
Abstract
Particulate matter (PM) has been demonstrated to be a significant risk for the onset of respiratory diseases worldwide. We used a generalized additive model (GAM) to evaluate the effect of PM2.5 on respiratory mortality at both single and multiple lag days based on the daily data of meteorological factors and air pollution levels in Shenyang, northeast China, from 2014 to 2016. We stratified the daily mean temperature into low (≤ P25), lower (P25–P50), higher (P50–P75), and high (≥ P75) to estimate the modifying effect of PM2.5 on respiratory mortality. The results indicated that for every inter-quartile range (IQR) increased concentration in PM2.5, respiratory death for the total, males and females increased by 0.35% (95% CI: 0.00%, 0.71%), 0.46% (95% CI: 0.00%, 0.93%), and 0.58% (95% CI: 0.05%, 1.11%) at lag 7, lag 7, and lag 1, respectively. Under the multi-day lags, the largest cumulative relative risks (RRs) were 1.016 (95% CI: 0.990, 1.042) and 1.038 (95% CI: 1.000, 1.077) at lag 0–2 days for the total and females, respectively. The largest death effect of PM2.5 was found at low temperatures. Females were at the highest risk in higher and higher temperatures, with RRs of 1.021 (95% CI: 0.999, 1.042) and 1.021 (95% CI: 0.993, 1.050) at lag 0 and lag 2, respectively. Males have the highest risk in lower temperatures at lag 1, with an RR of 1.006 (95% CI: 1.000, 1.012). In the multi-pollutant models, the effects of PM2.5 were mostly increased when NO2, SO2, or O3 were added to the models. The results of the study can provide a scientific basis for public health-friendly urban planning and long-term preventive measures in northeast China.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Air pollution has become the primary concern of the global environment (Cohen et al. 2017; Li et al. 2015a). The World Health Organization (WHO) claimed in 2021a) that air pollution accounted for 7 million premature deaths globally, with millions more being illnesses as a result of inhaling contaminated air (WHO, 2021b). Several time-series studies in Europe (Beelen et al. 2014), North America (Dai et al. 2014), and Asia (Liu et al. 2019; Bailie et al. 2023; Zhang et al. 2016) have demonstrated that air pollutants are linked with increased hospital admissions, mortality, and visits to both general practitioners and emergency departments.
Epidemiological studies have widely demonstrated the hazardous effects of air pollutants (Priyankara et al. 2021; Kanellopoulos et al. 2021). In recent years, China has become one of the countries facing the most serious environmental health problems in the past few years as a result of the rapid industry development and the massive increase in vehicles (Wu et al. 2011). Particulate matters (PMs) have evolved into a major critical factor affecting human health, increasing the morbidity and mortality rate of circulatory and respiratory systems particularly (Health Effects Institute 2022). PM with aerodynamic diameters of ≤ 2.5 μm (PM2.5) is considered particularly harmful to public health and is related to the increased risk of mortality and morbidity from diverse diseases (Xing et al. 2016). High concentration of PM2.5 can have a variety of negative health consequences (Liu et al. 2021). The fine particles could enter the tiny alveoli (WHO, 2021a). Subsequently, PM2.5 can cause irritation or injure alveolar walls, leading to dysfunction for the lung (Wang et al. 2017). In consequence, increasing level of PM2.5 has been related to a wide range of acute and long-term respiratory diseases (Manisalidis et al. 2020).
Previous studies have consistently demonstrated the significant impact of PM2.5 on respiratory diseases. For example, in the United States, per 10 µg/m3 increase in PM2.5 was related to a 1.012 (95% CI: 1.009, 1.01) increasing in non-accidental deaths (Dai et al. 2014). In Kandy, Sri Lanka, the number of hospitalized visits for respiratory diseases rose by 1.95% per 10 ug/m3 increase in PM2.5 concentration (Priyankara et al. 2021). Another multi-city analysis in East Asia discovered that respiratory mortality increased by 1.00% (95% CI: 0.23%, 1.78%) with per 10 µg/m3 increase in PM2.5 concentration (lag 01). Ma et al. (2016) found a 1.014 (95% CI: 1.007, 1.021) rise in respiratory emergency room visits at lag 3 for every 10 µg/m3 PM10 increase during the dust period in Lanzhou, China. Ren et al. (2021) discovered that a 10 µg/m3 rise in PM2.5 concentration was associated with a 1.95% (95% CI: 1.63%, 2.27%) higher hospital admissions for respiratory diseases at lag 0–2 in Wuhan, China. Meanwhile, studies examining the interaction between air pollution and temperature suggested that temperature may alter the relationship between air pollution and respiratory diseases (Wang et al., 2021; Jin et al. 2022; Qian et al. 2020; Song et al. 2021). For example, Shen et al. (2023) found the impact of PM2.5 on respiratory visits was greatest at low temperatures in Lanzhou, China. Jin et al. (2022) discovered low temperatures had a greater impact on asthma on high PM2.5 days in Hefei, China.
