
Abstract
China is among the countries with the worst air quality throughout the world. As PM2.5 was not included in the national air quality monitoring network before January 2013 in China, no study has investigated the associations of ambient PM2.5 and O3 with cardiovascular mortality in Hefei, China. In this time-series analysis, Poisson regression in generalized additive model was adopted to assess the associations between the air pollutants and cardiovascular mortality during the 2013–2015 in Hefei, China. The findings showed that the daily average level of PM2.5 and O3 was 77.8 μg/m3 and 60.1 μg/m3 in the study period, respectively. PM2.5 and O3 exposure tended to increase cardiovascular mortality, but the associations were statistically insignificant. Further stratified analyses by seasons showed that with every 10 μg/m3 increase of PM2.5 in the cold season (October–March), the risk of cardiovascular death increased by 0.22% (95% CI 0.05%, 0.39%); while every 10 μg/m3 increase of O3 in the warm season (April–September), the risk of cardiovascular death increased by 1.29% (95% CI 0.26%, 2.33%) on Lag0. Interestingly, stratified analysis by gender showed that the associations of PM2.5, but not O3 exposure, could significantly increase cardiovascular mortality in females, but not males. The findings of this study especially underscored the adverse associations of PM2.5 and O3 exposure with females in specific seasons. More studies are needed to verify our findings and further investigate the underlying mechanisms.

Graphical Abstract
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ambient air pollution has become a major concern throughout the world, especially in some developing countries including China that the intensive urbanization and construction in the past decade has led to substantial aggravation of air pollution (Tsai et al. 2014; Tsangari et al. 2016). In addition to respiratory disorders, accumulating evidence has also demonstrated that air pollution exposure contributes to cardiovascular mortality. For instance, in the largest and most definitive US nationwide cohort to date, Pope (Pope et al. 2015) found that long-term fine particulate matter (PM2.5) exposure could significantly increase the risk of cardiovascular mortality (HR per 10 μg/m3: 1.12, 95% confidential interval [CI] 1.08, 1.15), which has been confirmed by some other studies. Ozone (O3), in addition, has also been shown to be a pollutant associated with increased risk of cardiovascular and respiratory disorders (Coogan et al. 2017; Raza et al. 2018). On the other hand, however, some studies have only found weaker or even no association between air pollution and cardiovascular mortality. For example, the European Study of Cohorts for Air Pollution Effects [ESCAPE] investigated 367,383 individuals from 22 European cohorts, but found that PM2.5 exposure did not significantly increase the overall risk of cardiovascular mortality (Beelen et al. 2014). Therefore, there is still an interest in investigating the associations between outdoor air pollution exposure and mortality.
Air pollution in China is greatly different from the air pollution in western countries, both from the aspects of pollution level and components, which has already been widely acknowledged. A previous study in 2011 (Yang et al. 2011) has indicated that PM2.5 in China has high content of crustal materials due to transported dust from desert and arid loess-land and locally induced dust in relation to lower vegetation coverage and intensive urban construction. In the past decade, the accelerated urbanization in the major cities in China could have greatly increased the content of transported dusts (Chen et al. 2017). In addition, however, the sharp increase of the number of personal vehicles in recent years could also increase the components from biomass burning (Bai et al. 2018); the consequent exhausts from the vehicles can further give rise to particulate matters and ozone. Hefei is the capital city of Anhui province, which is also the economic and cultural center of this province. In the past decade, Hefei witnessed substantial changes regarding expansion and urbanization (Li et al. 2018; Zhang et al. 2017). Such changes, indeed, not only have brought great convenience to the residents in Hefei, but also led to worsening of air pollution. A previous time-series study (Zhang et al. 2017) has already shown that exposure of PM10, SO2, and NO2 could significantly increase cardiovascular mortality. However, the associations of PM2.5 and O3 with cardiovascular mortality have not been investigated in this city yet.
Since January 2013, Hefei has introduced PM2.5 in the air quality monitoring network (Lin et al. 2016a). The objective of this study was thus to evaluate the short-term associations of PM2.5 and O3 with cardiovascular mortality in the residents in Hefei, China, between January 1, 2013, and December 31, 2015.
