
Abstract
Background
With the growing use of endovascular therapy (EVT) to manage unruptured intracranial aneurysms (IAs), detailed information regarding periprocedural complication rates of microsurgical clipping and EVT becomes increasingly important in determining the optimal treatment for individual cases. We report the complication rates associated with open microsurgery in a large series of unruptured IAs and highlight the importance of maintaining surgical skill in the EVT era.
Methods
We reviewed all cases of unruptured IAs treated with open microsurgery by a single neurosurgeon between July 1997 and June 2019. We analyzed surgical complications, deaths, and patient-reported outcomes.
Results
A total of 1923 unruptured IAs in 1750 patients (mean age 44 [range: 6–84], 62.0% [1085/1750] female) were treated surgically during the study period. Of the aneurysms treated, 84.9% (1632/1923) were small, 11.1% (213/1923) were large, and 4.1% (78/1923) were giant. Aneurysm locations included the middle cerebral artery (44.2% [850/1923]), internal carotid artery (29.1% [560/1923]), anterior cerebral artery (21.0% [404/1923]), and vertebrobasilar system (5.7% [109/1923]). The overall mortality rate was 0.3% (5/1750). Surgical complications occurred in 7.4% (129/1750) of patients, but only 0.4% (7/1750) experienced permanent disability. The majority of patients were able to return to their preoperative lifestyles with no modifications (95.9% [1678/1750]).
Conclusions
At a high-volume, multidisciplinary center, open microsurgery in carefully selected patients with unruptured IAs yields favorable clinical outcomes with low complication rates. The improvement of EVT techniques and the ability to refer cases for EVT when a high complication rate with open microsurgery was expected have contributed to an overall decrease in surgical complication rates. These results may serve as a useful point of reference for physicians involved in treatment decision-making for patients with unruptured IAs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Over the past two decades, endovascular therapy (EVT) has emerged as an increasingly important treatment option for intracranial aneurysms (IAs) with EVT being a less-invasive procedure and carrying fewer short-term complications compared to open microsurgery [22, 30]. The ability to refer complex cases to EVT has improved overall outcomes [8], particularly among patients who are older and those who have medical comorbidities [37]. However, as fewer cases are treated with open microsurgery, microsurgical skills and surgical confidence may erode over time, and this may have the unintended adverse consequences of increasing complication rates and worsening outcomes associated with microsurgery.
Nevertheless, there remain select IAs that may be more safely and effectively treated with open microsurgery which, at times, carries the best opportunity for a good long-term outcome. When deciding whether or not to recommend treatment for an unruptured IA and whether conservative management, open microsurgery, or EVT is most appropriate, physicians must rely on a detailed understanding of the risks and potential complications associated with each of these options. We have previously reported decision-making algorithms and surgical outcomes in selected subgroups of patients with unruptured IAs [34,35,36,37]. In this report, we describe the overall complication rates in a large series of unruptured IAs treated with microsurgery at our center over a 23-year period.
Methods
Patient review
Between July 1997 and June 2019, 1750 patients with 1923 unruptured IAs were entered into a prospectively collected database of patients undergoing microsurgery for an unruptured IA. We retrospectively reviewed the operative reports, imaging studies, and follow-up clinic notes of all patients who suffered a postoperative complication in this series noting both permanently disabling and temporary or non-disabling complications.
Management strategy
Our algorithm for the management of patients with unruptured IAs has been described previously [32, 34,35,36,37]. All patients were evaluated by a multidisciplinary team including a neurovascular surgeon and an interventional neuroradiologist who reviewed all imaging studies and then recommended either conservative management, open microsurgery, or EVT. In general, we have recommended observation with follow-up imaging to older patients, those with smaller aneurysms, and those in poor medical condition. Treatment was generally recommended for younger patients with larger lesions, those patients with aneurysms that show interval enlargement on serial imaging studies, and those with a strong family history of IA or personal history of subarachnoid hemorrhage (SAH) from another aneurysm. Symptomatic aneurysms (those with perianeurysmal edema resulting in neurological dysfunction or seizure, or causing third nerve palsy) were also generally offered treatment.
When treatment was recommended, patients with narrow-necked or calcified IAs, patients over 70 years of age, and those with significant medical comorbidities were generally offered EVT, while surgical clipping was recommended to patients with very small IAs (≤ 3 mm) that were nevertheless deemed appropriate for treatment, patients with very wide necked or fusiform lesions, or when treatment with EVT was not felt to be feasible or was attempted and proved unsuccessful. When choosing between open microsurgery and EVT, we recommend the option that offers the lowest major complication rate while attempting to provide a reasonable chance for a long-term durable result.
Surgical procedures
Details of our specific surgical techniques and bypass procedures have been described previously [32,33,34,35,36,37]. All procedures were performed under general endotracheal anesthesia using barbiturate anesthesia and mild hypothermia (34 °C). Patients received mannitol (1 g/kg), decadron (4–10 mg intravenously), and a loading dose of either fosphenytoin or levetiracetam. Intravenous antibiotics were administered preoperatively and continued for 24 h postoperatively. Patients were secured in a radiolucent head frame for surgery. A standard pterional approach was used for most anterior circulation lesions. Additional skull base dissection, including orbitocranial, and orbitozygomatic approaches, were used to obtain optimal visualization of the aneurysm when necessary. Distal anterior cerebral artery (ACA) lesions were treated via parasagittal craniotomy. Basilar artery (BA) lesions were generally treated via a subtemporal approach or a combined half-and-half approach with orbitozygomatic osteotomy [32]. Posterior inferior cerebellar artery (PICA) aneurysms generally underwent a far lateral suboccipital craniotomy. An interhemispheric approach was used for anterior communicating artery (ACOMMA) aneurysms when it was anticipated that the local vascular anatomy would have hidden the aneurysm neck from view when approaching from either side.
