
Abstract
Aims
This study aimed to determine the trajectory of diabetic vascular diseases and to investigate the association between vascular diseases and dementia.
Methods
We included adults aged ≥ 50 years with newly diagnosed type 2 diabetes (n = 173,118) from 2001 to 2005 who were followed-up until December 31, 2013 in the Taiwan’s National Health Insurance Research Database. Multivariable Cox regression models were constructed to estimate hazard ratios (HRs) and confidence limits (CLs) for all-cause dementia in relation to the number, types, and occurrence patterns of vascular disease.
Results
Within 1 year of diabetes diagnosis, 26.3% of adults developed their first vascular disease. During the 1,864,279 person-years of follow-up, 17,426 adults had all-cause dementia, corresponding to an incidence of 97.9 cases/10,000 person-years in 127,718 adults with at least one vascular disease and 67.5 cases/10,000 person-years in 45,400 adults without vascular diseases. Across all age groups, adults who subsequently developed a vascular disease in two one-year windows since diabetes diagnosis had the highest incidence of all-cause dementia. In comparison with adults without vascular diseases, HR for all-cause dementia was 1.99 (CL: 1.92–2.07) for those with one vascular disease only; 2.04 (CL: 1.98–2.13) for two or more vascular diseases; 3.56 (CL: 3.44–3.70) for stroke only; and 2.06 (CL: 1.99–2.14) for neuropathy alone. Similar associations were also observed with a smaller magnitude for adults with nephropathy, retinopathy, cardiovascular disease, or peripheral arterial disease.
Conclusions
Patients with diabetes-related complications, particularly stroke and neuropathy, and those with rapidly developed vascular diseases appeared to have a high risk of dementia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes affects approximately one in three adults worldwide [1]. Adults with type 2 diabetes, even those with prediabetes or early-stage diabetes, have an increased risk of vascular diseases [2,3,4]. Approximately, 15% of adults with newly diagnosed diabetes may develop microvascular complications within five years [2], and more than 80% of older adults with type 2 diabetes die of coronary heart disease (CHD) or stroke [5]. The risk of cardiovascular disease is especially high among those adults who present multiple microvascular complications [6].
Dementia is commonly observed among diabetic adults who have cerebrovascular disease, CHD, severe hypoglycemic events, end-organ complications, or a high diabetes severity score [7,8,9,10,11]. It has been reported that adults with type 2 diabetes have an up to 2.5-fold increased risk of dementia, including both Alzheimer’s disease (AD) and vascular dementia, compared to those without diabetes [12, 13]. Chronic inflammation, hyperglycemia, insulin resistance, and vascular damages are some of the proposed mechanisms that may explain the increased risk of dementia in diabetes populations [9,10,11, 14,15,16,17]. Brain images and cognitive function studies of adults with diabetic retinopathy or nephropathy support the association between microangiopathy and dementia [18,19,20,21,22]. However, the evidence on the role of vascular complications among diabetic patients on the development or progression of dementia is limited [9,10,11].
The clinical course of type 2 diabetes and diabetic complications has changed greatly in the last two decades [23, 24]. However, the natural history of diabetic vascular complications and their associations with dementia in Asian populations remain unclear, considering that the incidence of dementia in diabetic adults in some Asian countries is three- to sevenfold lower than that in Asians with diabetes in the USA [7, 25,26,27,28]. The present study used a longitudinal cohort of adults with newly diagnosed type 2 diabetes to identify the natural course and trajectory of microvascular and macrovascular diseases. Information about dementia in terms of numbers, types, and occurrence patterns of vascular diseases from 2000 to 2013 was assessed using the Taiwanese National Health Insurance Research Database (NHIRD).
