
Abstract
Purpose
Unresectable recurrence is a critical predictor of outcomes for colorectal cancer patients. We attempted to identify the prognostic factors, especially for unresectable recurrence-free survival (URFS) as a new endpoint, in patients with resectable colorectal liver-only metastasis (CRLOM).
Methods
We investigated patients with resectable CRLOM, who underwent an R0 resection for both CRC and CRLOM between January, 2014 and March, 2019 at a single institution. The exclusion criteria were patients who received neoadjuvant treatment, the absence of data for genetic analyses, and the presence of multiple cancers, synchronous CRC, or familial adenomatous polyposis. The prognostic factors were examined retrospectively using data on pre-hepatectomy factors, including primary tumor molecular profiling results.
Results
We analyzed the data of 101 patients who underwent curative-intent surgery for CRLOM. Multivariate analysis revealed that KRAS G12D mutation-positivity (hazard ratio [HR]: 7.69; p < 0.01), RYR2 mutation-positivity (HR: 4.03; p < 0.01), and KRAS G12S mutation-positivity (HR: 3.96; p = 0.03), CA19-9 > 37 U/ml before hepatectomy (HR: 3.62; p < 0.01), and primary tumor pN2 stage (HR: 3.22; p = 0.03) were significant predictors of the URFS.
Conclusions
This is the first study to show that specific KRAS and RYR2 mutations were associated with the URFS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is a major cause of death worldwide. Liver metastases develop during the course of the disease in approximately 25% of patients diagnosed with CRC [1]. Liver resection is a curative treatment for colorectal liver metastases (CRLM); however, even after resection for CRLM, recurrence develops in 75% of patients during follow-up [2]. Despite the high recurrence rate, repeat resection appears to be effective for CRLM, potentially increasing the 5-year post-hepatectomy survival rate to up to 54% [2]. Unresectable recurrence thus represents an important predictor of the outcome of patients after curative-intent surgery for CRLM.
RAS and BRAF V600E mutations have been reported to shorten the relapse-free survival (RFS) and overall survival (OS) of patients with resectable CRLM [3]; however, the effects of other genetic factors remain unclear. There have been few reports of studies that used tumor molecular profiling. Furthermore, although RAS mutations are a strong prognostic factor for a poor outcome, few studies have analyzed the prognostic impact of subtypes of RAS mutations.
The present study focused on colorectal liver-only metastasis (CRLOM) because the prognosis of concurrent extrahepatic metastasis is worse than for CRLOM [4]. We used unresectable recurrence-free survival (URFS) as a new endpoint and defined URFS as the interval from the time of curative resection to the time of unresectable recurrence or death. The purpose of this study was to identify prognostic factors specific to URFS, in addition to RFS and cancer-specific survival (CSS), using primary tumor molecular profiling and clinicopathological factors before hepatectomy in patients with resectable CRLOM. We also examined the prognostic impact of subtypes of RAS mutations.
Materials and methods
Ethics statement
In 2014, Shizuoka Cancer Center initiated Project HOPE (High-Tech Omics-Based Patient Evaluation) to investigate the biological characteristics of cancers [5, 6]. That project subjected various types of cancers to multi-omics-based analysis with the aim of advancing precision medicine. The project was conducted at a single institution and designed in accordance with the “Ethical Guidelines for Human Genome and Genetic Analysis Research,” as revised in 2013. Informed consent was obtained from all the patients, and the institutional review board of Shizuoka Cancer Center approved all aspects of this study (authorization no. 25–33).
Patient selection and study design
We enrolled patients with resectable CRLOM who underwent R0 resection for both CRC and CRLOM between January, 2014 and March, 2019 at Shizuoka Cancer Center. CRLOM was defined as CRLM without concurrent extrahepatic metastasis that would worsen the prognosis [4]. In our institution, preoperative chemotherapy is not given when CRC and/or CRLOM is considered resectable. Synchronous metastasis was defined as CRLOM detected at the time of CRC diagnosis. Among patients with metachronous metastasis, those with CRLOM occurring as the first relapse were considered eligible for inclusion in the study. Exclusion criteria were a history of neoadjuvant treatment, the absence of data for genetic analyses, or the presence of multiple cancers, synchronous CRC, or familial adenomatous polyposis. All tumors were diagnosed pathologically as adenocarcinoma. All treatment strategies were approved at multidisciplinary team conferences in our institution. We used selected data from Project HOPE, and the study protocol was approved by the institutional review board of Shizuoka Cancer Center Hospital (institutional code: J2022-29).
