
Abstract
Introduction
The authors update their results of wrist hemiarthroplasty for irreparable distal radius fracture in the elderly, at a minimum of 2-year follow-up.
Materials and methods
Between 2011 and 2018, 25 consecutive independent elderly patients (24 female, 27 wrists) were treated with wrist hemiarthroplasty for distal radius fracture at a single institution. The average age was 77 years (range 65–88). They all were independent at home. A total of 19 wrists were treated at the acute stage, and 8 secondary procedures. The average follow-up was 32 months (range 24–44).
Results
There was no dislocation, loosening, infection nor removal of the implants. We observed 3 CRPS. At final follow-up, the average VAS pain was 1/10, mean forearm pronation/supination arc was 150°, and mean active flexion–extension arc was 60°. Average wrist extension was 36°. Mean grip strength was 68% of contralateral side. Mean Lyon wrist score was 74%. Mean Quick DASH score was 26%, and mean PRWE score was 25%.
Discussion
Our data suggest that treatment of acute irreparable distal radius fracture in the independent elderly patient with a bone-preserving primary wrist hemiarthroplasty may be a viable option. Longer-term follow-up are needed to confirm these preliminary data.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Volar plating for acute distal radius fractures (DRF) is widely used in elderly patients [1,2,3]. However, some recent papers emphasize both a significant percentage of complications and the lack of true clinical benefit [2, 4]. Other available treatment options include reduction and casting [4], percutaneous pinning, external fixation [2] or distraction plating [5]. It is the author’s opinion that none of these treatments is really satisfactory when faced with an irreparable acute DRF in an independent elderly patient. In a previous paper [6, 7], we proposed a definition of irreparable DRF.
Following the concept of treating acute complex fractures of the shoulder and elbow in the elderly with primary joint arthroplasty, several authors recently proposed to extend the concept to the wrist [8,9,10,11].
The purpose of this paper was to review our results of a preliminary prospective non-randomized series of wrist hemiarthroplasty for irreparable DRF in the independent elderly.
Materials and methods
Patients
Between 2011 and 2018, 25 consecutive independent elderly patients (24 female, 27 wrists) were treated with wrist hemiarthroplasty (WHA) for DRF at a single institution. The average age was 77 years (mini 65, maxi 88). All patients had some comorbidities, but they were all independent at home.
A total of 19 wrists were treated at the acute stage for acute irreparable DRF. The average time from injury to surgery was 4 days (1–7).
A total of 8 wrists sustained WHA as a secondary procedure (1 failed treatment of radio-carpal fracture-dislocation, 5 painful intra-articular malunions, 2 failed primary HWA for DRF). A total of 25 WHA were inserted with a press-fit, whereas 2 were cemented. A resection of the ulnar head was combined with the WHA in 21 wrists (77%).
A total of 16 wrists had clinical and radiological evaluation at more than 2 years of follow-up. The follow-up evaluation consisted of an interview, physical examination and standard anteroposterior (AP) and lateral radiographs. Follow-up clinical evaluation included VAS pain on a 10-points scale, Quick Dash, PRWE, evaluation of functional status, range of motion and grip strength. The Lyon wrist score [12] including information about pain, functional limitation with forearm rotation/wrist flexion–extension, active forearm rotation/wrist flexion–extension and grip strength (Jamar dynamometer) was used. The Lyon wrist score allows a diamond-shape representation of clinical results. The average follow-up was 32 months (24–44).
Follow-up radiological criteria included search for peri-prosthetic osteolysis as well as evaluation of translation of the carpus with respect to the distal cup of the implant. Coronal and sagittal inclination of the implant was also evaluated.
Surgical technique
