
Abstract
The antifracture efficacy of vitamin D in osteoporosis is due to its direct action on bones and indirect extraskeletal effects to prevent falls. Eldecalcitol is an analog of active vitamin D3 that improves bone mineral density and reduces the risk of osteoporotic fractures. However, the effects of eldecalcitol on muscle strength and static and dynamic postural balance are unclear. In this open-label randomized controlled study, we assessed the effects of eldecalcitol on muscle strength and static and dynamic postural balance in 50 postmenopausal women (mean age 74 years) with osteoporosis treated with bisphosphonate. Participants were randomly divided into a bisphosphonate group (alendronate at 35 mg/week; n = 25) or an eldecalcitol group (eldecalcitol at 0.75 μg/day and alendronate at 35 mg/week; n = 25) and were followed up for 6 months. Trunk muscle strength, including back extensor strength and iliopsoas muscle strength, was measured. Static standing balance was evaluated and the one leg standing test was performed to assess static postural balance. Dynamic sitting balance was evaluated and the 10-m walk test, functional reach test, and timed up and go test were performed to assess dynamic postural balance. At 6 months, there were no significant changes in any measure of muscle strength or balance in the bisphosphonate group, whereas eldecalcitol significantly increased back extensor strength (p = 0.012) and iliopsoas muscle strength (p = 0.035). Eldecalcitol also significantly improved findings on the timed up and go test (p = 0.001) and dynamic sitting balance (p = 0.015) at 6 months. These results with eldecalcitol may have an impact on prevention of falls.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The osteoporotic fractures that often occur in postmenopausal women, including vertebral fractures, hip fractures, wrist–forearm fractures, humeral fractures, and pelvic fractures, have a negative impact on quality of life and increase morbidity and mortality [1–5]. Thus, prevention of osteoporotic fractures is an important target of osteoporosis treatment.
Most nonvertebral osteoporotic fractures occur as a result of falls [6, 7]. Several factors have been considered risk factors for falls in the elderly, including a history of falls, impairment of muscle strength of the lower extremities and walking ability, postural imbalance, spinal deformity, and a decrease in spinal mobility [8, 9]. Studies have also indicated that osteoporosis with spinal deformity leads to impaired balance [10–13]. Therefore, improving postural balance and improving bone strength are important factors in the prevention of osteoporotic fractures.
Vitamin D has long been used in the prevention of osteoporosis because of its apparent fracture-preventive effects [14, 15]. Previous studies have shown that vitamin D acts directly on bones as well as extraskeletally on skeletal muscles to prevent falls [16, 17]. Activated vitamin D3 also inhibits osteoporotic fractures by acting on bone tissue, and improves muscle strength and sense of balance [18], thus helping prevent falls [19]. Alfacalcidol (1α-hydroxyvitamin D3), an activated vitamin D3, is known to improve muscle power and balance evaluated by the timed up and go (TUG) test and reduce the incidence of falls [20]. Eldecalcitol [ED-71; 2β-(3-hydroxypropyloxy)-1,25-dihydroxyvitamin D3] is a new, activated vitamin D3 analog that has been clinically available in Japan since 2011. It has been reported that eldecalcitol (0.75 μg/day) was more effective than alfacalcidol (1 μg/day) in suppressing bone turnover, increasing lumbar spine and total hip bone mineral density (BMD), and preventing vertebral fractures in patients with osteoporosis [21]. It was also reported that eldecalcitol significantly reduced the risk of forearm fractures compared with alfacalcidol [21]. The mechanism for this strong forearm fracture prevention effect is unknown, but it has been suggested that eldecalcitol may improve biomechanical properties of long bones and improve physical balance through the actions of vitamin D, which has been shown to prevent falls and improve muscle strength [22]. However, none of these possibilities have been studied in a clinical trial, especially regarding the effects of eldecalcitol on postural static and dynamic balance.
The TUG test and the functional reach test (FRT) are common methods to analyze dynamic balance [23, 24]. In addition to the TUG test, this study used a new device to measure dynamic sitting balance and response to external stimuli. The purpose of this study was to quantitatively assess the effects of eldecalcitol on muscle strength and static and dynamic postural balance in postmenopausal women with osteoporosis treated with a bisphosphonate with or without eldecalcitol.
