
Abstract
Parkinson’s disease (PD) patients show cognitive deficits that are relevant in terms of prognosis and quality of life. Degeneration of striatal dopaminergic afferents proceeds from dorsal/caudal to anterior/ventral and is discussed to account for some of these symptoms. Treatment with dopamine (DA) has differential effects on cognitive dysfunctions, improving some and worsening others. We hypothesized that cognitive performance during the dopaminergic OFF state correlates with DAT availability in the associative striatum. 16 PD patients underwent motor and cognitive examination ON and OFF DA. Global cognition was measured using the Montréal Cognitive Assessment (MoCA) test and executive functioning using a Stroop test. Nigrostriatal dopaminergic innervation was characterized with [123I]FP-CIT SPECT. A connectivity atlas of the striatum was used to assess DAT availability in functionally defined striatal subregions. Correlations between imaging data and behavioral data OFF medication were calculated. Correlations between DAT availability and MoCA performance in the dopaminergic OFF state was strongest in the associative part of the striatum (r = 0.674, p = 0.004). MoCA test performance did not differ between the ON and the OFF state. There was no correlation of DAT availability with Stroop performance in the OFF state but performance was significantly better during the ON state. Not only motor but also cognitive dysfunctions in PD are associated with striatal dopaminergic depletion. Cognitive decline in non-demented PD patients goes along with nigrostriatal degeneration, most pronounced in the associative subdivision of the striatum. In addition, the present findings suggest that executive dysfunctions are ameliorated by DA whereas global cognition is not improved by dopaminergic medication.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The pathological hallmark of PD consists in the loss of dopaminergic neurons of the substantia nigra pars compacta (SNc) and the consecutive dopamine depletion in the striatum (Kish et al. 1988). Apart from the extensively studied motor domains of the basal ganglia, increasing attention has been devoted to the cognitive and neuropsychiatric symptoms resulting from dopaminergic depletion as parallel frontostriatal circuits are also involved in cognitive and emotional processing (Alexander et al. 1986). Previous studies in PD patients have produced heterogeneous results about the effect of DA on cognition (Robbins and Cools 2014). On the one hand, DA leads to an improvement of the dysexecutive syndrome in non-demented PD patients (Cools et al. 2003; Costa et al. 2014) and improves executive task performance for example in the Stroop task (Fera et al. 2007). On the other hand, DA impairs domains like reversal learning, especially when feedback is negative (Cools et al. 2006) and increases impulsivity (Cools et al. 2003).
Functional imaging and clinical pathology studies suggest that cognitive and motor deficits relate to different patterns of degeneration of striatal dopamine afferents across the functional striatal subdivisions as PD progresses. The ventral part of the SNc projects primarily to the posterior/dorsal striatum and the dorsal part of the SNc sends its projections to the more anterior/ventral striatal parts (Vaillancourt et al. 2013). The pattern of degeneration within the SNc during the progression of PD proceeds from ventral to dorsal and is different from normal aging (Brück et al. 2006; Kaasinen and Rinne 2002). This gradient seems to be maintained during the course of the disease. Based on this observation it is hypothesized that motor and cognitive symptoms that predominantly rely on the primarily affected dorsal striatum are ameliorated by DA whereas those cognitive functions that are mediated by the relatively intact ventral striatum are worsened by dopamine according to the so-called overdose theory (Aarts et al. 2014; MacDonald et al. 2013). In line with this, Costa and colleagues showed that only PD patients with low cognitive performance significantly improved their mental flexibility performance under DA. In contrast, patients who performed well without DA got worse under dopaminergic medication (Costa et al. 2013).
However, it is not clear to date if the degree of dopaminergic loss in the striatum relates to a global cognitive decline in PD. Several studies that have investigated early stage non-medicated PD patients with [123I]FP-CIT SPECT suggest that impaired cognitive performance goes along with striatal degeneration (Pellecchia et al. 2015; Polito et al. 2012). Similar, DA neuron integrity of the caudate nucleus (CN) revealed by PET was reduced in PD patients with Montréal Cognitive Assessment (MoCA) scores below 26 in comparison to those with normal MoCA scores (Chou et al. 2014). The observed lack of correlations between cognitive function and dopaminergic imaging in PD patients with normal MoCA scores was attributed to the very homogenous study population with little variance regarding cognitive function and disease duration. These findings suggest a relationship between overall cognitive functioning as measured by the MoCA test and striatal integrity and motivated us to use this test in a more heterogenous cohort.