Materials and methods
Study area
Hefei, the capital city of Anhui province and also a core city of the Wanjiang Urban Belt, is located at the Yangtze River Delta (31.87° N, 117.28°E). Hefei includes 4 districts, one county-level-city, and 4 counties. According to the statistics of the Chinese National Bureau of Statistics, there were over 7.17 million permanent residents in Hefei at the end of 2015. Hefei witnessed rapid economic development in the past several years, which was accompanied with great decrease of the air quality. The annual mean value of PM2.5 in Hefei was 84.9 μg/m3 in 2013, which ranked 17th among the 74 cities measured. In this study, the study area was restricted to the urban area of Hefei, which included the 4 districts as follows: Shushan, Luyang, Yaohai, and Baohe Districts.
Air pollution and meteorological data
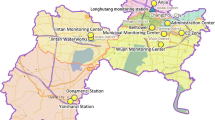
The daily air pollution data of Hefei between January 1, 2013, and December 31, 2015 were obtained from the Hefei Environmental Protection Bureau (HEPB). HEPB has established 10 monitoring stations in Hefei city area (Fig. 1), which continuously monitor the air quality 24 h a day, 365 days a year, without interruption. The major pollutants monitored include O3 and PM2.5. There were no missing data during the study period. The meteorological data, including mean temperature, pressure, relative humidity, and wind speed, at the same period, were obtained from the China Meteorological Data Network (http://data.cma.cn).

District map of Hefei, China, with air quality monitoring stations locations
Cardiovascular mortality data
The cardiovascular mortality data of the residents in Hefei between January 1, 2013, and December 31, 2015, were obtained from the Hefei Centers for Disease Control and Prevention (Hefei CDC). According to the International Statistical Classification of disease, 10th revision codes, the deaths of the permanent residents in the 4 districts of Hefei city with the code of ICD-10: I00-I99 were included in this study. The data of the subjects, including gender, age, permanent living address, data of death, and cause of death, were collected.
Statistical analysis
Microsoft Excel software was used to construct the database of the daily air pollution, meteorological data, and the daily cardiovascular deaths in Hefei. The database was then input into the SPSS 22.0 software for descriptive analysis. The data were firstly described by means, standard divisions, and percentiles, and then the associations between the air pollutants and meteorological data were assessed by Spearman correlation test.
For the time-series analysis, the MGCV in the R3.2.3 software (version 3.1.2, R Foundation for Statistical Computing, http://cran.r-project.org/) was used. Poisson regression in generalized additive model (GAM) (Rodopoulou et al. 2014) was adopted to assess the associations between the air pollutants and cardiovascular mortality. The equation of the model is as below:
In this equation, t is the date of death; Y is the number of the death on day t; α is the intercept; and E(Yt) is the predictive number of death on day t; β is the regression coefficient; DOW is the dummy variable of the weeks; Xt is the concentration of the air pollutant on day t; s is the smoothing spline function of the nonlinear variables; time is the date; df is the degree of freedom; and Zt is the meteorological data on day t (Lin et al. 2016b). The df (Tian et al. 2013) was chosen according to the minimum Akaike Information Criterion (AIC), of which the smaller value indicates better fitness of the model.
In this study, the df of time was set as 7, while the dfs of Zt (including temperature, relative humidity, mean wind speed, and pressure) were all 3. In the analysis, the lag associations between the pollutants and cardiovascular mortality were assessed, from the current day up to 5 days before (Lags0–5). In addition, 2 to 6 days moving average values (Lags01–05) of the pollutants were also used to assess the associations with cardiovascular mortality, to investigate the cumulative associations of the exposure. Furthermore, the data were also stratified by age (< 75 and ≥ 75 years) (Yin et al. 2017), gender (females and males), and season (cold [from October to March] and warm [from April to September] seasons) for further analysis. Multi-pollutant models were also used in addition to single-pollutant models to assess the interactions between the pollutants. Because the assumption of the linearity between the log of mortality and air pollutants may not be justified, the spline function was used to graphically analyze their relations (Kan et al. 2007). The dfs of air pollutants (including PM2.5 and O3) were set as 3. The results were described as excess risks (ERs) and corresponding 95% confidential intervals (CIs) for each 10 μg/m3 increase of the pollutant concentrations. P < 0.05 was considered statistically significant.
