
Abstract
Vertebral fracture (VF) is a common osteoporotic fracture, while its epidemiology varies according to regions and ethnicities, little is known about it in Japan. Using whole-spine radiographs from a population-based cohort study, the Research on Osteoarthritis/Osteoporosis Against Disability study 3rd survey performed in 2012–2013, we estimated the sex- and age-specific prevalence of VF in the Japanese. Genant’s semiquantitative method (SQ) was used to define VF; SQ ≥ 1 as VF, SQ = 1 as mild VF, SQ≥ 2 as severe VF. We also revealed accurate site-specific prevalence, and associated factors with mild and severe VF. The participants were 506 men [mean age 66.3 years, standard deviation (SD):13.0] and 1038 women (mean age 65.3 years, SD: 12.6). The prevalence of VF in participants aged under 40, in their 40s, 50s, 60s, 70s, and ≥ 80 years was 17.4, 7.9, 18.5, 25.6, 26.3, and 41.5%, respectively, in men, and 2.9%, 2.4%, 7,3, 10.3, 27.1, and 53.0%, respectively, in women. Men had a significantly higher prevalence of mild VF (21.2%) than women (10.0%, p < 0.001); whereas, severe VF was significantly more prevalent in women (9.1%) than in men (4.7%, p = 0.003). VF was distributed with 2 peaks regarding site; one large peak at the thoracolumbar region, and another at the middle thoracic lesion. Low back pain and decreased walking ability were independently associated with severe VF, but not with mild VF, after adjustment for participant characteristics. Decreased walking ability was associated with multiple VFs in women, but not in men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vertebral fracture (VF) is the most common among osteoporotic fractures [1]. VF not only affects activities of daily living (ADL) and health-related quality of life (HRQoL) [2,3,4,5], but also is related to high morality [6, 7]. Johnell et al. reported higher 5-year mortality after clinical VF than other osteoporotic fractures or general population [6]. Therefore, preventing VF to improve life expectancy and to maintain HRQoL of the elderly is imperative.
The first step to prevent VF is to know its precise epidemiology. However, Cooper et al. reported that only about a third of all vertebral deformities noted on radiographs come to medical attention [8]. Hence, researches at medical institutions alone do not provide sufficient information; conducting a survey on the general population with radiographs to know its epidemiology is mandatory. Due to this complexity, studies on the epidemiology of VF are still very limited worldwide. The reported prevalence of VF varies from 12 to 37% [9,10,11,12,13,14,15,16] depending on the studied regions and the criteria used to define VF. Recent reports on the epidemiology of VF in Japan launched their baseline studies in mid–late 1990s [13, 15, 16], that is, the reported prevalence of VF was that of 2 decades ago. In addition, most reports were based on radiographs of the thoracic spine and of the lumbar spine taken and assessed separately; thus, the accurate site of fracture, especially at the thoracolumbar region, was difficult to be estimated. [17, 18].
This study aimed to determine the prevalence and site of morphometric VF by sex and age in Japan, using whole-spine radiographs, and to analyze associated factors of the presence of VF. The data of the Research on Osteoarthritis/Osteoporosis Against Disability (ROAD) study 3rd survey performed in 2012–2013 were used in this study.
Materials and methods
Participants
The ROAD study is a large-scale population-based cohort study that started in 2005 in three communities in Japan: an urban region in Itabashi, Tokyo; a mountainous region in Hidakagawa, Wakayama; and a coastal region in Taiji, Wakayama. Details of the study have been described previously [19, 20]. In the present study, we used the 3rd survey of the ROAD study from the mountainous region and the coastal region; hence, we describe the cohort in the 2 regions. This is a cross-sectional observational study.
After the baseline and 2nd surveys, a third survey was performed in the same communities from 2012 to 2013. Invitation letters were distributed to the inhabitants whose names were listed in the ROAD study baseline and 2nd survey database. In addition to the former participants, inhabitants aged ≥ 40 years from Hidakagawa and Taiji, who were willing to participate in the 2012–2013 ROAD survey, were included in the third survey. The inclusion criteria were as follows: ability to (1) walk to the clinic where the survey was performed, (2) provide self-reported data, and (3) understand and sign an informed consent form. No other exclusion criteria were used. Thus, 1629 residents (mountainous area, Hidakagawa, Wakayama, 722 individuals; and coastal area, Taiji, Wakayama, 907 individuals) participated in the third survey. Of them, whole-spine X-ray examinations were performed on a total of 1544 participants (506 men and 1038 women, mean age 65.6 years). We did not perform the examination in participants who could not stand alone or who did not give their consent for the examination. We used the data obtained from 1544 participants in the present study.
