
Abstract
Purpose
In the last couple of years, a significant amount of studies comparing the UKA and TKA for unicompartmental knee osteoarthritis have been published. However, there is a lack of recent meta-analysis comparing the two implants. Since the number of performed UKAs is currently increasing and the indications are obsolete, it becomes important to update current evidences and outcomes. With these premises, a meta-analysis of clinical trials comparing UKA versus TKA was conducted.
Methods
In October 2018, the following databases were accessed: Cochrane Systematic Reviews, Scopus, PubMed and Google Scholar. According to the Oxford Center of Evidence-based Medicine, level of evidence articles I to III were included. Only studies reporting quantitative data concerning the outcomes of interest were included. For the statistical analysis and the methodological quality assessment, we referred to the Review Manager Software 5.3. Dichotomous data were analyzed through the Mantel–Haenszel statistical method with the odd ratio effect measure. For continuous data, the inverse variance statistical method was used with the mean difference effect measure. A confidence interval of 95% was considered for analysis. To evaluate study heterogeneity, both Chi-square and Higgins tests were performed. Values of P < 0.05 were considered statistically significant.
Results
The overall methodological quality assessment was moderate. The risk of publication’s bias was moderate. We enrolled in this study a total of 13,789 patients. The mean follow-up was 42.69 months. The UKA evidenced increased risk of revision’s surgeries (OR 2.16, P > 0.0001). All the other scores of interest were in favor of the UKA: Oxford Knee Score, KSS Clinical, WOMAC overall and related subscales. The UKA also reported better functional outcomes: KSS Function, longer walking distance, improvement of the joint flexion and ROM. Moreover, in the UKA group have been reported a shorter length of stay, reduced estimated total blood loss and shorter surgical duration.
Conclusion
The main findings of this meta-analysis are that UKA reported a reduced survivorship but better clinical and functional performances compared to TKA. Furthermore, shorter surgical duration, lower total estimated blood loss and quicker hospitalization length were observed in the UKA cohort.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The prevalence of symptomatic osteoarthritis (OA) in Caucasian population is around 10% in men and 20% in women aged 45 years and above [1]. Total knee arthroplasty (TKA) represents the gold standard treatment for end-stage OA, being both functional and cost-effective procedure [2, 3]. However, OA affects in ca 30% of cases only one joint compartment, mostly the medial one [4, 5]. Unicompartmental knee arthroplasty (UKA) is an available option to treat selected patients. The indications to perform a UKA were first outlined in 1989 by Kozinn and Scott [6]: presence of unicompartmental OA and of an efficient anterior cruciate ligament, varus deformity < 5°, range of motion > 90° without flexion contracture, body mass index (BMI) < 30 kg/m2. Compared to the total knee arthroplasty, the UKA preserves the cruciate ligaments, meniscus and tibia plateau of the healthy compartment, thus sparing more bone stock for further revision. In the last decades, a significant amount of published studies compared the UKA and TKA for unicompartmental knee OA [7,8,9,10,11,12,13,14,15,16]. However, there is a lack of recent meta-analysis comparing the two implants. Since the number of performed UKAs is currently increasing [17] and the indications are obsolete [18, 19], it becomes of fundamental importance to update current evidences and outcomes. With these premises, a meta-analysis of clinical trials comparing UKA versus TKA was conducted. We focused on implant’s survivorship, clinical, functional and perioperative outcomes.
Materials and methods
Search strategy
The literature search was independently performed by two authors (FM, JE). This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20]. Criteria for inclusion were the following:
-
Patient cohort: unicompartmental knee degeneration;
-
Intervention: unicompartmental knee arthroplasty (UKA);
-
Comparison: total knee arthroplasty (TKA);
-
Outcomes: clinical and functional scores, length of stay, ROM, total estimated blood loss, surgical duration, further revisions.
Data extraction
Data extraction was performed by two independent authors (FM, JE). For the initial database search, we accessed the Cochrane Systematic Reviews, Scopus, PubMed and Google Scholar, using the following keywords in isolation or combined: knee, total, unicondylar, partial, unicompartmental, osteoarthritis, replacement, prosthesis, implant, arthroplasty. The search was performed in October 2018. The authors independently read title and eventually the abstract of each paper, accessing the full text of the articles of interest. The bibliographies of the articles of interest were also screened.