In this study, we evaluate effects of PM2.5 on respiratory death from 2014 to 2016 by gender subgroups in Shenyang, northeast China. Considering the limited study on temperature modification and pollutant impacts in northeast China, we stratified the temperature to four levels. The synergistic effects of multiple pollutants on respiratory death were also explored. The results would provide scientific guidelines for regulatory policies to mitigate the negative effects of PM2.5 and temperature on public health.
2 Materials and methods
2.1 Study area
Shenyang, situated at 41.8°N and 123.4°E in northeast China, serves as the capital city of Liaoning province. It holds significant importance as a hub for economic activities, culture, transportation, and trade in the Northeast region of China. Shenyang experiences a temperate, sub-humid continental climate. Being a quintessential heavy industry city in northern China, Shenyang grapples with severe air pollution issues and has been actively monitoring PM2.5 levels since 2013, along with other pollutants such as PM10 (Li et al. 2015a). Despite efforts to combat pollution in recent years, PM2.5 pollution remains a persistent concern in the region.
2.2 Data collection
The daily data on respiratory deaths from 2014 to 2016 in Shenyang was provided by the Liaoning Center for Disease Control and Prevention (CDC) with gender classification. The data was coded using the International Classification of Diseases, Tenth Edition (ICD-10). In our study, we extracted respiratory death with the ICD-10 codes J00–J99. During the study period, there were no omissions of data.
Daily average concentrations of four air pollutants (PM2.5, O3, NO2 and SO2) were obtained from air quality monitoring stations in Shenyang (Fig. 1). We used the average concentrations of eleven stations. Daily meteorological data were provided by the Shenyang Meteorological Bureau. The elements include average air temperature (T), wind speed (V), air pressure (P), relative humidity (RH) and sunlight duration (SD).

Locations of eleven air pollutant monitoring stations in Shenyang, China
2.3 Statistical method
The Spearman correlation test was used to analyze the association between pollutants and meteorological factors. Since the daily death rate of respiratory diseases among Shenyang residents is a low-probability event that usually obeys a Poisson distribution (Ravindra et al. 2019), a generalized additive model (GAM) was performed to quantify the relationship between pollutants and death. The core model is built as follows:
where i is the day of observation, E(Yi) denotes the predictive number of deaths on day i; α is the intercept; β is the coefficient of the exposure-response relationship; Xi respects the concentration of PM2.5 on day i; s is the non-parameter spline function, excluding the influence of long-term trend, seasonality, calendar effect, weather, and other confounding factors; time is calendar time on day i; df means the degree of freedom; Dow is the dummy variable reflecting the weekend effect; Fi respects the daily meteorological element, which is the explanatory variable that has a nonlinear effect on the dependent variable including V, P, SD, and RH. The Akaike’s Information Criterion (AIC) is applied to guide the selection of the smoothing df. A smaller AIC value indicates a more suitable model. The specific value of df was listed in Appendix (Table S1).
In view of the adverse impacts of atmospheric pollutants on human health, which have an estimated lag of generally 0 to 7 days (Wang et al. 2019), several lag configurations have been devised to investigate the lagged impacts. A single-day lag (derived present day to the previous 7 days: lag0 to lag7) and a multi-day lag (the moving mean of the present day and the previous 1–7 days: lag01 to lag07) were considered. The daily mean temperature was categorized into low (≤ P25), lower (P25-P50), higher (P50-P75), and high (≥ P75) temperatures according to the 25th (-2.60℃), 50th (11.15℃) and 75th (21.20℃) percentiles to investigate its modification effect on respiratory death. In our study, the relative risk (RR) and 95% confidence interval (CI) were chosen as metrics to express the impact of PM2.5 on respiratory health with an IQR increase. The RR and 95% CI are calculated as follows:
All analyses were performed using the MGCV package in R (version 4.2.2). We used the two-sided method to perform the statistical tests (p < 0.05 means statistical significance).