The study was approved by the ethics committees of the University of Tokyo (nos. 1264 and 1326) and the Tokyo Metropolitan Institute of Gerontology (no. 5). Written informed consent was provided by all participants.
Questionnaire, interview, and anthropometric measurements
Participants completed a 400-item interviewer-administered questionnaire that included lifestyle information such as occupational career, smoking habits, alcohol consumption, family history, medical history, physical activity, reproductive variables, and health-related quality of life. Anthropometric measurements included height, weight, arm length, and body mass index (BMI; weight [kg]/height2 [m2]). Medical information was taken by well-experienced orthopedists on systemic, local, and mental status including information of low back pain. Low back pain was defined as pain on low back on most days during the past month.
The 6-m walking time
The time of participants’ walking a 6-m course at their usual speed was measured. The method of measurement of walking time was identical to that performed in the large-scale cohort study entitled “The Osteoporotic Fractures in Men (MrOS)”, which started prior to the ROAD study [21]. In the present study, a cutoff value of 0.8 m/s was used [22, 23] to indicate decreased walking ability. In addition, participants who needed any support or assistance such as a cane, a walker, or a wheel chair in their usual walking were also defined as having decreased walking ability.
Radiographic assessment
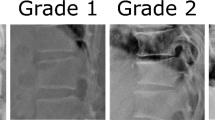
Stand-up lateral radiographs of the whole spine were taken for each subject by licensed radiography technicians using standard radiographic techniques. The radiographs were read by one spine surgeon (C.H.). VF and its severity were determined on all vertebrae from T4 to the most caudal vertebra of each participant, using the Genant semiquantitative (SQ) method [24] as indicated by the 2015 Official Position of International Society of Clinical Densitometry [25]. SQ is graded from 0 to 3, where 0 is normal; 1, mildly deformed; 2, moderately deformed; and 3, severely deformed. Morphometric VF was defined as SQ ≥ 1, mild VF as SQ = 1, and severe VF as SQ ≥ 2, respectively. Each participant was defined as having VF when at least 1 vertebra was determined as SQ ≥ 1; as mild VF when the maximum grade of SQ = 1; and as severe VF when the maximum grade of SQ ≥ 2.
Each vertebra was numbered on the principle of the most caudal vertebra being L5 and the cranial vertebra to L1 being T12. The most caudal vertebra was exceptionally numbered as L6 when all the vertebrae from C2 to C7 and from T1 to T12 were visible, and 6 vertebrae completely apart from the sacrum were recognized caudal to T12. Another exception included a case when all the vertebrae from C2 to C7 and from T1 to T12 were visible, and only 4 vertebrae were recognized caudal to T12. In that case, the most caudal vertebra was numbered as L4. Eleven participants were determined to have L6 as the most caudal vertebra, but L6 vertebrae were excluded from the analysis because all of them were scored as grade 0.
To investigate the intra- and inter-observer reliability of SQ grading, 50 randomly selected radiographs were scored by the same reader (C.H.) again with an interval of > 2 weeks and another orthopedist (T.I.) who was blinded to the scores graded by C.H. The percentage of agreement and kappa statistic were 98.1 and 0.70%, and 98.0 and 0.62% for the intra-observer reliability and inter-observer reliability, respectively.
Bone mineral density measurement
Bone mineral density (BMD) was measured at the lumbar spine (L2–L4) and the proximal femur using dual-energy X-ray absorptiometry (DXA) (Hologic Discovery; Hologic, Waltham, MA, USA). To control quality, the same DXA equipment was used, and the same spine phantom was scanned daily to monitor the machine’s performance in study populations at different regions. The BMD of the phantom was adjusted to 1.032 ± 0.016 g/cm2 (± 1.5%) during all examinations. In addition, the same physician (N.Y.) examined all participants to prevent observer variability.
Statistical analysis
All statistical analyses were performed using STATA statistical software, version 15.1 (STATA, College Station, TX, USA). Differences in proportion were compared using Chi-square test unless frequency of at least one cell was 5 or less; Fisher’s exact test was used instead. Differences in continuous variables were examined using non-paired Student’s t test. A p value < 0.05 was regarded to suggest a significant difference.
