
Abstract
Purpose
This study reviews our 17-year experience of managing blunt traumatic aortic injury (BTAI).
Methods
We analyzed information collected retrospectively from a tertiary trauma center.
Results
Between October 1995 and June 2012, 88 patients (74 male and 14 female) with a mean age of 39.9 ± 17.9 years (range 15–79 years) with proven BTAI were enrolled in this study. Their GCS, ISS, and RTS scores were 12.9 ± 3.7, 29.2 ± 9.8, and 6.9 ± 1.4, respectively. Twenty-one (23.8 %) patients were managed non-operatively, 49 (55.7 %) with open surgical repair, and 18 (20.5 %) with endovascular repair. The in-hospital mortality rate was 17.1 % (15/81) and there were no deaths in the endovascular repair group. The mean follow-up period was 39.9 ± 44.2 months. The survivors of blunt aortic injury had lower ISS, RTS, TRISS, and serum creatinine level and lower rate of massive blood transfusion, shock, and intubation than the patients who died, despite higher rates of endovascular repair, hemoglobin, and GCS on presentation. The degree of aortic injury, different therapeutic options, GCS, shock presentation, and intubation on arrival all had significant impacts on outcome.
Conclusions
Shock, aortic injury severity, coexisting trauma severity, and different surgical approaches impact survival. Endovascular repair achieves a superior mid-term result and is a reasonable option for treating BTAI.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Blunt traumatic aortic injury (BTAI) is the second leading cause of death, after head injury, from vehicle crashes [1, 2]. The fact that most victims die before arriving at the hospital is attributable to massive bleeding from the injured aorta. In 1958, Parmley reported an 85 % pre-hospital mortality for patients with BTAI [3]. However, this has decreased remarkably by improved motor vehicle safety, pre-hospital resuscitation, as well as traumatology and imaging techniques promoting the early detection of blunt aortic injury at experienced trauma centers [1, 4–6].
Traditionally, BTAI was repaired surgically with graft interposition under cardiopulmonary bypass, usually a few days after the traumatic event [7–9]. However, major complex operations and systemic heparinization can exacerbate other associated injuries such as head, intra-abdominal, and lung injuries [1, 7, 10]. Historically, open surgical repair of BTAI carries a 28 % mortality rate and a 16 % paraplegia rate [1, 11]. Endovascular aortic repair has emerged as the treatment of choice for aortic pathology because it is less invasive, and has been available in our country since 2006. Endovascular repair of BTAI can render unnecessary the posterolateral thoracotomy and cardiopulmonary bypass required by traditional open surgery. [7, 10, 12] Furthermore, the aortic stent graft can be deployed in the secondary triage of major trauma, along with coagulation and massive transfusion. Thus, the Food and Drug Administration (FDA) has approved no specific graft for acute BTAI to date and the off-label use of commercially available stents is very common worldwide [1, 13]. We review our 17-year experience in treatment modalities for BTAI and examine the factors that influence survival.
Patients and methods
Patients
This retrospective study was conducted after obtaining the approval of our institutional review board (IRB). Patients with a typical aortic lesion caused by blunt trauma between October 1995 and June 2012 were enrolled. The following information was collected: age, gender, mechanism of trauma, presenting symptoms, associated injuries, initial vital signs and laboratory test results, diagnostic tools, Glasgow Coma Scale (GCS), Injury Severity Score (ISS), Revised Trauma Score (RTS), survival probability according to the Trauma and Injury Severity Score (TRISS), time to diagnosis and surgery, surgical procedures (non-operative, open surgery, and endovascular aortic repair), degree of aortic injury rupture, hospital events, and final outcome.
Therapeutic strategy
Either traditional open surgery or endovascular intervention was attempted once BTAI was proven, unless the patient was at extremely high risk or the aortic lesion was very minor. Most open surgeries for aortic lesions were scheduled 3–7 days after major trauma if there was no free rupture or involvement of the ascending aorta. Traditional open surgery was done with a double-lumen endotracheal tube under general anesthesia. Left posterolateral thoracotomy was the preferred incision and the repair was generally carried out under full cardiopulmonary bypass support (Sarns 8000 Heart–Lung Bypass, DRE Inc. Louisville KY, US) and deep hypothermic circulatory arrest. Sternotomy was performed only for patients with blunt injury involving the ascending aorta. All patients, including those treated non-operatively, were admitted to the intensive care unit for at least 48 h to monitor late bleeding, rupture, ventricular arrhythmia, and deterioration of concomitant trauma.