Results
Description of the data
There were no missing data about the air pollutants and meteorological data during the study period. The daily average level of PM2.5 was 77.8 μg/m3, of which the highest level was up to 373.0 μg/m3.When stratified by season, the daily average level of PM2.5 in the warm and cold seasons was 61.8 and 94.1 μg/m3, respectively. While for the level of O3, the daily average level of O3 was 60.1 μg/m3, of which the highest level was up to 200.8 μg/m3. When stratified by season, the daily average level of O3 in the warm and seasons was 74.4 and 45.5 μg/m3, respectively. The daily average level of the temperature, pressure, wind speed, and relative humidity was 16.8 °C, 101.3 kPa, 2.0 m/s, and 75.7%, respectively, in the study period (Table 1). The daily average level of PM2.5 appeared as a sinusoidal distribution curve, with the levels in cold seasons higher than in warm seasons, while the daily average level of O3 was higher in warm seasons than in cold seasons (Fig. 2).

Daily average levels of PM2.5 and O3 in Hefei, China, between January 1, 2013, and December 31, 2015
The number of all-cause death (ICD10: A00-R99) in Hefei between January 1, 2013, and December 31, 2015, was 28,999, among which 12,262 (42.28%) were cardiovascular deaths (I00-I99). The number of daily average cardiovascular death was 11.20 (SD 3.88). Among the cardiovascular deaths, 6615 (53.95%) were males, and the daily average death was 6.04 (SD 2.68); 5647 (46.05%) were females, and the daily average death was 5.16 (SD 2.44). In addition, 69.06% (n = 8468) of the deaths were ≥ 75 years old, with the daily average death of 7.73 (SD: 3.17), while 30.94% (n = 3794) of the deaths were < 75 years old, with the daily average death of 3.46 (SD 1.94) (Table 1).The five major types of the diseases were cerebral infarction (I61.9), coronary heart disease (CHD: I25.1), intracerebral hemorrhage (I63.9), acute myocardial infarction (AMI: I21-22), and hypertensive heart disease (HHD;I11.9), with the average daily death of 2.24, 1.95, 1.81, 1.64, and 0.66, respectively (Table 2).
Associations between the air pollutants and meteorological factors
The associations between the air pollutants and meteorological factors during the study period were assessed by Spearman correlation, and the results are shown in Table 3. There were significant correlations between any two factors (P < 0.05). The strongest correlation was found between daily average temperature and O3 (r = 0.508, P < 0.01).
Associations between air pollutants and cardiovascular mortality in single-pollutant model
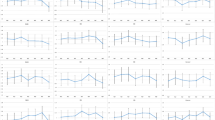
Figure 3 shows the exposure-response relationships between air pollutants and cardiovascular mortality outcomes. An almost linear relationship between air pollutants (including PM2.5 and O3) and cardiovascular mortality was observed for most air pollutant levels in this study (chi-square test for linearity, P > 0.05).

Smoothing plots of air pollutants against mortality risk (df = 3). X-axis is air pollutants concentrations (μg/m3) on Lag0. The estimated mean percentage of change in daily mortality is shown by the solid line, and the dotted lines represent twice the point-wise standard error. Air pressure (Lag0) was used, and the df of air pressure was 3
Table 4 shows the ERs and corresponding CIs of cardiovascular mortality with every 10 μg/m3 increase of PM2.5 or O3 concentration in single-pollutant model. The findings show that although exposure to PM2.5 and O3 tended to increase the risk of cardiovascular death, the associations were not statistically significant (Table 4). However, when stratified by seasons, the results showed that with every 10 μg/m3 increase of O3 in the warm season, the risk of cardiovascular death increased by 1.29% (95% CI 0.26%, 2.33%) and 1.17% (95% CI 0.20%, 2.14%) on Lag0 and Lag2, respectively. The moving average values also showed that O3 exposure could increase the cardiovascular mortality by 1.16–1.37%. However, no significant associations of PM2.5 on cardiovascular mortality were found in the warm season. In contrast, the results in the cold season showed that every 10 μg/m3 increase of PM2.5 could result in 0.22% increase of cardiovascular on Lag0 by 0.22% (95% CI 0.05%, 0.39%), although no significant cumulative associations were found as shown by the moving average values. However, similar to the results in the warm season, the increase of O3 significantly increased the risk of cardiovascular mortality on Lag2, as well as the moving average associations of Lags01–04 (Table 4).