To test the association between the presence of mild and severe VF with potential associated factors, multinomial logistic regression analysis was used. In the analysis, the presence of mild VF and severe VF was used as the objective variable (0, group without VF; 1, group with mild VF; 2, group with severe VF), and explanatory variables were selected in addition to the basic characteristics, such as sex, age, residing area, BMI, smoking, alcohol consumption, and BMD at L2–L4. Other explanatory variables included the presence of low back pain and decreased walking ability. After the multinomial logistic regression analysis, the relative risk ratios (RRRs) were evaluated. In addition, to determine associations of multiple VFs with low back pain and decreased walking ability in both sexes, multiple logistic regression analysis was used after adjustment for sex, age, residing area, BMI, smoking, alcohol consumption, and BMD at L2–L4 in the overall population and after adjustment for age, residing area, BMI, smoking, alcohol consumption, and BMD at L2–L4 in men and women.
Results
Characteristics of the participants
Table 1 shows the characteristics of the 1544 participants in the present study. The mean age was not significantly different between both sexes (p = 0.17). The mean BMD of men was significantly higher than women at both L2–L4 and the femoral neck (p < 0.001, both).
Sex- and age- specific prevalence
Table 2 shows the prevalence of VF, mild VF (the maximum grade of SQ = 1), and severe VF (the maximum grade of SQ ≥ 2) in men and women, classified according to age. Number of patients with maximum of each grade is shown in Table 3. Men had significantly higher prevalence of VF than women in their 50s and 60s (p = 0.006 and p < 0.001, respectively), but the difference was not significant in other age strata. As a whole, men had significantly higher prevalence of VF (25.9%) than women (19.1%) (p = 0.002). VF increased in an age-dependent way in women, and > 50% of women aged 80 years or older had at least one VF. Severe VF increased in an age-dependent way in both men and women, and the prevalence of severe VF was significantly higher in women than in men in their 70s, at age 80 years or older, and as a whole. By contrast, the prevalence of mild VF was significantly higher in men than in women in their 50s, 60s, and as a whole.
Site-specific prevalence
Figure 1 shows the site-specific prevalence of mild and severe VF in men and women. T12 had the highest prevalence of VF both in men (11.6%) and in women (6.4%). In both sexes, 2 peaks of the prevalence of VF were observed: one at the thoracolumbar lesion (T11–L1) and the other small peak at the middle thoracic lesion (T7–T8). Severe VF had similar peaks in women; whereas in men, it was almost evenly distributed at the lesion T8 or caudal with a small peak at T12.

Prevalence (%) of mild vertebral fracture (VF) and severe VF in both sexes classified according to site
Associated factors for mild and severe VF
We next examined the associated factors for mild and severe VF. Table 4 shows the characteristics of each group; normal, mild VF, and severe VF. Table 5 shows the RRRs obtained from the multinomial logistic regression analysis using the presence of mild VF and severe VF as objective variables. All the variables in the left column in Table 5 were included as explanatory variables. As different tendency in prevalence of mild and severe VF between sexes was observed, this analysis was performed initially as a whole with sex as one of the explanatory variables, and then separately in men and women. After adjustment for basic characteristics, significant association was found between the presence of low back pain and decreased walking ability and severe VF, but none between the presence of low back pain and decreased walking ability and mild VF. Especially, a strong relationship was observed between severe VF and decreased walking ability in women (RRR = 3.03, 95% confidence interval: 1.72–5.23).
The prevalence of multiple VFs and their associated factors
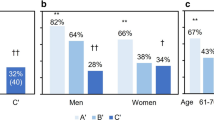
Figure 2 shows the prevalence of single VF, multiple VFs, and multiple severe VFs in men and women, classified according to age. Men in their 50s and 60s had significantly higher prevalence of multiple VFs (3.7% and 8.3%, respectively) than women (0.0% and 3.0%, respectively) (p = 0.03, 0.02, respectively). In men and women in their 70s and 80s or older, no significant difference was observed between sexes. The overall prevalence of multiple VFs was 10.7% and 8.0% in men and women, respectively, without significant difference (p = 0.08). In contrast, the prevalence of multiple severe VFs was significantly higher in women (3.0%) than in men (1.2%) (p = 0.03). In women aged 80 years or older, 20/132 participants (15.2%) had multiple severe VFs. We next examined the association of multiple VFs with low back pain and decreased walking ability by multiple logistic regression analysis as shown in Table 6. As different clinical significance of multiple morphometric VFs between sexes has been reported [26], the analysis was performed by sex. After adjustment for age, residing area, BMI, smoking, alcohol consumption, and BMD at L2–L4, no association was found between low back pain and multiple VFs in men or women; decreased walking ability was significantly associated with multiple VFs in the whole population and in women.