An intentional subtotal aneurysm clipping was performed when attempted complete occlusion resulted in significant narrowing of the parent artery or perforator compromise or when calcification or atheroma precluded safe clip placement at the aneurysm neck. In these cases, the area left untreated was subsequently wrapped with muslin-type gauze, cotton, or Gore-Tex.
The intradural portion of all surgeries, including opening of the Sylvian fissure and dissection and clipping of the aneurysm, was performed under microsurgical magnification. No neuromonitoring was used except when parent artery occlusion (PAO) was employed. Intraoperative digital subtraction angiography (DSA) was used in all cases to evaluate IA occlusion and to exclude the presence of vascular compromise. Indocyanine green (ICG) video angiography was also used in all cases after 2010 to evaluate perforator patency. All patients were monitored overnight in a neurointensive care unit, and systolic blood pressure was kept below 140 mm Hg. Patients were mobilized the night of surgery as tolerated. Postoperative CT and MR imaging were performed only when patients demonstrated a new deficit or severe headache after surgery.
For patients undergoing revascularization with PAO, intraoperative angiography was used to confirm bypass patency. Once revascularization was complete, the IA was treated surgically by sacrificing the parent artery with proximal occlusion when possible; otherwise, a distal occlusion was performed when anatomy precluded access to the parent artery proximal to the aneurysm.
Post-operative follow-up and complications
Peri-procedural and immediate post-operative complications were recorded to determine the incidence of non-disabling complications versus disabling and/or fatal complications following microsurgical clipping of unruptured IAs. We evaluated patients daily during their initial hospitalization, at the time of discharge, again 1–2 weeks post-procedure at the time of suture removal, and then at a 4–6-week follow-up visit. Patients who developed a new deficit or any complication that was noted during any of these examinations were followed beyond this period. Patients who traveled from out of state for treatment were seen in follow-up by their local physician, and telephone follow-up was performed by our nursing staff. Postoperative infection was recorded in patients who required hospital readmission for intravenous antibiotic therapy or surgical revision; this study did not account for cases in which the patient’s primary care physician may have prescribed oral antibiotics for a minor or superficial wound infection.
Because neurosurgeons have been criticized for inadequately assessing postoperative cognitive and quality-of-life concerns in patients undergoing craniotomy, we have used Short-Form patient questionnaires SF-12 and/or SF-36 for all patients at last follow-up. Patients were asked to categorize their abilities to return to work or previous lifestyle as requiring no modification, minor modification, major modification, or as unable to return.
For imaging follow-up, patients less than age 60 with complete intraoperative aneurysm occlusion were recommended to undergo 5-year follow-up imaging with magnetic resonance angiography (MRA) or computed tomography angiography (CTA). Patients older than age 60 with complete intraoperative occlusion did not have scheduled follow-up imaging. Patients with > 90% but < 100% aneurysm occlusion were recommended follow-up MRA or CTA at 1 and 5 years after surgery. Patients with < 90% occlusion underwent DSA at 1 year, with additional follow-up determined by our team based on the results of that study. When examining occlusion as an outcome of this study, rates of > 95% occlusion (complete or near-complete occlusion) and 90–95% occlusion are reported.
Results
Patient characteristics and aneurysm morphology
Patient demographics and aneurysm characteristics are presented in Tables 1 and 2. Collectively, there were 1923 unruptured IAs treated in 1750 patients (mean age 44 [range: 6–84], 62.0% [1085/1750] female). The most common comorbidities included smoking in 23.0% (403/1750) of patients, hypertension in 22.0% (385/1750), hyperlipidemia in 19.0% (333/1750), and diabetes mellitus in 11.0% (193/1750). A total of 5.2% (91/1750) of patients had experienced subarachnoid hemorrhage (SAH) from a previously treated IA, 12.0% (210/1750) had a family history of IA, and 4.3% (82/1923) of treated aneurysms had been previously coiled but suffered repeated coil compaction. In 22 additional cases, we attempted coiling but were unsuccessful due to local aneurysm anatomy or vascular morphology/tortuosity of the carotid or vertebral artery; these patients were then treated surgically.
Microsurgical clipping was performed in 93.0% (1789/1923) of cases, while 1.2% (22/1923) of aneurysms were treated with wrapping alone, and 5.3% (102/1923) were treated with bypass and PAO. In 7.1% (137/1923) of cases, repair of another aneurysm was performed simultaneously, and 1.5% (26/1750) patients underwent multiple craniotomies to treat their aneurysms. Intraoperative rupture occurred in 0.4% (7/1923) of treated aneurysms.
