341. https://doi.org/10.1016/j.jsmc.2016.04.003
Aurora RN, Casey KR, Kristo D, Auerbach S, Bista SR, Chowdhuri S, Karippot A, Lamm C, Ramar K, Zak R, Morgenthaler TI, American Academy of Sleep Medicine (2010) Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep 33:1408–1413
Hatamleh M, Turner C, Bhamrah G, Mack G, Osher J (2016) Improved virtual planning for bimaxillary orthognathic surgery. J Craniofac Surg 27:e568–e573. https://doi.org/10.1097/SCS.0000000000002877
Cevidanes LHC, Tucker S, Styner M, Kim H, Chapuis J, Reyes M, Proffit W, Turvey T, Jaskolka M (2010) Three-dimensional surgical simulation. Am J Orthod Dentofac Orthop 138:361–371. https://doi.org/10.1016/j.ajodo.2009.08.026
Guijarro-Martinez R, Swennen GRJ (2011) Cone-beam computerized tomography imaging and analysis of the upper airway: a systematic review of the literature. Int J Oral Maxillofac Surg 40:1227–1237. https://doi.org/10.1016/j.ijom.2011.06.017
Hofmann E, Schmid M, Lell M, Hirschfelder U (2014) Cone beam computed tomography and low-dose multislice computed tomography in orthodontics and dentistry. J Orofac Orthop/Fortschritte der Kieferorthopädie 75:384–398. https://doi.org/10.1007/s00056-014-0232-x
Van Holsbeke CS, Verhulst SL, Vos WG et al (2014) Change in upper airway geometry between upright and supine position during tidal nasal breathing. J Aerosol Med Pulm Drug Deliv 27:51–57. https://doi.org/10.1089/jamp.2012.1010
Sutthiprapaporn P, Tanimoto K, Ohtsuka M, Nagasaki T, Iida Y, Katsumata A (2008) Positional changes of oropharyngeal structures due to gravity in the upright and supine positions. Dentomaxillofacial Radiol 37:130–135. https://doi.org/10.1259/dmfr/31005700
Barrera JE, Pau CY, Forest V-I, Holbrook AB, Popelka GR (2017) Anatomic measures of upper airway structures in obstructive sleep apnea. World J Otorhinolaryngol - head neck Surg 3:85–91. https://doi.org/10.1016/j.wjorl.2017.05.002
Qu X, Li G, Zhang Z, Ma X (2011) Comparative dosimetry of dental cone-beam computed tomography and multi-slice computed tomography for oral and maxillofacial radiology. Zhonghua Kou Qiang Yi Xue Za Zhi 46:595–599. https://doi.org/10.3760/cma.j.issn.1002-0098.2011.10.006
Camacho M, Capasso R, Schendel S (2014) Airway changes in obstructive sleep apnoea patients associated with a supine versus an upright position examined using cone beam computed tomography. J Laryngol Otol 128:824–830. https://doi.org/10.1017/S0022215114001686
Verin E, Tardif C, Buffet X, Marie JP, Lacoume Y, Andrieu-Guitrancourt J, Pasquis P (2002) Comparison between anatomy and resistance of upper airway in normal subjects, snorers and OSAS patients. Respir Physiol 129:335–343. https://doi.org/10.1016/S0034-5687(01)00324-3
Lye KW (2008) Effect of orthognathic surgery on the posterior airway space (PAS). Ann Acad Med Singap 37:677–682. https://doi.org/10.1007/s12663-014-0687-8
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The study was reviewed and approved by the local ethics committee of University Hospital Aachen (EK266/17).
Informed consent
For this type of study, formal consent was not required. All data were collected anonymously.
Rights and permissions
About this article

Cite this article
Ayoub, N., Eble, P., Kniha, K. et al. Three-dimensional evaluation of the posterior airway space: differences in computed tomography and cone beam computed tomography. Clin Oral Invest 23, 603–609 (2019). https://doi.org/10.1007/s00784-018-2478-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2478-y