Prevalence (%) of single, multiple, and multiple severe vertebral fractures (VFs) classified according to age and sex. Single VF: participants with 1 VF only. Multiple VFs: participants with 2 or more VFs. Multiple severe VFs: participants with 2 or more severe VFs
Discussion
In the present study, we determined the latest prevalence and the accurate site of morphometric VF classified by severity in general population in Japan using whole-spine radiographs. The following were the major findings of this study: the prevalence of mild VF was significantly higher in men than in women, whereas the prevalence of severe VF was significantly higher in women than in men, and VF had the 2-peak distribution in both men and women. We also revealed that low back pain and decreased walking ability were significantly associated with severe VF, but not with mild VF. Multiple VFs were associated with decreased walking ability in women.
As mentioned above, surveys at medical institutions alone do not provide sufficient information about the epidemiology of VF; conducting a survey on general population with radiographs is mandatory. Due to this complexity, studies on the epidemiology of VF have been very limited in Japan. Based on population-based surveys involving both men and women, only 3 studies reporting the prevalence of VF in Japan have been conducted [12, 15, 16], except the present study. The reported prevalence of VF varies from 3.3% [15] to 20.5% [16]. A wide range of prevalence is reported even in a Japanese study. One of the supposed reasons for the variance is the difference in the definition and diagnostic methods of VF, resulting from lack of gold standards to diagnose VF. Age of the participants can also be a reason for differences.
Fujiwara et al. [15] also used the Genant SQ method to determine VF, but their criteria of VF were set at SQ ≥ 2, which corresponds to severe VF in the present study. Their reported prevalence of VF in men and women (3.3% and 10.3%, respectively) is comparable to the prevalence of severe VF in the present study (4.7% and 9.1%, respectively).
Two population-based studies worldwide have been conducted on the prevalence of VF, which was composed of both men and women, containing age stratification information and using Genant’s SQ method to define VF. One was surveyed on Brazilian residents between 2005 and 2007 [27] and the other on Hong Kong residents between 2001 and 2003 [28]. To compare the results, the prevalence of VF and severe VF of the present study in men and women aged 65–69 years was calculated as follows: men VF, 24.6%; severe VF, 3.3%; women VF, 13.8%; and severe VF, 5.6%. Table 7 shows the comparison among the present study and the previous 2 studies. Compared to the results from the Hong Kong study, the prevalence of both VF and severe VF in the present study was generally higher, except severe VF in women aged 65–69 years and 70–70 years. Compared to the Brazilian study, the prevalence of VF was lower in younger generation (aged 65–69 years) and higher in older generation (aged 80 years or more). Because all 3 studies were population-based, were voluntary participated, and used the same diagnostic criteria, these differences are considered to reflect ethnic and regional differences.
To the best our knowledge, this is the first study to report on the prevalence of VF using whole-spine radiographs, which enabled us to number each vertebra accurately. As Lian et al. reported, the whole-spine view was mandatory for accurate vertebral numbering. [17] We revealed site-specific prevalence of VF and 2-peak prevalence of VF with one main peak at the thoracolumbar lesion and the other small peak at the middle thoracic lesion. The same tendency was reported using thoracic and lumbar radiographs [12, 24, 29]. This tendency was confirmed with greater accuracy using whole-spine radiographs.
To confirm whether the participants of the present study are representative of the Japanese population, we compared anthropometric measurements and frequency of smoking and alcohol consumption between the participants and the general Japanese population. The details of the comparison are in Supplementary Tables 1 and 2. Briefly, the overall BMI of the participants was basically comparable to that of the broader Japanese population; whereas, the participants had healthier lifestyles than the general Japanese population in terms of smoking and alcohol consumption. Given that the results obtained from the present study were applicable to the total age–sex distribution derived from the Japanese census in 2015 [30], it would be assumed that 14,600,000 Japanese people (19.4%) [74,00,000 men (21.2%) and 71,00,000 women (18.0%)] aged 40 years and older would be affected by morphometric VF and that 4700,000 Japanese people (6.3%) [1,200,000 men (3.5%) and 3,500,000 women (8.8%)] aged 40 years and older would be affected by morphometric severe VF.
Our study showed that severe VF was significantly associated with low back pain after adjustment for basic characters (Table 5). The results are consistent with previous literature [11, 28]. Although the tendency was the same in both men and women when analyzed separately, the association between low back pain and severe VF was not significant in men or women in a sex-separate analysis; whereas, the association was significant in the whole-cohort model. The supposed reason for the discrepancy is the low number of participants with severe VF (men; 24, women; 94, shown in Table 3, as this model had 8 explanatory variables. Hence, the whole-cohort model is considered more plausible than the separate model. The association between VF and decreased walking ability has not been clearly demonstrated to date. Our results revealed that severe VF was significantly associated with decreased walking ability after adjustment for basic characters. As severe VF can be a cause of sagittal imbalance and sagittal imbalance has been reported to correlate with walking disability [31], it may be considered that severe VF associates with decreased walking ability through sagittal imbalance. However, Lafage et al. reported that the strongest correlation was observed between walking disability and pelvic tilt [31], which was a pelvic parameter not manifesting spinal deformity. Therefore, our results revealed a new aspect of the association between VF and walking disability.