Materials and methods
Patients and study design
A total of 50 Japanese women (mean age 74 years, range 63–86 years) who met the entry criteria between December 1, 2011 and September 30, 2012 were enrolled in this open-label randomized controlled study, which was conducted at the Oga-Minato General Hospital. They were drawn from Oga-Minato City in Japan. Inclusion criteria were postmenopausal osteoporosis diagnosed according to the criteria of the Japanese Society for Bone and Mineral Research (year 2000 revision) [25] and the ability to take part in the measurement of physical function parameters. Exclusion criteria were the presence of dementia, Parkinson’s disease, cranial nerve disorders, spinal disorders, antipsychotic use, or severe osteoarthritis of the knee; the presence of comorbidities, including gastrectomy, renal failure, or bone diseases other than osteoporosis, such as cancer-induced bone loss, primary hyperparathyroidism, hyperthyroidism, Cushing’s syndrome, multiple myeloma, Paget’s disease of the bone, and osteogenesis imperfecta; and use of glucocorticoids, hormone therapy, active vitamin D3, or raloxifene.
Participants were randomly divided into two groups. The bisphosphonate-only group (BP group; n = 25) was the control group and received alendronate (35 mg/week). The combination therapy group (ELD group, n = 25) received eldecalcitol (0.75 μg/day) and alendronate (35 mg/week). Treatment continued for 6 months in both groups.
The protocol was approved by the Ethical Committee of our institute. Written informed consent for the study and its publication was obtained from all patients.
Variables assessed
Age, height, body weight, body mass index, BMD of the distal forearm, and spinal curvature were assessed before treatment. Blood samples were obtained for biochemical analysis. Muscle strength and static and dynamic balance were evaluated before treatment and after 6 months of treatment. The researcher who performed the balance assessments was blinded to the allocation of participants.
Measurement of bone mass and spinal curvature
The BMD of the distal third of the radius was measured by dual-energy X-ray absorptiometry with a DTX-200 instrument (Osteometer MediTech, Hawthorne, CA, USA) at the start of treatment. Spinal curvature was evaluated with a SpinalMouse® (Idiag, Volkerswill, Switzerland), a computer-assisted and noninvasive device to measure spinal shape and mobility with use of surface-based techniques [26]. The thoracic kyphosis angle (Cobb angle between T1 and T12), lumbar kyphosis angle (Cobb angle between T12 and S1), and spinal inclination angle (angle between a straight line from T1 to S1 and true vertical) were evaluated. Spinal inclination reflected a forward-stooped posture. All parameters were measured with the participant in a neutral standing position without any support. All spinal data could be measured and then calculated automatically and easily by the sliding of the SpinalMouse® along the spine within a short amount of time to complete the measurement. The intraclass coefficients for curvature measurement with the SpinalMouse® were 0.92–0.95 [26].
Blood biochemical tests
Serum samples were obtained from each patient, and the levels of total protein, serum albumin, alkaline phosphatase, aspartate aminotransferase, creatinine, calcium, phosphorus, cross-linked N-telopeptide of type I collagen, and bone-specific alkaline phosphatase were assessed by standard laboratory techniques before treatment. Cross-linked N-telopeptide of type I collagen was measured by enzyme-linked immunosorbent assay (Osteomark; Mochida Pharmaceutical, Tokyo, Japan), and bone-specific alkaline phosphatase was measured by enzyme immunoassay (Osteolinks-BAP; DS Pharma Biomedical, Osaka, Japan). All blood samples were drawn in the morning.
Measurements of muscle strength
For grip strength, the mean value from measurements of both hands with a hand grip dynamometer (TH-YO2, Tsutsumi, Tokyo, Japan) was used, with participants in the upright position. Iliopsoas muscle strength was measured twice manually with a handheld dynamometer (Power Track II; JTEC Med, Salt Lake City, UT, USA), and the mean value of the right hand and the left hand was used. For back extensor strength, isometric muscle strength was measured twice with the participant in the prone position with a dynamometer with a strain gauge (DPU-1000 N digital force gauge; Imada, Toyohashi, Japan), and the larger value was used. With regard to precision of measurement, the coefficient of variation was 2.3 % [9, 27].
Assessment of static postural balance
Static postural balance was measured with a one leg standing (OLS) test and a stabilometer (UM-BAR; Unimec, Tokyo, Japan). The OLS test was performed with participants standing on their left leg for as long as possible. The participants stood with their eyes open and aligned both arms with their body trunk without using any support.