We further stratified the subjects by gender. The results showed no statistically significant associations of PM2.5 and O3 exposure with cardiovascular death in males. To our surprise, however, the associations between PM2.5 exposure and the cardiovascular mortality in females were all statistically significant, regardless of the lag days. The association on the exposure day (Lag0) was the strongest 1.11% (95% CI 0.56%, 1.66%), which attenuated gradually with the increase of the lag days. In addition, the association tended to accumulate, as shown in the moving average results. No statistically significant associations of O3 exposure on cardiovascular mortality in females were found (Table 5).
In addition, the associations of PM2.5 exposure on Lag0 were evidently stronger in the subjects younger than 75 years old than the ones ≥ 75 years (ER 0.67% vs. 0.26%), although the results were statistically insignificant. Similarly, no significant associations of O3 exposure on cardiovascular mortality were found in either age group (Table 6).
Associations of air pollutants with cardiovascular mortality in two-pollutant model
The associations of PM2.5 and O3 exposure with cardiovascular mortality in the subjects declined a little in the two-pollutant model, comparing with the single-pollutant model. When O3 was introduced, the ER of PM2.5 on cardiovascular on Lag0 decreased from 0.37% (95% CI − 0.06%, 0.79%) to 0.33% (95% CI − 0.10%, 0.76%); while when PM2.5 was introduced, the ER of O3 on cardiovascular mortality on Lag0 decreased from 0.68% (95% CI − 0.12%, 1.49%) to 0.61% (95% CI − 0.20%, 1.42%) (Table 7).
Discussion
This study investigated the association between air pollutants (PM2.5 and O3) exposure and cardiovascular mortality risk in Hefei, China, between January 1, 2013, and December 31, 2015. The results of this time-series analysis suggested that the acute effects of O3 exposure could significantly increase the risk of cardiovascular mortality in warm seasons, while PM2.5 mainly increase the risk in cold seasons. To our knowledge, this is the first study that investigated the associations of PM2.5 and O3 with cardiovascular mortality in Hefei.
Studies have pointed out that when pollutant level increase to a certain degree, it could result in a “harvesting effect” in sensitive subjects, and therefore accelerate the death of such people (Costa et al. 2017). Accordingly, accumulating evidence has shown that PM2.5 and O3 exposure could result in detrimental effects on human health. For instance, a previous time-series study in 75 cities in the USA found that in every 10 μg/m3 increase of PM2.5 level, the risk of cardiovascular mortality increase by 1.03% (95% CI 0.65%, 1.41%) (Dai et al. 2014). On the contrary, however, studies in China showed that although the daily average level of PM2.5 was very high, the associations with daily mortality were almost negligible (Lee et al. 2015). In agreement with these studies in China, the overall associations of PM2.5 and O3 exposure with cardiovascular mortality in Hefei residents were also not statistically significant. This could be the result of a very interesting fact, that when the level of pollutant reach a very high degree, the exposure-effect curve will shift to plateau stage, in which stage the slope of the curve is very low, thus mask the effects of the pollutants on health. The findings of the present study showed that air pollution in Hefei was very heavy during the study period, with the highest PM2.5 level of 373 μg/m3, and the highest O3 level of 200.80 μg/m3. Although the exact exposure-effect curve in Hefei was not estimated, we can still speculate that such high levels of PM2.5 and O3 could be in the plateau stage of the curve. Therefore, the associations between the exposures and cardiovascular mortality are seemingly to be not so pronounced. In addition, several studies have also shown that the components of particulate matters in China are different from those in western countries (Aguilera et al. 2016; Alam et al. 2012; Thurston et al. 2016). For instance, a great proportion of the particulate matters in China are from the transported dust from desert and arid loess-land, as well as locally induced dust due to intensive urban construction (Chen et al. 2017; Lee et al. 2014). Therefore, such particulate matters contain high content of crustal materials, of which the toxicity is relatively lower than the particulate matters from fossil combustion.