Aneurysm sizes and locations are detailed in Table 2. The majority (84.9%, 1632/1923) of aneurysms were small (< 10 mm), 11.1% (213/1923) were large (10–< 25 mm), and 4.1% (78/1923) were giant (≥ 25 mm). Aneurysm locations included the middle cerebral artery (MCA) in 44.2% (850/1923), the internal carotid artery (ICA) in 29.1% (560/1923), the ACA in 21.0% (404/1923), mostly at the ACOMMA (15.6% [300/1923]), and the vertebrobasilar system in 5.7% (109/1923).
Postoperative follow-up
No aneurysms bled during the follow-up period, which ranged from 12 months to 21 years, mean 8.8 years. Two small ACOMMA aneurysms and one small basilar apex aneurysm were stable based on imaging at 1 year, but showed minimal growth (< 2 mm) at 5 years and continue to be followed 6, 9, and 11 years post-surgery. One fusiform MCA aneurysm that had been treated with wrapping alone showed significant enlargement and was subsequently treated with endovascular stenting without incident. No patient with intraoperative rupture suffered a complication, and all had good outcomes at the time of last follow-up visit.
Occlusion rates, complications, and mortality
Complete or near-complete (> 95%) aneurysm occlusion was achieved in 92.9% (1786/1923) aneurysms; 5.4% (104/1923) had 90–95% occlusion, and 1.2% (23/1923) aneurysms were wrapped only due to atheroma or calcification involving the aneurysm wall/neck.
Surgical complications resulting in permanent deficit or death are presented in Table 3. Overall treatment-related complications occurred in 7.4% (129/1750) of patients, among whom 0.4% (7/1750) experienced a permanent disability and 0.3% (5/1750) died. Serious surgical complications resulting in new permanent disability included one case of delayed saphenous vein graft thrombosis in a patient with a giant MCA aneurysm that lead to severe permanent disability requiring assistance with activities of daily living; perforator artery injury in two patients with an MCA aneurysm resulting in permanent hemiparesis (one case was severe, and one was mild), one subdural hemorrhage in a patient with a small ACOMMA aneurysm that lead to a prolonged dependent state, one case of subfrontal contusion in a patient with a small paraclinoid aneurysm leading to persistent mild dysphasia, one case of severe visual impairment in a patient with a giant paraclinoid aneurysm, and one case of third nerve palsy in a patient with a large basilar artery aneurysm leading to permanent ptosis.
Five patients (0.3% [5/1750]) died as a result of major complications in the post-operative period. One patient with a small ACOMMA aneurysm experienced a disseminated intravascular coagulation on post-operative day 1, resulting in multi-system organ failure; the patient died despite treatment with anticoagulation and supportive care. Another patient with a small ACOMMA aneurysm experienced severe myocardial infarction, and died despite treatment with an intra-aortic balloon pump. An older woman with a giant cavernous ICA aneurysm died after a suffering large infarct of the MCA following ICA sacrifice. This patient passed her balloon test occlusion both clinically and in terms of single-photon emission computed tomography (SPECT) analysis. We believe she suffered a large embolic MCA infarction despite low-dose anticoagulation and antiplatelet therapy. One patient with a small carotid ophthalmic aneurysm died suddenly at home on post-operative day 21 due to a pulmonary embolism that was subsequently identified at autopsy. One patient with a giant PICA aneurysm died after experiencing post-operative pneumonia and meningitis leading to sepsis and multisystem organ failure despite prolonged antibiotic therapy and lumbar drainage.
Surgical complications not resulting in permanent deficit or death are presented in Table 4. The most frequent non-disabling complication was deep vein thrombosis (DVT) with or without pulmonary embolism (PE) occurring in 2.2% (38/1750) of patients. A total of 1.8% (31/1750) of patients were displeased with the cosmetic result of the surgery, and five of these elected to undergo delayed cosmetic reconstruction by a plastic surgeon. Chronic subdural hematoma occurred in 1.0% (17/1750) of patients; four underwent delayed surgical evacuation 5 weeks to 6 months after their initial surgery. Major wound infections occurred in 12 cases, 5 of which required reoperation, with immediate replacement of the bone flap with a titanium mesh cranioplasty in four and delayed cranioplasty in one. The remainder were managed with antibiotic therapy alone. Postoperative seizure occurred in 0.5% (8/1750) patients; one had a prior history of epilepsy, and no other patients required permanent anticonvulsant therapy thereafter. Other less frequently occurring (< 1.0%) non-disabling complications included transient third nerve palsy, asymptomatic myocardial infarction, ipsilateral vocal cord paralysis and/or transient dysphagia (following PICA aneurysm repair), complete olfactory loss, transient hemiparesis, epidural hematoma, and venous ischemia in one patient undergoing an interhemispheric approach for a distal ACA aneurysm. This last patient required prolonged intensive care unit (ICU) monitoring for cerebral edema but ultimately had an excellent outcome.
Overall, the vast majority of patients (95.9% [1678/1750]) were able to return to their previous lifestyles with no modifications (Table 5). A smaller percentage reported the need for minor (3.3% [58/1750]) or major (0.2% [5/1750]) modifications to their lifestyle, and 0.5% (9/1750) were unable to return to work or previous lifestyle due to death or poor outcome. Three patients with permanent disabilities were able to return to work or previous lifestyle with modifications (Patients 7, 10, and 12 in Table 3). Among the patients requiring modifications, 49 who would have been judged to have good clinical outcomes based on traditional reporting measures nevertheless felt their quality of life was worse postoperatively on a subjective basis, due to complaints including anxiety regarding potential aneurysm recurrence, headaches, intermittent facial swelling, anosmia, and attention difficulties interfering with job performance. A total of 25/72 (34.7%) of these patients requiring modifications or unable to return to previous lifestyle carried psychiatric diagnoses before surgery including major depression and/or anxiety disorder. All of these patients were able to return to work or previous lifestyle with minor or major modification with the exception of the patient with anosmia who chose not to return to work.