Treatment indications
The standard operative procedure for CRC was colorectal resection with D3 lymph node (LN) dissection according to the Japanese Society for Cancer of the Colon and Rectum Guidelines for the Treatment of Colorectal Cancer [7, 8]. If the patient was over 75 years of age or had a high risk of preoperative comorbidities, D2 LN dissection was permitted in our institution. As previously reported, for locally advanced rectal cancer, we performed surgery without giving neoadjuvant chemoradiotherapy [9,10,11].
The preoperative assessments and resection criteria for CRLM were as described previously in detail [12]. Briefly, CRLM were resected whenever technically possible, with the preservation of liver function. No limit was set on the number or size of the CRLM. Resectable CRLM were generally resected without giving preoperative chemotherapy. For patients with synchronous metastasis, we usually performed colorectal resection and hepatectomy separately. In principle, colorectal resection was performed first, followed by hepatectomy. Between each surgery, imaging examinations involving computed tomography (CT), magnetic resonance imaging, or both, were done to determine the resectability. The levels of carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA19-9) were measured before colorectal resection and before hepatectomy, and each value was assessed. When a relapse occurred, oncologically resectable recurrences were generally resected.
Adjuvant chemotherapy after hepatectomy remains controversial [13]. In the present study, the patient decided about whether to be treated with adjuvant chemotherapy, after informed consent.
Indications for treating relapses and definition of unresectable recurrence
In our institution, surgery is selected if the relapse site can be completely resected. Patients with a relapse that is initially unresectable can undergo surgery if the relapse site becomes resectable after response to chemotherapy.
For patients with hematogenous recurrence only or local recurrence only, unresectable recurrence was defined as a recurrence that could not be resected completely. For patients with LN recurrence only or peritoneal dissemination relapse only, if the relapse was localized, surgery was selected. When an R0 resection could not be performed, it was considered an unresectable relapse. If the recurrence was not localized, it was considered an unresectable relapse. Simultaneous multiple relapses were considered an unresectable relapse, but if there was no new relapse or growth only in an existing recurrence after several months of chemotherapy, resection was considered, and if an R0 resection could be performed, it was considered a resectable relapse.
Surveillance protocol
Patients were monitored for 5 years after surgery. The surveillance protocol at our institution consisted of interviews, physical examinations, blood testing (including the CEA and CA19-9 levels), and CT of the chest, abdomen, and pelvis every 3 months for the first 3 years after the final surgery, and then every 6 months thereafter. Colonoscopy was performed annually for the first 3 years after surgery.
Definitions of survival
RFS was defined as the interval from the first hepatectomy to the first recurrence or death. CSS was defined as the interval from the first hepatectomy until death from CRC. As described in “Introduction”, URFS was defined as the interval from the first hepatectomy to the time of the finally unresectable recurrence or death. For patients with unresectable recurrence that responded to chemotherapy and was able to be resected by conversion surgery, the URFS could not be determined. (Fig. 1).

Definitions of relapse-free survival, unresectable relapse-free survival, and cancer-specific survival. BSC, best supportive care; CRC, colorectal cancer; RFS, relapse-free survival; URFS, unresectable relapse-free survival; CSS, cancer-specific survival
Whole-exome sequencing and comprehensive cancer panel
The protocols for the whole-exome sequencing (WES) and comprehensive cancer panel (CCP) were as described previously in detail [6, 14, 15]. All samples were analyzed by WES (mean read depth of approximately 100) and CCP, which is a sequencing panel targeting 409 genes, including genes considered important in CRC, with a high read depth (mean read depth of > 1000). The results from WES and CCP were combined. Driver gene mutations were classified as described in a previous study [5] according to the predicted effect of the mutation: Tier 1, a driver mutation; Tier 2, likely to be a driver mutation; Tier 3, predicted to be a driver mutation; Tier 4, a nonsynonymous mutation; and Tier 5, a silent mutation. In the present study, Tier 1 and Tier 2 mutations were considered driver mutations. Gene mutations with a frequency of less than 10% were omitted from the univariate and multivariate analyses because low-frequency gene mutations may be significantly different by chance. Since RAS has already been reported as a prognostic factor for resectable CRLM, RAS was analyzed by subtype. Microsatellite instability (MSI)-high was defined as reported previously [6].