When we stratified the analyses by seasons to warm and cold seasons, the results showed that every 10 μg/m3 increase of PM2.5 could increase the cardiovascular mortality by 0.22% (95% CI 0.05%, 0.39%) in cold season on Lag0; however, the associations in warm season were still statistically insignificant. We speculate that these effects could, at least partially, resulted from the changes of the components of particulate matters in cold season, in which time period more fuels were consumed, which could add some highly toxic components, such as benzopyrene (BaP) and heavy metals, to particulate matters. In addition, wood burning was identified as the dominant source of fine particles in the winter (Rodopoulou et al. 2015). Interestingly, stratified analyses by gender in this study also showed that PM2.5 exposure can significantly increase cardiovascular mortality in females. This is in agreement with several previous studies (Chen et al. 2017; Qin et al. 2017), which have demonstrated that the adverse associations of PM2.5 are stronger in females than in their male counterparts. This gender difference regarding the associations of PM2.5 exposure could be attributed to the variations in physiological features, lifestyles, and chances of specific exposures between males and females (Bell et al. 2013).
A growing body of evidence has demonstrated that the associations of O3 with daily cardiovascular mortality are higher than on daily all-cause mortality (Peng et al. 2013). In addition, O3 exposure could also lead to significant changes of certain biomarkers in the circulation, which could be reflected by the changes in inflammatory factors, oxidative stress, coagulation, vascular activity, and glucose metabolism. Furthermore, O3 could activate neural reflex, affect cardiac rhythm, and influence the automatic regulation of blood vessels (Bero Bedada et al. 2016; Goodman et al. 2015). However, findings of the present study showed that although O3 exposure tended to increase the annual cardiovascular mortality, the associations were statistically insignificant. These findings were in agreement with several previous studies, such as the time-series studies conducted in Arkansas, USA, and in Montreal, Canada (Goldberg et al. 2013; Rodopoulou et al. 2015). Interestingly, when we stratified the analyses by seasons to warm and cold seasons, the associations of O3 exposure with cardiovascular mortality appeared to be more pronounced. For instance, the exposure can increase the cardiovascular mortality by 1.29% and 1.17% on Lag0 and Lag2 in warm season, respectively. Similarly, the cumulative associations, as shown in the moving average values, also showed that O3 exposure in warm season can increase cardiovascular mortality. In summer, residents of Hefei spend more time outdoors and windows are commonly open, which could potentially increase their exposure. However, interestingly, the results showed that O3 exposure in cold season tended to reduce cardiovascular mortality. We speculated that during cold seasons, the prominent pollution was particulate matters, while the weakened ultraviolet could only lead to limited levels of O3 (45.52 μg/m3 in cold season, comparing with 74.35 μg/m3 in warm season), which could result in protective effects on cardiovascular mortality. Similar to the findings in PM2.5, stratified analysis also showed that the associations of O3 were more pronounced in females than in males, although the results were statistically insignificant, which were in agreement with several previous studies (Mercedes and Joel 2008; Stafoggia et al. 2010).
The two-pollutant models in this study showed that when PM2.5 or O3 was introduced, the associations of PM2.5 or O3 with cardiovascular mortality were slightly, but not statistically significantly changed, which were in agreement with a previous time series in Hong Kong (Lin et al. 2017). We speculated that the findings that ER decreased slightly when the second pollutant was included were partially caused by the fact that O3 and PM2.5 were negatively correlated. As shown in Fig. 2, PM2.5 level peaked in winter, while O3 level peaked in summer; therefore, it is possible that the combined associations between O3 and PM2.5 could be masked. In contrast, an experimental study showed that when ultra-fine particulate matters and O3 were co-applied, the cardiovascular diseases and pulmonary injuries in mice could be aggravated, and the additional application of O3 to mice did increase the toxic effects of ultra-fine particulate matters (Wong et al. 2018).
This study is limited by the following factors: first of all, the air pollution level was estimated by the average level of Hefei, which could not loyally reflect the exposure of each individual; therefore, ecological fallacy could affect the results; second, only two major pollutants were investigated in this study, while the other factors could also affect the adverse associations of PM2.5 and O3; and other factors such as characteristics of certain groups of people could also affect the results; and third, there is only 3 years of air pollutant data for the analysis in this study. However, despite these drawbacks, the findings of this study showed that PM2.5 and O3 exposure could increase the risk of cardiovascular mortality, especially in females and in cold season. More studies are needed to verify our findings and investigate the underlying mechanisms.