Endovascular aortic repair
Endovascular repair has been available at our institution since 2006. All patients had preoperative imaging done as a contrast CT angiography of the chest and abdomen. Evaluation for suitability of endovascular aortic repair included aortic morphology, aortic arch involvement, and size of the thoracic/abdominal aorta and iliac arteries. All procedures were performed in the operating room, typically through open femoral arteries. Adjunctive surgical procedures, including thoracic aortic debranching procedure of the innominate, carotid, or subclavian arteries, were performed at the same time as the endovascular procedures.
Statistical analysis
All data were entered into an Excel spreadsheet (Excel 2007, Microsoft Inc. USA) and analyzed using STATA software, version 8.0 (Stata Corporation, College Station, TX). Categorical variables were reported as frequencies, and all continuous variables were calculated as mean ± standard deviation. Continuous data were compared using a one-sample t test for paired data and a two-sample t test for unpaired data, when appropriate. Categorical data were compared using the \(\chi ^{2}\) test. Non-parametrical tests were applied to data not following a normal distribution. A significance level of 5 % was applied when comparing differences. Cox regression analysis was used to compare different influences on mortality among the study groups, adjusting for sex, age, TRISS, and aortic injury type. The adjusting variables were selected according to their clinical relevance in patients with multisystem trauma and to previously published literature. Adjusted hazard ratio, 95 % confidence intervals, and p values were derived.
Results
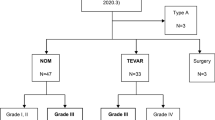
The subjects of this study were 88 patients with documented evidence of BTAI, who were admitted to a tertiary trauma center between October 1995 and June 2012. Table 1 summarizes the patients’ characteristics, comparing the treatment subgroups of non-operative treatment, traditional open surgery, and endovascular aortic repair. The features analyzed include injury mechanisms, timing, arrival status, presenting symptoms, biochemistry, injury severity, hospital course, and follow-up interval. There were 74 men and 14 women, with a mean age of 39.9 ± 17.9 years (range 15–79 years). The injury mechanism was motorbike collision in 46 patients (52.3 %), automobile collision in 23 (26.1 %), auto–pedestrian collision in 5 (5.7 %), and others (falls, bicycle, and crash-over) in 14 (15.9 %).The interval between trauma and arrival at the emergency room (ER) was 5.7 ± 13.9 h, with aortic injury disclosed in 19.1 ± 78.6 h after arriving at the ER. Most patients presented with shock (37/88, 42.1 %) and chest pain (19/88, 21.6 %), although 25 patients had no signs of aortic injury. Fourteen patients (14/88, 15.9 %) left the ER with an endotracheal tube in place and on ventilatory support. Their GCS, ISS, and RTS scores were 12.9 ± 3.7, 29.2 ± 9.8, and 6.9 ± 1.4, respectively. There were 13 (13/88, 14.7 %) patients who required massive transfusion and 15 (17.1 %) who died in hospital. The mean ICU stay, hospital stay, and follow-up time were 3.7 ± 4.1 days, 23.5 ± 21.7 days, and 39.9 ± 44.2 months, respectively. Intervention, including open surgery and endovascular repair, was attempted once blunt aortic injury was proven, except in 21 patients at extremely high risk and/or with only minor aortic lesions (21/88, 23.9 %). Forty-nine patients were treated with open surgery and 18 with endovascular aortic repair. Table 1 compares the three treatment groups (non-operative treatment, open surgery, and endovascular repair). The interval from arrival in ER to diagnosis, hemoglobin on arrival, ventilator support, ISS (Injury Severity Score), TRISS, ICU stay, hospital stay, in-hospital death, and follow-up time differed among the three groups. Table 2 summarizes the aortic injury grading and distribution for the 88 patients. More than 25 % of the aorta were ruptured or contained rupture from BTAI. Intramural hematoma in BTAI (6/7, 85.7 %) trended to be managed non-operatively. Most of the aortic lesions were located in the aortic arch, aortic isthmus, or descending aorta (31.8, 31.8, and 29.5 %, respectively), with few in the ascending aorta (3/88, 3.4 %) and abdominal aorta (3/88, 3.4 %), which tended to be treated with traditional open surgery or non-operative management rather than endovascular aortic repair.