Executive functions also have been discussed in the light of dopaminergic degeneration. Here, a positive but small correlation between striatal DAT availability and executive function has been found in a large cohort of early drug-näive PD patients (Siepel et al. 2014) and in the dopaminergic ON state (Rektorova et al. 2008). More specifically, reduced tracer uptake in the (right) CN correlated negatively with Stoop performance in two [18F]Fluorodopa PET studies (Brück et al. 2006; Rinne et al. 2000) which is in line with improvement of Stroop performance under DA in several studies (Fera et al. 2007; Costa et al. 2013).
Taking these considerations together, cognitive performance in non-demented PD patients seems dependent on task requirements, on the degree of dopamine loss and its relative replacement at the time of the study. However, all above-mentioned studies analysed DA uptake in the entire striatum not taking into consideration the functional subareas or only made an anatomical dissociation between the CN and the putamen (see Pellecchia et al. 2015; Polito et al. 2012; Chou et al. 2014). As the course of striatal degeneration in PD follows a dorsal/caudal to anterior/ventral gradient, we applied a functional striatal atlas based on the work of Tziortzi and colleagues (2014) that allowed us to segment the striatum in its three main parts that were labeled according to their cortical connections: the sensorimotor, associative and limbic subdivision.
In order to investigate the effects of functionally distinct striatal dopamine depletion on cognitive performance, we asked 16 non-demented PD patients in different stages of the disease to perform two well characterized cognitive tasks for global cognition (MoCA test) and executive functions (Stroop test) ON and OFF DA and correlated task performance with individual patterns of striatal dopaminergic degeneration. We hypothesized that cognitive performance during the dopaminergic OFF state correlates with DAT availability, especially in the associative striatum.
Methods
Patients
16 patients (8 women and 8 men) with idiopathic PD participated in this study after having given their written informed consent. Study procedures were approved by the ethics committee of the Charité-Universitätsmedizin Berlin and the German Federal Office for Radiation Protection. Patients were recruited from the clinics of neurology and nuclear medicine. The diagnosis of idiopathic PD was given according to the United Kingdom Parkinson’s Disease Society Brain Bank Clinical Diagnostic Criteria (Hughes et al. 1992). Table 1 shows the demographic and clinical characteristics of our cohort, which entail a wide range of age, disease duration and severity of motor symptoms covering a broad clinical spectrum of PD. Nine patients showed an akinetic-rigid, two patients a tremor dominant and five an equivalent type of PD.
Clinical assessment
The UPDRS motor part III was performed to evaluate the motor deficit ON and OFF medication in all patients. On medication we used the second version of the Beck Depression Inventory (Hautzinger 1991), a self-reported questionnaire to evaluate the intensity of depressive symptoms; the self-reported questionnaire SF-36 [Short Form 36 Health Survey Questionnaire (Bullinger 1995)] to assess health-related quality of life and the Barratt Impulsiveness Scale [BIS-11 (Hartmann et al. 2011)] that is widely used and validated to investigate self-reported impulsiveness. For assessment of global cognitive function, we used the Montréal Cognitive Assessment (MoCA) and the Stroop test for executive function (paradigm according to JR Stroop 1935) ON and OFF medication.
The MoCA test measures global cognition and represents a valid screening instrument for mild cognitive impairment in PD (Dalrymple-Alford et al. 2010). It evaluates different cognitive domains including attention, concentration, executive functions, memory, language, visuoconstructive skills, conceptual thinking, calculations and orientation without major motor speed effects which is important when investigating cognition in PD. The test consists of 11 categories with a maximum score of 30 points. One point is added for participants who received only 12 years or less of formal education. A score of 26 or more is considered normal. Screening cutoffs for mild cognitive impairment (PD-MCI) and dementia (PD-D) are <26/30 and <21/30, respectively. Different German versions of the full MoCA test were used for evaluation in ON and OFF state in a randomized order.
The Stroop test was applied in order to assess attention, selective inhibition and working memory. It consists of two subtests: color naming (subjects are asked to name the color of differently colored rectangles) and the interference task (subjects have to name the color of color-words which are written in differently colored font and therefore have to suppress the automatic process of reading and instead have to consciously name the color the word is written in). Time needed for the subtasks and the number of errors in the interference task were counted. The difference of processing time between the interference task and the color naming task was calculated as a measure of pure executive functioning minus motor speed (nomination and reading speed) so there is no interference by motor speed.