For measurement of static postural balance, center of gravity (COG) deviation was recorded by a microcomputer with the participant standing unaided in the upright position for 30 s with the eyes open and closed. Total movement of the COG during measurement was calculated as the total length. In addition, we evaluated the rectangular area, which was the area covered by the movement of the COG, calculated as the product of the maximal anteroposterior and right–left distances of the track, expressed as the two-dimensional extent of swaying.
Assessment of dynamic postural balance
The 10-m walk test was used to assess dynamic physical function. The FRT was used to determine dynamic postural balance with a fixed base of support. Participants stood on two legs, positioned shoulder-width apart, and lifted one arm up to 90° forward with flexion and extended fingers [23]. Participants were required to reach forward beyond the length of their arm without losing their balance. Test–retest reliability and validity were reported previously [23]. The TUG test measured the amount of time required for participants to rise from a standard armchair, walk 3 m, turn, return, and sit down again. The reliability and validity were reported previously [24].
Dynamic sitting balance was measured with an originally developed dynamic balance measuring device [28] (Fig. 1). This device tilts to a maximum of 3° to both sides by means of a direct current motor (BHM62MT-G2; Oriental Motor, Tokyo, Japan). It can calculate the COG with three triaxial force sensors (USL06-H5; Tec Gihan, Kyoto, Japan) arranged under the seat surface. Participant sat on the device with their arms across the anterior chest, eyes open, and without their feet touching the floor (Fig. 2). Dynamic trunk sway during external stimuli was measured with the COG trajectory for 30 s, and the ability to respond to external stimuli was assessed. The total length of the COG trajectory and the rectangular area were considered indicators of dynamic postural balance.

a, b Our novel balance device. The device can tilt to a maximum of 3° to both sides by means of a direct current motor (c, d). It can calculate the center of gravity with three triaxial force sensors arranged under the seat surface

A participant sat on the device with the arms crossed over the chest (a), eyes open, and without the feet touching the floor (b). Dynamic trunk sway during external stimuli was measured with the center of pressure trajectory for 30 s
Statistical analysis
Data are shown as the mean and standard deviation for each variable. Participant characteristics and differences between the BP group and the ELD group were compared by the unpaired Student t test or the Mann–Whitney test. Differences in measurements before and after treatment were compared by the paired Student t test. All data were analyzed using SPSS version 19.0 for Windows (SPSS, Chicago, IL, USA). The significance level was p < 0.05.
Results
Background of participants at the baseline
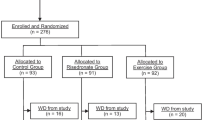
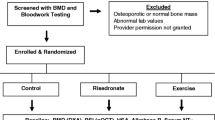
During the 6-month treatment period, 15 women dropped out of the study, including eight who withdrew for personal reasons, and seven who withdrew for an acute-phase reaction to bisphosphonates (nausea two; stomachache four; and diarrhea one). The final analysis included 35 women (17 in the BP group and 18 in the ELD group) (Fig. 3). Participant characteristics are shown in Table 1. There were no significant differences between groups in age, height, weight, body mass index, BMD, and its percentage of the young adult mean. Static standing spinal curvatures, including thoracic and lumbar kyphosis angles and spinal inclination angles, did not differ significantly between groups at the baseline.

Flow diagram of the study. BP group bisphosphonate monotherapy group, ELD group combined bisphosphonate and eldecalcitol therapy group,
Biochemical and bone metabolic markers at the baseline
Table 2 shows the levels of the biochemical and bone metabolic markers at the baseline. There were no significant differences between groups in any variable except for phosphorus level, which was significantly higher in the BP group (p = 0.024).
Muscle strength and static and dynamic postural balance
There were no significant differences between groups in muscle strength or static and dynamic postural balance at the baseline (Tables 3, 4). After 6 months, there were no significant differences in muscle strength or static and dynamic postural balance in the BP group (Tables 3, 4). In the ELD group, back extensor strength (p = 0.012) and iliopsoas muscle strength (p = 0.035) were significantly increased at 6 months compared with the baseline. Similarly, the TUG test findings (p = 0.001), the total length of the COG trajectory (p = 0.015), and the rectangular area (p = 0.034) were also significantly improved at 6 months compared with the baseline. There were no significant differences between the levels at the baseline and at 6 months in grip strength, the OLS test findings, static standing postural balance, the 10-m walk test findings, and the FRT findings in the ELD group.