Traditional surgical repair
Forty-nine (49/88, 55.7 %) patients were treated with traditional aortic surgery (Fig. 1). Table 3 summarizes the surgical procedures, application of cardiopulmonary bypass technique, location of the aortic injuries, type of aortic injury, concomitant procedures, death, early complications, and late events. The surgical procedures for blunt traumatic aortic injury included clamp and saw (2), thoracotomy with partial cardiopulmonary bypass support (13), thoracotomy with full cardiopulmonary support in deep hypothermic circulatory arrest (31), and sternotomy (3). Notably, one patient received 5-day ECMO support for traumatic respiratory distress syndrome before undergoing open surgery for the aortic lesion. Two patients were found to have a residual dissecting intimal flap after the aortic surgery, one of whom underwent total arch replacement for her dissecting aortic aneurysms 7 years after the BTAI.

A typical location of aortic injury at the aortic isthmus. This injury was treated by traditional open aortic repair. The patient was a 26-year-old man involved in a vehicle to pedestrian crash. The interval from injury to ER was 3 h and the interval from arrival in ER to diagnosis was 4 h. The aortic surgery was done 17 days after the trauma. He was ventilated for 24 h in the intensive care unit for 5 days and hospitalized for 46 days. a Surgical view via left thoracotomy demonstrated a diffuse hematoma over the distal aortic arch to the descending aorta. The white asterisk indicates the hematoma over the aortic isthmus to the descending aorta. b The aortic lesion was identified after deep hypothermic circulatory arrest under full cardiopulmonary bypass. The black asterisk indicates the focal aortic dissection near the aortic intimal tear at the aortic isthmus. c The proximal aorta was anastomosed with a wovenvascular graft. d The injured aortic isthmus and descending aorta were resected and reconstructed
Endovascular aortic repair
Eighteen of the 88 patients (20.5 %) underwent endovascular aortic repair, which has been a therapeutic option in our institution since 2006 (Fig. 2). Table 3 lists the aortic injury location, aortic injury type, adjuvant aortic procedures, surgical procedures, and late events. We performed aortic stent operations with intended left subclavian artery coverage without revascularization in 11 patients and aortic arch branches manipulation in 6 patients. There was no death in the endovascular aortic repair group and the only complication was left forearm hypo-perfusion, which improved with conservative treatment in one patient.

Typical location of an aortic pseudoaneurysm in the aortic isthmus after blunt chest trauma. This injury was treated via an endovascular approach. The patient was a 31-year-old man who fell from a height of 3 m. The interval from injury to ER was 0.5 h and the interval from arrival in ER to diagnosis was 1 h. The aortic operation was done 27 days after the trauma. The patient was ventilated for 6 h, in the intensive unit care for 1 day, and hospitalized for 31 days. a Preoperative contrast chest tomography (sagittal view) demonstrated a pseudoaneurysm in the aortic isthmus. b Endovascular repair was performed with intended left subclavian arterial coverage. The white arrow shows that the pseudoaneurysm was completely excluded from the aortic blood flow
Comparison of survivors and non-survivors
Table 4 compares the characteristics of the 73 survivors and 15 non-survivors. There were no differences in gender, age, interval between injury, and ER arrival, or between ER arrival and diagnosis. More of the non-survivors had shock on presentation and required a ventilator in ER (p = 0.01), were in a worse conscious status on ER arrival (p = 0.002), had higher RTS (p = 0.001), higher TRISS (p = 0.001), lower hemoglobin and serum creatinine level (p = 0.001), and a greater number of blood transfusions (p < 0.0001). There were no non-survivors among the patients who underwent endovascular aortic repair.
Risk factor analysis
There were 15 in-hospital deaths: 8 in the non-operative group and 7 in the open surgical group. Risk factors potentially affecting in-hospital mortality were tested further through the Cox proportional hazard model (Table 5).Shock had the most profound impact (hazard ratio: 4.47, p = 0.03) on mortality, followed by aortic injury grading (hazard ratio: 2.24, p = 0.02). Higher Glasgow Coma Score (hazard ratio: 0.72, p = 0.001) and different aortic surgery techniques (hazard ratio: 0.22, p = 0.002) also impacted mortality. The survival curves for non-operative treatment, traditional open surgical repair, and endovascular aortic repair differed significantly (p = 0.001; Fig. 3).