Eligibility criteria
All the studies comparing UKA versus TKA for primary knee replacement were considered for inclusion. According to the Oxford Center of Evidence-based Medicine [21], level of evidence articles I to III were included. Biomechanics, animal and in vitro studies were excluded, along with case reports, reviews and meta-analysis, editorials, letters and expert opinions. According to the author language capabilities, studies in English, Italian, German, Spanish and French were considered. Due to the continuous innovations in components design and surgical progresses, the search was limited in a time frame from 2000 to 2018. Studies concerning bi- or tri-compartmental implants were excluded, along with cementless prosthesis. Studies providing navigation systems were included. Only studies reporting quantitative data concerning the outcomes of interest were included. Authors’ disagreements were debated and mutually solved.
Outcomes of interest
First, demographic data of each study were collected: mean age and BMI, percentage of female subjects, number of knees treated, mean follow-up. The primary outcome was to compare the revision’s rate between the implants. Secondary outcomes were: the Oxford Knee Score (OKS) [22], Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and related subscale [23], the clinical and functional subscales of the Knee Society Rating System (KSS) [24] and the postoperative range of motion (ROM). Duration of surgery and total estimated blood loss were also considered.
Methodological quality assessment
Two independent authors (FM and JE) evaluated the methodological quality assessment using the Review Manager Software 5.3 (The Nordic Cochrane Centre, Copenhagen). For the evaluation, we referred to allocation concealment (selection bias), blinding of outcome assessments (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other possible uncharged/unexplained risks.
Statistical analysis
For the statistical analysis, we referred to the Review Manager Software 5.3 (The Nordic Cochrane Centre, Copenhagen). Dichotomous data were analyzed through the Mantel–Haenszel statistical method with the odd ratio (OR) effect measure. For continuous data, the inverse variance statistical method was used with a mean difference effect measure. A confidence interval (CI) of 95% was considered for the analysis. We performed a forest plot for each outcome of interest. To analyze the heterogeneity, both Chi-square and Higgins (I2) tests were performed. Value of I2 of 25%, 50% and 75% represents, respectively, low, moderate and high grades of heterogeneity. An initial fixed analysis model to the comparisons was used. If high value of heterogeneity was detected, a random analysis model was adopted. To evaluate the risk of publication’s bias, the funnel plot was performed. To evaluate the component survivorship, the Kaplan–Meier curve was performed. Values of P < 0.5 were considered statistically significant.
Results
Search result
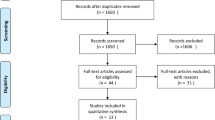
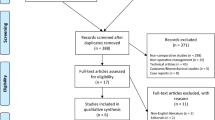
A total of 356 studies from database search and cross-references screening were obtained. Of these, 112 were removed because of duplicates. Other 175 articles were rejected because they did not match the topic. Other 66 studies were rejected because they did not report informations under the outcomes of interest. This left 23 articles for this study. The literature search is shown in Fig. 1.

PRISMA flow-chart of the literature search
Methodological quality assessment
The methodological quality assessment reported a moderate risk of selection and detection bias, a low to moderate risk of reporting bias and a low level of attrition bias. Other not-specified biases have a low to moderate risk. The methodological quality assessment is negatively affected by the overall low level of evidence of the included studies. Concluding, the methodological quality assessment revealed a moderate quality. The methodological quality assessment is shown in Fig. 2.

Cochrane methodological quality assessment
Risk of publication’s bias
To analyze the risk of publication’s bias, the funnel plot of the primary outcome of interest was performed (revision’s rate). All studies are detected in the range of acceptability and are positioned moderately symmetrically close to the no-effect line, indicating a low to moderate risk of publication’s bias. The funnel plot is shown in Fig. 3.

Funnel plot to assess the publication’s bias. SE standard error, OR odd ratio
Patients’ demographics
A total of 13,789 patients were enrolled, undergoing a mean follow-up of 42.69 ± 24.76 months. To the UKA cohort belonged 3254 patients: The mean age was 66.75 ± 4.43 years, the mean BMI was 31 ± 2.75 kg/m2 and 57% of the patients were females. The TKA group included 10,649 patients, 61% of which were females, with mean age of 66.00 ± 3.06 years and mean BMI of 29.33 ± 2.87 kg/m2. The demographic baseline is shown in Table 1.