Materials and methods
Data source
Taiwan initiated its universal National Health Insurance program in March 1995. This social insurance program requires mandatory enrollment for all Taiwanese citizens, covering 99.9% of its population in 2014, and it provides access to emergency visit services, hospice care, inpatient and outpatient care, dental care, and prescription drugs [29]. The NHIRD has been collecting all data related to medical claims, including disease diagnoses, procedures, and prescription filling in the records of inpatient, outpatient, and emergency visits since 2000 for research purposes. This research was approved by the Institutional Review Board of National Yang-Ming University, Taiwan (YM104104E).
Study design
We established a base cohort that included 90% of all adults, aged ≥ 50 years, who had newly diagnosed type 2 diabetes (n = 238,025) from 2001 to 2005 in the NHIRD (eFig. 1). Newly diagnosed type 2 diabetes was defined as having had at least three diagnosis codes of type 2 diabetes (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 250. × 0 and 250. × 2; eTable 1) within one year in the inpatient or outpatient records and having had at least one fill of prescription for oral anti-diabetic drugs within one year of the diabetes diagnosis date. Diabetes diagnosis date was defined as the date of the first type 2 diabetes diagnosis.
From the base cohort, we formed a study cohort of 173,118 adults, aged ≥ 50 years, with newly diagnosed diabetes and without a history of dementia or vascular diseases. We excluded 2,776 adults with dementia diagnosis and 62,131 adults who developed vascular diseases within one year prior to the diabetes diagnosis date (eFig. 1).
Diabetic vascular diseases
Diabetes-related microvascular and macrovascular diseases were identified using the ICD-9-CM diagnosis and/or procedure codes in the records of inpatient, outpatient, or emergency department visits (eTable 1) [23, 24]. Microvascular diseases included nephropathy, retinopathy, and neuropathy. Meanwhile, macrovascular diseases included CHD, stroke, and peripheral artery diseases (PADs). Vascular disease was identified using one of the following four criteria: having (1) one occurrence of an inpatient primary diagnosis, (2) two occurrences of an outpatient diagnosis, (3) two occurrences of an inpatient secondary diagnosis, or (4) one inpatient diagnosis and one outpatient secondary diagnosis. The date of the first encounter with a diagnosis for the first, second, and third vascular disease was considered as the diagnosis date of the first, second, and third vascular disease, respectively.
Incident all-cause dementia
Incident dementia was identified using ICD-9-CM codes that appeared at least once in the inpatient records or at least three times in the outpatient records (eTable 1) [7]. The date of the first dementia diagnosis was considered as the event date. The dementia subtypes included vascular dementia, AD, and other dementia types (senile dementia or uncomplicated presenile dementia, senile dementia with delusional or depressive features, and senile dementia with delirium).
Follow-up and index date
Follow-up started from the index date to the earliest date of a dementia event, a new vascular disease, or death, or on December 31, 2013 (Fig. 1). The index date for adults with diabetes who developed a vascular disease was the diagnosis date of the vascular disease. The index date for adults with diabetes but without vascular diseases was the date of diabetes diagnosis plus an imputed duration so that the duration of diabetes from the index date would be comparable between adults with and without vascular diseases (Fig. 1).

Study design. *The imputed duration for diabetic adults without vascular diseases (the reference group) was imputed from those with vascular diseases who had a similar distribution of age, sex, comorbidities (hyperlipidemia, hypertension, hypoglycemia, arrhythmia, and depression), and use of medications (anti-diabetic drugs, ant-ihypertensive drugs, lipid-lowering agents, anti-depressants, anti-coagulants, and anti-platelet agents) on the diabetes diagnosis date as did adults in the reference group
Comorbidities and use of medications
Comorbidities, such as hypertension, hyperlipidemia, hypoglycemia, arrhythmia, and depression without a concurrent diagnosis of bipolar disorder, were identified using the ICD-9-CM codes in the inpatient and outpatient records (eTable 1). The use of medication was defined as cumulative prescription ≥ 90 days in the outpatient and pharmacy administrative records. The medications included anti-diabetic drugs (metformin, sulfonylurea, thiazolidinedione, and insulin), anti-hypertensive drugs (angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, beta blockers, calcium channel blockers, and diuretics), lipid-lowering agents (statins, fibrates, and niacin), anti-depressants, and anti-platelet agents. Comorbidities and use of medication were identified from the date of diabetes diagnosis to the index date.