Survival examination groups according to the different therapeutic methods
Discussion
A large proportion of the patients with BTAI in this study period died at the scene of injury or did not reach hospital alive. According to a recent autopsy report, 34 % of fatalities resulting from a blunt mechanism had a thoracic aortic injury and 80 % of those patients died at the scene. [14] Moreover, the surviving patients in this series included approximately 5 % who were hemodynamically unstable or deteriorated within 6 h of admission, leading to in-hospital mortality as high as 90 %. Historically, these outcomes led to emergency surgical approach to aortic injuries after blunt trauma. Subsequent studies suggest that some patients with major associated injuries, or even with no severe associated injuries or major comorbidities, can be safely managed with delayed repair, provided blood pressure and contractility are adequately controlled [4, 15, 16]. Delayed repair has been associated with a significant risk-adjusted survival benefit as seen in the Second American Association for the Surgery of Trauma (AAST) trial, regardless of the presence or absence of major associated injuries [2]. In the last decade, thoracic endovascular repair has revolutionized the therapy of descending aortic pathology. This therapeutic approach has been successfully applied in the treatment of BTAI. The prospective second AAST trial evaluated the impact of TEVAR for BTAI across major trauma centers in the USA. The use of TEVAR increased dramatically from 0 to 65 % between the first AAST study in 1997 and the second one in 2007. A comparative analysis in the second AAST study identified a 16 % mortality rate after traditional open surgery versus 9 % after endovascular repair (p = 0.001) [1, 2]. Our experience was consistent with the result of the AAST study, with a 14.3 % mortality rate after traditional open aortic surgery versus 0 % after endovascular repair. TEVAR accounts for 63.3 % (19/30) of all aortic interventions for BTAI since the aortic stented graft became available in our institution in 2006.
Our open surgery group of patients demonstrates the increasing complexity of BTAI and the crucial role of extracorporeal cardiopulmonary circulation. Two patients who were injured at the ascending aorta could only be rescued by cardiopulmonary bypass with deep hypothermic circulatory arrest via median sternotomy. Most of the patients treated with open surgery (46/49, 93.8 %) underwent aorta repair under extracorporeal cardiopulmonary support. One patient even required veno-venous mode extracorporeal life support for his traumatic respiratory distress syndrome. In contrast to the high frequency of clamp-and-sew technique (16 %) in the AAST trial, we used this technique in only 6 % of patients, preferring cardiopulmonary support to prevent uncontrolled bleeding and procedure-related spinal cord ischemia. The higher application of cardiopulmonary bypass and deep hypothermic technique may be why no procedure-related paraplegia occurred in our open surgical group. Notably, two patients were left with a residual aortic intimal flap with dissecting aortic aneurysms, one of whom underwent total aortic arch replacement 7 years after the trauma.
The application of thoracic endovascular aortic repair (TEVAR) for BTAI has seen rapid expansion. The Society for Vascular Surgery (SVS) reviewed 7768 patients and provided therapeutic recommendations on endovascular repair of BTAI, including intervention timing, left subclavian artery (LSA) coverage, the use of prophylactic spinal drainage or general anesthesia, open femoral access control, and follow-up strategy [17]. The mortality rate was lowest for patients who underwent endovascular repair, followed by those who underwent open repair, and then those treated non-operatively (9, 19, and 46 %, respectively). Obviously, there is a selection bias for anatomic suitability, injury severity, and the type of repair chosen in the SVS study and our studies. The mortality rate in the present series was similar to that in the SVS study for endovascular repair, open repair, and non-operative management (0, 14.3, and 38.1 %, respectively).The early results of the second AAST trial demonstrated an alarmingly high risk (20 %) of device-related complications, and included 18 patients (14 %) with endoleak treated by repeat endovascular procedures or endograft explantation with traditional open surgical repair. We did not encounter those complications in our endovascular aortic repair group because of careful selection of patients [2]. If the proximal landing zone for the endografts was uncertain, we chose delayed open surgery over endovascular repair, with the need for a carotid arterial debranching procedure.