Outcomes
A total of 16 studies reported revision’s rate, including 10,629 patients. The UKA reported a statistically significant higher risk compared to the TKA (OR 2.16; CI 1.66–2.81; I2 = 43%; P < 0.0001, Fig. 4).

Forest plot of the comparison revision. SD standard deviation, IV inverse variance, CI confidence interval
All the analyzed scores are statistically significant in favor of the UKA: the Oxford Knee Score (EE 1.30; CI − 1.08, 3.67; I2: 85%; P = 0.28), KSS Clinical (EE 1.22; CI 0.25, 2.19; I2: 0%; P = 0.01), KSS Function (EE 5.40; CI − 3.14, 13.94; I2: 91%; P = 0.22), WOMAC overall (EE 5.22; CI − 0.57, 11.01; I2 75%; P = 0.08) and related subscales: pain (EE 5.77; CI − 2.87, 14.42; I2: 88%; P = 0.19), stiffness (EE 3.20; CI 2.79, 9.18; I2: 67%; P = 0.30), function (EE 6.02; CI 3.22, 8.82; I2: 24%; P < 0.0001). The UKA reported also statistically significant longer walking distance (EE 36.80; CI 13.40, 60.20; I2: 66%; P = 0.002), improvement of the joint flexion (EE 11.33; CI 7.92, 14.73; I2: 73%; P < 0.00001) and ROM (EE 6.42; CI 1.84, 11.00; I2: 72%; P = 0.006). Moreover, in the UKA group have been reported statistically significant shorter length of stay (EE − 1.88; CI − 2.84, − 0.92; I2: 98%; P = 0.0001), reduced estimated blood loss (EE − 70.66; CI − 142.27, 0.95; I2: 100%; P = 0.5) and shorter surgical duration (EE − 23.16; CI − 41.51, − 4.81; I2: 98%; P = 0.01). Table 2 summarizes the results of the comparisons.
Discussion
The main findings of this meta-analysis are that UKA reported a reduced survivorship but better clinical and functional performances compared to TKA. Furthermore, even shorter surgical duration, lower estimated blood loss and quicker hospitalization length were observed in the UKA cohort. Current evidences demonstrated also a quicker return to high-level sports after UKA, which is of special interest in younger patients [37,38,39,40]. These results suggest that the UKA implants are more suitable for physically active patients, since they allow better clinical and functional performances. TKA are indicated in patients presenting comorbidities, cognitive impairment and reduced performance status, since a lower revision’s rate is preferable to higher functional performances.
The analysis of the comparison revision (Fig. 4) showed overlapping of the CI and heterogeneous statistical weights distribution. The level of heterogeneity expressed by the Chi-square and Higgins (I2) tests was acceptable, and a fixed analysis model was used. The overall result was statistically significant in favor of the UKA group, reporting a risk doubled (OR 2.16) compared to the TKA. This result is highlighted even by the Kaplan–Meier curve (Fig. 5), which clearly reported a reduction of the survivorship during the follow-up term. This result was coherent with other previous published studies [41,42,43]. Several studies analyzed the causes of revision: implant loosening, tibial collapse, worn-out of the inlay, mechanical failures, fractures and OA progression [44,45,46,47,48]. Since UKA implants are extremely sensible to the components alignment [49,50,51], it is easier to incur into technical errors [52]. A typical example is the overcorrection of the tibiofemoral angle, causing overload of the contralateral joint compartment [53]. The long learning curve characterizing the UKA implants contributes as well to improve the revision’s rate [54]. Furthermore, even the higher athletic performances observed after UKA implants can be related to the survivorship reduction.

Kaplan–Meier survivorship curve
The Oxford Knee Score and WOMAC pain subscales were used to analyze the level of pain after surgery. The UKA evidenced statistically significant improvement in both the scores. To analyze the functional performances of the implants, we referred to the walking distance, flexion, ROM, KSFS and WOMAC (functional and stiffness subscales). The UKA scored better results in all the mentioned parameters, providing statistically significant results. We hypothesize that these functional improvements arise from the retention of the cruciate ligaments and the meniscus. These structures are involved in the joint kinematics, improving the flexion by promoting the rollback [55, 56]. Moreover, the cruciate ligaments function as mechanoreceptors [57], detecting body kinesthesia and proprioception [58]. Regarding the clinical scores, the KSCS and the overall WOMAC were both in favor of the UKA group, providing statistically significant results. Furthermore, a statistically significant shorter hospitalization, lower estimated blood loss and shorter surgical duration were evidenced. Overall, these results explain the high satisfaction rate observed in patients after the UKA implants [34, 59, 60].