In this study, multiple VFs were significantly associated with decreased walking ability in women, but not in men. Some studies have reported increased mortality with multiple VFs in women. [26, 32] Further, Mutikanen et al. reported that walking disability was associated with increased mortality in older community-dwelling women. [33]. The result of the current study corresponds with these reports. As walking disability is one of the major risk factors for falls in elderly people [34] and falls are the biggest cause of VF, multiple VFs are considered to have the tendency to lead to the next VF. Several reports have supported that prevalent VF is a risk factor for incident VF [35,36,37]. Furthermore, vitamin D deficiency is considered to accelerate the reproducing cycle of VF through being a cause of osteoporosis [38, 39] and being a risk factor for falls [40].
Mild VF was not associated with low BMD, low back pain, or decreased walking ability, which indicates that mild VF lack characteristics specific to clinical VF [41]. Szulc et al. [42] and Kherad et al. [29] also reported low clinical relevance of mild VF in elderly men; however, both studies were conducted on only men. In the present study, we confirmed the same tendency both on men and women. Low clinical relevance of mild VF may partly be because of confusion between true VF and deformity, which is a nonosteoporotic condition, as Szulc et al. discussed. [42] This would be a limitation of morphometrical diagnosis of VF in a cross-sectional study. The clinical importance of mild VF is still obscure from the present study. However, Roux et al. reported that prevalent morphometric VF, even mild, was a significant risk factor for incidence of new VF in elderly women [43]. Pongchaiyakul et al. reported a higher rate of incident symptomatic fracture and higher mortality after a symptomatic fracture among those with prevalent morphometric VF [44]. Therefore, to clarify the significance of mild VF, following the same participants and analyzing following subsequent clinical and radiological outcomes are necessary. We will continue to follow the participants in the ROAD study 3rd visit and will clarify the subsequent outcomes of VF in the near future.
This study has several limitations. First, the present cohort may not be truly representative of the general population. Especially, participants aged ≥ 80 years of the present study were significantly smaller in BMI than the general Japanese population. This difference should be taken into consideration when estimating the prevalence of VF in people aged ≥ 80 years, since a small body build is associated with osteoporosis. Therefore, our results might represent an overestimation. Second, mild VF in the present study may include vertebral deformity, which is unrelated to osteoporosis, as discussed above. This is a limitation attributed to morphometrical diagnosis. Thus, prevalence of overall VF may be an overestimation; whereas, prevalence of severe VF would be reasonable. Third, the present study does not reveal a cause-and-effect link as it is a cross-sectional study. In addition, there is a possibility that measuring the change in vertebral height enables us to diagnose VF more accurately in a longitudinal study. However, we have one of the largest cohorts among recent Japanese studies of VF, and we can and will analyze the longitudinal results as the ROAD study is still ongoing.
Despite these limitations, we estimated age- and sex-specific prevalence of mild and severe VF with accurate site-specific distribution determined according to whole-spine radiographs in Japanese men and women. Our results suggested that the characteristics of mild and severe VF were different, such as mild VF had male dominancy, whereas severe VF had female dominancy; not mild VF but severe VF was significantly associated with low back pain and decreased walking ability. Further, we revealed that multiple VFs were associated with decreased walking ability in women.