Discussion
The optimal management of unruptured IAs requires meticulous selection of the best treatment regimen for each individual patient based on a thorough appreciation of the risks and potential complications associated with conservative management, open microsurgery, and EVT. Such a detailed understanding of each treatment option is central to the decision-making process because the natural history of many unruptured IAs is benign and because there may be selected subsets of IAs that are best treated with EVT while others, due to location, size, morphology, or patient characteristics, will be better managed with open microsurgery. Our series demonstrates that microsurgical treatment provides low morbidity and mortality rates when a multidisciplinary team approach is used to determine the optimal treatment pathway at a high-volume center. Although the diminishing incidence of serious complications over time may be related to increased surgical experience by the senior author, we suggest that the improvement of EVT techniques and the ability to refer cases for EVT when a high complication rate with open microsurgery was expected have played a major role in improving our complication rates.
Microsurgery and endovascular treatment
The rapid evolution of EVT including the introductions of flow diversion and intrasaccular flow disruption techniques has resulted in proportionally fewer aneurysms being treated via microsurgical clipping [14, 44]. We suggest that increasing technical experience over time as well as the ability to refer complicated cases to EVT as a treatment option have contributed to an overall decrease in our surgical complication rates. For example, following the introduction of stenting as a useful option for the management of wide-necked aneurysms, we have only rarely performed microsurgery for larger basilar apex aneurysms, effectively eliminating surgical complications in this challenging group of aneurysms. Paradoxically, however, this trend has likely resulted in an erosion of microsurgical skills which may increase complication rates with open microsurgery performed by less experienced surgeons. This phenomenon has led some to predict the appropriateness of replacing open microsurgery with EVT in almost all IA cases. In contrast, at our center, we have always viewed EVT and open surgery as complementary rather than competitive and have recommended whichever option we believe will result in good aneurysm obliteration while carrying the lowest complication rates, offering the patient the best chance for a good long-term outcome. Based on this experience, we suggest that such a combined team approach can offer better results than an imbalanced approach where EVT or surgery dominate the treatment decision.
Microsurgery continues to be safe and effective for many patients [34], especially younger individuals [25, 37], those with smaller lesions, wide-necked aneurysms [1, 2, 37, 40], unruptured MCA aneurysms [9, 13, 16, 35], and aneurysms with complex perforator involvement [20]. As a consequence, we typically offer open microsurgery to patients with MCA aneurysms which tend to have a wide neck often incorporating the M2 branches and which therefore carry lower treatment-related morbidity with open surgery in our experience. In contrast, we recommend open surgery for VBA aneurysms only when EVT is felt to be impossible or to carry a significantly higher risk than open microsurgery. Therefore, the vast majority of VBA aneurysms, and particularly VB junction aneurysms and those occurring at the basilar apex, are currently treated using EVT in our practice.
Importantly, a number of reviews have found similar overall complication rates between microsurgical and EVT techniques in patients with unruptured IAs [10, 19, 41, 43]. A recent meta-analysis by Kang et al. reviewed data from 129,317 patients with unruptured IAs and showed a significantly lower rate of procedural complications with coiling vs. surgical clipping (4.6% vs. 7.0%, P < 0.001) [22], but notably showed that EVT had a lower rate of complete occlusion at short-term (OR 0.179, 95% CI 0.064–0.499, P = 0.001) and 1-year follow-up (OR 0.307, 95% CI 0.146–0.646, P = 0.002) [22]. Higher rates of complete occlusion and lower rates of recurrence in patients treated surgically have been corroborated in other studies [15, 16, 19, 26, 31, 41, 42, 44, 45]. However, several reports have found higher morbidity and mortality rates in patients treated microsurgically, including a study by Brinjikji et al. that analyzed NIS hospital discharge data to evaluate the outcomes of 64,043 patients with unruptured IAs (29,918 treated with surgery and 34,125 treated with EVT) [8]. Compared to EVT, the authors reported higher rates of mortality (1.2% vs. 0.6%, P < 0.0001), surgical complications (3.3% vs. 1.6%, P < 0.0001), neurological complications (7.8% vs. 2.3%, P < 0.0001), and overall complications including discharge to long-term facility (14.0% vs. 4.9%, P < 0.0001) among patients treated with clipping [8].
Though a number of large studies have found relatively high complication rates associated with open microsurgery for IAs, with mortality rates as high as 2.66% [4, 8, 27], such large national sample studies include patients managed with open surgery at low volume centers which may inappropriately inflate complication and death rates. By centralizing the management of IAs at higher volume multidisciplinary centers that offer a team approach, patients that would be best treated with EVT can be removed from the equation, and better outcomes can be offered for those complex aneurysms still requiring open surgery. It should come as no surprise that when looking at an unselected series of IAs at all locations, EVT will offer lower short-term complication rates than open microsurgery. But by using a careful selection process, teams can optimize surgical results, offering better outcomes with lower complication and mortality rates. In addition, microsurgical techniques avoid particular device-related complications such as coil stretching or migration [38, 43], and numerous studies have reported that microsurgery confers a lower risk of thromboembolic complications [7, 22, 24, 38, 43], and provides better long-term occlusion and reduced recurrence/retreatment rates in patients with unruptured IAs [7, 15, 42].