Outcome variables
Data on the patient characteristics, pathological findings, genetic characteristics, and postoperative prognosis were collected. The primary tumor T stage and N stage were defined according to the tumor node metastasis (TNM) classification. RFS, URFS, and CSS rates were evaluated as long-term outcomes.
Statistical analysis
Categorical variables are expressed as numbers and percentages. Continuous variables are expressed as median values and ranges. Fisher’s exact test or the Chi-square test was used to assess categorical variables, and the Mann–Whitney U test was used to compare continuous variables between two groups. When data, such as CEA and CA19-9 data, were available from before colorectal resection and before hepatectomy, the data obtained before hepatectomy were used. The RFS, URFS, and CSS rates were calculated from the time of curative surgery using the Kaplan–Meier method. Univariate and multivariate analyses of the pre-hepatectomy factors that potentially influence the RFS, URFS, and CSS were performed using a Cox proportional hazard regression model with a backward stepwise selection. Risk factors showing values of p < 0.05 in the univariate analyses were included in the multivariate analysis. Differences were considered significant at p < 0.05. Statistical analyses were performed using R (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinicopathological characteristics
A total of 151 consecutive patients with resectable CRLOM underwent curative-intent surgery. The following patients were excluded: those who had received neoadjuvant chemotherapy and/or radiotherapy (n = 27); those without genetic analysis data (n = 10); those with multiple cancers (n = 7); those with synchronous CRC (n = 5); and those with familial adenomatous polyposis (n = 1). The remaining 101 patients were included in the final analyses (Supplemental Fig. S1).
Table 1 summarizes the clinicopathological characteristics of the 101 patients. The median age was 64 years (range, 27–86 years) and 69 patients (68%) were male. Eight patients (8%) underwent simultaneous resection. The primary tumor was right colon cancer, left colon cancer, and rectal cancer in 25 (25%), 31 (31%), and 45 (45%) patients, respectively. Most patients had pT3 or deeper tumors and LN metastasis. The median number of CRLOM was 2 (range, 1–19) and the median maximum size of the CRLOM was 27 mm (range, 6–122 mm). Thirty-two patients (32%) had bilateral lesions, 73 patients (72%) had synchronous CRLOM, and 39 patients (39%) underwent major hepatectomy. Among the patients with synchronous CRLOM, the median duration between colorectal resection and hepatectomy was 48 days (range, 0–95 days). Thirty-seven patients (37%) received adjuvant chemotherapy after hepatectomy.
Gene mutation profiling of primary tumors
Figure 2 shows the results of the primary tumor molecular profiling. Mutations were found most frequently in APC, TP53, and RAS. Driver mutations (Tier 1 or 2 mutations) overlapped with Tier 3 or 4 mutations in some patients. APC mutations were detected in 80 patients (79.2%), 79.2% of whom had driver mutations and 1.0% had Tier 3 or 4 mutations (one patient had both a driver mutation and a Tier 3 or 4 mutation). TP53 mutations were detected in 74 patients (73.3%), 64.4% of whom had driver mutations and 9.9% had Tier 3 or 4 mutations (one patient had both a driver mutation and a Tier 3 or 4 mutation). RAS mutations were detected in 42 patients (41.6%), 41.6% of whom had driver mutations and 2.0% had Tier 3 or 4 mutations (two patients had both a driver mutation and a Tier 3 or 4 mutation). In more detail, KRAS mutations were seen in 39 patients (38.6%), 38.6% of whom had driver mutations and 0% had Tier 3 or 4 mutations, NRAS mutations were seen in 4 patients (4.0%), 3.0% of whom had driver mutations and 1.0% had Tier 3 or 4 mutations, and HRAS mutations were seen in 1 patient (1.0%), 0% of whom had driver mutations and 1.0% had Tier 3 or 4 mutations. Figure 2 shows the KRAS mutations according to the gene base status. Highly frequent mutations were KRAS G12D, seen in 12 patients (12.0%); KRAS G13D, seen in 9 patients (8.9%); KRAS G12V, seen in 6 patients (5.9%); KRAS G12C, seen in 4 patients (4.0%), and KRAS G12S, seen in 4 patients (4.0%). The other mutations were seen in one patient each.