3 Results
A total of 12,399 respiratory deaths were recorded for 11 cases each day (Table 1). The female-to-male ratio was 1 to 1.29. The daily mean concentration of PM2.5 was 66.67 µg/m3. PM2.5 concentrations of 30.6% days during the study period exceeded the National Grade II standard level (PM2.5: 75 µg/m3). Meanwhile, the daily average temperature, relative humidity, air pressure, wind speed, and sunshine duration were 9.08 °C, 61.06%, 1010.52 hPa, 2.17 m/s and 6.73 h respectively, reflecting the temperate continental monsoon climate of Shenyang.

Monthly variation of PM2.5 and number of respiratory deaths
Figure S1 and Fig. 2 showed the daily and monthly trends in PM2.5 and respiratory death for different groups. PM2.5 peaked in winter (from November to February), corresponding to a low temperature. Respiratory death number also peaked in the winter (December, January, and February). PM2.5 concentrations are highest in winter, mainly because of coal-fired heating. The concentration of PM2.5 was low in the warm season (from May to September), lowest in August, and increased sharply from September to November, reaching its highest value (108 µg/m³) in November.
A significant positive correlation was found between respiratory death and PM2.5 (R = 0.113). PM2.5 was negatively correlated with wind speed (R= -0.18), temperature (R= -0.42), precipitation (R= -0.23) and sunshine duration (R= -0.18), while air pressure (R = 0.43) and relative humidity (R = 0.06) were positively correlated with PM2.5 (Figure S2).

Exposure-response curve between PM2.5 and respiratory death (a: whole year; b: low temperature (≤ P25); c: lower temperature (P25-P50); d: higher temperature (P50-P75); e: high temperature (≥ P75). The solid line is the exposure-response curve, and the dotted lines are the 95% confidence intervals)
The exposure-response curve of PM2.5 and the total were linearly distributed, and RR increased rapidly with the increasing concentration of PM2.5 (Fig. 3a). Under the conditions of low temperatures (Fig. 3b), lower temperatures (Fig. 3c), and higher temperatures (Fig. 3d), when the concentration of PM2.5 rises, the log RR value increases linearly. The results suggest that the health risk of PM2.5 increases with an increase in pollutant concentration. Under high temperatures (Fig. 3e), the relationship between PM2.5 and death showed a V-shaped curve. When PM2.5 concentration was less than 70 µg/m³, the log RR value decreased with the increasing concentration of PM2.5; when the concentration was higher than 70 µg/m³, the log RR value rose as PM2.5 concentration increased.

RRs of PM2.5 to respiratory death at different lag structure
Figure 4 reveals the RR of respiratory death with an IQR increase in PM2.5 concentrations in single and multiple lag models. In single-day lag models, the increasing percentages for the total, males, and females’ deaths were 0.4% (0.0%, 0.7%), 0.5% (0.0%, 0.9%), and 0.6% (0.1%, 1.1%) at lag 7, lag 7, and lag 1, respectively. In multi-day lag models, the strongest effect is observed at lag 0–2 for both the total and females, with an RR of 1.021 (95% CI: 0.991, 1.042) and 1.038 (95% CI: 1.000, 1.077), respectively. No significant impact was observed for males.
The three-dimensional distribution of temperature and PM2.5 with the number of deaths reveals that the daily mean temperature and the linear state with the number of deaths in the whole year are positively correlated. There was a slight reduction in the number of deaths from diseases (Figure S3a). Under low temperatures (Figure S3b), respiratory death falls first and then rises with the increase in PM2.5 concentration. Under lower temperatures (Figure S3c), the number of deaths caused by PM2.5 increases linearly, revealing that respiratory deaths were affected by the interaction between temperature and PM2.5. Under higher temperatures (Figure S3d) and high temperatures (Figure S3e), the continuous increase in PM2.5 concentration caused a linear and slow increase in the number of deaths.