The present study has some limitations. We included studies with low levels of evidence, since high-quality studies concerning this topic are very limited, increasing the risk of selection bias. Further studies providing samples randomization and longer follow-up are required to improve the evidences regarding UKA implants. Points of strengths of this work were the comprehensive nature of the literature search, the rigorously methodological quality assessment and the good baseline comparability of the samples.
Conclusion
The main findings of this meta-analysis are that UKA reported a reduced survivorship but better clinical and functional performances compared to TKA. Furthermore, shorter surgical duration, lower estimated blood loss and quicker hospitalization length were observed in the UKA cohort.
References
March LM, Schwarz JM, Carfrae BH, Bagge E (1998) Clinical validation of self-reported osteoarthritis. Osteoarthr Cartil 6(2):87–93. https://doi.org/10.1053/joca.1997.0098
Richmond J, Hunter D, Irrgang J, Jones MH, Snyder-Mackler L, Van Durme D, Rubin C, Matzkin EG, Marx RG, Levy BA, Watters WC 3rd, Goldberg MJ, Keith M, Haralson RH 3rd, Turkelson CM, Wies JL, Anderson S, Boyer K, Sluka P, St Andre J, McGowan R, Academy American, American Academy of Orthopaedic Surgeons (2010) American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of osteoarthritis (OA) of the knee. J Bone Joint Surg Am 92(4):990–993. https://doi.org/10.2106/JBJS.I.00982
Ghomrawi HM, Eggman AA, Pearle AD (2015) Effect of age on cost-effectiveness of unicompartmental knee arthroplasty compared with total knee arthroplasty in the U.S. J Bone Joint Surg Am 97(5):396–402. https://doi.org/10.2106/jbjs.n.00169
Ackroyd CE (2003) Medial compartment arthroplasty of the knee. J Bone Joint Surg Br 85(7):937–942
Longo UG, Loppini M, Fumo C, Rizzello G, Khan WS, Maffulli N, Denaro V (2012) Osteoarthritis: new insights in animal models. Open Orthop J 6:558–563. https://doi.org/10.2174/1874325001206010558
Kozinn SC, Scott R (1989) Unicondylar knee arthroplasty. J Bone Joint Surg Am 71(1):145–150
Danford NGM, Heller MS, Murtaugh T, Shah RP, Cooper HJ, Lakra A, Geller JA (2017) Which do patients prefer unicompartmental or total knee arthroplasty? J Clin Orthop Trauma. https://doi.org/10.1016/j.jcot.2017.08.012
Horikawa A, Miyakoshi N, Shimada Y, Kodama H (2015) Comparison of clinical outcomes between total knee arthroplasty and unicompartmental knee arthroplasty for osteoarthritis of the knee: a retrospective analysis of preoperative and postoperative results. J Orthop Surg Res 10:168. https://doi.org/10.1186/s13018-015-0309-2
Siman H, Kamath AF, Carrillo N, Harmsen WS, Pagnano MW, Sierra RJ (2017) Unicompartmental knee arthroplasty vs total knee arthroplasty for medial compartment arthritis in patients older than 75 years: comparable reoperation, revision, and complication rates. J Arthroplasty 32(6):1792–1797. https://doi.org/10.1016/j.arth.2017.01.020
Shankar S, Tetreault MW, Jegier BJ, Andersson GB, Della Valle CJ (2016) A cost comparison of unicompartmental and total knee arthroplasty. Knee 23(6):1016–1019. https://doi.org/10.1016/j.knee.2015.11.012
Purcell RL, Cody JP, Ammeen DJ, Goyal N, Engh GA (2018) Elimination of preoperative flexion contracture as a contraindication for unicompartmental knee arthroplasty. J Am Acad Orthop Surg 26(7):e158–e163. https://doi.org/10.5435/JAAOS-D-16-00802
Ode Q, Gaillard R, Batailler C, Herry Y, Neyret P, Servien E, Lustig S (2018) Fewer complications after UKA than TKA in patients over 85 years of age: a case–control study. Orthop Traumatol Surg Res. https://doi.org/10.1016/j.otsr.2018.02.015