Primary tumor molecular profiling and clinicopathological factors. From top to bottom: the survival events, clinicopathologic factors, tumor mutation burden (TMB) in the primary tumor, microsatellite instability (MSI) in the primary tumor, and a table of genetic mutations in the primary tumor. Survival events are shown in reddish brown for relapse, unresectable relapse, and death. Genetic mutations in the primary tumor are shown in dark green for Tier 1 or 2 mutations (driver mutations), and in light green for Tier 3 or 4 mutations. Three lines were added under RAS for KRAS, NRAS, and HRAS in parentheses. The KRAS mutations are color-coded by gene base status, and the frequency of each is labeled. CA19-9, carbohydrate antigen 19–9, CEA, carcinoembryonic antigen
In addition to the three major mutations listed above, other driver mutations found at a high frequency were mutations in FBXW7, seen in 14 patients (13.9%) 10.9% of whom had driver mutations and 4.0% had Tier 3 or 4 mutations (one patient had both a driver mutation and a Tier 3 or 4 mutation); and PIK3CA, which was seen in 12 patients (11.9%) 6.9% of whom had driver mutations and 5.0% had Tier 3 or 4 mutations. Tier 3 or 4 mutations found at a high frequency were mutations in TTN, seen in 33 patients (32.7%), SYNE1, seen in 14 patients (13.9%), RYR2, seen in 13 patients (12.9%), PKHD1, seen in 12 patients (11.9%), FLG, seen in 11 patients (10.9%), CSMD3, seen in 10 patients (9.9%), MUC16, seen in 10 patients (9.9%), and PCDH17, seen in 10 patients (9.9%).
The median tumor mutation burden in the primary tumors was 3.0 mutations/Mb (range, 0.2–6.3 mutations/Mb). Six patients showed MSI-high, but neither BRAF V600E nor Lynch syndrome was identified in any of these patients.
Long-term outcomes
The median follow-up was 47 months (range, 10–87 months). The 3-year RFS, URFS, and CSS rates were 37.2%, 61.9%, and 81.2%, respectively (Supplemental Fig. S2). Among the 63 first recurrences, 53 patients had hematogenous recurrences, of which 37 (70%) were resectable. Five LN metastases and five disseminated recurrences were unresectable. Only one patient did not die from CRC. The median interval from the first hepatectomy to the first relapse, unresectable relapse, and death was 8.1, 12.4, and 27.6 months, respectively.
Prognostic factors
Table 2 summarizes the results of the univariate and multivariate analyses for each long-term outcome. The multivariate analysis results showed that KRAS G12D mutation-positivity (hazard ratio (HR): 7.69; 95% confidence interval (95% CI): 3.44–17.2; p < 0.01), RYR2 mutation-positivity (HR: 4.03; 95% CI: 1.68–9.68; p < 0.01), KRAS G12S mutation-positivity (HR: 3.96; 95% CI: 1.13–13.9; p = 0.03), CA19-9 level of > 37 U/ml before hepatectomy (HR: 3.62; 95% CI: 1.76–7.42; p < 0.01), and primary tumor pN2 stage (HR: 3.22; 95% CI: 1.12–9.27; p = 0.03) were significantly associated with a poor URFS. The multivariate analysis results also revealed that KRAS G12V mutation-positivity (HR: 4.65; 95% CI: 1.77–12.2; p < 0.01), KRAS G12D mutation-positivity (HR: 3.14; 95% CI: 1.56–6.35; p < 0.01), KRAS G12S mutation-positivity (HR: 3.06; 95% CI: 1.05–8.88; p = 0.04), and CA19-9 level of > 37 U/ml before hepatectomy (HR: 2.57; 95% CI: 1.51–4.37; p < 0.01) were significant predictors of RFS. Moreover, the multivariate analysis results revealed that the maximum size of the primary tumor < 30 mm (HR: 18.6; 95% CI: 3.42–103; p < 0.01), the primary tumor pT4 stage (HR: 9.12; 95% CI: 2.52–33.0; p < 0.01), and KRAS G12D mutation-positivity (HR: 7.55; 95% CI: 2.65–21.5; p < 0.01) were significant predictors of the CSS.