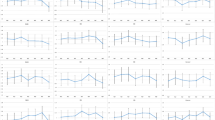
RRs and 95% CIs of respiratory death in low (a), lower (b), higher (c) and high (d) temperatures
Fig. 5 depicts the health effects of PM2.5 on different genders at low, lower, higher, and high temperatures. In low temperatures (Fig. 5a), PM2.5 had a lagging effect on subgroups. For the total and females, RR was greatest at lag0, with values of 1.007 (95% CI: 0.999, 1.015) and 1.009 (95% CI: 0.996, 1.021), respectively. The effect on males was greatest at lag4 with a RR value of 1.008 (95% CI: 0.999, 1.017). In lower temperatures (Fig. 5b), PM2.5 had an effect on lag of 1 to 5 days on the total, with the highest RR value of 1.005 (95% CI: 1.001, 1.010) at 1 day. There was an effect on females at lag 2 to 4 days, with the strongest effect at lag 3 of 1.006 (95% CI: 0.999, 1.012). There was an effect on the lag of 1 and 5 days on males, with the highest RR value of 1.006 (95% CI: 1.000, 1.012) at lag 1. In higher temperatures (Fig. 5c), PM2.5 had an effect on the lag of 1, 3 to 4, 6 to 7 days, with the highest RR value of 1.013 (95% CI: 1.000, 1.027) for the total. The highest RR value of 3 days’ lag of 1.017 (95% CI: 0.999, 1.035) was observed for males. The effect on females was found at a lag of 1–7 days, except lag 2 and lag 5, with the highest RR on the present day of 1.021 (95% CI: 0.999, 1.042). In high temperatures (Fig. 5d), no lag effect of PM2.5 was observed for the total and males. For females, there was an effect on a lag of 0–6 days except lag 1, with a highest RR of 1.021 (95% CI: 0.993, 1.050) at lag 2.
Table 2 indicated the highest RR of PM2.5 in the different temperature conditions, and the strongest effect (RR: 1.021 (95% CI: 0.993, 1.050) for females was found at lag 2 under high temperature conditions. Females were at greater risk than males. The precise cause of these discrepancies is unknown. However, they might be ascribed to behavioral, physiological, and psychological health variables (Burnett et al. 2018). Disparities in lifestyle between sexes may result in gaps in exposure patterns, resulting in this imbalance (Yue et al. 2020). The mechanisms by which PM2.5 exposure affects the health of males and females need to be investigated further.
Figure S2 shows that when SO2 or O3 was added to the dual-pollutant model (PM2.5+SO2, PM2.5+O3), the effects of respiratory death in both males and females were reduced slightly. The effects on all categories increased once NO2 was included in the model (PM2.5+NO2). The impacts of PM2.5 were amplified slightly in both the total and females at the multiple pollutants model (PM2.5+O3+SO2 + NO2), with corresponding RRs of 1.019 (95% CI:0.994, 1.044) and 1.031 (95% CI:0.996, 1.066).
4 Discussion
In the current study, PM2.5 was found to increase the risk of respiratory death, consistent with previous research findings (Huang et al. 2023; Veremchuk et al. 2021; Jin et al. 2022; Pride et al. 2015). Specifically, we observed that an interquartile range (IQR) increase in PM2.5 corresponded to a 0.4% increase in respiratory death for the total population, a 0.6% increase for females, and a 0.5% increase for males. Similar associations between PM2.5 exposure and death risk have been documented globally, although the magnitude of the effect may vary across regions. For instance, Ji et al. (2022) reported a mortality hazard ratio of 1.244 (95% CI:1.221, 1.268) for every 10 µg/m³ increase in PM2.5. In a study conducted in Beijing, Ma et al. (2016) found a relative risk of 1.140 (95% CI:1.071, 1.214) for each 10 µg/m³ increase in PM10. Similarly, Li et al. (2023) identified a significant association between PM exposure and respiratory diseases in Southern China, with odds ratios of 1.007 (95% CI: 1.006, 1.009) for PM10 and 1.010 (95% CI: 1.007, 1.013) for PM2.5 for every 10 µg/m³ increase in concentration.
We investigated both the immediate and delayed health effects of exposure to air pollutants, as epidemiological research has shown that these effects may manifest with a lag (Chien et al. 2018; Liu et al. 2021). Specifically, we examined the single-day and cumulative lagged effects of PM2.5 exposures. Our analysis revealed that the adverse effects of PM2.5 peaked at lag 7 in single-day models and at lag 0–2 in cumulative-day models. Importantly, the estimates from cumulative lag models were consistently higher than those from single-day lag models, suggesting a cumulative effect of exposure over time. Similar investigations into the lag time of air pollution’s impact on public health have been conducted in other regions. For example, a study in Beijing, China, found that the strongest effect of PM2.5 on respiratory emergencies occurred with no lag (lag 0) (Liang et al. 2017). In Guangzhou, south China, Wu et al. (2018) observed an increase of 0.95% (95% CI: 0.16%, 1.73%) in respiratory mortality at lag 0–1 of PM2.5 concentration. Additionally, in Lanzhou, northwest China, Chai et al. (2019) reported substantial cumulative effects of PM2.5 on both males and females over lag 0–14 days, with the largest relative risks observed at lag days 0–11 and 0–13, respectively. These findings underscore the importance of considering both short-term and long-term exposure to PM2.5 in assessing its health impacts. Furthermore, the method used to estimate exposure is a critical consideration in environmental epidemiology. Research from Poland suggested that using moving average concentrations may be more appropriate for modeling biological responses to PM2.5 or PM10 exposure (Nieuwenhuijsen et al., 2003; Kowalska et al. 2019). This highlights the importance of selecting appropriate exposure assessment methods to accurately capture the health effects of air pollutants.