References
Aguilera I, Dratva J, Caviezel S, Burdet L, de Groot E, Ducret-Stich RE, Eeftens M, Keidel D, Meier R, Perez L, Rothe T, Schaffner E, Schmit-Trucksäss A, Tsai MY, Schindler C, Künzli N, Probst-Hensch N (2016) Particulate matter and subclinical atherosclerosis: associations between different particle sizes and sources with carotid intima-media thickness in the SAPALDIA study. Environ Health Perspect 124:1700–1706. https://doi.org/10.1289/EHP161
Alam DS, Chowdhury MAH, Siddiquee AT, Ahmed S, Hossain MD, Pervin S, Streatfield K, Cravioto A, Niessen LW (2012) Adult cardiopulmonary mortality and indoor air pollution: a 10-year retrospective cohort study in a low-income rural setting. Glob Heart 7:215–221. https://doi.org/10.1016/j.gheart.2012.06.008
Bai L, Su X, Zhao D, Zhang Y, Cheng Q, Zhang H, Wang S, Xie M, Su H (2018) Exposure to traffic-related air pollution and acute bronchitis in children: season and age as modifiers. J Epidemiol Community Health 72:426–433. https://doi.org/10.1136/jech-2017-209948
Beelen R, Stafoggia M, Raaschou-Nielsen O, Andersen ZJ, Xun WW, Katsouyanni K, Dimakopoulou K, Brunekreef B, Weinmayr G, Hoffmann B, Wolf K, Samoli E, Houthuijs D, Nieuwenhuijsen M, Oudin A, Forsberg B, Olsson D, Salomaa V, Lanki T, Yli-Tuomi T, Oftedal B, Aamodt G, Nafstad P, de Faire U, Pedersen NL, Östenson CG, Fratiglioni L, Penell J, Korek M, Pyko A, Eriksen KT, Tjønneland A, Becker T, Eeftens M, Bots M, Meliefste K, Wang M, Bueno-de-Mesquita B, Sugiri D, Krämer U, Heinrich J, de Hoogh K, Key T, Peters A, Cyrys J, Concin H, Nagel G, Ineichen A, Schaffner E, Probst-Hensch N, Dratva J, Ducret-Stich R, Vilier A, Clavel-Chapelon F, Stempfelet M, Grioni S, Krogh V, Tsai MY, Marcon A, Ricceri F, Sacerdote C, Galassi C, Migliore E, Ranzi A, Cesaroni G, Badaloni C, Forastiere F, Tamayo I, Amiano P, Dorronsoro M, Katsoulis M, Trichopoulou A, Vineis P, Hoek G (2014) Long-term exposure to air pollution and cardiovascular mortality: an analysis of 22 European cohorts. Epidemiology 25:368–378. https://doi.org/10.1097/EDE.0000000000000076
Bell ML, Zanobetti A, Dominici F (2013) Evidence on vulnerability and susceptibility to health risks associated with short-term exposure to particulate matter: a systematic review and meta-analysis. Am J Epidemiol 178:865–876. https://doi.org/10.1093/aje/kwt090
Bero Bedada G, Raza A, Forsberg B, Lind T, Ljungman P, Pershagen G, Bellander T (2016) Short-term exposure to ozone and mortality in subjects with and without previous cardiovascular disease. Epidemiology 27:663–669. https://doi.org/10.1097/EDE.0000000000000520
Chen R, Yin P, Meng X, Liu C, Wang L, Xu X, Ross JA, Tse LA, Zhao Z, Kan H, Zhou M (2017) Fine particulate air pollution and daily mortality. A nationwide analysis in 272 Chinese cities. Am J Respir Crit Care Med 196:73–81. https://doi.org/10.1164/rccm.201609-1862OC
Coogan PF, White LF, Yu J, Brook RD, Burnett RT, Marshall JD, Bethea TN, Rosenberg L, Jerrett M (2017) Long-term exposure to NO2 and ozone and hypertension incidence in the black women’s health study. Am J Hypertens 30:367–372. https://doi.org/10.1093/ajh/hpw168
Costa AF, Hoek G, Brunekreef B, Ponce de Leon AC (2017) Air pollution and deaths among elderly residents of Sao Paulo, Brazil: an analysis of mortality displacement. Environ Health Perspect 125:349–354. https://doi.org/10.1289/EHP98
Dai L, Zanobetti A, Koutrakis P, Schwartz JD (2014) Associations of fine particulate matter species with mortality in the United States: a multicity time-series analysis. Environ Health Perspect 122:837–842. https://doi.org/10.1289/ehp.1307568