Statuses of specific RAS mutations and RYR2 mutations, and long-term outcomes
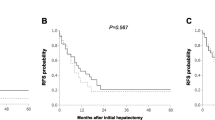
We examined the long-term outcomes for the RAS and RYR2 mutations, which were identified as significant prognostic factors, according to the gene base status. Figure 3 summarizes the 3-year RFS, URFS, and CSS rates for specific RAS statuses. KRAS G12D showed the second-worst 3-year RFS rate (8%), the worst 3-year URFS rate (8%), and the worst 3-year CSS rate (42%). KRAS G12S showed the worst 3-year RFS rate (0%) and the second-worst 3-year URFS rate (25%) and CSS rate (75%). KRAS G12V showed the third-worst 3-year RFS rate (17%), URFS rate (50%), and CSS rate (83%). Since the RYR2 mutations were all distinct mutations, the long-term outcomes could not be determined.

Relapse-free survival, unresectable relapse-free survival, and cancer-specific survival for specific RAS mutations. RFS, relapse-free survival; URFS, unresectable relapse-free survival; CSS, cancer-specific survival
Clinicopathological and genetic factors in the unresectable cases
Supplemental Table S1 shows the clinicopathological and genetic factors of the 37 patients who had unresectable recurrence at 3 years. Twelve patients were positive for the primary KRAS G12D mutation, 11 of whom eventually had unresectable recurrence. Seven patients had multiple and diffusely distributed hepatic and pulmonary metastases, which were deemed unresectable because of insufficient predicted residual liver and lung function. The diffuse distribution of metastases was a less common reason for unresectability in patients with other mutations and in wild-type cases.
Discussion
Little evidence exists regarding the usefulness of performing curative surgery alone or in combination with preoperative chemotherapy [16]. In our institution, curative surgery is generally performed for CRLM without preoperative treatment. While previous reports have included patients undergoing R1 resection, those who received preoperative treatment, and those with extrahepatic disease [17], we excluded these patients from the present study to enable us to more accurately determine whether upfront surgery affects the risk of unresectable recurrence. The present study identified, for the first time, that specific KRAS mutations, RYR2 mutations, and the maximum size of the primary tumor were prognostic factors.
Although many studies have reported RAS mutations to be a negative prognostic factor for RFS and OS [18], only one study has shown that KRAS was associated with a worse URFS [19]. There are several key differences between the past studies and the present study: first, the past reports included cases of R1 resection, whereas the present study included only cases with R0 resection; second, the past studies included only KRAS mutations in codon 12 or 13, whereas the present study included all RAS mutations; and third, the past studies included preoperative treatment in half of the cases, whereas the present study excluded all preoperative treatments.
The present study is the first to show that KRAS G12D, KRAS G12S, and KRAS G12V are significantly associated with a poor prognosis for patients with CRLOM. Two previous papers have reported relationships between specific KRAS mutation statuses and the prognosis of resectable CRLM [17, 20]. Other studies have examined only a limited number of mutations, such as those in KRAS codons 12, 13, and 61, whereas in the present study, we investigated all mutations using next-generation sequencing. The distributions of specific RAS mutations in CRLOM were similar between our study and the TCGA dataset [21]. Examining all mutations allowed us to classify the wild-type genes accurately, and therefore, to assess the prognosis associated with each subtype of RAS mutations accurately. The results showed that unresectable recurrence was more prevalent in patients with a mutation in KRAS codon 12. A previous in vitro study found that patients with KRAS codon 12 gene mutations exhibited more aggressive tumor activity than those with KRAS codon 13 mutations because of the differences in the threshold for apoptosis induction [22]. Another study showed that KRAS codon 12 mutations are associated with the increased upregulation of vascular endothelial growth factor, and more stable bonds between RAS and guanosine triphosphate [23].