Statistical analysis
We described the occurrence patterns of vascular diseases and calculated the cumulative prevalence. Chi-square tests were performed to assess the differences in baseline characteristics at index date between diabetic adults with and without vascular diseases.
We calculated the incidence rates of all-cause dementia and its subtype across the number and type of vascular diseases. Multivariable Cox proportional-hazards models were used to estimate hazard ratios (HRs) for the incident all-cause dementia in relation to the number and type of vascular diseases. The reference group was diabetic adults without vascular diseases. The models were adjusted for age, sex, comorbidities, use of medications, and number of metabolic and hypoglycemic events during follow-up. These covariates were either potential confounders or dementia risk factors. We repeated all the aforementioned steps 100 times and obtained the median HR. We used the 1st and the 99th percentiles of HRs as confidence limits (CLs).
In the secondary analyses, we repeated all the analyses for the subtypes of dementia. Stroke is significantly correlated to vascular dementia [17]. Therefore, we also performed analyses that excluded adults with stroke.
We conducted sensitivity analyses using a matched cohort and multivariable Cox proportional-hazards regression analyses. We compared the risk of dementia in adults with and without vascular diseases and matched them by age (± 1 year), sex, and duration of diabetes (± 6 months) at the diagnosis date of vascular disease.
Results
Baseline characteristics
At the index date, the mean age of the study cohort was 67 years. By December 31, 2013, 73.8% (n = 127,718) of the adults had at least one diabetic vascular disease. Among them, 29.1% presented with macrovascular diseases and 27.8% with microvascular diseases (Table 1). Within the five years of diabetes diagnosis, 22% of the cohort members developed CHD and 11–16% developed microvascular diseases (eFig. 2). Adults with diabetic vascular diseases were more likely to have comorbidities and receive anti-diabetic drugs (63.1% vs 37.7%) or anti-hypertensive drugs (42.7% vs 22.4%) than those without vascular diseases (all P values < 0.05, Table 1).
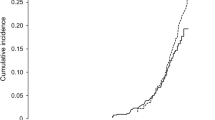
Occurrence patterns of diabetic vascular diseases
Within one year of the diabetes diagnosis, 26.3% of adults developed their first vascular disease, and within one year of the first vascular disease, 22.8% of those subsequently developed a second vascular disease (Fig. 2). Longer the duration from the diabetes diagnosis to the first vascular disease, less likely was the second vascular disease within one year of the first one. These occurrence patterns were observed across all types of vascular diseases (eFig. 3). Of those adults with a history of vascular diseases at the time of diabetes diagnosis, more than 30% developed a new microvascular disease and over 40% had a new macrovascular disease (eFig. 4).

Trajectory of the first and second vascular disease occurrence after the diagnosis of diabetes
Dementia incidence across occurrence patterns of diabetic vascular diseases
During the 1,864,279 person-years of follow-up, all-cause dementia occurred in 14,536 of the 127,718 (11.4%) adults with at least one vascular disease and 2890 of the 45,400 (6.3%) adults without, corresponding to incidence of 97.9 and 67.5 cases per 10,000 person-years, respectively (eTable 2). Across the age groups of diabetes diagnosis except for those aged 76 years or older, incidence of all-cause dementia was highest for adults who developed two vascular diseases within two one-year windows (Fig. 3).