The steps of the surgical technique have been reported elsewhere [6]. Briefly, the surgical approach was dorsal longitudinal in the midline of the wrist, in line with the third metacarpal. The third dorsal extensor compartment was exposed and entered longitudinally. The EPL tendon was elevated from the radio-carpal level to the distal third of the forearm and retracted. An osteotome was used to open the comminuted fracture like a book by elevating radially and ulnarly two 1-cm-thick osteo-tendinous flaps. The second and fourth extensor tendon compartments were left undisturbed. The convexity of the first carpal row was exposed through a 1-cm capsular incision, and the wrist was bent 80° on towels. The comminuted osteo-cartilaginous distal radius fragments were excised, while a peripheral layer of cancellous bone was preserved for later surrounding of the implant.
The radius diaphysis was then broached with the wrist in 90° flexion. During this step, the assistant kept the radial diaphysis in pronation with a bone clamp so that the flat part of the radial metaphysis was parallel to the floor. Avoiding any rotational malposition of the implant was made easier if the surgeon’s position was distal to the wrist and hand and not lateral or medial.
The implant was gently impacted into the radial canal. About 1.5 cm of implant was left out of the diaphysis to allow for further surrounding by the osteo-tendinous flaps and preservation of the radial length. Reduction of the carpus on the distal aspect of the trial implant was then performed. No more than 2 mm of pistoning was tolerated. Primary stability of the carpus within the distal cup of the implant was checked in both coronal and sagittal planes.
If the sigmoid notch fragments could be re-approximated, the ulnar head was left intact for DRUJ salvage. If the sigmoid notch fragments were non-reparable or if there was an associated ulnar head or neck fracture, the ulnar head was removed obliquely according to Watson.
The final implant was used without cement most of the time and was cemented in a few case where the bone quality was very poor.
The two thick peripheral osteo-tendinous flaps were brought back together as a closing book and sutured together with non-absorbable threaded sutures. Free cancellous bone was used around the implant to fill in the bony defects if necessary. The short dorsal capsule incision was closed with two non-absorbable monofilament sutures.
Postoperative care consisted of wrist immobilization in 20° extension in a long-arm cast for 3 weeks followed by a volar wrist splint in 20° wrist extension for 3 weeks. Gentle self-rehabilitation was begun at 3 weeks.
Results
There was no dislocation, loosening, infection nor removal of the implants. We observed 3 CRPS. All resolved within 18 months. One patient was re-operated 20 months after the index operation because of finger stiffness due to tendon adhesions at the wrist level along with a tendency to ulnar deviation of the wrist. We performed extensor tenolysis and transfer of ECRL to ECRB. At final follow-up, her clinical status was improved and the contact between the long finger tips and the palm was restored.
At final follow-up, the average VAS pain was 1/10 (range 0–3). Mean forearm pronation/supination arc was 150° (range 120°–170°). Mean active flexion–extension arc was 60° (range 30°–95°). Average wrist extension was 36° (mini 15, maxi 55°). Mean grip strength was 68% of contralateral side (8–100%). Mean Lyon wrist score was 74%. Mean Quick DASH score was 26%, and mean PRWE score was 25%. Among the 21 cases with combined ulnar head resection, no patient had symptomatic radio-ulnar impingement.
There was no subsidence of the implants, peri-prosthetic osteolysis nor significant worrisome erosion of the carpus. Bone healing around the implants was satisfactory in all but one case. One wrist showed a dorsal bone defect on the lateral view at 1-year follow-up. This defect was already present on the early postoperative radiographs suggesting insufficient dorsal bone coverage of the implant during the operation. We did not observe any translation of the carpus relative to the implant in the coronal or sagittal planes. Each implant remained well seated within the distal cup of the implant. An example of a case where we were able to keep the innate ulnar head is shown in Figs. 1, 2, 3, 4, 5 and 6.