Multiple factors likely contributed to the favorable outcomes achieved in this series. We have alluded to increasing experience over time at a high-volume center with the experience being concentrated in the hands of a single surgeon. Equally important in our opinion was the integrated team approach, creating a collaborative rather than competitive environment in which each patient was discussed openly, and the treatment option felt to carry the best long-term result balanced with the lowest complication rate was recommended to the patient. As endovascular techniques have improved, we have increasingly relied on EVT, allowing us to treat the most dangerous surgical aneurysms using less risky means. Finally, a standardized approach incorporating repeated application of the same principles to pre-, intra-, and post-operative care have likely improved our outcomes as well. We believe that such a standardized approach allows everyone who touches the patient to develop a high level of comfort and expertise with the issues unique to IA patients, and we consider this important in optimizing outcomes.
Predictors of complications
A major meta-analysis of 54 studies including data on 108,263 unruptured IAs treated surgically found an overall pooled postoperative complication rate of 8.34% [3]. Ischemic complication rates in these studies range between 2.5 and 10% [3, 23, 44], ischemic stroke rates range from 4.3 to 8.16% [4, 6, 23], hemorrhagic complications rates from 2.38 to 5% [3, 4, 44], cardiac complications rates from 0.15 to 3.18% [4, 8, 23], and PE rates from 0.91 to 2.11% [4, 23]. Specific preoperative comorbidities associated with poor outcome and readmission include older age, obesity (class II or III), hypertension, congestive heart failure, coagulopathy, smoking, alcohol/drug use, anemia, preoperative hyponatremia, aneurysm size, and posterior circulation unruptured IA [1, 3, 11, 12, 17, 23, 27, 29]. If surgical morbidity is anticipated to be high due to these factors, then EVT should be considered or conservative management without intervention may be most appropriate.
The current study found lower rates of morbidity and mortality than were found in other large studies for EVT or microsurgery, indicating that the range of patient outcomes in treating IAs may be influenced by factors other than the chosen treatment modality. Given the invasive nature and technical challenges associated with microsurgical treatment, outcomes are also heavily dependent on a given center’s microsurgical and interventional experience, institutional support, and the implementation of effective treatment algorithms based on careful risk stratification of patients [5, 18, 21, 28, 39]. Morbidity and mortality have been found to correlate with treatment volumes, and this study’s findings for these outcome measures may reflect the high volume and experience that intense subspecialization and institutional competencies can provide. We recommend that discussions of IA treatment strategies be focused not only on treatment modality choice but also on optimizing patient access to institutions with the resources and support to improve outcomes above those seen in broad national samples. The American Heart Association/American Stroke Association have similarly recommended that the surgical treatment of IAs be performed at high volume centers [44], highlighting the continued need for proper training of young cerebrovascular surgeons to safely undertake these types of operations and deliver superior outcomes to patients.
Limitations
The principal limitations of this report include its retrospective nature, which introduces potential selection bias, and the fact that the operations were performed by a single surgeon at a large volume multidisciplinary center over the course of 23 years, potentially limiting the generalizability of its data. At the same time, since this study describes complications in a large cohort of patients with aneurysms at a wide variety of locations treated during the era of EVT, it is hoped that this work may help address questions regarding the incidence and spectrum of complications as well as the mortality associated with the microsurgical treatment of unruptured IA aneurysms, a technique being used less frequently as EVT improves. This information may become increasingly important to physicians who must decide how to manage patients with unruptured IAs in the future.
Conclusion
Our results in a large series of unruptured IAs demonstrate that careful patient selection by a multidisciplinary team at a high-volume center can yield low complication and mortality rates. This data, from the largest single-center surgical IA treatment series published to date, suggests that tailoring treatment for each unruptured IA can minimize the surgical risk to patients. By providing data regarding the morbidity and mortality rates that can be achieved realistically by applying a multidisciplinary dedicated team approach to the management of unruptured IAs, it is hoped that this work will help physicians better decide between the available treatment options for these complex patients.