The most recent publications on blunt aortic injury focus on the impact of different treatment options, the midterm complication of endovascular aortic repair, diagnosis, and anatomic grading [18–23]. In contrast, the emphasis of this study is on the traumatic demographics, risk factor analysis, and long-term outcomes. Its major limitation was the small retrospective characteristic of heterogeneity of the cohort. Moreover, other significant prognostic factors, including brain injury, pelvic fracture, and coexistent abdominal trauma, could not be well illustrated according to the different management strategies for the BTAI. With such limitations, we attempted to identify variables associated with poor prognosis and the influence of the different therapeutic options. More than 20 % (23.9 %, 21/88) of our patients with BTAI were treated non-operatively and these patients tended to have a greater incidence of shock, more blood transfusion, higher injury severity, and higher mortality than those who underwent open surgery or endovascular repair. Fatalities of patients with BTAI are associated with shock on presentation, ventilator use in the ER, worse consciousness status, higher RTS/TRISS, lower hemoglobin, and more blood transfusions. The Cox proportional hazard model shows shock, aortic injury grade, GCS, and different aortic intervention to be potential risk factors impacting mortality. The durability of endovascular aortic repair, increased risk of re-intervention, and the need for repeated CT follow-up were concerns at the beginning of TEVAR application in the treatment of BTAI [24–26]. Our experience has shown that open repair can still leave residual aortic dissection, necessitating a repeat operation years later. The complications of endovascular aortic repair can be minimized with careful selection and patient-tailored therapeutic strategies. Meanwhile, advances in traumatology, including ventilation manipulation and ERCP in biliary tract injury, and the application of extracorporeal circulation, such as ECLS support and conventional ascending aortic replacement, should be made widely available to help manage patients with complicated BTAI [27–29].
Conclusion
BTAI continues to be a challenge in contemporary trauma care. This study analyzes the clinical presentation, traumatic severity, diagnostic tools, outcomes of different interventions, and predictors of mortality in a cohort of patients with BTAI. Shock, aortic injury severity, coexisting trauma severity, and different therapeutic approaches impact survival. Endovascular repair has a good mid-term result and is a reasonable option for treating BTAI.
References
Neschis DG, Scalea TM, Flinn WR, Griffith BP. Blunt Aortic Injury. N Engl J Med. 2008;359:1708–16.
Demetriades D, Velmahos GC, Scalea TM, Jurkovich GJ, Karmy-Jones R, Teixeira PG, et al. Diagnosis and treatment of blunt thoracic aortic injuries: changing perspectives. J Trauma Inj Infect Crit Care. 2008;64:1415–9.
Parmeley LF, Mattingly TW, Manion WC, Jahnke EJ. Nonpenetrating traumatic injury of the aorta. Circulation. 1958;17:1086–101.
Estrera AL, Gochnour DC, Azizzadeh A, Miller CC, Coogan S, Charlton-Ouw K, et al. Progress in the treatment of blunt thoracic aortic injury: 12-year single-institution experience. ATS. 2010;90:64–71.
Forman MJ, Mirvis SE, Hollander DS. Blunt thoracic aortic injuries: CT characterisation and treatment outcomes of minor injury. Eur Radiol. 2013;23:2988–95.
Harris DG, Drucker CB, Brenner ML, Sarkar R, Narayan M, Crawford RS. Patterns and management of blunt abdominal aortic injury. Ann Vasc Surg. 2013;27:1074–80.
Di Eusanio M, Folesani G, Berretta P, Petridis FD, Pantaleo A, Russo V, et al. Delayed management of blunt traumatic aortic injury: open surgical versus endovascular repair. Ann Thorac Surg. 2013;95:1591–7.
Sincos IR, Aun R, Belczak SQ, Nascimento LD, Mioto NB, Casella I, et al. Endovascular and open repair for blunt aortic injury, treated in one clinical institution in Brazil: a case series. Clinics. 2011;66:267–74.
Watson J, Slaiby J, Garcia-Toca M, Marcaccio EJ, Chong TT. A 14-year experience with blunt thoracic aortic injury. J Vasc Surg. 2013;58:380–5.
Kitagawa RS, Van Haren RM, Yokobori S, Cohen D, Beckerman SR, Ahmad F, et al. Management of simultaneous traumatic brain injury and aortic injury. J Neurosurg. 2013;119:324–31.
Lebl DR, Dicker RA, Spain DA, Brundage SI. Dramatic shift in the primary management of traumatic thoracic aortic rupture. Arch Surg. 2006;141:177–80.
Klima DA, Hanna EM, Christmas AB, Huynh TT, Etson KE, Fair BA, et al. Endovascular graft repair for blunt traumatic disruption of the thoracic aorta: experience at a nonuniversity hospital. Am Surg. 2013;79:594–600.