KRAS G12D, the most frequent subtype, was the worst prognostic factor for the URFS, and was also a significantly poor prognostic factor for RFS and CSS. KRAS G12D appears to be the most common (28%) mutation in patients with CRC [21]. In the present study, KRAS G12D was associated with worse RFS, URFS, and CSS. Notably, the 3-year RFS and URFS were the same, probably because almost all first relapses are unresectable recurrences, and unresectable relapses often occur soon after the first relapse. Moreover, we found that more than half of the KRAS G12D-positive patients had diffuse liver and lung metastases within a short period after R0 resection (Supplemental Table S1). This suggests that KRAS G12D mutation-positivity might be associated with high malignancy. Even if R0 resection is performed, it is possible that micrometastases or small residual lesions may develop aggressively and result in unresectable recurrence. However, to date, there have been no basic studies reported on KRAS G12D mutation-specific or RAS subtype-specific malignancies.
Since KRAS G12S is associated with a worse RFS and URFS, and it appears to be associated with unresectable relapse, treatment interventions, such as preoperative or postoperative chemotherapy, should be considered if a KRAS G12D mutation is identified using tissue from the initial surgery. However, preoperative and postoperative chemotherapy after curative resection of CRLM remains controversial because a randomized controlled trial showed that it could improve RFS, but not OS [14, 17].
Over the last few years, KRAS inhibitors have gained much attention. Mutated KRAS protein had been deemed “undruggable” for many decades due to its high affinity for guanosine triphosphate and its lack of accessible binding pockets [24]. However, recently, structural analyses of mutant KRAS proteins have led to the identification of a pocket that is useful for drug binding, and the development of direct KRAS inhibitors utilizing this pocket is ongoing [25]. A selective KRAS G12D inhibitor was recently identified as a potent noncovalent, selective inhibitor that suppresses KRAS G12D signaling in cells in vitro and in vivo, and the antitumor benefits of this agent were demonstrated in an animal model [26]. Further clinical trials of potential KRAS G12D treatments are expected.
In summary, identifying specific RAS mutations may help not only to individualize therapeutic regimens, but also to guide follow-up strategies for patients with resected CRLOM. RYR2 mutation-positivity was associated with poor URFS. Unlike RAS mutations, which are Tier 1 mutations, RYR2 mutations were all Tier 4 mutations. Recent studies have demonstrated significantly mutated RYR2 in several cancers [27,28,29]. While no studies have evaluated the associations between RYR2 mutations and the prognosis of CRC, a previous investigation demonstrated that RYR2 mutations were a favorable prognostic biomarker for breast, esophageal, and lung cancers [28, 29]. In contrast, RYR2 mutations worsened the prognosis of resectable CRLOM. Thus, the association between RYR2 mutations and the prognosis for resectable CRLOM warrants further investigation.
The prognostic clinicopathological factors seen in the present study were similar to those reported previously [9], except for one: the relationship between the maximum size of the primary tumor and the CSS. Generally, a larger tumor size is associated with a worse prognosis. However, in the present study, counterintuitively, tumors with a median diameter of < 30 mm were more likely to lead to a rapid worsening of the prognosis. We speculate that metastasis occurring even when the primary tumor is small might be highly malignant and progress enough to worsen the 3-year CSS rate. Other than the CEA and CA19-9 levels, the pre-hepatectomy CRLOM factors had little impact on the prognosis of resectable CRLOM. In contrast, the primary tumor pT stage, pN stage, and gene mutations had a large impact on the prognosis. CRLOM has a better prognosis than other distant metastases because multiple repeat hepatectomies are often possible for liver metastases, whereas multiple repeat resections are usually not feasible for other distant metastases.
Several limitations of this study must be kept in mind when considering the results. First, this was a retrospective study with the potential inclusion of several selection biases. However, we tried to minimize the prognostic discrepancies by excluding patients with extrahepatic metastasis and R1/R2 resection. Second, this study was conducted in a well-equipped hospital where difficult surgeries that may be considered unfeasible in general hospitals could be performed. However, all technically resectable recurrences were resected in this study, improving the accuracy of our results. Third, because of the small numbers of the specific RAS mutation subtypes examined, the results may be unreliable. Data from more patients need to be accumulated in the future.