Stratified analysis by sex indicated that females are more susceptible to pollutants than males for respiratory death, which agrees with the results in Beijing (Song et al. 2021) and Shenzhen, China (Zhang et al. 2020). In the case of temperature stratification, the health effect of PM2.5 on females is significantly higher than that of males at lag0 in all temperature stratifications. At lag1 to lag7, the impact of PM2.5 on males is higher than that on females. The result might be attributed to factors such as female sex hormones (Chowdhury et al. 2021). We suggest that further research could explain this phenomenon in terms of the physiological characteristics of both sexes. One study suggests that air pollution may affect non-smokers more than smokers (Xu 2005). The prevalence of smoking is much lower in females than males (2.0% vs. 50.5%) (WHO, 2021b). Smoking’s oxidative and inflammatory effects can desensitize males to more air pollutants, which may not further exacerbate effects along the same routes (Xu 2005).
The present study found that respiratory mortality increases with decreasing temperature even when pollutant concentrations remain constant, suggesting that low temperature is a major trigger for its onset (Shen et al. 2023; Gao et al. 2022). We revealed that PM2.5 had the greatest effect at low temperatures. Although many studies have linked respiratoration to air pollution and temperature, few studies have examined their interactive effects on mortality. We found the strongest death effect of PM2.5 at low temperatures compared with other stratifications, which agreed with the findings in the study by Zhu et al. (2022). In their study, exposure to moderate cold and extreme cold temperatures was associated with 1.68% and 1.73% odds of asthma exacerbations, respectively. Feng et al. (2022) found a strong link between PM2.5 concentrations and respiratory mortality, with a cumulative RR (lag0-4) of 1.026 (95% CI: 1.008, 1.044). According to Chai et al. (2019), the RR values for respiratory hospitalizations visits for males and females were 1.014 (95% CI: 1.006, 1.022) and 1.013 (95% CI: 1.005, 1.022), respectively, for every 10 µg/m³ rise in PM2.5 concentration. A previous study suggested that on low-temperature days, reduced beating frequency of nasal and tracheal cilia affects PM clearance, making people more susceptible to PM2.5, which is suspected to be a potential mechanism for the greater impact of PM2.5 on mortality on low-temperature days (Jiang et al. 2019). Furthermore, cold temperatures may aggravate airway inflammation and impose additional stress on respiratory function (Deng et al. 2020).
In the two-pollutant models, we observed that the estimated impact of PM2.5 on respiratory death was slightly attenuated compared to the estimates from the single-pollutant models, which is consistent with findings reported in previous studies (Ren et al. 2021; Feng et al. 2022). These results suggest that additional pollutants may indeed influence the health effects attributed to PM2.5. However, in the multiple pollutants models, where PM2.5 was analyzed in conjunction with O3, SO2, and NO2, we observed an amplification of the impacts of PM2.5 on both the total population and females. Similar findings have been reported in studies conducted in Finland (Balogun et al. 2020) and Beijing, China (Zhang et al. 2021), where significant relationships between synergistic effects and maximum exposure levels for PM2.5, SO2, NO2, and O3 were identified across all groups examined. Although the intensity of these relationships varied between studies, the overarching conclusions were consistent. These findings underscore the importance of considering multiple pollutants simultaneously when assessing their health impacts, as they often exhibit strong covariance and may interact synergistically to exacerbate adverse health outcomes. Nevertheless, the underlying mechanisms driving these pollutant interactions remain complex and warrant further investigation. Future studies aimed at elucidating these mechanisms will be crucial for informing effective air quality management strategies and public health interventions. According to toxicological studies, PM2.5 exposures can promote lung inflammation and impair pulmonary immune function (Liang et al. 2017). Several studies conducted over the last two decades have demonstrated the effects of PM2.5 on total death due to respiratory diseases (Senthil et al. 2018; Samek et al., 2016) or hospital admissions for cause-specific respiratory diseases such as asthma, pneumonia, and chronic obstructive pulmonary disease (Luo et al. 2018; Krall et al. 2017). Furthermore, it is known that airborne pollutants interact with airborne allergens, raising the likelihood of atopic sensitization and worsening of respiratory illness symptoms (Ma et al. 2017). When fine PM and allergens penetrate deep into the lungs, irritation occurs, causing alveolar inflammation, which inhibits air flow and results in acute respiratory episodes (Li et al. 2016). The consequences of acute PM inhalation endanger public health, particularly among vulnerable populations.