References
Acioly MA, Shaikh KA, White IK, Ziemba-Davis M, Bohnstedt BN, Cohen-Gadol A (2019) Predictors of outcomes and complications after microsurgical and endovascular treatment of 1300 intracranial aneurysms. World Neurosurg 122:e516–e529
Aghakhani N, Vaz G, David P, Parker F, Goffette P, Ozan A, Raftopoulos C (2008) Surgical management of unruptured intracranial aneurysms that are inappropriate for endovascular treatment: experience based on two academic centers. Neurosurgery 62:1227–1234 (discussion 1234–1225)
Algra AM, Lindgren A, Vergouwen MDI, Greving JP, van der Schaaf IC, van Doormaal TPC, Rinkel GJE (2019) Procedural clinical complications, case-fatality risks, and risk factors in endovascular and neurosurgical treatment of unruptured intracranial aneurysms: a systematic review and meta-analysis. JAMA Neurol 76:282–293
Alshekhlee A, Mehta S, Edgell RC, Vora N, Feen E, Mohammadi A, Kale SP, Cruz-Flores S (2010) Hospital mortality and complications of electively clipped or coiled unruptured intracranial aneurysm. Stroke 41:1471–1476
Barker FG 2nd, Amin-Hanjani S, Butler WE, Ogilvy CS, Carter BS (2003) In-hospital mortality and morbidity after surgical treatment of unruptured intracranial aneurysms in the United States, 1996–2000: the effect of hospital and surgeon volume. Neurosurgery 52:995–1007 (discussion 1007–1009)
Beydoun HA, Beydoun M, Zonderman A, Eid SM (2020) Perioperative ischemic stroke in unruptured intracranial aneurysm surgical or endovascular therapy. Cureus 12:e7645
Blackburn SL, Abdelazim AM, Cutler AB, Brookins KT, Fargen KM, Hoh BL, Kadkhodayan Y (2014) Endovascular and surgical treatment of unruptured mca aneurysms: meta-analysis and review of the literature. Stroke Res Treat 2014:348147
Brinjikji W, Rabinstein AA, Nasr DM, Lanzino G, Kallmes DF, Cloft HJ (2011) Better outcomes with treatment by coiling relative to clipping of unruptured intracranial aneurysms in the United States, 2001–2008. AJNR Am J Neuroradiol 32:1071–1075
Dammann P, Schoemberg T, Muller O, Ozkan N, Schlamann M, Wanke I, Sandalcioglu IE, Forsting M, Sure U (2014) Outcome for unruptured middle cerebral artery aneurysm treatment: surgical and endovascular approach in a single center. Neurosurg Rev 37:643–651
Darsaut TE, Findlay JM, Magro E, Kotowski M, Roy D, Weill A, Bojanowski MW, Chaalala C, Iancu D, Lesiuk H, Sinclair J, Scholtes F, Martin D, Chow MM, O’Kelly CJ, Wong JH, Butcher K, Fox AJ, Arthur AS, Guilbert F, Tian L, Chagnon M, Nolet S, Gevry G, Raymond J (2017) Surgical clipping or endovascular coiling for unruptured intracranial aneurysms: a pragmatic randomised trial. J Neurol Neurosurg Psychiatry 88:663–668
Dasenbrock HH, Rudy RF, Gormley WB, Smith TR, Frerichs KU, Aziz-Sultan MA, Du R (2016) 111 Predictors of complications after clipping of unruptured intracranial aneurysms: a national surgical quality improvement program analysis. Neurosurgery 63:147–147
Dasenbrock HH, Smith TR, Rudy RF, Gormley WB, Aziz-Sultan MA, Du R (2018) Reoperation and readmission after clipping of an unruptured intracranial aneurysm: a National Surgical Quality Improvement Program analysis. J Neurosurg 128:756–767
Diaz OM, Rangel-Castilla L, Barber S, Mayo RC, Klucznik R, Zhang YJ (2014) Middle cerebral artery aneurysms: a single-center series comparing endovascular and surgical treatment. World Neurosurg 81:322–329
Golnari P, Nazari P, Garcia RM, Weiss H, Shaibani A, Hurley MC, Ansari SA, Potts MB, Jahromi BS (2020) Volumes, outcomes, and complications after surgical versus endovascular treatment of aneurysms in the United States (1993–2015): continued evolution versus steady-state after more than 2 decades of practice. J Neurosurg 134:848–861
Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW (2010) A review of the management of posterior communicating artery aneurysms in the modern era. Surg Neurol Int 1:88
Guresir E, Schuss P, Berkefeld J, Vatter H, Seifert V (2011) Treatment results for complex middle cerebral artery aneurysms. A prospective single-center series Acta Neurochir (Wien) 153:1247–1252
Hackenberg KAM, Hanggi D, Etminan N (2018) Unruptured Intracranial Aneurysms. Stroke 49:2268–2275
Hsu CE, Lin TK, Lee MH, Lee ST, Chang CN, Lin CL, Hsu YH, Huang YC, Hsieh TC, Chang CJ (2016) The Impact of surgical experience on major intraoperative aneurysm rupture and their consequences on outcome: a multivariate analysis of 538 microsurgical clipping cases. PLoS One 11:e0151805
Huang C, You C (2019) Clipping Versus coiling in the management of unruptured aneurysms with multiple risk factors. World Neurosurg 126:e545–e549
Ihn YK, Shin SH, Baik SK, Choi IS (2018) Complications of endovascular treatment for intracranial aneurysms: Management and prevention. Interv Neuroradiol 24:237–245
Jabbarli R, Wrede KH, Pierscianek D, Dammann P, El Hindy N, Ozkan N, Muller O, Stolke D, Forsting M, Sure U (2016) Outcome After Clipping of Unruptured Intracranial Aneurysms Depends on Caseload. World Neurosurg 89:666–671 (e661)
Kang XK, Guo SF, Lei Y, Wei W, Liu HX, Huang LL, Jiang QL (2020) Endovascular coiling versus surgical clipping for the treatment of unruptured cerebral aneurysms: direct comparison of procedure-related complications. Medicine 99:e19654