References
Riggs BL, Melton Lii LJ (1995) The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 17:505S–511S
Suzuki N, Ogikubo O, Hansson T (2009) The prognosis for pain, disability, activities of daily living and quality of life after an acute osteoporotic vertebral body fracture: its relation to fracture level, type of fracture and grade of fracture deformation. Eur Spine J 18:77–88. https://doi.org/10.1007/s00586-008-0847-y
Oleksik A, Lips P, Dawson A, Minshall ME, Shen W, Cooper C, Kanis J (2000) Health-related quality of life in postmenopausal women with low BMD with or without prevalent vertebral fractures. J Bone Miner Res 15:1384–1392. https://doi.org/10.1359/jbmr.2000.15.7.1384 (in Eng)
Cockerill W, Lunt M, Silman AJ, Cooper C, Lips P et al (2004) Health-related quality of life and radiographic vertebral fracture. Osteoporos Int 15:113–119. https://doi.org/10.1007/s00198-003-1547-4
Pluijm SMTA, Smit JH, Deeg DJ, Lips P (2000) Consequences of vertebral deformities in older men and women. J Bone Miner Res 15:1564–1572. https://doi.org/10.1359/jbmr.2000.15.8.1564
Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jonsson B (2004) Mortality after osteoporotic fractures. Osteoporos Int 15:38–42. https://doi.org/10.1007/s00198-003-1490-4
Edidin AA, Ong KL, Lau E, Kurtz SM (2015) Morbidity and mortality after vertebral fractures: comparison of vertebral augmentation and nonoperative management in the medicare population. Spine 40:1228–1241. https://doi.org/10.1097/brs.0000000000000992 (Phila Pa 1976)
Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ 3rd (1992) Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 7:221–227. https://doi.org/10.1002/jbmr.5650070214 (in Eng)
Eastell R, Cedel SL, Wahner HW, Riggs BL, Melton LJ 3rd (1991) Classification of vertebral fractures (in eng). J Bone Miner Res 6:207–215. https://doi.org/10.1002/jbmr.5650060302
Black DM, Palermo L, Nevitt MC, Genant HK, Epstein R, San Valentin R, Cummings SR (1995) Comparison of methods for defining prevalent vertebral deformities: the Study of Osteoporotic Fractures. J Bone Miner Res 10:890–902. https://doi.org/10.1002/jbmr.5650100610 (in eng)
O’Neill TWFD, Varlow J, Cooper C, Kanis JA, Silman AJ (1996) The prevalence of vertebral deformity in european men and women: the European Vertebral Osteoporosis Study. J Bone Miner Res 11:1010–1018. https://doi.org/10.1002/jbmr.5650110719
Yoshimura N, Kinoshita H, Danjoh S, Yamada H, Tamaki T, Morioka S, Kasamatsu T, Hashimoto T, Inoue T (1995) Prevalence of vertebral fractures in a rural japanese population. J Epidemiol 5:171–175. https://doi.org/10.2188/jea.5.171
Kadowaki E, Tamaki J, Iki M, Sato Y, Chiba Y, Kajita E, Kagamimori S, Kagawa Y, Yoneshima H (2010) Prevalent vertebral deformity independently increases incident vertebral fracture risk in middle-aged and elderly Japanese women: the Japanese Population-based Osteoporosis (JPOS) Cohort Study. Osteoporos Int 21:1513–1522. https://doi.org/10.1007/s00198-009-1113-9
Kwok AW, Leung JC, Chan AY, Au BS, Lau EM, Yurianto H, Yuktanandana P, Yoshimura N, Muraki S, Oka H, Akune T, Leung PC (2012) Prevalence of vertebral fracture in Asian men and women: comparison between Hong Kong, Thailand, Indonesia and Japan. Public Health 126:523–531. https://doi.org/10.1016/j.puhe.2012.03.002
Fujiwara S, Hamaya E, Goto W, Masunari N, Furukawa K, Fukunaga M, Nakamura T, Miyauchi A, Chen P (2011) Vertebral fracture status and the World Health Organization risk factors for predicting osteoporotic fracture risk in Japan. Bone 49:520–525. https://doi.org/10.1016/j.bone.2011.05.021
Nishimura A, Akeda K, Kato K, Asanuma K, Yamada T, Uchida A, Sudo A (2014) Osteoporosis, vertebral fractures and mortality in a Japanese rural community. Mod Rheumatol 24:840–843. https://doi.org/10.3109/14397595.2013.866921
Lian J, Levine N, Cho W (2018) A review of lumbosacral transitional vertebrae and associated vertebral numeration. Eur Spine J 27:995–1004. https://doi.org/10.1007/s00586-018-5554-8
O’Brien MF, Blanke KM, Lenke LG, Spinal Deformity Study Group (SDSG) (2008) Radiographic Measurement Manual. Medtronic Sofamor Danek USA Inc., Memphis
Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, Saika A, Yoshida H, Suzuki T, Yamamoto S, Ishibashi H, Kawaguchi H, Nakamura K, Akune T (2009) Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab 27:620–628. https://doi.org/10.1007/s00774-009-0080-8