In conclusion, this is the first study to identify that specific KRAS mutations, RYR2 mutations, and the maximum size of the primary tumor are prognostic factors for CRLOM. In daily clinical practice, awareness of the subtypes of RAS gene mutations is important, rather than simple determination of their presence or absence. The prognostic factors identified in this study may be useful in clinical practice and may enable surgeons to provide optimal and personalized treatment options for patients with CRLOM in the future.
References
Hackl C, Neumann P, Gerken M, Loss M, Klinkhammer-Schalke M, Schlitt HJ. Treatment of colorectal liver metastases in Germany: a ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer. 2014;14:810.
Oba M, Hasegawa K, Shindoh J, Yamashita S, Sakamoto Y, Makuuchi M, et al. Survival benefit of repeat resection of successive recurrences after the initial hepatic resection for colorectal liver metastases. Surgery. 2016;159:632–40.
Tsilimigras DI, Ntanasis-Stathopoulos I, Bagante F, Moris D, Cloyd J, Spartalis E, et al. Clinical significance and prognostic relevance of KRAS, BRAF, PI3K and TP53 genetic mutation analysis for resectable and unresectable colorectal liver metastases: a systematic review of the current evidence. Surg Oncol. 2018;27:280–8.
Sawada Y, Sahara K, Endo I, Sakamoto K, Honda G, Beppu T, et al. Long-term outcome of liver resection for colorectal metastases in the presence of extrahepatic disease: a multi-institutional Japanese study. J Hepatobiliary Pancreat Sci. 2020;27:810–8.
Yamaguchi K, Urakami K, Ohshima K, Mochizuki T, Akiyama Y, Uesaka K, et al. Implementation of individualized medicine for cancer patients by multiomics-based analyses-the Project HOPE. Biomed Res. 2014;35:407–12.
Nagashima T, Yamaguchi K, Urakami K, Shimoda Y, Ohnami S, Ohshima K, et al. Japanese version of The Cancer Genome Atlas, JCGA, established using fresh frozen tumors obtained from 5143 cancer patients. Cancer Sci. 2020;111:687–99.
Watanabe T, Itabashi M, Shimada Y, Tanaka S, Ito Y, Ajioka Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer. Int J Clin Oncol. 2015;20:207–39.
Hashiguchi Y, Muro K, Saito Y, Ito Y, Ajioka Y, Hamaguchi T, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 2020;25:1–42.
Yamaguchi T, Kinugasa Y, Shiomi A, Kagawa H, Yamakawa Y, Furuatni A, et al. Short- and long-term outcomes of robotic-assisted laparoscopic surgery for rectal cancer: results of a single high-volume center in Japan. Int J Colorectal Dis. 2018;33:1755–62.
Hino H, Yamaguchi T, Kinugasa Y, Shiomi A, Kagawa H, Yamakawa Y, et al. Robotic-assisted multivisceral resection for rectal cancer: short-term outcomes at a single center. Tech Coloproctol. 2017;21:879–86.
Yamaoka Y, Shiomi A, Kagawa H, Hino H, Manabe S, Kato S, et al. Robotic surgery for clinical T4 rectal cancer: short- and long-term outcomes. Surg Endosc. 2022;36:91–9.
Ito T, Sugiura T, Okamura Y, Yamamoto Y, Ashida R, Uesaka K. The impact of posthepatectomy liver failure on long-term survival after hepatectomy for colorectal liver metastasis. HPB (Oxford). 2019;21:1185–93.
Kanemitsu Y, Shimizu Y, Mizusawa J, Inaba Y, Hamaguchi T, Shida D, et al. Hepatectomy followed by mFOLFOX6 versus hepatectomy alone for liver-only metastatic colorectal cancer (JCOG0603): a phase II or III randomized controlled trial. J Clin Oncol. 2021;39:3789–99.
Shimoda Y, Nagashima T, Urakami K, Tanabe T, Saito J, Naruoka A, et al. Integrated next-generation sequencing analysis of whole exome and 409 cancer-related genes. Biomed Res. 2016;37:367–79.
Nagashima T, Shimoda Y, Tanabe T, Naruoka A, Saito J, Serizawa M, et al. Optimizing an ion semiconductor sequencing data analysis method to identify somatic mutations in the genomes of cancer cells in clinical tissue samples. Biomed Res. 2016;37:359–66.
Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14:1208–15.