Goldberg MS, Burnett RT, Stieb DM, Brophy JM, Daskalopoulou SS, Valois MF, Brook JR (2013) Associations between ambient air pollution and daily mortality among elderly persons in Montreal, Quebec. Sci Total Environ 463-464:931–942. https://doi.org/10.1016/j.scitotenv.2013.06.095
Goodman JE, Prueitt RL, Sax SN, Pizzurro DM, Lynch HN, Zu K, Venditti FJ (2015) Ozone exposure and systemic biomarkers: evaluation of evidence for adverse cardiovascular health impacts. Crit Rev Toxicol 45:412–452. https://doi.org/10.3109/10408444.2015.1031371
Kan H, London SJ, Chen G, Zhang Y, Song G, Zhao N, Jiang L, Chen B (2007) Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ Int 33:376–384. https://doi.org/10.1016/j.envint.2006.12.001
Lee H, Honda Y, Lim YH, Yue LG, Hashizume M, Kim H (2014) Effect of Asian dust storms on mortality in three Asian cities. Atmos Environ 89:309–317
Lee H, Honda Y, Hashizume M, Guo YL, Wu CF, Kan H, Jung K, Lim YH, Yi S, Kim H (2015) Short-term exposure to fine and coarse particles and mortality: a multicity time-series study in East Asia. Environ Pollut 207:43–51. https://doi.org/10.1016/j.envpol.2015.08.036
Li YR, Xiao CC, Li J, Tang J, Geng XY, Cui LJ, Zhai JX (2018) Association between air pollution and upper respiratory tract infection in hospital outpatients aged 0-14 years in Hefei, China: a time series study. Public Health 156:92–100. https://doi.org/10.1016/j.puhe.2017.12.006
Lin H, Liu T, Xiao J, Zeng W, Li X, Guo L, Zhang Y, Xu Y, Tao J, Xian H, Syberg KM, Qian Z(M), Ma W (2016a) Mortality burden of ambient fine particulate air pollution in six Chinese cities: results from the Pearl River Delta study. Environ Int 96:91–97. https://doi.org/10.1016/j.envint.2016.09.007
Lin H, Tao J, du Y, Liu T, Qian Z, Tian L, di Q, Rutherford S, Guo L, Zeng W, Xiao J, Li X, He Z, Xu Y, Ma W (2016b) Particle size and chemical constituents of ambient particulate pollution associated with cardiovascular mortality in Guangzhou,China. Environ Pollut 208:758–766. https://doi.org/10.1016/j.envpol.2015.10.056
Lin H, Ma W, Qiu H, Wang X, Trevathan E, Yao Z, Dong GH, Vaughn MG, Qian Z, Tian L (2017) Using daily excessive concentration hours to explore the short-term mortality effects of ambient PM2.5 in Hong Kong. Environ Pollut 229:896–901. https://doi.org/10.1016/j.envpol.2017.07.060
Mercedes MR, Joel S (2008) Who is more vulnerable to die from ozone air pollution? Epidemiology 19:672–679
Peng RD, Samoli E, Pham L, Dominici F, Touloumi G, Ramsay T, Burnett RT, Krewski D, le Tertre A, Cohen A, Atkinson RW, Anderson HR, Katsouyanni K, Samet JM (2013) Acute effects of ambient ozone on mortality in Europe and North America: results from the APHENA study. Air Qual Atmos Health 6:445–453. https://doi.org/10.1007/s11869-012-0180-9
Pope CA 3rd et al (2015) Relationships between fine particulate air pollution, cardiometabolic disorders, and cardiovascular mortality. Circ Res 116:108–115. https://doi.org/10.1161/CIRCRESAHA.116.305060
Qin RX, Xiao C, Zhu Y, Li J, Yang J, Gu S, Xia J, Su B, Liu Q, Woodward A (2017) The interactive effects between high temperature and air pollution on mortality: a time-series analysis in Hefei, China. Sci Total Environ 575:1530–1537. https://doi.org/10.1016/j.scitotenv.2016.10.033
Raza A, Dahlquist M, Lind T, Ljungman PLS (2018) Susceptibility to short-term ozone exposure and cardiovascular and respiratory mortality by previous hospitalizations. Environ Health: a global access science source 17:37. https://doi.org/10.1186/s12940-018-0384-z
Rodopoulou S, Chalbot MC, Samoli E, Dubois DW, San Filippo BD, Kavouras IG (2014) Air pollution and hospital emergency room and admissions for cardiovascular and respiratory diseases in Dona Ana County, New Mexico. Environ Res 129:39–46. https://doi.org/10.1016/j.envres.2013.12.006