Yoshimura N, Muraki S, Oka H, Kawaguchi H, Nakamura K, Akune T (2010) Cohort profile: research on Osteoarthritis/Osteoporosis Against Disability study. Int J Epidemiol 39:988–995. https://doi.org/10.1093/ije/dyp276
Orwoll E, Blank JB, Barrett-Connor E, Cauley J, Cummings S, Ensrud K, Lewis C, Cawthon PM, Marcus R, Marshall LM, McGowan J, Phipps K, Sherman S, Stefanick ML, Stone K (2005) Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study—a large observational study of the determinants of fracture in older men. Contemp Clin Trials 26:569–585. https://doi.org/10.1016/j.cct.2005.05.006
Yoshimura N, Muraki S, Oka H, Tanaka S, Ogata T, Kawaguchi H, Akune T, Nakamura K (2015) Association between new indices in the locomotive syndrome risk test and decline in mobility: third survey of the ROAD study. J Orthop Sci 20:896–905. https://doi.org/10.1007/s00776-015-0741-5
Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW et al (2014) Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 15:95–101. https://doi.org/10.1016/j.jamda.2013.11.025
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148. https://doi.org/10.1002/jbmr.5650080915 (in Eng)
Densitometry TISFC (2015) 2015 ISCD Official Positions—Adult
Trone DW, Kritz-Silverstein D, von Muhlen DG, Wingard DL, Barrett-Connor E (2007) Is radiographic vertebral fracture a risk factor for mortality? Am J Epidemiol 166:1191–1197. https://doi.org/10.1093/aje/kwm206
Lopes JB, Danilevicius CF, Takayama L, Caparbo VF, Menezes PR, Scazufca M, Kuroishi ME, Pereira RM (2011) Prevalence and risk factors of radiographic vertebral fracture in Brazilian community-dwelling elderly. Osteoporos Int 22:711–719. https://doi.org/10.1007/s00198-010-1258-6
Kwok AW, Gong JS, Wang YX, Leung JC, Kwok T, Griffith JF, Leung PC (2013) Prevalence and risk factors of radiographic vertebral fractures in elderly Chinese men and women: results of Mr. OS (Hong Kong) and Ms. OS (Hong Kong) studies. Osteoporos Int 24:877–885. https://doi.org/10.1007/s00198-012-2040-8
Kherad M, Rosengren BE, Hasserius R, Nilsson JA, Redlund-Johnell I, Ohlsson C, Lorentzon M, Mellstrom D, Karlsson MK (2015) Low clinical relevance of a prevalent vertebral fracture in elderly men—the MrOs Sweden study. Spine J 15:281–289. https://doi.org/10.1016/j.spinee.2014.09.016
Japanese Official Statistics MoIAaC (2015) Population Census 2015
Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP (2009) Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine 34:E599–E606. https://doi.org/10.1097/brs.0b013e3181aad219 (in Eng, Phila Pa 1976)
Kado DMBW, Palermo L, Nevitt MC, Genant HK, Cummings SR (1999) Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 159:1215–1220
Mutikainen S, Rantanen T, Alen M, Kauppinen M, Karjalainen J, Kaprio J, Kujala UM (2011) Walking ability and all-cause mortality in older women. Int J Sports Med 32:216–222. https://doi.org/10.1055/s-0030-1268506
American Geriatrics Society, British Geriatrics Society, American Academy of Orthopaedic Surgeons Panel on Falls Prevention (2001) Guideline for the prevention of falls in older persons. J Am Geriatr Soc 49:664–672 (in Eng)
Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB, Licata A, Benhamou L, Geusens P, Flowers K, Stracke H, Seeman E (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285:320–323 (in Eng)
Cauley JA, Hochberg MC, Lui LY, Palermo L, Ensrud KE, Hillier TA, Nevitt MC, Cummings SR (2007) Long-term risk of incident vertebral fractures. JAMA 298:2761–2767. https://doi.org/10.1001/jama.298.23.2761 (in Eng)
Siris ES, Genant HK, Laster AJ, Chen P, Misurski DA, Krege JH (2007) Enhanced prediction of fracture risk combining vertebral fracture status and BMD. Osteoporos Int 18:761–770. https://doi.org/10.1007/s00198-006-0306-8
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501. https://doi.org/10.1210/edrv.22.4.0437 (in Eng)
Bischoff-Ferrari HA, Zhang Y, Kiel DP, Felson DT (2005) Positive association between serum 25-hydroxyvitamin D level and bone density in osteoarthritis. Arthritis Rheum 53:821–826. https://doi.org/10.1002/art.21601