Our study is one of the few to search for the synergic effects of PM2.5 and temperature on respiratory death in northeast China. The findings are helpful in determining the real incubation duration and effect estimates for respiratory diseases. However, some limits also need to be mentioned. First, air pollutant data from 11 monitoring sites may not adequately reflect individual exposure, and RR is used to describe the effects of air pollution exposure on daily deaths rather than the number of daily death itself, resulting in varying degrees of overestimation or underestimation of the impact estimates. Then, while we account for long-term trends and confounding factors, we cannot totally eliminate the effects of individual factors, which can alter individual reactions to pollutants and result in varied results. As a result, effect estimates may not be applicable to everyone in Shenyang. Furthermore, the chemical composition of PM2.5 and its sources vary by geography, which may result in diverse impacts on death.
5 Conclusion
We found a strong association between PM2.5 and the RRs for respiratory death in Shenyang, northeast China. Temperature significantly modified the effects of PM2.5 on respiratory death. Stratified analysis by sex showed that females were more vulnerable to PM2.5. This study will help to better understand the impact of the overall atmospheric environment on respiratory diseases. The findings of this study might help local health authorities take preventative actions in the long term.
Data availability
Data will be available on request
References
Bailie CR, Ghosh JK, Kirk MD et al (2023) Effect of ambient PM2.5 on healthcare utilisation for acute respiratory illness, Melbourne, Victoria, Australia, 2014–2019. J Air Waste Manage Assoc 73(2):120–132
Balogun HA, Rantala AK, Antikainen H et al (2020) Effects of air pollution on the risk of low birth weight in a cold climate. Appl Sciences-Basel 10(18):6399
Beelen R, Raaschou-Nielsen O, Stafoggia M et al (2014) Effects of long-term exposure to air pollution on natural-cause mortality: an analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 383(9919):785–795
Burnett R, Chen H, Szyszkowicz M et al (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc Natl Acad Sci USA 115(38):9592–9597
Chai GR, He H, Sha YZ et al (2019) Effect of PM2.5 on daily outpatient visits for respiratory diseases in Lanzhou, China. Sci Total Environ 649:1563–1572
Chien LC, Guo Y, Li X et al (2018) Considering spatial heterogeneity in the distributed lag non-linear model when analyzing spatiotemporal data. J Expo Sci Environ Epidemiol 28:13–20
Chowdhury NU, Guntur VP, Newcomb DC et al (2021) Sex and gender in asthma. Eur Respiratory Rev 30(162):210067
Cohen AJ, Brauer M, Burnett R et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the global burden of diseases study 2015. Lancet (London England) 389(10082):1907–1918
Dai L, Zanobetti A, Koutrakis P et al (2014) Associations of fine particulate matter species with mortality in the United States: a multicity time-series analysis. Environ Health Perspect 122:837–842
Deng LJ, Ma P, Wu Y et al (2020) High and low temperatures aggravate airway inflammation of asthma: evidence in a mouse model. Environ Pollut 256:113433
Feng Q, Chen Y, Su S et al (2022) Acute effect of fine particulate matter and respiratory mortality in Changsha, China: a time-series analysis. BMC Pulm Med 22(416):11
Gao CH, Yao X, Wang X et al (2022) Effects of air pollutants and temperature on the number of asthma outpatient visits in Hohhot, China. Int J Environ Health Res 26:1–8
Health Effects Institute (2022) Burden of Disease Attributable to Coal-Burning and other. Air Pollution Sources in China
Huang YJ, Wang YY, Zhang T et al (2023) Exploring health effects under specific causes of mortality based on 90 definitions of PM2.5 and cold spell combined exposure in Shanghai, China. Environ Sci Technol 57:2423–2434
Ji JS, Liu LX, Zhang JF et al (2022) NO2 and PM2.5 air pollution co-exposure and temperature effect modification on pre-mature mortality in advanced age: a longitudinal cohort study in China. Environ Health 21:97