Demetriades D, Velmahos GC, Scalea TM, Jurkovich GJ, Karmy-Jones R, Teixeira PG, et al. Operative repair or endovascular stent graft in blunt traumatic thoracic aortic injuries: results of an American Association for the surgery of trauma multicenter study. J Trauma Inj Infect Crit Care. 2008;64:561–71.
Prijon T, Ermenc B. Classification of blunt aortic injuries a new systematic overview of aortic trauma. Forensic Sci Int. 2010;195:6–9.
Hilgenberg AD, Logan DL, Akins CW, Buckley MJ, Daggett WM, Vlahakes GJ, et al. Blunt injuries of the thoracic aorta. ATS. 1992;53:233–9.
Hemmila MR, Arbabi S, Rowe SA, Brandt M-M, Wang SC, Taheri PA, et al. Delayed repair for blunt thoracic aortic injury: is it really equivalent to early repair? J Trauma Inj Infect Crit Care. 2004;56:13–23.
Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the society for vascular surgery. YMVA. 2011;53:187–92.
Cheng D, Martin J, Shennib H, Dunning J, Muneretto C, Schueler S, et al. Endovascular aortic repair versus open surgical repair for descending thoracic aortic disease. JAC. 2010;55:986–1001.
Garcia-Toca M, Naughton PA, Matsumura JS, Morasch MD, Kibbe MR, Rodriguez HE, et al. Endovascular repair of blunt traumatic thoracic aortic injuries: seven-year single-center experience. Arch Surg. 2010;145:679–83.
Brinster DR. Endovascular repair of blunt thoracic aortic injuries. YSTCS. 2011;21:393–8.
Farber MA, Mendes RR. Endovascular repair of blunt thoracic aortic injury: techniques and tips. YMVA. 2009;50:683–6.
Sepehripour AH, Ahmed K, Vecht JA, Anagnostakou V, Suliman A, Ashrafian H, et al. Management of the Left Subclavian Artery during Endovascular Stent Grafting for Traumatic Aortic Injury e A Systematic Review. Eur J Vasc Endovasc Surg. 2011;41:758–69.
Xenos ES, Minion DJ, Davenport DL, Hamdallah O, Abedi NN, Sorial EE, et al. Endovascular versus open repair for descending thoracic aortic rupture: institutional experience and meta-analysis. Eur J Cardiothorac Surg. 2009;35:282–6.
Patel HJ, Hemmila MR, Williams DM, Diener AC, Deeb GM. Late outcomes following open and endovascular repair of blunt thoracic aortic injury. YMVA. 2011;53:615–21.
Martinelli O, Malaj A, Gossetti B, Bertoletti G, Bresadola L, Irace L. Late outcomes in the emergency endovascular repair of blunt thoracic aortic injuries. J Vasc Surg. 2013;58(3):832–5.
Watanabe Ken-ichi, Fukuda Ikuo, Asari Yasushi. Management of traumatic aortic rupture. Surg Today. 2013;43:1339–46.
Kao KC, Tsai YH, Wu YK, Huang CT, Shih MJ, Huang CC. High frequency oscillatory ventilation for surgical patients with acute respiratory distress syndrome. J Trauma Inj Infect Crit Care. 2006;61:837–43.
Huang YK, Liu KS, Lu MS, Wu MY, Tsai FC, Lin PJ. Extracorporeal life support in post-traumatic respiratory distress patients. Resuscitation. 2009;80:535–9.
Lin BC, Chen RJ, Fang JF, Hsu YP, Kao YC, Kao JL. Management of blunt major pancreatic injury. J Trauma Inj Infect Crit Care. 2004;56:774–8.
Acknowledgments
This study was supported in part by the National Science Council of the Republic of China, Taiwan (Contract Nos. NSC 103-2314-B-182A-073-MY2) and the Chang-Gung Memorial Hospital (Contract Nos. CMRPG380841, CMRPG6B0501 and CMRPG6C0341).
Conflict of interest
Huang Yao-Kuang and the other coauthors have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lin, CC., Liu, KS., Chen, HW. et al. Blunt aortic injury: risk factors and impact of surgical approaches. Surg Today 46, 188–196 (2016). https://doi.org/10.1007/s00595-015-1152-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-015-1152-0