Discussion
This study showed that the new active vitamin D3 analog, eldecalcitol, significantly increased muscle strength of the lower extremity and back extensor, improved dynamic balance evaluated with the TUG test, and improved the response to external stimuli evaluated with an originally developed dynamic balance measuring device. This is the first study to show that eldecalcitol improved dynamic sitting balance and response to external stimuli.
Conventional active vitamin D3, alfacalcidol (0.5–1.0 μg/day), has been shown to significantly improve muscle strength, postural balance, and physical function [20, 29–31]. These clinical studies revealed alfacalcidol reduced the fear of falls and the incidence of falls in elderly women with osteoporosis [20, 32]. Active vitamin D3 exerts significant effects on prevention of falls by improving muscle strength, postural balance, and physical function. However, the effect of the new active vitamin D3 analog, eldecalcitol, on muscle strength and body balance has been reported in only one article [33], which demonstrated that eldecalcitol improved muscle power evaluated by chair-rising time in postmenopausal women with osteoporosis treated with a bisphosphonate. The present study also revealed that eldecalcitol significantly increased muscle strength of the lower extremities and back extensor as well as dynamic physical function assessed by the TUG test. These results indicate that eldecalcitol may also inhibit falls and osteoporotic fractures through its effects on muscle strength and dynamic physical function. Hagino et al. [34] reported that eldecalcitol reduced the risk of lower spinal vertebral fractures and/or severe vertebral fractures and improved health-related quality of life in patients with osteoporosis.
Recent studies have described the use of a force platform under stable and unstable conditions to measure sitting balance in stroke patients [35, 36]. These studies have indicated that sitting balance correlated with motor function, Barthel index score, and walking ability in stroke patients [37, 38]. Sitting balance is an important factor in predicting functional outcome after stroke. On the basis of these studies, we speculated that evaluation of sitting balance in elderly patients with osteoporosis would also be important in the prevention of falls.
Control of an upright posture is a complex function achieved through multisensory integration, central motor control, and context-specific response [39]. Balance control is classified as static balance control, dynamic balance control, and the ability to respond to external stimuli [40, 41]. The balance assessment measures used in this study were a standing stabilometer for static balance control, the FRT for dynamic physical function with a fixed base of support, the TUG test for dynamic physical function with a moving base of support (movement control), and dynamic sitting balance for the ability to respond to external stimuli. The TUG test and the dynamic sitting balance test findings were significantly improved with the administration of eldecalcitol.
Many falls are caused by sudden external stimuli such as slipping or tripping [42], and falls that are a consequence of balance dysfunction are more closely related to the ability to respond to external stimuli and dynamic balance than maintaining a static posture [43]. Moreover, a quick reaction is necessary to prevent falls in response to external disturbances, in which the presence of abundant type II muscle fibers in proximal muscles plays an important role. This study suggests that, in addition to the effects on muscle reported to date, eldecalcitol improves movement control and response to external stimuli. These actions are thought to be part of the mechanism for fall prevention in elderly people.
This study has several limitations. First, although this randomized controlled study strictly evaluated the effects of eldecalcitol on balance and muscle strength, it included only a small number of patients. It will be necessary to increase the number of patients and conduct a long-term investigation of the fall prevention effects of eldecalcitol. Second, we did not evaluate vitamin D insufficiency/deficiency by measuring serum 25-hydroxyvitamin D levels. Although serum vitamin D levels are also correlated with the incidence of falls, the measurement of serum 25-hydroxyvitamin D levels is not covered by health insurance in Japan.
In conclusion, the findings of this study suggest that the addition of eldecalcitol to alendronate therapy may help prevent falls by improving dynamic physical function, response to external stimuli, and proximal muscle strength in postmenopausal women with osteoporosis.