Jiang YX, Chen RJ, Kan HD (2019) The interaction of ambient temperature and air pollution in China. Ambient Temperature and Health in China 105 – 116
Jin XY, Xu ZW, Liang YF et al (2022) The modification of air particulate matter on the relationship between temperature and childhood asthma hospitalization: an exploration based on different interaction strategies. Environ Res 214(2):113848
Kanellopoulos N, Pantazopoulos I, Mermiri M et al (2021) Effect of PM2.5 levels on respiratory pediatric ed visits in a semi-urban Greek peninsula. Int J Environ Res Public Health 18(12):6384
Kowalska M, Skrzypek M, Kowalski M et al (2019) The relationship between daily concentration of fine particulate matter in ambient air and exacerbation of respiratory diseases in silesian agglomeration, Poland. Int J Environ Res Public Health 16(7):1131
Krall JR, Mulholland JA, Russell AG et al (2017) Associations between source-specific fine particulate matter and Emergency Department visits for respiratory disease in four U.S. cities. Environ Health Perspect 125:97–103
Li Y, Zhao HJ, Wu YF (2015) Characteristics of Particulate Matter during Haze and Fog (Pollution) episodes over Northeast China, Autumn 2013. Aerosol Air Qual Res 15(3):853–864
Li Y, Ma ZQ, Zheng CJ et al (2015a) Ambient temperature enhanced acute cardiovascular-respiratory mortality effects of PM2.5 in Beijing, China. Int J Biometeorol 59(12):1761–1770
Li MH, Fan LC, Mao B et al (2016) Short-term exposure to ambient fine particulate matter increases hospitalizations and mortality in COPD: a systematic review and Meta-analysis. Chest 149:447–458
Li HP, Liang LZ, Zhang SY et al (2023) Short-term ambient particulate matter pollution of different sizes and respiratory hospital admission in the Beibu Gulf area of southern China. Atmos Environ 294:119524
Liang F, Tian L, Guo Q et al (2017) Associations of PM2.5 and black carbon with hospital emergency room visits during heavy haze events: a case study in Beijing, China. Int J Environ Res Public Health 14(7):725
Liu C, Chen R, Sera F et al (2019) Ambient Particulate Air Pollution and Daily Mortality in 652 cities. N Engl J Med 381:705–715
Liu XB, Wen XM, Sun XH et al (2021) The short-term effects of Ambient Air pollutants are Associated with Daily Mortality in Northeast China from 2014 to 2018: a Time Series Analysis. J Occup Environ Med 63:173–180
Luo L, Zhang Y, Jiang J et al (2018) Short-term effects of Ambient Air Pollution on hospitalization for respiratory disease in Taiyuan, China: a Time-Series Analysis. Int J Environ Res Public Health 15(10):2160
Ma YX, Xiao BS, Liu C et al (2016) Association between ambient air pollution and emergency room visits for respiratory diseases in spring dust storm season in Lanzhou, China. Int J Environ Res Public Health 13(6):613
Ma YX, Zhang HP, Zhao YX et al (2017) Short-term effects of Air Pollution on Daily Hospital admissions for Cardiovascular diseases in Western China. Environ Sci Pollut Res 24:14071–14079
Manisalidis I, Stavropoulou E, Stavropoulos A et al (2020) Environmental and health impacts of air pollution: a review. Front Public Health 8:14
Nieuwenhuijsen MJ (2003) Exposure Assessment in Occupational and Environmental Epidemiology. Oxford University Press, pp 21–38
Pride KR, Peel JL, Robinson BF et al (2015) Association of short-term exposure to ground-level ozone and respiratory outpatient clinic visits in a rural location - Sublette County, Wyoming, 2008–2011. Environ Res 137:1–7
Priyankara S, Senarathna M, Jayaratne R et al (2021) Ambient PM2.5 and PM10 exposure and respiratory disease hospitalization in Kandy, Sri Lanka. Int J Environ Res Public Health 18(18):9617
Qian X, Zbs B, Yan TA et al (2020) Impacts of urbanization on the temperature-cardiovascular mortality relationship in Beijing, China. Environ Res 191:110234
Ravindra K, Rattan P, Mor S et al (2019) Generalized additive models: building evidence of Air Pollution, Climate Change and Human Health. Environ Int 132:104987
Ren Z, Liu XY, Liu TY et al (2021) Effect of ambient fine particulates (PM2.5) on hospital admissions for respiratory and cardiovascular diseases in Wuhan, China. Respir Res 22(128):11
Samek L (2016) Overall human mortality and morbidity due to exposure to air pollution. Int J Occup Med Environ Health 29(3):417–426