Incidence of all-cause dementia according to the occurrence patterns of vascular disease (VasD) across the age groups at the time of diabetes diagnosis. *Two VasDs occurred in two one-year windows since the diagnosis of diabetes
Risk of all-cause dementia in terms of diabetic vascular disease
The risk of all-cause dementia in adults with diabetes was greater in those with vascular diseases than those without (Table 2), with an adjusted HR of 1.99 (CL: 1.92–2.07) for those with only one vascular disease and 2.04 (CL: 1.98–2.13) for two or more vascular diseases. Across all types of vascular complications, the risk of all-cause dementia was the highest in adults with one stroke only (adjusted HR: 3.56, CL: 3.44–3.70), followed by those with one neuropathy only (adjusted HR: 2.06, CL: 1.99–2.14).
Secondary and Sensitivity Analyses
Diabetic vascular diseases were associated with an increased risk of AD and vascular dementia, except for adults with CHD (Table 2). Adults with CHD and those without vascular diseases had a similar risk of AD. Analyses excluding adults with stroke showed that HRs for all-cause dementia, AD, and vascular dementia were greater in those with only microvascular diseases than in those with only macrovascular diseases (Table 2). Sensitivity analyses from the matched cohort study yielded consistent results as the initial analyses (eTable 3).
Discussion
In this cohort of adults 50 years or older with type 2 diabetes, approximately three-quarters (73.8%) of the study population developed a vascular disease, and approximately 10% had an all-cause dementia during the follow-up. The risk of all-cause dementia was elevated in those with even one diabetic vascular disease. The risk appeared to be particularly high for adults who developed multiple vascular diseases in a fast-occurring pattern, and those with stroke or neuropathy. This study has identified potential dementia high-risk subgroups in the diabetes population and underlined the impact of progression rate and types of vascular complications on the risk of dementia.
Several lines of evidence support the conception that diabetic vascular diseases lead to an increased risk of dementia. Diabetic vascular diseases and dementia have similar pathophysiologic risk factors, such as variability in glycemic status, insulin resistance, cardiometabolic risk factors, inflammation, and oxidative stress [10, 14,15,16]. Observational studies, including those examining brain magnetic resonance imaging and cognitive function, also supported the hypothesis that vascular diseases are on the causal pathway of diabetes and dementia [7, 9,10,11, 17,18,19,20,21,22]. These studies have shown that older adults with diabetes who present with stroke, diabetic retinal disease, kidney disease, diabetic foot, CHD, or PAD had an increased risk of AD or vascular dementia [9,10,11] and a greater decline in future cognitive function, as well as brain structure and function [18,19,20,21,22]. In addition, this study and the study by Chiu and colleagues [7] suggested that a fast progressing rate of diabetes or diabetic vascular diseases accelerates or indicates the occurrence of dementia in adults with diabetes. Alternative explanation is that diabetic vascular diseases are only indicators of the underlying factors, such as poor cerebral circulation or inflammation, which increase the risk of dementia.
In the literature, three cohort studies published to date supported a moderate, up to two-fold increase in risk of dementia associated with vascular diseases and diabetic complications [9,10,11]. These studies, included mostly white adults, assessed prevalent vascular diseases at one time-point and did not investigate the component, combination, or progression of diabetic vascular diseases. Moreover, these studies did not perform separate analyses in adults without stroke; therefore, results in the literature may be subject to residual confounding related to the history of stroke.
Based on the findings of this study, it can be hypothesized that diabetes-related dementia can be classified into two major types: one related to macrovascular complications, primarily resulting from stroke, and the other associated with microvascular complications or small vessel diseases that often manifest as neuropathy. The fact that the risk of all-cause dementia with neuropathy ranked second to stroke among all vascular diseases underlies the role of microvascular complications in dementia. When we excluded adults with history of stroke, we observed that the strength of associations with microvascular complications was greater than macrovascular complications. This increases the credibility of the findings related to microvascular complications.
In this study, the cumulative prevalence of microvascular diseases ranged from 11% to 16% within five years of the diabetes diagnosis. This is comparable with the Diabetes Prevention Program Outcome Study [2], where nearly 15% of the multi-racial population developed a microvascular disease within five years of the diabetes diagnosis. Moreover, in this study we found that already 26% of adults had vascular diseases when first diagnosed with diabetes and that 12–20% of the adults with newly diagnosed diabetes developed a new CHD, PAD, or stroke in five years. These findings support the belief that vascular and nerve damages most likely occur in prediabetes and during the early stage of diabetes [2,3,4]. This emphasizes that early screening for macrovascular diseases in adults with newly diagnosed diabetes is critical to successful long-term diabetes disease management.