Rodopoulou S, Samoli E, Chalbot MG, Kavouras IG (2015) Air pollution and cardiovascular and respiratory emergency visits in Central Arkansas: a time-series analysis. Sci Total Environ 536:872–879. https://doi.org/10.1016/j.scitotenv.2015.06.056
Stafoggia M, Forastiere F, Faustini A, Biggeri A, Bisanti L, Cadum E, Cernigliaro A, Mallone S, Pandolfi P, Serinelli M, Tessari R, Vigotti MA, Perucci CA (2010) Susceptibility factors to ozone-related mortality: a population-based case-crossover analysis. Am J Respir Crit Care Med 182:376–384. https://doi.org/10.1164/rccm.200908-1269OC
Thurston GD, Burnett RT, Turner MC, Shi Y, Krewski D, Lall R, Ito K, Jerrett M, Gapstur SM, Diver WR, Pope CA III (2016) Ischemic heart disease mortality and long-term exposure to source-related components of U.S. fine particle air pollution. Environ Health Perspect 124:785–794. https://doi.org/10.1289/ehp.1509777
Tian L, Qiu H, Pun VC, Lin H, Ge E, Chan JC, Louie PK, Ho KF, Yu ITS (2013) Ambient carbon monoxide associated with reduced risk of hospital admissions for respiratory tract infections. Am J Respir Crit Care Med 188:1240–1245. https://doi.org/10.1164/rccm.201304-0676OC
Tsai JH, Chang LP, Chiang HL (2014) Airborne pollutant characteristics in an urban, industrial and agricultural complex metroplex with high emission loading and ammonia concentration. Science Total Environ 494-495:74–83. https://doi.org/10.1016/j.scitotenv.2014.06.120
Tsangari H, Paschalidou AK, Kassomenos AP, Vardoulakis S, Heaviside C, Georgiou KE, Yamasaki EN (2016) Extreme weather and air pollution effects on cardiovascular and respiratory hospital admissions in Cyprus. Sci Total Environ 542:247–253. https://doi.org/10.1016/j.scitotenv.2015.10.106
Wong EM, Walby WF, Wilson DW, Tablin F, Schelegle ES (2018) Ultrafine particulate matter combined with ozone exacerbates lung injury in mature adult rats with cardiovascular disease. Toxicol Sci 163:140–151. https://doi.org/10.1093/toxsci/kfy018
Yang F et al (2011) Characteristics of PM2.5 speciation in representative megacities and across China. Atmos Chem Phys 11:1025–1051
Yin P, Chen R, Wang L, Meng X, Liu C, Niu Y, Lin Z, Liu Y, Liu J, Qi J, You J, Zhou M, Kan H (2017) Ambient ozone pollution and daily mortality: a nationwide study in 272 Chinese cities. Environ Health Perspect 125:117006. https://doi.org/10.1289/EHP1849
Zhang C, Ding R, Xiao C, Xu Y, Cheng H, Zhu F, Lei R, di D, Zhao Q, Cao J (2017) Association between air pollution and cardiovascular mortality in Hefei, China: a time-series analysis. Environ Pollut 229:790–797. https://doi.org/10.1016/j.envpol.2017.06.022
Acknowledgments
The authors wish to thank all the staff members at the Hefei Centre for Disease Control and Prevention of Anhui for their strong support of this study.
Funding
This work was supported by the Natural Science Foundation of Anhui Province (no. 1708085MH220), the Project Foundation for the Young Talents in Colleges of Anhui Province (no. gxyq2017003), and the Grant for Scientific Research of BSKY from Anhui Medical University (no. XJ201621).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
First author: Han Cheng
Rights and permissions
About this article

Cite this article
Cheng, H., Zhu, F., Lei, R. et al. Associations of ambient PM2.5 and O3 with cardiovascular mortality: a time-series study in Hefei, China. Int J Biometeorol 63, 1437–1447 (2019). https://doi.org/10.1007/s00484-019-01766-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-019-01766-2