Senthil KS, Muthuselvam P, Pugalenthi V et al (2018) Toxicoproteomic analysis of human lung epithelial cells exposed to steel industry ambient particulate matter (PM) reveals possible mechanism of PM related carcinogenesis. Environ Pollut 239:483–492
Shen JH, Ma YX, Zhang YF et al (2023) Temperature modifies the effects of air pollutants on respiratory diseases. Environ Sci Pollut Res 30:61778–61788
Song XP, Jiang LZ, Wang SG et al (2021) The impact of main air pollutants on respiratory emergency department visits and the modification effects of temperature in Beijing, China. Environ Sci Pollut Res 28:6990–7000
Veremchuk LV, Vitkina TI, Barskova LS et al (2021) Estimation of the size distribution of suspended particulate matters in the Urban Atmospheric Surface Layer and its influence on Bronchopulmonary Pathology. Atmosphere 12(8):1010
Wang P (2021) China’s air pollution policies: Progress and challenges. Curr Opin Environ Sci Health 19:100227
Wang W, Mao FY, Du L et al (2017) Deriving hourly PM2.5 concentrations from Himawari-8 AODs over Beijing-Tianjin-Hebei in China. Remote Sens 9(8):858
Wang C, Feng L, Chen K (2019) The impact of ambient particulate matter on hospital outpatient visits for respiratory and circulatory system disease in an urban Chinese population. Sci Total Environ 666:672–679
World Health Organization (2021a) Global report on trends in prevalence of tobacco use 2000–2025, fourth edition
World Health Organization (2021b) What are the WHO Air quality guidelines? Improving health by reducing air pollution
Wu Y, Wang R, Zhou Y et al (2011) On-road vehicle emission control in Beijing: past, present, and future. Environ Sci Technol 45(1):147–153
Wu R, Zhong L, Huang X et al (2018) Temporal variations in ambient particulate matter reduction associated short-term mortality risks in Guangzhou, China: a time-series analysis (2006–2016). Sci Total Environ 645:491–498
Xing YF, Xu YH, Shi MH et al (2016) The impact of PM2.5 on the human respiratory system. J Thorac Dis 8(1):69–74
Xu ZY (2005) Effect evaluation on smoking control plan for one year in Beijing, China, WHO smoking control capability construction cooperation items. Chin J Health Educ 21:412–416
Yue HB, He CY, Huang QX et al (2020) Stronger policy required to substantially reduce deaths from PM2.5 pollution in China. Nat Commun 11:1462
Zhang S, Li G, Tian L et al (2016) Short-term exposure to air pollution and morbidity of COPD and asthma in east Asian area: a systematic review and meta-analysis. Environ Res 148:15–23
Zhang YQ, Ding Z, Xiang QQ et al (2020) Short-term effects of ambient PM1 and PM2.5 air pollution on hospital admission for respiratory diseases: case-crossover evidence from Shenzhen, China. Int J Hyg Environ Health 224:113418
Zhang YF, Ma YX, Feng FL et al (2021) Association between PM10 and specific circulatory system diseases in China. Sci Rep 11:12129
Zhu YX, Yang T, Huang SJ et al (2022) Cold temperature and sudden temperature drop as novel risk factors of asthma exacerbation: a longitudinal study in 18 Chinese cities. Sci Total Environ 814:151959
Acknowledgements
This research was supported by the National Natural Science Foundation of China (Grant Nos. 42375177, 41975141), Natural Science Foundation of Gansu (Grant No. 23JRRA1079) and Fundamental Research Funds for the Central Universities (number: lzujbky-2022-it21).
Author information
Authors and Affiliations
Contributions
Ma.Y. designed and carried out the research; Zhao. Y. set up models and result analysis; Liu. Z.and Qin. P. analyzed data; Wang. W., Jiao.H. and Zhang.Y. collected and assembled data; Zhao.Y. and Ma.Y. wrote and revised the manuscript.
Corresponding author
Ethics declarations
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Conflict of interest
The authors have no conflict of interest to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhao, Y., Ma, Y., Liu, Z. et al. Evaluation of temperature modifying effect of PM2.5 on respiratory mortality in high latitude monsoon area. Theor Appl Climatol 155, 6167–6175 (2024). https://doi.org/10.1007/s00704-024-05002-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00704-024-05002-9