Rothenbacher D, Klenk J, Denkinger MD, Herbolsheimer F, Nikolaus T, Peter R, Boehm BO, Rapp K, Dallmeier D, Koenig W, Acti FESG (2014) Prospective evaluation of renal function, serum vitamin D level, and risk of fall and fracture in community-dwelling elderly subjects. Osteoporos Int 25:923–932. https://doi.org/10.1007/s00198-013-2565-5
Giangregorio LM, Macintyre NJ, Thabane L, Skidmore CJ, Papaioannou A (2013) Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst Rev: CD008618 https://doi.org/10.1002/14651858.cd008618.pub2
Szulc P, Munoz F, Marchand F, Delmas PD (2001) Semiquantitative evaluation of prevalent vertebral deformities in men and their relationship with osteoporosis: the MINOS study. Osteoporos Int 12:302–310. https://doi.org/10.1007/s001980170120 (in Eng)
Roux C, Fechtenbaum J, Kolta S, Briot K, Girard M (2007) Mild prevalent and incident vertebral fractures are risk factors for new fractures. Osteoporos Int 18:1617–1624. https://doi.org/10.1007/s00198-007-0413-1
Pongchaiyakul C, Nguyen ND, Jones G, Center JR, Eisman JA, Nguyen TV (2005) Asymptomatic vertebral deformity as a major risk factor for subsequent fractures and mortality: a long-term prospective study. J Bone Miner Res 20:1349–1355. https://doi.org/10.1359/JBMR.050317
Ministry of Health, Labour and Welfare. The report of National Health and Nutrition Survey 2012. https://www.mhlw.go.jp/bunya/kenkou/eiyou/h24-houkoku.html. Accessed 12 Dec 2018
Acknowledgements
The authors wish to thank Dr. Naoki Hirabayashi of Kawakami Clinic, Hidakagawa Town; Mrs. Tomoko Takijiri, Mrs. Rie Takiguchi, Mrs. Kyoko Maeda, Ms. Ikuyo Ueyama, Mrs. Michiko Mori, Mrs. Hisayo Sugimoto, and other members of the public office in Hidakagawa Town; and Mrs. Tamako Tsutsumi, Mrs. Kanami Maeda, Mrs. Megumi Takino, Mrs. Shuko Okada, Mrs. Kazuyo Setoh, Mrs. Chise Ryouno, Mrs. Miki Shimosaki, Mrs. Chika Yamaguchi, Mrs. Yuki Shimoji, and other members of the public office in Taiji Town for their assistance in locating and scheduling participants for examinations. We would also like to thank Ms. Kyoko Yoshimura, Mrs. Toki Sakurai, Mrs. Saeko Sahara, and Mr. Noriyuki Oe for their assistance with data reduction and administration.
Funding
This work was supported by Grant-in-Aid funding from the Ministry of Health, Labour and Welfare: H17-Men-eki-009 (Director, Kozo Nakamura), H20-Choujyu-009 (Director, Noriko Yoshimura), H23-Choujyu-002 (Director, Toru Akune), H25-Choujyu-007 (Director, Noriko Yoshimura), and H25-Nanchitou (Men)-005 (Director, Sakae Tanaka). The study was also supported by Scientific Research grants B26293139, B23390172, B20390182, and Challenging Exploratory Research grants 15K15219, 24659317 to Noriko Yoshimura; Scientific Research grants B23390356, C20591774, and Challenging Exploratory Research grants 23659580 to Shigeyuki Muraki; Challenging Exploratory Research grants 24659666 and 21659349 and Young Scientists A18689031 to Hiroyuki Oka; Scientific Research grants B26293329, B23390357, C20591737 and Challenging Exploratory Research grants 25670293 to Toru Akune; and by Collaborating Research with NSF from the Ministry of Education, Culture, Sports, Science and Technology in Japan 08033011-00262 (Director, Noriko Yoshimura). The study was partly supported by grants from the Japan Agency for Medical Research and Development (17gk0210007h0003, Director, Sakae Tanaka). Further, the study was partly supported by grants from the Japan Osteoporosis Society (Noriko Yoshimura, Shigeyuki Muraki, Hiroyuki Oka, and Toru Akune), Japan Osteoporosis Foundation (2015, Noriko Yoshimura, and 2018, Chiaki Horii), research aids from the Japanese Orthopaedic Association (JOA-Subsidized Science Project Research 2006-1 and 2010-2, Director, Hiroshi Kawaguchi; and 2014-1, Director, Kozo Nakamura), the Japanese Society for Musculoskeletal Medicine (2015, Director, Shigeyuki Muraki; and 2017, Director, Noriko Yoshimura), Mitsui Sumitomo Insurance Welfare Foundation (2016, Director, Noriko Yoshimura), and Japan Dairy Association (2017, Director, Noriko Yoshimura).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Horii, C., Asai, Y., Iidaka, T. et al. Differences in prevalence and associated factors between mild and severe vertebral fractures in Japanese men and women: the third survey of the ROAD study. J Bone Miner Metab 37, 844–853 (2019). https://doi.org/10.1007/s00774-018-0981-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-018-0981-5