Patients were withdrawn from their dopaminergic medication for a minimum of two halftimes of their specific medication but at least 12 h for the OFF medication session. Assessment ON medication was performed about 1 h after intake of their usual dopaminergic medication of at least 200 mg levodopa. We excluded one patient as she did not show motor improvement of 30% in the UPDRS III score ON versus OFF dopaminergic medication indicating no clear ON and/or OFF state at the time of study participation. The temporal sequence of ON and OFF study sessions was randomized in order to rule out learning effects.
[123I]FP-CIT SPECT: image acquisition and data analysis
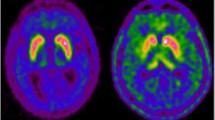
[123I]FP-CIT SPECT to measure DAT availability in the striatum was performed according to common guidelines (Darcourt et al. 2010). Patients avoided taking medications or drugs of abuse known to significantly interfere with DAT imaging (Booij and Kemp 2007). Antiparkinsonian medication was not withdrawn for DAT imaging. SPECT acquisition was performed with a dual head SPECT camera, either a Symbia S (Siemens Healthcare, Hoffman Estates, USA) or a Millenium VG-Hawkeye (GE Healthcare, Haifa, Israel), equipped with low-energy, high-resolution, parallel-hole collimators. The acquisition started between 3 and 4 h after intravenous injection of about 180 MBq FP-CIT following blocking of the thyroid gland by oral administration of perchlorate. A 128 × 128 matrix was used and an energy window of 20% centered at the photopeak of I-123 at 159 keV. Three-dimensional SPECT images were reconstructed by filtered back-projection with a Butterworth filter (harmonized between the two SPECT cameras). Post reconstruction uniform attenuation correction was performed using Chang’s method with linear attenuation coefficient µ = 0.11/cm. No scatter correction was applied.
Quantitative analysis of FP-CIT uptake was performed using a fully automated processing pipeline based on the statistical parametric mapping (SPM) software package (version SPM8). First, the patient’s FP-CIT SPECT image was stereotactically normalized into the anatomical space of the Montreal Neurological Institute (MNI) using SPM’s normalize tool and a custom-made FP-CIT template (Lange et al. 2014). Stereotactical normalization included both affine transformation and warping. Mean FP-CIT uptake was determined separately in the unilateral limbic, associative and sensorimotor part of the striatum using regions of interest (ROI) provided by the Oxford-GSK-Imanova Striatal Connectivity Atlas with three subregions (and 50% threshold) based on cortico-striatal anatomical connections (Tziortzi et al. 2014). For this atlas, striatal voxels have previously been labeled in a sample of 26 healthy individuals corresponding to the cortical region showing the highest probability of connection using diffusion weighted MRI data and probabilistic tractography (Behrens et al. 2003). The striatal subregions (corresponding cortical regions of interests in brackets) are from dorsal/caudal to anterior/ventral: sensorimotor (area 4 and 6, supplementary motor area, pre-SMA and frontal eye field), “executive” (rostral superior and middle frontal gyri, dorsal prefrontal cortex) and limbic subregion (orbital gyrus, gyrus rectus, subcallosal gyrus, ventral anterior cingulate and area 25). The striatal subregion labeled “executive” in this atlas has wide connections to cortical areas (see above) that are not only involved in executive functions but in a wide range of cognitive domains. We therefore denote it as “associative” subdivision of the striatum in this paper. The volume of the striatal subregions is 2.65/2.26 ml for left/right sensorimotor part, 5.87/5.71 ml for left/right associative part, and 2.89/2.73 ml for left/right limbic part of the striatum. Whole brain without striata, thalamus and brainstem was used as reference region for the quantitative analysis of striatal FP-CIT uptake (Buchert et al. 2016; Kupitz et al. 2014). The FP-CIT binding ratio (BR) in a ROI was computed as BR = mean FP-CIT uptake in ROI/mean FP-CIT uptake in reference region. The BR is a measure of the concentration of available DAT in the ROI. The BR of the whole striatum was obtained as the volume weighted average of limbic, associative and sensorimotor BR. As cognition is not as much lateralized as motoric deficits, bilateral BR values were obtained by volume weighted averaging over left and right hemisphere.