Strengths and limitations
Our study had several limitations in terms of using claims data. First, dementia was identified based on diagnosis codes, and the results for dementia subtypes should be interpreted with caution as dementia diagnoses and classifications are still evolving [30] and AD may be misclassified as vascular dementia in adults with diabetes, stroke, or CHD. Second, the actual time of disease occurrence cannot be identified, as in virtually all observational studies. Our study might have underestimated the incidence rates of dementia because we cannot identify adults with mild dementia who did not receive health care. Third, data about smoking status, alcohol use, HbA1c level, family history of dementia, years of education, and economic status were not available. Lack of adjustment for these confounding factors may have led to biased HR estimates toward or away from the null association. Fourth, results from this study may not be generalizable to other racial/ethnic groups or different healthcare systems. Finally, the occurrence of neuropathies is common, but not all neuropathies in type 2 diabetes are attributed to diabetes or microvascular disease.
This study also had some strengths. First, a conservative algorithm was used to identify diabetic vascular diseases in a cohort that included 90% of all adults aged ≥ 50 years with type 2 diabetes in Taiwan. The proportion of patients who were lost to follow-up was low. Second, the confounding effect of history of stroke was eliminated in this study. In contrast, the previous studies have not excluded the influence of stroke [7, 9,10,11, 28, 31]. Third, we reduced immortal-time bias and confounding bias by considering the duration between diabetes diagnosis and vascular disease diagnosis and by conducting multivariable regression analyses. In addition, the results of the original analyses and the sensitivity analyses of the matched cohorts were consistent.
Conclusion
In adults with newly diagnosed type 2 diabetes, vascular diseases became prevalent within five years of diabetes diagnosis and the risk of dementia appeared to be the greatest for patients who rapidly developed diabetes-related complications. Intervention strategies for dementia prevention, including screening tests and risk factor modifications, should target high-risk subgroups of the diabetes populations, including those with multiple vascular diseases, stroke, or neuropathy. Delaying the onset and progression of vascular diseases may also prevent the development of dementia.
Data availability
The data that supported the study findings are available from the National Health Insurance Administration, Ministry of Health and Welfare, Taiwan, but restrictions may apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from the National Health Insurance Administration, Ministry of Health and Welfare, Taiwan.
References:
International Diabetes Federation (2017) IDF Diabetes Atlas—8th ed. Available from http://www.diabetesatlas.org/. Accessed Nov 5 2018
Diabetes Prevention Program Research Group (2015) Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the diabetes prevention program outcomes study. Lancet Diabet Endocrinol 3(11):866–875. https://doi.org/10.1016/s2213-8587(15)00291-0
Ramlo-Halsted BA, Edelman SV (1999) The natural history of type 2 diabetes. Implic Clinical Pract Prim Care 26(4):771–789
Selvin E, Steffes MW, Zhu H et al (2010) Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults. N Engl J Med 362(9):800–811. https://doi.org/10.1056/NEJMoa0908359
Benjamin EJ, Blaha MJ, Chiuve SE et al (2017) Heart disease and stroke statistics-2017 update: a report from the american heart association. Circulation 135(10):e146–e603. https://doi.org/10.1161/CIR.0000000000000485