Kerezoudis P, McCutcheon BA, Murphy M, Rayan T, Gilder H, Rinaldo L, Shepherd D, Maloney PR, Hirshman BR, Carter BS, Bydon M, Meyer F, Lanzino G (2016) Predictors of 30-day perioperative morbidity and mortality of unruptured intracranial aneurysm surgery. Clin Neurol Neurosurg 149:75–80
Klotzsch C, Nahser HC, Henkes H, Kuhne D, Berlit P (1998) Detection of microemboli distal to cerebral aneurysms before and after therapeutic embolization. AJNR Am J Neuroradiol 19:1315–1318
Komotar RJ, Mocco J, Solomon RA (2008) Guidelines for the surgical treatment of unruptured intracranial aneurysms: the first annual J. Lawrence pool memorial research symposium–controversies in the management of cerebral aneurysms. Neurosurgery 62:183–193 (discussion 193–184)
Kwinta BM, Klis KM, Krzyzewski RM, Wilk A, Dragan M, Grzywna E, Popiela T (2019) Elective management of unruptured intracranial aneurysms in elderly patients in a high-volume center. World Neurosurg 126:e1343–e1351
Lawson MF, Neal DW, Mocco J, Hoh BL (2013) Rationale for treating unruptured intracranial aneurysms: actuarial analysis of natural history risk versus treatment risk for coiling or clipping based on 14,050 patients in the Nationwide Inpatient Sample database. World Neurosurg 79:472–478
Lawton MT, Du R (2005) Effect of the neurosurgeon’s surgical experience on outcomes from intraoperative aneurysmal rupture. Neurosurgery 57:9–15 (discussion 19–15)
Mahaney KB, Brown RD Jr, Meissner I, Piepgras DG, Huston J 3rd, Zhang J, Torner JC, Investigators I (2014) Age-related differences in unruptured intracranial aneurysms: 1-year outcomes. J Neurosurg 121:1024–1038
Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R, International Subarachnoid Aneurysm Trial Collaborative G (2002) International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 360:1267–1274
Nanda A, Patra DP, Bir SC, Maiti TK, Kalakoti P, Bollam P (2017) Microsurgical Clipping of unruptured intracranial aneurysms: a single surgeon’s experience over 16 years. World Neurosurg 100:85–99
Nussbaum ES (2012) Video Atlas of Intracranial Aneurysm Surgery, 1st edn. Thieme Medical Publishers Inc, New York
Nussbaum ES, Mocco J (2011) Cerebral revascularization: microsurgical and endovascular techniques. Thieme Medical Publishers, Stuttgart
Nussbaum ES, Madison MT, Myers ME, Goddard J (2007) Microsurgical treatment of unruptured intracranial aneurysms. A consecutive surgical experience consisting of 450 aneurysms treated in the endovascular era. Surg Neurol 67:457–464 (discussion 464–456)
Nussbaum ES, Madison MT, Goddard JK, Lassig JP, Kallmes KM, Nussbaum LA (2018) Microsurgical treatment of unruptured middle cerebral artery aneurysms: a large, contemporary experience. J Neurosurg 1:1–7
Nussbaum ES, Kallmes KM, Lassig JP, Goddard JK, Madison MT, Nussbaum LA (2018) Cerebral revascularization for the management of complex intracranial aneurysms: a single-center experience. J Neurosurg 1:1–11
Nussbaum ES, Touchette JC, Madison MT, Goddard JK, Lassig JP, Nussbaum LA (2020) Microsurgical treatment of unruptured anterior communicating artery aneurysms: approaches and outcomes in a large contemporary series and review of the literature. Oper Neurosurg 19:678–690
Pierot L, Spelle L, Vitry F, Investigators A (2008) Immediate clinical outcome of patients harboring unruptured intracranial aneurysms treated by endovascular approach: results of the ATENA study. Stroke 39:2497–2504
Rinaldo L, McCutcheon BA, Murphy ME, Shepherd DL, Maloney PR, Kerezoudis P, Bydon M, Lanzino G (2017) Quantitative analysis of the effect of institutional case volume on complications after surgical clipping of unruptured aneurysms. J Neurosurg 127:1297–1306
Rodriguez-Hernandez A, Sughrue ME, Akhavan S, Habdank-Kolaczkowski J, Lawton MT (2013) Current management of middle cerebral artery aneurysms: surgical results with a “clip first” policy. Neurosurgery 72:415–427
Ruan C, Long H, Sun H, He M, Yang K, Zhang H, Mao B (2015) Endovascular coiling vs. surgical clipping for unruptured intracranial aneurysm: A meta-analysis. Br J Neurosurg 29:485–492
Smith TR, Cote DJ, Dasenbrock HH, Hamade YJ, Zammar SG, El Tecle NE, Batjer HH, Bendok BR (2015) Comparison of the efficacy and safety of endovascular coiling versus microsurgical clipping for unruptured middle cerebral artery aneurysms: a systematic review and meta-analysis. World Neurosurg 84:942–953
Song J, Kim BS, Shin YS (2015) Treatment outcomes of unruptured intracranial aneurysm; experience of 1,231 consecutive aneurysms. Acta Neurochir (Wien) 157:1303–1310 (discussion 1311)
Thompson BG, Brown RD Jr, Amin-Hanjani S, Broderick JP, Cockroft KM, Connolly ES Jr, Duckwiler GR, Harris CC, Howard VJ, Johnston SC, Meyers PM, Molyneux A, Ogilvy CS, Ringer AJ, Torner J, American Heart Association Stroke Council CoC, Stroke N, Council on E, Prevention, American Heart A, American Stroke A (2015) Guidelines for the Management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 46:2368–2400
Zhu Y, Pan J, Shen J, Liu C, Fan Z, Shen Y, Wen L, Tong Y, Zhan R (2015) Clinical and radiological outcomes after treatment of unruptured paraophthalmic internal carotid artery aneurysms: a comparative and pooled analysis of single-center experiences. World Neurosurg 84:1726–1738
Acknowledgements
The authors acknowledge Superior Medical Experts for research and drafting assistance.