References
Bianchi ML, Orsini MR, Saraifoger S, Ortolani S, Radaelli G, Betti S (2005) Quality of life in post-menopausal osteoporosis. Health Qual Life Outcomes 3:78
Cauley JA, Thompson DE, Ensrud KC, Scott JC, Black D (2000) Risk of mortality following clinical fractures. Osteoporos Int 11:556–561
Ensrud KE, Thompson DE, Cauley JA, Nevitt MC, Kado DM, Hochberg MC, Santora AC 2nd, Black DM (2000) Prevalent vertebral deformities predict mortality and hospitalization in older women with low bone mass. J Am Geriatr Soc 48:241–249
Nguyen ND, Center JR, Eisman JA, Nguyen TV (2007) Bone loss, weight loss, and weight fluctuation predict mortality risk in elderly men and women. J Bone Miner Res 22:1147–1154
Suzuki T, Yoshida H (2010) Low bone mineral density at femoral neck is a predictor of increased mortality in elderly Japanese women. Osteoporos Int 21:71–79
Albrand G, Munoz F, Sornay-Rendu E, DuBoeuf F, Delmas PD (2003) Independent predictors of all osteoporosis-related fractures in healthy postmenopausal women: the OFELY study. Bone 32:78–85
Pluskiewicz W, Adamczyk P, Czekajlo A, Grzeszczak W, Burak W, Drozdzowska B (2012) Epidemiological data on osteoporosis in women from the RAC-OST-POL study. J Clin Densitom 15:308–314
Barrett-Connor E, Weiss TW, McHorney CA, Miller PD, Siris ES (2009) Predictors of falls among postmenopausal women: results from the National Osteoporosis Risk Assessment (NORA). Osteoporos Int 20:715–722
Kasukawa Y, Miyakoshi N, Hongo M, Ishikawa Y, Noguchi H, Kamo K, Sasaki H, Murata K, Shimada Y (2010) Relationships between falls, spinal curvature, spinal mobility and back extensor strength in elderly people. J Bone Miner Metab 28:82–87
Ishikawa Y, Miyakoshi N, Kasukawa Y, Hongo M, Shimada Y (2009) Spinal curvature and postural balance in patients with osteoporosis. Osteoporos Int 20:2049–2053
Kuczynski M, Ostrowska B (2006) Understanding falls in osteoporosis: the viscoelastic modeling perspective. Gait Posture 23:51–58
Lynn SG, Sinaki M, Westerlind KC (1997) Balance characteristics of persons with osteoporosis. Arch Phys Med Rehabil 78:273–277
Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR (2005) Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporos Int 16:1004–1010
Papadimitropoulos E, Wells G, Shea B, Gillespie W, Weaver B, Zytaruk N, Cranney A, Adachi J, Tugwell P, Josse R, Greenwood C, Guyatt G (2002) Meta-analyses of therapies for postmenopausal osteoporosis. VIII: meta-analysis of the efficacy of vitamin D treatment in preventing osteoporosis in postmenopausal women. Endocr Rev 23:560–569
Tanizawa T, Imura K, Ishii Y, Nishida S, Takano Y, Mashiba T, Endo N, Takahashi HE (1999) Treatment with active vitamin D metabolites and concurrent treatments in the prevention of hip fractures: a retrospective study. Osteoporosis Int 9:163–170
Bischoff-Ferrari HA, Borchers M, Gudat F, Durmuller U, Stahelin HB, Dick W (2004) Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res 19:265–269
Zanello SB, Collins ED, Marinissen MJ, Norman AW, Boland RL (1997) Vitamin D receptor expression in chicken muscle tissue and cultured myoblasts. Horm Metab Res 29:231–236
Muir SW, Montero-Odasso M (2011) Effect of vitamin D supplementation on muscle strength, gait and balance in older adults: a systematic review and meta-analysis. J Am Geriatr Soc 59:2291–2300
Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore MG, Zee RY, Wong JB (2004) Effect of vitamin D on falls: a meta-analysis. JAMA 291:1999–2006
Dukas L, Schacht E, Runge M, Ringe JD (2010) Effect of a six-month therapy with alfacalcidol on muscle power and balance and the number of fallers and falls. Arzneimittelforschung 60:519–525
Matsumoto T, Ito M, Hayashi Y, Hirota T, Tanigawara Y, Sone T, Fukunaga M, Shiraki M, Nakamura T (2011) A new active vitamin D3 analog, eldecalcitol, prevents the risk of osteoporotic fractures—a randomized, active comparator, double-blind study. Bone 49:605–612
Ito M, Nakamura T, Fukunaga M, Shiraki M, Matsumoto T (2011) Effect of eldecalcitol, an active vitamin D analog, on hip structure and biomechanical properties: 3D assessment by clinical CT. Bone 49:328–334