Statistical analyses
The Kolmorogov-Smirnov test was used to test for normal distribution. Mean values were compared using paired Student’s t tests or Wilcoxon signed rank tests where applicable. Correlation between two variables was tested by Pearson’s method or Spearman’s rho method depending or whether normal distribution could be assumed or not. Correlation analysis for DAT binding in subregions of the striatum was performed for the respective motor or cognitive tasks. Partial correlation analysis was used to correct correlations for confounding effects of disease duration. Two-sided p values ≤0.05 were considered significant. Correlation between striatal DAT uptake and MoCA scores during OFF have been corrected for disease duration, BDI-II and UPDRS III (during OFF).
Hochberg correction for multiple comparisons was ensured using pplot (Turkheimer et al. 2001). Statistical analyses were performed with IBM SPSS Statistics version 23 (SPSS Inc., Chicago).
Results
Self-reported questionnaires
Table 2 lists the results of the BDI-II, the SF-36 and the BIS-11. Questionnaires were filled in the ON state. Two of the participants had BDI-II scores of 15 and 16, respectively, and therefore fulfilled the screening criteria of minor depressive symptoms (>14). In the SF-36, the item General Health was rated most impaired by participants with a mean of 52.7 and a wide range between 25 and 92 reflecting a poor self-rated overall health state. Limitations due to Emotional Problems (87.5 ± 26.9) and Social Functioning (87.5 ± 16.5) were rated least impaired. BIS-11 scores of 1.90 in average and similar values in the three subscores indicated normal traits of impulsivity in our sample of PD patients.
Cognitive tests performed during the ON and OFF state
MoCA scores in the ON condition showed a mean of 27.6 (±1.8) and ranged from 24 to 30. MoCA scores in the OFF condition ranged from 23 to 30 and were 27.5 (±2.0) on average. During ON, three patients with MoCA scores of 24 and 25 fulfilled the criteria of PD-MCI. During OFF, two patients scored below 26 with scores of 25 and 23. None of the patients was demented, neither clinically (as no limitations in activities of daily living due to cognitive decline were reported) nor according to the MoCA score. The MoCA score did not differ between ON and OFF state (paired t test, p = 0.842, see Fig. 1a) and there was no difference in MoCA scores with respect to the order of ON and OFF medication states.

a MoCA scores during dopaminergic ON and OFF. b Stroop performance (time difference between the color naming and the interference condition in seconds) during dopaminergic ON and OFF
In the Stroop test patients showed significantly longer reaction times OFF medication as compared to ON medication. Specifically, for the completion of the interference condition, patients needed 35.1 s (±9.2 s) in the ON and 40.0 s (±12.5 s) in the OFF state (paired t test, p = 0.006). The Stroop effect, i.e. the time difference between color naming and the interference condition was 14.4 s (±7.0 s) in the ON and 19.7 s (±11.3 s) in the OFF condition. This difference was statistically highly significant (paired t test, p = 0.008, see Fig. 1b) although there was no difference in committed errors.
[123I]FP-CIT SPECT
The FP-CIT BR in the whole striatum was significantly decreased in the hemisphere contralateral to the clinically more affected body side in all patients in line with the diagnosis of PD and ranged between 1.58 and 2.44 (mean ± standard deviation of the sample = 2.04 ± 0.25). FP-CIT BR in the striatal subregions ranged between 1.32 and 1.93 (1.65 ± 0.18) in the sensorimotor part, between 1.71 and 2.61 (2.18 ± 0.27) in the associative part and between 1.47 and 2.53 (2.10 ± 0.29) for the limbic striatal part reflecting the gradient from dorsal/caudal to anterior/ventral. The relative variance in the sample was similar in all striatal subregions (coefficient of variance = standard deviation/mean = 10.9, 12.4 and 13.8% in sensorimotor, associative and limbic striatal subregion).
Correlations between motor and cognitive scores and [123I]FP-CIT SPECT
UPDRS III during OFF was negatively correlated with DAT availability in the whole striatum (Pearson correlation: r = −0.519, p = 0.039). Correlation between UPDRS III in the OFF state and DAT availability in the sensorimotor part of the striatum did not reach the level of statistical significance (r = −0.424, p = 0.102). However, duration of PD symptoms correlated negatively with sensorimotor (Spearman correlation: r = −0.500, p = 0.049) DAT binding. After correction for disease duration, the correlation between the UPDRS III and striatal degeneration did not reach significance anymore (r = 0.442, p = 0.099). Age did not show significant correlations with disease duration or symptom severity as measured by the UPDRS III during OFF also after correction for disease duration.