Irreparable intra-articular distal radius fracture in an independent 70-year female

Same patient, lateral view

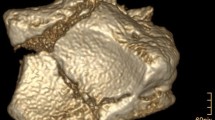
Same patient, CT scan coronal slice showing the impaction–separation type of displacement and suggesting that the sigmoid notch may be preserved during the arthroplasty procedure

Same patient, CT scan in sagittal plane confirmed a very distal and comminuted fracture not amenable to volar plating

Same patient, early postoperative PA radiograph showing the implant in place with DRUJ repair

Same patient, early postoperative lateral radiograph
Discussion
Our current data suggest that the use of WHA to treat irreparable DRF in the independent elderly patient as a primary or secondary procedure may be a viable option. Indeed, there are no really good options to treat what we defined as irreparable DRF [6, 7, 13] in elderly patients.
Closed reduction and casting may leave significant deformity and functional impairment [2, 3, 14].
Percutaneous pinning is doomed to failure due the very limited purchase into osteoporotic fractured fragments [1].
External fixation [3] in an elderly patient is cumbersome. Moreover, the ligamentotaxis of external fixation alone provides good reduction in the coronal plane but not in the sagittal plane [15].
Distraction plating has been proposed for severely comminuted DRF in elderly patients. However, the postoperative immobilization period is long and there is a potential for skin complications in the elderly [5].
Volar plating is currently the gold standard for displaced comminuted DRF in the elderly [1]. However, in Orbay’s study [1], only 33% were classified as AO-type “C” fractures. Arora [4] showed in a level I study that ORIF with volar plating in this group of patients did not provide any improvement in terms of function and range of motion when compared with closed reduction and cast immobilization. In our experience, successful volar plating is very difficult to achieve in so-called irreparable DRF in elderly and secondary displacement frequently occurs.
According to the concept used in the shoulder and elbow [16,17,18], Roux was the first to propose to treat complex comminuted DRF in the elderly with WHA [9, 10]. Within Roux’s series, there were 6 cases of acute DRF in the elderly that were treated with primary WHA. The results of this subgroup were not specifically addressed. Using the same implant, Vergnenegre [8] reported 8 cases with satisfactory functional results and no implant removal at an average follow-up of 27 months. However, this implant was massive. In case of implant removal, the loss of substance would be difficult to reconstruct. The use of this implant is contra-indicated if the DRF is associated with an ulnar neck or head fracture. This is not the case with the bone-preserving WHA used in our series or in other series [11].
Metal on cartilage contact between the implant and the convexity of the articular cartilage of the proximal carpal row is not the best contact for an arthroplasty. However, metal on cartilage contact is well accepted for shoulder and elbow salvage procedures from acute trauma since the benefits outweigh the drawbacks. Moreover, WHA was recently proposed for treatment of wrist arthritis.
Long-term follow-up studies are needed to confirm the usefulness of WHA to treat irreparable DRF in autonomous elderly patients.
References
Orbay JL, Fernandez DL (2004) Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. YJHSU 29:96–102
Day CS, Daly MC (2012) Management of geriatric distal radius fractures. J Hand Surg 37:2619–2622. https://doi.org/10.1016/j.jhsa.2012.07.038
Brogan DM, Ruch DS (2015) Distal radius fractures in the elderly. J Hand Surg 40:1217–1219. https://doi.org/10.1016/j.jhsa.2015.01.001
Arora R, Lutz M, Deml C et al (2011) A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am 93:2146–2153. https://doi.org/10.2106/JBJS.J.01597
Richard MJ, Katolik LI, Hanel DP et al (2012) Distraction plating for the treatment of highly comminuted distal radius fractures in elderly patients. J Hand Surg 37:948–956. https://doi.org/10.1016/j.jhsa.2012.02.034
Herzberg G, Burnier M, Marc A, Izem Y (2015) Primary wrist hemiarthroplasty for irreparable distal radius fracture in the independent elderly. J Wrist Surg 04:156–163. https://doi.org/10.1055/s-0035-1558841
Herzberg G, Burnier M (2016) What is the role of primary or secondary hemiarthroplasty for distal radius fractures in independent elderly patients? Hand Surg Rehabil 35S:S137–S140. https://doi.org/10.1016/j.hansur.2016.03.004
Vergnenègre G, Mabit C, Charissoux J-L et al (2014) Treatment of comminuted distal radius fractures by resurfacing prosthesis in elderly patients. Chir Main 33:112–117. https://doi.org/10.1016/j.main.2014.01.007
Roux J-L (2009) Replacement and resurfacing prosthesis of the distal radius: a new therapeutic concept. Chir Main 28:10–17. https://doi.org/10.1016/j.main.2008.11.009
Roux J-L (2011) Treatment of intra-articular fractures of the distal radius by wrist prosthesis. Orthop Traumatol Surg Res 97S:S46–S53
Ichihara S, Díaz JJH, Peterson B et al (2015) Distal radius isoelastic resurfacing prosthesis: a preliminary report. J Wrist Surg 4:150–155. https://doi.org/10.1055/s-0035-1556855
Herzberg G, Burnier M, Nakamura T (2018) A new wrist clinical evaluation score. J Wrist Surg 07:109–114. https://doi.org/10.1055/s-0037-1607328
Herzberg G, Merlini L, Burnier M (2017) Hemi-arthroplasty for distal radius fracture in the independent elderly. Orthop Traumatol Surg Res. https://doi.org/10.1016/j.otsr.2017.03.029
Brogan DM, Richard MJ, Ruch D, Kakar S (2015) Management of severely comminuted distal radius fractures. J Hand Surg 40:1905–1914. https://doi.org/10.1016/j.jhsa.2015.03.014
Bartosh RA, Saldana MJ (1990) Intraarticular fractures of the distal radius: a cadaveric study to determine if ligamentotaxis restores radiopalmar tilt. YJHSU 15:18–21
Schultzel M, Scheidt K, Klein CC et al (2017) Hemiarthroplasty for the treatment of distal humeral fractures: midterm clinical results. J Shoulder Elbow Surg 26:389–393. https://doi.org/10.1016/j.jse.2016.09.057
Shukla DR, McAnany S, Kim J et al (2016) Hemiarthroplasty versus reverse shoulder arthroplasty for treatment of proximal humeral fractures: a meta-analysis. J Shoulder Elbow Surg 25:330–340. https://doi.org/10.1016/j.jse.2015.08.030
Desai SJ, Lalone E, Athwal GS et al (2016) Hemiarthroplasty of the elbow: the effect of implant size on joint congruency. J Shoulder Elbow Surg 25:297–303. https://doi.org/10.1016/j.jse.2015.09.022
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The senior author of this paper has a conflict of interests with this paper.
Rights and permissions
About this article

Cite this article
Herzberg, G., Walch, A. & Burnier, M. Wrist hemiarthroplasty for irreparable DRF in the elderly. Eur J Orthop Surg Traumatol 28, 1499–1503 (2018). https://doi.org/10.1007/s00590-018-2228-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-018-2228-5