Duncan PW, Weiner DK, Chandler J, Studenski S (1990) Functional reach: a new clinical measure of balance. J Gerontol 45:M192–M197
Ng SS, Hui-Chan CW (2005) The timed up & go test: its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch Phys Med Rehabil 86:1641–1647
Orimo H, Hayashi Y, Fukunaga M, Sone T, Fujiwara S, Shiraki M, Kushida K, Miyamoto S, Soen S, Nishimura J, Oh-hashi Y, Hosoi T, Gorai I, Tanaka H, Igai T, Kishimoto H (2001) Diagnostic criteria for primary osteoporosis: year 2000 revision. J Bone Miner Metab 19:331–337
Post RB, Leferink VJ (2004) Spinal mobility: sagittal range of motion measured with the SpinalMouse, a new non-invasive device. Arch Orthop Trauma Surg 124:187–192
Miyakoshi N, Hongo M, Maekawa S, Ishikawa Y, Shimada Y, Okada K, Itoi E (2005) Factors related to spinal mobility in patients with postmenopausal osteoporosis. Osteoporos Int 16:1871–1874
Saito K, Matsunaga T, Iwami T, Shimada Y (2014) Evaluation of trunk stability in the sitting position using a new device. Biomed Res 35:127–131
Hara S, Kishimoto KN, Okuno H, Tanaka M, Saito H, Oizumi A, Itoi E (2013) Effects of alfacalcidol on back extensor strength gained through back extensor exercise in postmenopausal women with osteoporosis. Am J Phys Med Rehabil 92:101–110
Songpatanasilp T, Chailurkit LO, Nichachotsalid A, Chantarasorn M (2009) Combination of alfacalcidol with calcium can improve quadriceps muscle strength in elderly ambulatory Thai women who have hypovitaminosis D: a randomized controlled trial. J Med Assoc Thai 92:S30–S41
Verhaar HJ, Samson MM, Jansen PA, de Vreede PL, Manten JW, Duursma SA (2000) Muscle strength, functional mobility and vitamin D in older women. Aging (Milano) 12:455–460
Schacht E, Ringe JD (2012) Alfacalcidol improves muscle power, muscle function and balance in elderly patients with reduced bone mass. Rheumatol Int 32:207–215
Iwamoto J, Sato Y (2014) Eldecalcitol improves chair-rising time in postmenopausal osteoporotic women treated with bisphosphonates. Ther Clin Risk Manag 10:51–59
Hagino H, Takano T, Fukunaga M, Shiraki M, Nakamura T, Matsumoto T (2013) Eldecalcitol reduces the risk of severe vertebral fractures and improves the health-related quality of life in patients with osteoporosis. J Bone Miner Metab 31:183–189
Genthon N, Vuillerme N, Monnet JP, Petit C, Rougier P (2007) Biomechanical assessment of the sitting posture maintenance in patients with stroke. Clin Biomech (Bristol, Avon) 22:1024–1029
van Nes IJ, Nienhuis B, Latour H, Geurts AC (2008) Posturographic assessment of sitting balance recovery in the subacute phase of stroke. Gait Posture 28:507–512
Loewen SC, Anderson BA (1990) Predictors of stroke outcome using objective measurement scales. Stroke 21:78–81
Sandin KJ, Smith BS (1990) The measure of balance in sitting in stroke rehabilitation prognosis. Stroke 21:82–86
Nashner LM, Shupert CL, Horak FB, Black FO (1989) Organization of posture controls: an analysis of sensory and mechanical constraints. Prog Brain Res 80:411–418; discussion 395−417
Huxham FE, Goldie PA, Patla AE (2001) Theoretical considerations in balance assessment. Aust J Physiother 47:89–100
Wang LY, Liaw MY, Huang YC, Lau YC, Leong CP, Pong YP, Chen CL (2013) Static and dynamic balance performance in patients with osteoporotic vertebral compression fracture. J Back Musculoskelet Rehabil 26:199–205
Gabell A, Simons MA, Nayak USL (1985) Falls in the healthy elderly: predisposing causes. Ergonomics 28:965–975
Bhatt T, Espy D, Yang F, Pai YC (2011) Dynamic gait stability, clinical correlates, and prognosis of falls among community-dwelling older adults. Arch Phys Med Rehabil 92:799–805
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Saito, K., Miyakoshi, N., Matsunaga, T. et al. Eldecalcitol improves muscle strength and dynamic balance in postmenopausal women with osteoporosis: an open-label randomized controlled study. J Bone Miner Metab 34, 547–554 (2016). https://doi.org/10.1007/s00774-015-0695-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-015-0695-x