Margonis GA, Kim Y, Spolverato G, Ejaz A, Gupta R, Cosgrove D, et al. Association between specific mutations in KRAS Codon 12 and colorectal liver metastasis. JAMA Surg. 2015;150:722–9.
Pikoulis E, Papaconstantinou D, Pikouli A, Wang J, Theodoridis C, Margonis GA. Reevaluating the prognostic value of RAS mutation status in patients with resected liver metastases from colorectal cancer: a systematic review and meta-analysis. J Hepatobiliary Pancreat Sci. 2021;28:637–47.
Shindoh J, Nishioka Y, Yoshioka R, Sugawara T, Sakamoto Y, Hasegawa K, et al. KRAS mutation status predicts site-specific recurrence and survival after resection of colorectal liver metastases irrespective of Location of the Primary Lesion. Ann Surg Oncol. 2016;23:1890–6.
Margonis GA, Kim Y, Sasaki K, Samaha M, Amini N, Pawlik TM. Codon 13 KRAS mutation predicts patterns of recurrence in patients undergoing hepatectomy for colorectal liver metastases. Cancer. 2016;122:2698–707.
Chuang SC, Huang CW, Chen YT, Ma CJ, Tsai HL, Chang TK, et al. Effect of KRAS and NRAS mutations on the prognosis of patients with synchronous metastatic colorectal cancer presenting with liver-only and lung-only metastases. Oncol Lett. 2020;20:2119–30.
Guerrero S, Casanova I, Farre L, Mazo A, Capella G, Mangues R. K-ras codon 12 mutation induces higher level of resistance to apoptosis and predisposition to anchorage-independent growth than codon 13 mutation or proto-oncogene overexpression. Cancer Res. 2000;60:6750–6.
Renaud S, Guerrera F, Seitlinger J, Costardi L, Schaeffer M, Romain B, et al. KRAS exon 2 codon 13 mutation is associated with a better prognosis than codon 12 mutation following lung metastasectomy in colorectal cancer. Oncotarget. 2017;8:2514–24.
Forbes SA, Bindal N, Bamford S, Cole C, Kok CY, Beare D, et al. COSMIC: mining complete cancer genomes in the Catalogue of Somatic Mutations in Cancer. Nucleic Acids Res. 2011;39:D945–50.
Lito P, Solomon M, Li LS, Hansen R, Rosen N. Allele-specific inhibitors inactivate mutant KRAS G12C by a trapping mechanism. Science. 2016;351:604–8.
Wang X, Allen S, Blake JF, Bowcut V, Briere DM, Calinisan A, et al. Identification of MRTX1133, a Noncovalent, Potent, and Selective KRAS(G12D) Inhibitor. J Med Chem. 2022;65:3123–33.
Wolff RK, Hoffman MD, Wolff EC, Herrick JS, Sakoda LC, Samowitz WS, et al. Mutation analysis of adenomas and carcinomas of the colon: early and late drivers. Genes Chromosomes Cancer. 2018;57:366–76.
Xu Z, Xiang L, Wang R, Xiong Y, Zhou H, Gu H, et al. Bioinformatic analysis of immune significance of RYR2 mutation in breast cancer. Biomed Res Int. 2021;2021:8072796.
Wang Y, Chen Y, Zhang L, Xiong J, Xu L, Cheng C, et al. Ryanodine receptor (RYR) mutational status correlates with tumor mutational burden, age and smoking status and stratifies non-small cell lung cancer patient prognosis. Transl Cancer Res. 2022;11:2070–83.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
595_2024_2900_MOESM1_ESM.tif
Supplementary file1 (TIF 100 KB)Fig. S1 Patient selection. CRLOM: colorectal liver-only metastasis, CRC: colorectal cancer
595_2024_2900_MOESM2_ESM.tif
Supplementary file2 (TIF 80 KB)Fig. S2 Relapse-free survival, unresectable relapse-free survival, and cancer-specific survival. RFS: relapse-free survival, URFS: unresectable relapse-free survival, CSS: cancer-specific survival
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chen, K., Okamura, Y., Hatakeyama, K. et al. The KRAS G12D mutation increases the risk of unresectable recurrence of resectable colorectal liver-only metastasis. Surg Today (2024). https://doi.org/10.1007/s00595-024-02900-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00595-024-02900-3