Brownrigg JR, Hughes CO, Burleigh D et al (2016) Microvascular disease and risk of cardiovascular events among individuals with type 2 diabetes: a population-level cohort study. Lancet Diabet Endocrinol 4(7):588–597. https://doi.org/10.1016/s2213-8587(16)30057-2
Chiu WC, Ho WC, Liao DL et al (2015) Progress of diabetic severity and risk of dementia. J Clin Endocrinol Metab 100(8):2899–2908. https://doi.org/10.1210/jc.2015-1677
Whitmer RA, Karter AJ, Yaffe K, Quesenberry CP, Selby JV (2009) Hypoglycemic episodes and risk of dementia in older patients with type 2 diabetes mellitus. JAMA 301(15):1565–1572
Exalto LG, Biessels GJ, Karter AJ et al (2013) Risk score for prediction of 10 year dementia risk in individuals with type 2 diabetes: a cohort study. Lancet Diabet Endocrinol 1(3):183–190. https://doi.org/10.1016/S2213-8587(13)70048-2
Exalto LG, Biessels GJ, Karter AJ, Huang ES, Quesenberry CP Jr, Whitmer RA (2014) Severe diabetic retinal disease and dementia risk in type 2 diabetes. J Alzheimers Dis 42(Suppl 3):S109-117. https://doi.org/10.3233/jad-132570
Haroon NN, Austin PC, Shah BR, Wu J, Gill SS, Booth GL (2015) Risk of dementia in seniors with newly diagnosed diabetes: a population-based study. Diabet Care 38(10):1868–1875. https://doi.org/10.2337/dc15-0491
Biessels GJ, Staekenborg S, Brunner E, Brayne C, Scheltens P (2006) Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol 5(1):64–74. https://doi.org/10.1016/S1474-4422(05)70284-2
Chatterjee S, Peters SAE, Woodward M et al (2016) Type 2 diabetes as a risk factor for dementia in women compared with men: a pooled analysis of 2.3 million people comprising more than 100,000 cases of dementia. Diabet Care 39(2):300–307. https://doi.org/10.2337/dc15-1588
Crane PK, Walker R, Hubbard RA et al (2013) Glucose levels and risk of dementia. N Engl J Med 369(6):540–548. https://doi.org/10.1056/NEJMoa1215740
Strachan MWJ, Reynolds RM, Marioni RE, Price JF (2011) Cognitive function, dementia and type 2 diabetes mellitus in the elderly. Nat Rev Endocrinol 7(2):108–114. https://doi.org/10.1038/nrendo.2010.228
Arnold SE, Arvanitakis Z, Macauley-Rambach SL et al (2018) Brain insulin resistance in type 2 diabetes and Alzheimer disease: concepts and conundrums. Nat Rev Neurol 14(3):168–181. https://doi.org/10.1038/nrneurol.2017.185
Gorelick PB, Scuteri A, Black SE et al (2011) Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association. Stroke 42(9):2672–2713. https://doi.org/10.1161/STR.0b013e3182299496
Hugenschmidt CE, Lovato JF, Ambrosius WT et al (2014) The cross-sectional and longitudinal associations of diabetic retinopathy with cognitive function and brain MRI findings: the action to control cardiovascular risk in diabetes (ACCORD) trial. Diabet Care 37(12):3244–3252. https://doi.org/10.2337/dc14-0502
Barzilay JI, Lovato JF, Murray AM et al (2013) Albuminuria and cognitive decline in people with diabetes and normal renal function. Clin J Am Soc Nephrol 8(11):1907–1914. https://doi.org/10.2215/cjn.11321112
Freedman BI, Sink KM, Hugenschmidt CE et al (2017) Associations of early kidney disease with brain magnetic resonance imaging and cognitive function in african americans with type 2 diabetes mellitus. Am J Kidney Dis 70(5):627–637. https://doi.org/10.1053/j.ajkd.2017.05.006
Sink KM, Divers J, Whitlow CT et al (2015) Cerebral structural changes in diabetic kidney disease: African American-diabetes heart study MIND. Diabet Care 38(2):206–212. https://doi.org/10.2337/dc14-1231
Marseglia A, Xu W, Rizzuto D et al (2014) Cognitive functioning among patients with diabetic foot. J Diabet Complic 28(6):863–868
Huang ES, Laiteerapong N, Liu JY, John PM, Moffet HH, Karter AJ (2014) Rates of complications and mortality in older patients with diabetes mellitus: the diabetes and aging study. JAMA Intern Med 174(2):251–258. https://doi.org/10.1001/jamainternmed.2013.12956