With respect to cognitive task performance, the better patients performed in the MoCA test during the OFF condition, the more striatal DAT binding was seen overall (Pearson correlation: r = 0.659, p = 0.005) and in the associative striatal subregion (associative r = 0.674, p = 0.004). These correlations between MoCA scores and striatal degeneration became even more pronounced when corrected for disease duration (striatum r = 0.693, p = 0.004; associative r = 0.690, p = 0.004). This correlation was similar when corrected for BDI-II and UPDRS III (during OFF) leading to a correlation for the overall striatum of r = 0.612, p = 0.020 and for the associative striatum r = 0.640, p = 0.014.
In the Stroop test, the time difference between the interference and the color naming condition indicating executive functioning per se did not show correlations with striatal DAT.
After Hochberg correction for multiple comparisons for all correlations between behavioural measures and DAT availability on an α-level of 0.05, only the correlations between MoCA scores and overall striatal DAT and that in the associative part of the striatum stayed significant (see Fig. 2). These correlations were not significant for the motor and limbic subregion of the striatum.

a Correlation of overall striatal DAT binding and MoCA scores. After correction for disease duration the correlation coefficient is r = 0.693, p = 0.004. b Correlation of striatal DAT binding in the associative subdivision and MoCA scores. After correction for disease duration the correlation coefficient is r = 0.690, p = 0.004
Discussion
A link between striatal dopaminergic integrity and cognition in non-demented PD patients has been suggested but the role of the striatal subdivisions and the effects of dopaminergic medication have not been specified yet. As striatal degeneration follows a disease-specific temporospatial gradient, we used a functional striatal atlas to correlate DAT availability according to [123I]FP-CIT SPECT and overall cognitive performance as well as executive functioning in the dopaminergic OFF state. We confirm that global cognitive impairment shows a significant correlation with reduced striatal DAT availability. Importantly, this correlation was significant for the associative subdivision of the striatum underscoring the role of spatially distinct neurodegeneration for global cognitive function in PD.
DA depletion in striatal subregions is differentially correlated with cognitive decline
According to our hypothesis that the functional subdivisions of the striatum are relevant when looking at the striatal impact on cognitive performance, MoCA scores during OFF showed a negative relationship with DAT availability in the overall striatum as well as in the associative striatal subdivision which became more evident when controlling for disease duration. These results stress the importance of functional entities of the striatum with differing behavioral correlates and susceptibility for DA. The associative subdivision of the striatum in the con3 atlas has been labeled according to its cortical connections, namely to the rostral superior and middle frontal gyri as well as the dorsal prefrontal cortex. These cortical areas are connected to the striatum via segregated circuits (Alexander et al. 1986). Thereby, in an anatomical sense the correlations are plausible as the multifaceted MoCA test encompasses an array of different cognitive functions recruiting cortico-striatal circuitry. Our sample of PD patients was not demented but partly fulfilled the criteria of PD-MCI. This heterogeneity was a prerequisite for the correlations found between cognition and DAT availability. Previous studies have primarily looked at early untreated PD patients or subgroups of PD-MCI patients (Chou et al. 2014; Christopher et al. 2014; Pellecchia et al. 2015). Christopher and colleagues investigated PD-MCI patients with dual tracer PET applying [11C]Dihydrotetrabenazine and [11C]FLB 457 as marker of cortical D2 receptors and found significantly greater DA depletion in the region of interest of the associative striatal subdivision and reduced D2 receptor availability in the bilateral insula as compared to HC. The associative striatal subdivision is comparable to the associative subdivision of the con3 atlas. DA depletion was predictive of insular receptor loss thus demonstrating interrelated cortico-striatal circuitry.
More specific testing of executive function using the Stroop test did not reveal a correlation with striatal DAT decline in our patients. This is in contrast to the previously described relationship of striatal DAT decline and executive deficits (Siepel et al. 2014). Different PET and SPECT tracers have been applied in order to study correlations between executive functioning and striatal DA depletion in previous studies. Two of the studies that also used a Stroop test should be mentioned here: Rinne and colleagues found reduced [18F]Fluorodopa uptake in the striatum and the frontal cortex in PD patients as compared to age-matched HC that was not correlated with overall cognitive performance but the tracer uptake in the CN correlated negatively with performance in the Stroop test (Rinne et al. 2000). A similar result was found in another [18F]Fluorodopa PET study in de novo PD patients with no previous dopaminergic medication: Here, Brück and colleagues found a negative correlation between uptake in the right CN and slow processing in the Stroop test (Brück et al. 2001). Reasons that might explain the discrepancy between these and the present study include the difference in striatal subregions used (CN versus limbic, associative and sensorimotor part) and higher spatial resolution of PET compared to SPECT imaging. In other words we think that the very specific Stroop task is clearly dependent on the dopaminergic system but the spatial resolution of [123I]FP-CIT SPECT was not sensitive enough to detect effects that are limited to a small part of the ROI or not clearly localized to any of the three ROIs.