Lum ZC, Lombardi AV, Hurst JM, Morris MJ, Adams JB, Berend KR (2016) Early outcomes of twin-peg mobile-bearing unicompartmental knee arthroplasty compared with primary total knee arthroplasty. Bone Joint J 98-B(10 Supple B):28–33. https://doi.org/10.1302/0301-620x.98b10.bjj-2016-0414.r1
Lum ZC, Crawford DA, Lombardi AV Jr., Hurst JM, Morris MJ, Adams JB, Berend KR (2018) Early comparative outcomes of unicompartmental and total knee arthroplasty in severely obese patients. Knee 25(1):161–166. https://doi.org/10.1016/j.knee.2017.10.006
Zuiderbaan HA, van der List JP, Khamaisy S, Nawabi DH, Thein R, Ishmael C, Paul S, Pearle AD (2017) Unicompartmental knee arthroplasty versus total knee arthroplasty: Which type of artificial joint do patients forget? Knee Surg Sports Traumatol Arthrosc 25(3):681–686. https://doi.org/10.1007/s00167-015-3868-1
van der List JP, Chawla H, Villa JC, Pearle AD (2017) The role of patient characteristics on the choice of unicompartmental versus total knee arthroplasty in patients with medial osteoarthritis. J Arthroplasty 32(3):761–766. https://doi.org/10.1016/j.arth.2016.08.015
Harrysson OL, Robertsson O, Nayfeh JF (2004) Higher cumulative revision rate of knee arthroplasties in younger patients with osteoarthritis. Clin Orthop Relat Res 421:162–168
Lombardi AV Jr., Berend KR, Berend ME, Della Valle CJ, Engh GA, Fitz W, Hurst JM, Jinnah RH, Lonner JH, Macaulay WB, Repicci JA, Scuderi GR (2012) Current controversies in partial knee arthroplasty. Instr Course Lect 61:347–381
Archibeck MJ, White RE Jr., Council of Musculoskeletal Specialty Societies AAoOS (2004) What’s new in adult reconstructive knee surgery. J Bone Joint Surg Am 86A(8):1839–1849
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Open Med 3:e123–e130
Howick JCI, Glasziou P, Greenhalgh T, Carl H, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine. https://www.cebmnet/indexaspx?o=5653. Accessed Sept 2018
Dawson J, Fitzpatrick R, Murray D, Carr A (1998) Questionnaire on the perceptions of patients about total knee replacement. J Bone Joint Surg Br 80(1):63–69
Gandek B (2015) Measurement properties of the Western Ontario and McMaster Universities Osteoarthritis Index: a systematic review. Arthritis Care Res (Hoboken) 67(2):216–229. https://doi.org/10.1002/acr.22415
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Costa CR, Johnson AJ, Mont MA, Bonutti PM (2011) Unicompartmental and total knee arthroplasty in the same patient. J Knee Surg 24(4):273–278
Ko Y, Narayanasamy S, Wee HL, Lo NN, Yeo SJ, Yang KY, Yeo W, Chong HC, Thumboo J (2011) Health-related quality of life after total knee replacement or unicompartmental knee arthroplasty in an urban asian population. Value Health 14(2):322–328. https://doi.org/10.1016/j.jval.2010.08.005
Laurencin CT, Zelicof SB, Scott RD, Ewald FC (1991) Unicompartmental versus total knee arthroplasty in the same patient. A comparative study. Clin Orthop Relat Res 273:151–156
Lim JW, Cousins GR, Clift BA, Ridley D, Johnston LR (2014) Oxford unicompartmental knee arthroplasty versus age and gender matched total knee arthroplasty—functional outcome and survivorship analysis. J Arthroplasty 29(9):1779–1783. https://doi.org/10.1016/j.arth.2014.03.043
Lombardi AV Jr., Berend KR, Walter CA, Aziz-Jacobo J, Cheney NA (2009) Is recovery faster for mobile-bearing unicompartmental than total knee arthroplasty? Clin Orthop Relat Res 467(6):1450–1457. https://doi.org/10.1007/s11999-009-0731-z