Gregg EW, Li Y, Wang J et al (2014) Changes in diabetes-related complications in the United States, 1990–2010. N Engl J Med 370(16):1514–1523. https://doi.org/10.1056/NEJMoa1310799
Mayeda ER, Glymour MM, Quesenberry CP, Whitmer RA (2016) Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Alzheimers Dement 12(3):216–224. https://doi.org/10.1016/j.jalz.2015.12.007
Mayeda ER, Karter AJ, Huang ES, Moffet HH, Haan MN, Whitmer RA (2014) Racial/ethnic differences in dementia risk among older type 2 diabetic patients: the diabetes and aging study. Diabet Care 37(4):1009–1015. https://doi.org/10.2337/dc13-0215
Li TC, Yang CP, Tseng ST et al (2017) Visit-to-visit variations in fasting plasma glucose and HbA1c associated with an increased risk of Alzheimer disease: Taiwan diabetes study. Diabet Care 40(9):1210–1217. https://doi.org/10.2337/dc16-2238
Kuo S-C, Lai S-W, Hung H-C et al (2015) Association between comorbidities and dementia in diabetes mellitus patients: population-based retrospective cohort study. J Diabet Complic 29(8):1071–1076. https://doi.org/10.1016/j.jdiacomp.2015.06.010
National Health Research Institutes National Health Insurance Research Database, Taiwan. Available from https://nhird.nhri.org.tw/en/index.html. Accessed Nov 6 2019
James BD, Bennett DA (2019) Causes and patterns of dementia: an update in the era of redefining Alzheimer’s disease. Ann Rev Publ Health 40:65–84. https://doi.org/10.1146/annurev-publhealth-040218-043758
Li CI, Li TC, Liu CS et al (2018) Risk score prediction model for dementia in patients with type 2 diabetes. Eur J Neurol 25(7):976–983. https://doi.org/10.1111/ene.13642
Acknowledgement
The authors would like to thank the editors of CACTUS Communications (editage in Taiwan) for providing language editing and proofreading services.
Funding
The present study was supported in part by grants from the Ministry of Health and Welfare (MOHW104-TDU-B-211–113-003, MOHW106-TDU-B-211–113001) and an intramural grant from National Yang-Ming University (E107F-M01-0501). These funding sources have no role in the study design and conduct, writing of the report, and submission of the article for publication.
Author information
Authors and Affiliations
Contributions
Chang, Henderson, Tsai, and Cheng were involved in study concept and design. Tsai helped in acquisition of data. All contributed to analysis and/or interpretation of data. Chang, Wang, and Tsai were involved in drafting of the manuscript. All helped in critical revision of the manuscript for important intellectual content. All contributed to approval of the version to be published. Drs. Tsai and Cheng accepted full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Corresponding authors
Ethics declarations
Conflict of interest
All authors have no conflict of interest to disclose.
Ethical approval
This research study was conducted retrospectively from data obtained for clinical purposes. We consulted extensively with the IRB of National Yang-Ming University, Taiwan, who determined that our study did not need ethical approval. An IRB official waiver of ethical approval was granted from the IRB of National Yang-Ming Univeristy, Taiwan (YM104104E).
Informed consent
An IRB official waiver of ethical approval and acquisition of informed consents was granted from the IRB of National Yang-Ming University (YM104104E).
Additional information
Managed by Massimo Porta.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
Chang, PY., Wang, IT., Chiang, CE. et al. Vascular complications of diabetes: natural history and corresponding risks of dementia in a national cohort of adults with diabetes. Acta Diabetol 58, 859–867 (2021). https://doi.org/10.1007/s00592-021-01685-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-021-01685-y