Effects of DA on global cognition and specific executive functioning
Global cognition did not change ON dopaminergic medication, possibly due to the fact that distinct mental abilities are tested here that have been shown to respond differentially to DA treatment. Interestingly, we observed that patients with advanced dopaminergic degeneration tend to improve in MoCA scores with DA whereas patients with a smaller loss of dopamine perform worse but this correlation (MoCA during ON minus MoCA during OFF and striatal DAT binding) did not reach significance (r = −0.376, p = 0.151). The Stroop test, however, requires a high load of cognitive flexibility and the interference condition is not influenced by additional learning effects or motor speed. We found a dopaminergic effect on Stroop performance when comparing the ON and OFF state. This is in line with other studies that have seen an improvement of the dysexecutive syndrome with DA in non-demented PD patients (Cools et al. 2003; Costa et al. 2014).
Study strengths and limitations
This study has to be interpreted considering its strengths as well as its limitations. To our knowledge, we are the first to look into specific striatal subregions of dopaminergic degeneration combined with cognitive testing OFF DA. Within our cohort a wide clinical range was covered as a prerequisite to correlate the spatiotemporal pattern of striatal degeneration with cognitive performance. Due to the fact that most patients in more advanced stages of PD are not able to withdraw from their dopaminergic medication, the number of patients studied is limited. This may have played a role in the missing correlation between DAT uptake in the associative striatum and Stroop outcome measures. Also, the predefined associative striatal ROI is not specifically related to subareas of executive processing. Furthermore, it has to be considered that [123I]FP-CIT SPECT is only able to measure the DA system so we chose to solely investigate non-demented PD patients. It may be postulated that in PD-D the correlation between DAT and cognition may not have been found as result of a ceiling effect of striatal degeneration (as opposed to the floor effect in early PD without MCI) and the involvement of other transmitter systems during the course of the disease (Halliday et al. 2014). SPECT is limited due to restricted spatial resolution that can lead to partial volume effects. This is especially relevant in the small sensorimotor region of the striatum. We could not apply an additional test specific for the limbic striatum as we kept the time to a limit of 2 h in the interest of the patients. Otherwise, fatigue would have been a major confounding factor as well as fluctuations between ON and OFF phases in more severely affected patients. Finally, due to the limited number of patients we are not able to comment on the influence of motor-subtypes or gender on striatal DAT binding.
Conclusions and perspective
We were able to show that cognitive decline in non-demented PD patients goes along with degeneration in the associative subdivision of the striatum. Our data also suggest that executive dysfunctions as measured by the Stroop test are ameliorated by DA whereas global cognition as measured by the MoCA test is not altered by dopaminergic medication and associated with marked striatal neurodegeneration within the associative subdivision. These findings could be relevant for the interpretation of [123I]FP-CIT SPECT data in routine clinical use. As it becomes increasingly obvious that non-motor symptoms are relevant for quality of life it would be helpful to have an imaging marker for the development of cognitive deficits. For example, Ramani and colleagues (2016) were able to show that in akinetic-rigid PD patients, the degree of dopaminergic deficiency on [123I]FP-CIT SPECT correlated inversely with motor severity after 3 years. Our results show the importance of the relative DAT availability in the associative subdivision of the striatum for global cognition. Its potential role as a prognostic value for cognitive decline could be evaluated in future studies.