Lyons MC, MacDonald SJ, Somerville LE, Naudie DD, McCalden RW (2012) Unicompartmental versus total knee arthroplasty database analysis: Is there a winner? Clin Orthop Relat Res 470(1):84–90. https://doi.org/10.1007/s11999-011-2144-z
Manzotti A, Confalonieri N, Pullen C (2007) Unicompartmental versus computer-assisted total knee replacement for medial compartment knee arthritis: a matched paired study. Int Orthop 31(3):315–319. https://doi.org/10.1007/s00264-006-0184-x
Schwab PE, Lavand’homme P, Yombi JC, Thienpont E (2015) Lower blood loss after unicompartmental than total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 23(12):3494–3500. https://doi.org/10.1007/s00167-014-3188-x
Sun PF, Jia YH (2012) Mobile bearing UKA compared to fixed bearing TKA: a randomized prospective study. Knee 19(2):103–106. https://doi.org/10.1016/j.knee.2011.01.006
Von Keudell A, Sodha S, Collins J, Minas T, Fitz W, Gomoll AH (2014) Patient satisfaction after primary total and unicompartmental knee arthroplasty: an age-dependent analysis. Knee 21(1):180–184. https://doi.org/10.1016/j.knee.2013.08.004
Walker T, Gotterbarm T, Bruckner T, Merle C, Streit MR (2014) Total versus unicompartmental knee replacement for isolated lateral osteoarthritis: a matched-pairs study. Int Orthop 38(11):2259–2264. https://doi.org/10.1007/s00264-014-2473-0
Yang KY, Wang MC, Yeo SJ, Lo NN (2003) Minimally invasive unicondylar versus total condylar knee arthroplasty—early results of a matched-pair comparison. Singap Med J 44(11):559–562
Na SE, Ha CW, Lee CH (2012) A new high-flexion knee scoring system to eliminate the ceiling effect. Clin Orthop Relat Res 470(2):584–593. https://doi.org/10.1007/s11999-011-2203-5
Zahiri CA, Schmalzried TP, Szuszczewicz ES, Amstutz HC (1998) Assessing activity in joint replacement patients. J Arthroplasty 13(8):890–895
Waldstein W, Kolbitsch P, Koller U, Boettner F, Windhager R (2017) Sport and physical activity following unicompartmental knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc 25(3):717–728. https://doi.org/10.1007/s00167-016-4167-1
Naal FD, Fischer M, Preuss A, Goldhahn J, von Knoch F, Preiss S, Munzinger U, Drobny T (2007) Return to sports and recreational activity after unicompartmental knee arthroplasty. Am J Sports Med 35(10):1688–1695. https://doi.org/10.1177/0363546507303562
Weale AE, Murray DW, Newman JH, Ackroyd CE (1999) The length of the patellar tendon after unicompartmental and total knee replacement. J Bone Joint Surg Br 81(5):790–795
Emerson RH Jr., Higgins LL (2008) Unicompartmental knee arthroplasty with the oxford prosthesis in patients with medial compartment arthritis. J Bone Joint Surg Am 90(1):118–122. https://doi.org/10.2106/JBJS.F.00739
Kuipers BM, Kollen BJ, Bots PC, Burger BJ, van Raay JJ, Tulp NJ, Verheyen CC (2010) Factors associated with reduced early survival in the Oxford phase III medial unicompartment knee replacement. Knee 17(1):48–52. https://doi.org/10.1016/j.knee.2009.07.005
Lewold S, Robertsson O, Knutson K, Lidgren L (1998) Revision of unicompartmental knee arthroplasty: outcome in 1,135 cases from the Swedish Knee Arthroplasty study. Acta Orthop Scand 69(5):469–474
Saldanha KA, Keys GW, Svard UC, White SH, Rao C (2007) Revision of Oxford medial unicompartmental knee arthroplasty to total knee arthroplasty—results of a multicentre study. Knee 14(4):275–279. https://doi.org/10.1016/j.knee.2007.03.005
Springer BD, Scott RD, Thornhill TS (2006) Conversion of failed unicompartmental knee arthroplasty to TKA. Clin Orthop Relat Res 446:214–220. https://doi.org/10.1097/01.blo.0000214431.19033.fa
Barrett WP, Scott RD (1987) Revision of failed unicondylar unicompartmental knee arthroplasty. J Bone Joint Surg Am 69(9):1328–1335