Funding
This manuscript was supported by a grant from the United Hospital Foundation, awarded to ESN.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
JCT is CEO and has ownership interest in Superior Medical Experts. The authors declare no conflict of interest concerning the materials or methods used in this study.
Informed consent
All patients gave informed consent prior to inclusion in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Comments:
First, we would like to congratulate the authors on their effort across almost a quarter of century to establish a new standard for morbidity and mortality of unruptured intracranial aneurysm surgery. Notwithstanding, the paper and the data deserve some comments.
First, microsurgery for unruptured intracranial aneurysms is a well established, effective and durable treatment. Neurosurgeons should not apologize when they decide to treat aneurysms microsurgically, especially those on MCA tree and anterior circulation. No study to the present date showed unequivocally the superiority of other treatments over microsurgery.
Having said that, unruptured aneurysms have a rupture rate on the long-term, recurrence after treatment,and a biology that is different from ruptured ones. It’s a common mistake to look to this group retrospectively with data gathered from the analysis of ruptured aneurysms. This means that we should be very careful with the selection of those unruptured aneurysms that deserve treatment as well as our M&M should be kept at a very low level. That level remains to be determined.
In the years to come, hopefully, new modalities to help us determine which aneurysms deserve treatment will come to our armamentarium. Then, we’ll rely less on morphological criteria and more on biological characteristics of the aneurysm’ wall. Considering the complexity of the disease this won’t be an easy task. Until then and also from then on the focus should be on prevention, especially on restricted smoking public policies as well as hypertension awareness and effective treatment.
Another point of interest is the reporting of occlusion rates as a measure of success in aneurysm surgery. Complete occlusion is unquestionably important or mandatory in ruptured aneurysms since the inflammation process proved to come to a ‘no-return’ point and the re-rupture is a big concern. Contrariwise, in unruptured aneurysms the focus should be on the side of avoiding complications, since rupture of a neck remnant is an extremely uncommon event. The authors should be congratulated for this.
Finally, the authors tried to evaluate cognitive and quality-of-life issues in this paper. They claim, correctly, that this is a commonly overlooked problem in neurosurgery. However, in our opinion, worst than non-assessment is a bad or confusing one. Without a proper pre-operative neuropsychological evaluation, a post-operative MRI searching for new lesions (especially minor asymptomatic strokes or contusions) followed by new neuropsychological assessment it’s not possible to judge on this issue properly. New studies with new designs should be undertaken with this purpose.
Joao Silva and Mika Niemelä
Helsinki, Finland
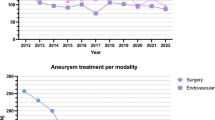
In this manuscript the authors describe a large number of unruptured aneurysms which have undergone clipping by a single neurosurgeon. The study is generally descriptive in that they are selected from a larger cohort, about half of which underwent endovascular treatment and half of which underwent open surgical treatment. The overall mortality rate was low at 0.3% (5/1750). Permanent disability occurred in 0.4% (7/1750). A return to preoperative lifestyles with no modifications occurred in 95.9% (1678/1750). While more granular data regarding specific quality of life measures and neurocognitive outcomes is lacking, this constitutes an endorsement of the safety of microsurgery in experienced hands. This study does not provide data regarding different epochs in the surgeon's experience, but the event numbers are so low that it is unlikely that there would be any significant difference between the early and later parts of the surgeon's career. The retrospective and selected nature of the study means that the low complication rates cannot be attributed to any specific factors, but one can speculate that clipping aneurysms under the favorable conditions present in the unruptured state makes very good outcomes possible. Endovascular techniques and technology continue to evolve and produce better and better outcomes. However, arguably a major role still exists for clipping as is employed in this practice, provided the practitioner is careful, skilled, and experienced. Preservation and perfection of the skill of open clipping should still be emphasized strongly so that whatever the choice of modality, the best outcome for that modality is being offered to the patient. Loss of clipping skills may lead to a bias in favor of endovascular treatment outcomes, with a commensurate bias in modality selection generating a self-fulfilling prophecy in favor of more endovascular treatment. It has been our observation that the clipping learning curve is longer and more difficult to navigate; this is not a reason not to attain such expertise.
Roland Jabre,
Brittany Madison Gerald,
Peter Nakaji,
Phoenix, Arizona, USA
This article is part of Topical Collection on Vascular Neurosurgery – Aneurysm
Rights and permissions
About this article

Cite this article
Nussbaum, E., Touchette, J., Madison, M. et al. Procedural complications in patients undergoing microsurgical treatment of unruptured intracranial aneurysms: a single-center experience with 1923 aneurysms. Acta Neurochir 164, 525–535 (2022). https://doi.org/10.1007/s00701-021-04996-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-021-04996-9