References
Aarts E, Nusselein A, Smittenaar P, Helmich R, Bloem B, Cools R (2014) Greater striatal responses to medication in Parkinson’s disease are associated with better task-switching but worse reward performance. Neuropsychologia 62:390–397
Alexander GE, DeLong MR, Strick PL (1986) Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annu Rev Neurosci 9:357–381
Behrens TEJ, Johansen-Berg H, Woolrich MW, Smith SM, Wheeler-Kingshott CAM, Boulby PA, Barker GJ, Sillery EL, Sheehan K, Ciccarelli O, Thompson AJ, Brady JM, Matthews PM (2003) Non-invasive mapping of connections between human thalamus and cortex using diffusion imaging. Nat Neurosci 6:750–757
Booij J, Kemp P (2007) Dopamine transporter imaging with [(123)I]FP-CIT SPECT: potential effects of drugs. Eur J Nucl Med Mol I 35:424–438
Brück Portin, Lindell Laihinen, Bergman Haaparanta, Solin Rinne (2001) Positron emission tomography shows that impaired frontal lobe functioning in Parkinson’s disease is related to dopaminergic hypofunction in the caudate nucleus. Neurosci Lett 311:81–84
Brück A, Aalto S, Nurmi E, Vahlberg T, Bergman J, Rinne J (2006) Striatal subregional 6-[18F]fluoro-l-dopa uptake in early Parkinson’s disease: a two-year follow-up study. Mov Disord Off J Mov Disord Soc 21:958–963
Buchert R, Kluge A, Tossici-Bolt L, Dickson J, Bronzel M, Lange C, Asenbaum S, Booij J, Kapucu Ö, Svarer C, Koulibaly P-M, Nobili F, Pagani M, Sabri O, Sera T, Tatsch K, Borght T, Laere K, Varrone A, Iida H (2016) Reduction in camera-specific variability in [123I]FP-CIT SPECT outcome measures by image reconstruction optimized for multisite settings: impact on age-dependence of the specific binding ratio in the ENC-DAT database of healthy controls. Eur J Nucl Med Mol I 43:1323–1336
Bullinger M (1995) German translation and psychometric testing of the SF-36 Health Survey: preliminary results from the IQOLA Project. Int Qual Life Assess Soc Sci Med 41:1359–1366
Chou K, Lenhart A, Koeppe R, Bohnen N (2014) Abnormal MoCA and normal range MMSE scores in Parkinson disease without dementia: cognitive and neurochemical correlates. Parkinsonism Relat Disord 20:1076–1080
Christopher L, Marras C, Duff-Canning S, Koshimori Y, Chen R, Boileau I, Segura B, Monchi O, Lang A, Rusjan P, Houle S, Strafella A (2014) Combined insular and striatal dopamine dysfunction are associated with executive deficits in Parkinson’s disease with mild cognitive impairment. Brain 137:565–575
Cools R, Barker R, Sahakian B, Robbins T (2003) l-Dopa medication remediates cognitive inflexibility, but increases impulsivity in patients with Parkinson’s disease. Neuropsychologia 41:1431–1441
Cools R, Altamirano L, D’Esposito M (2006) Reversal learning in Parkinson’s disease depends on medication status and outcome valence. Neuropsychologia 44:1663–1673
Costa A, la Fougère C, Pogarell O, Möller H-J, Riedel M, Ettinger U (2013) Impulsivity is related to striatal dopamine transporter availability in healthy males. Psychiatry Res Neuroimaging 211:251–256
Costa A, Peppe A, Mazzù I, Longarzo M, Caltagirone C, Carlesimo G (2014) Dopamine treatment and cognitive functioning in individuals with Parkinson’s disease: the “cognitive flexibility”. Hypothesis seems to work. Behav Neurol 2014:260896
Dalrymple-Alford JC, MacAskill MR, Nakas CT, Livingston L, Graham C, Crucian GP, Melzer TR, Kirwan J, Keenan R, Wells S, Porter RJ, Watts R, Anderson TJ (2010) The MoCA: well-suited screen for cognitive impairment in Parkinson disease. Neurology 75:1717–1725
Darcourt J, Booij J, Tatsch K, Varrone A, Borght T, Kapucu Ö, Någren K, Nobili F, Walker Z, Laere K (2010) EANM procedure guidelines for brain neurotransmission SPECT using 123I-labelled dopamine transporter ligands, version 2. Eur J Nucl Med Mol I 37:443–450
Fera F, Nicoletti G, Cerasa A, Romeo N, Gallo O, Gioia M, Arabia G, Pugliese P, Zappia M, Quattrone A (2007) Dopaminergic modulation of cognitive interference after pharmacological washout in Parkinson’s disease. Brain Res Bull 74:75–83
Halliday G, Leverenz J, Schneider J, Adler C (2014) The neurobiological basis of cognitive impairment in Parkinson’s disease. Mov Disord 29:634–650