Furnes O, Espehaug B, Lie SA, Vollset SE, Engesaeter LB, Havelin LI (2007) Failure mechanisms after unicompartmental and tricompartmental primary knee replacement with cement. J Bone Joint Surg Am 89(3):519–525. https://doi.org/10.2106/JBJS.F.00210
Chatellard R, Sauleau V, Colmar M, Robert H, Raynaud G, Brilhault J, Societe d’Orthopedie et de Traumatologie de lO (2013) Medial unicompartmental knee arthroplasty: does tibial component position influence clinical outcomes and arthroplasty survival? Orthop Traumatol Surg Res 99(4 Suppl):S219–S225. https://doi.org/10.1016/j.otsr.2013.03.004
Hernigou P, Deschamps G (2004) Alignment influences wear in the knee after medial unicompartmental arthroplasty. Clin Orthop Relat Res 423:161–165
Vasso M, Del Regno C, D’Amelio A, Viggiano D, Corona K, Schiavone Panni A (2015) Minor varus alignment provides better results than neutral alignment in medial UKA. Knee 22(2):117–121. https://doi.org/10.1016/j.knee.2014.12.004
Lewold S, Goodman S, Knutson K, Robertsson O, Lidgren L (1995) Oxford meniscal bearing knee versus the Marmor knee in unicompartmental arthroplasty for arthrosis. A Swedish multicenter survival study. J Arthroplasty 10(6):722–731
Price AJ, Short A, Kellett C, Beard D, Gill H, Pandit H, Dodd CA, Murray DW (2005) Ten-year in vivo wear measurement of a fully congruent mobile bearing unicompartmental knee arthroplasty. J Bone Joint Surg Br 87(11):1493–1497. https://doi.org/10.1302/0301-620X.87B11.16325
Zhang Q, Zhang Q, Guo W, Liu Z, Cheng L, Yue D, Zhang N (2014) The learning curve for minimally invasive Oxford phase 3 unicompartmental knee arthroplasty: cumulative summation test for learning curve (LC-CUSUM). J Orthop Surg Res 9:81. https://doi.org/10.1186/s13018-014-0081-8
Isaac SM, Barker KL, Danial IN, Beard DJ, Dodd CA, Murray DW (2007) Does arthroplasty type influence knee joint proprioception? A longitudinal prospective study comparing total and unicompartmental arthroplasty. Knee 14(3):212–217. https://doi.org/10.1016/j.knee.2007.01.001
Thompson SA, Liabaud B, Nellans KW, Geller JA (2013) Factors associated with poor outcomes following unicompartmental knee arthroplasty: redefining the “classic” indications for surgery. J Arthroplasty 28(9):1561–1564. https://doi.org/10.1016/j.arth.2013.02.034
Zhang K, Mihalko WM (2012) Posterior cruciate mechanoreceptors in osteoarthritic and cruciate-retaining TKA retrievals: a pilot study. Clin Orthop Relat Res 470(7):1855–1859. https://doi.org/10.1007/s11999-011-2120-7
Hogervorst T, Brand RA (1998) Mechanoreceptors in joint function. J Bone Joint Surg 80(9):1365–1378
Felts E, Parratte S, Pauly V, Aubaniac JM, Argenson JN (2010) Function and quality of life following medial unicompartmental knee arthroplasty in patients 60 years of age or younger. Orthop Traumatol Surg Res 96(8):861–867. https://doi.org/10.1016/j.otsr.2010.05.012
Walker T, Streit J, Gotterbarm T, Bruckner T, Merle C, Streit MR (2015) Sports, physical activity and patient-reported outcomes after medial unicompartmental knee arthroplasty in young patients. J Arthroplasty 30(11):1911–1916. https://doi.org/10.1016/j.arth.2015.05.031
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent is not required for this type of study.
Rights and permissions
About this article

Cite this article
Migliorini, F., Tingart, M., Niewiera, M. et al. Unicompartmental versus total knee arthroplasty for knee osteoarthritis. Eur J Orthop Surg Traumatol 29, 947–955 (2019). https://doi.org/10.1007/s00590-018-2358-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-018-2358-9