Hartmann A, Rief W, Hilbert A (2011) Psychometric properties of the German version of the Barratt Impulsiveness Scale, Version 11 (BIS-11) for adolescents. Percept Motor Skill 112:353–368
Hautzinger M (1991) The Beck Depression Inventory in clinical practice. Nervenarzt 62:689–696
Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55:181–184
Kaasinen V, Rinne J (2002) Functional imaging studies of dopamine system and cognition in normal aging and Parkinson’s disease. Neurosci Biobehav Rev 26:785–793
Kish SJ, Shannak K, Hornykiewicz O (1988) Uneven pattern of dopamine loss in the striatum of patients with idiopathic Parkinson’s disease. Pathophysiologic and clinical implications. N Engl J Med 318:876–880
Kupitz D, Apostolova I, Lange C, Ulrich G, Amthauer H, Brenner W, Buchert R (2014) Global scaling for semi-quantitative analysis in FP-CIT SPECT. Nuklearmedizin Nucl Med 53:234–241
Lange C, Seese A, Schwarzenböck S, Steinhoff K, Umland-Seidler B, Krause B, Brenner W, Sabri O, Kurth J, Hesse S, Buchert R (2014) CT-based attenuation correction in I-123-ioflupane SPECT. PLoS One 9:e108328
MacDonald A, Monchi O, Seergobin K, Ganjavi H, Tamjeedi R, MacDonald P (2013) Parkinson’s disease duration determines effect of dopaminergic therapy on ventral striatum function. Mov Disord 28:153–160
Pellecchia Picillo, Santangelo Longo, Moccia Erro, Amboni Vitale, Vicidomini Salvatore, Barone Pappatà (2015) Cognitive performances and DAT imaging in early Parkinson’s disease with mild cognitive impairment: a preliminary study. Acta Neurol Scand 131:275–281
Polito C, Berti V, Ramat S, Vanzi E, Cristofaro M, Pellicanò G, Mungai F, Marini P, Formiconi A, Sorbi S, Pupi A (2012) Interaction of caudate dopamine depletion and brain metabolic changes with cognitive dysfunction in early Parkinson’s disease. Neurobiol Aging 33:206.e29–206.e39
Ramani L, Malek N, Patterson J, Nissen T, Newman EJ (2016) Relationship between [123I]-FP-CIT SPECT and clinical progression in Parkinson’s disease. Acta Neurol Scand 134:378–381
Rektorova I, Srovnalova H, Kubikova R, Prasek J (2008) Striatal dopamine transporter imaging correlates with depressive symptoms and tower of London task performance in Parkinson’s disease. Mov Disord 23:1580–1587
Rinne J, Portin R, Ruottinen H, Nurmi E, Bergman J, Haaparanta M, Solin O (2000) Cognitive impairment and the brain dopaminergic system in Parkinson disease: [18F]fluorodopa positron emission tomographic study. Arch Neurol Chicago 57:470–475
Robbins T, Cools R (2014) Cognitive deficits in Parkinson’s disease: a cognitive neuroscience perspective. Mov Disord 29:597–607
Siepel F, Brønnick K, Booij J, Ravina B, Lebedev A, Pereira J, Grüner R, Aarsland D (2014) Cognitive executive impairment and dopaminergic deficits in de novo Parkinson’s disease. Mov Disord 29:1802–1808
Stroop JR (1935) Studies of interference in serial verbal reactions. J Exp Psychol 18(6):643–662. doi:10.1037/h0054651
Turkheimer FE, Smith CB, Schmidt K (2001) Estimation of the number of “true” null hypotheses in multivariate analysis of neuroimaging data. Neuroimage 13:920–930
Tziortzi A, Haber S, Searle G, Tsoumpas C, Long C, Shotbolt P, Douaud G, Jbabdi S, Behrens T, Rabiner E, Jenkinson M, Gunn R (2014) Connectivity-based functional analysis of dopamine release in the striatum using diffusion-weighted MRI and positron emission tomography. Cereb Cortex 24:1165–1177
Vaillancourt D, Schonfeld D, Kwak Y, Bohnen N, Seidler R (2013) Dopamine overdose hypothesis: evidence and clinical implications. Mov Disord 28:1920–1929
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The project was funded by the DFG (German research Council, grant KU2261/6-1) to AAK. Dorothee Kübler is a participant in the BIH-Charité Clinician Scientist Program funded by the Charité-Universitätsmedizin Berlin and the Berlin Institute of Health.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kübler, D., Schroll, H., Buchert, R. et al. Cognitive performance correlates with the degree of dopaminergic degeneration in the associative part of the striatum in non-demented Parkinson’s patients. J Neural Transm 124, 1073–1081 (2017). https://doi.org/10.1007/s00702-017-1747-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-017-1747-2