
Abstract
Introduction
Distal radius fractures (DRFs) are very common. One of the most significant complications after intraarticular DRF is arthrofibrosis with loss of wrist motion and pain. Wrist arthroscopy has become increasingly popular in the treatment of DRF with the advantage of good visualization of the joint surface and soft tissue injuries. In intraarticular DRFs injuries of the dorsal capsule are a characteristic finding which potentially cause loss of wrist motion. In this study, we investigated if arthroscopic debridement of dorsal capsule injuries at time of surgical fixation provides superior outcomes compared to the same treatment without debridement.
Materials and methods
Between 2013 and 2017, we included 42 patients who underwent arthroscopy-assisted palmar plating for intraarticular DRFs in a prospective randomized controlled study. In group A (intervention group), the dorsal capsule tears were debrided during primary surgery, while in group B these were left in place. Active range of motion (AROM), grip strength, subjective outcomes and radiographic results were assessed 3, 6 and 12 months after primary surgery. A subgroup analysis was performed for patient age, fracture severity and duration of immobilization.
Results
Arthroscopic debridement of the dorsal capsule improved AROM in patients over 60 years of age, more severe fractures (AO 23 C2/C3) and prolonged postoperative immobilization for more than two weeks, while it was not relevant for younger patients with simple fractures and short immobilization.
Conclusions
Debridement of the injured dorsal capsule in arthroscopic-assisted surgical treatment of intraarticular DRFs can improve surgical performance and optimize patient outcomes in a specific subgroup of patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Distal radius fractures (DRFs) are common injuries accounting for 15% of all fractures [1]. The incidence of intraarticular patterns is variable and can be more than 50% [2, 3].
The goal in the management of intraarticular DRFs is anatomical reduction of the articular surface in addition to restoration of extraarticular alignment. This plays an important role in the prevention of posttraumatic arthritis [4, 5].
Wrist arthroscopy has become increasingly popular in the treatment of DRFs. Arthroscopy provides direct visualization of the articular surface, ligaments and TFCC complex, which allows accurate fracture reduction and soft tissue diagnosis and treatment in an acute setting [1].
DRFs have a high incidence of associated lesions, including chondral and soft tissue injuries such as triangular fibrocartilage complex (TFCC), scapholunate (SL) ligament, lunotriquetral (LT) ligament or extrinsic ligament tears [6, 7]. These injuries are relevant for the stability and must be addressed to avoid long-term consequences of instability leading to osteoarthritis and pain.
Research on soft tissue injuries associated with DRFs focuses mainly on structures relevant for the stability of the wrist and soft tissues without or little importance for stability have been mostly neglected with a lack of evidence clarifying their clinical relevance.
One of those non-stability-related soft tissue injuries are injuries of the joint capsule, which is relevant for joint function. In the wrist, it is more tight on the volar side with close relationship to the volar radiocarpal and ulnocarpal ligaments preventing a volar shift of the carpals. On the dorsal side, it is more loose forming a dorsal recess and hereby allowing a wide range of motion with less restrictive ligament guidance.
In intraarticular DRFs, injuries of the dorsal joint capsule are a characteristic finding, which potentially cause loss of wrist motion. A retrospective study on 20 patients with limited wrist motion after intraarticular DRFs caused by arthrofibrosis described the location and mechanical characteristics of fibrous tissue formations. These motion limiting scars originated mostly from the dorsal capsule—the area of the primary soft tissue injury—often filling or blocking the dorsal recess. This limited the normal carpal gliding [8].
Starting from this observation injuries of the dorsal capsule seem to be a source in the development of motion limiting arthrofibrosis and therefore, debridement of soft tissue flaps of the dorsal capsule may avoid intraarticular scar formation.
Aim of our study was to assess if arthroscopic debridement of the dorsal capsule injuries at the time of surgical fixation of intraarticular DRFs improves outcomes.
Materials and methods
Patients
We included 42 adult patients (12 males, 30 females) with a mean age of 54.4 years (min. 20, max. 76 years) in a prospective randomized controlled study.
All patients were treated for intraarticular fractures of the distal radius and underwent arthroscopic assisted volar plate osteosynthesis by three specialized hand surgeons with substantial experience in wrist arthroscopy between 2013 and 2017. The dominant hand was involved in 18 patients.
Institutional research ethics committee approved the study (registration number AN4991) and written informed consent was obtained from all patients.
X-ray and CT scans were performed preoperatively. Using the AO trauma classification for distal radius fractures, we observed C3 (10), C2 (17), C1 (11), B3 (1) and B2 (3) fractures.
Patient-blinded randomization was performed at the day of surgery. Group A (intervention group) consisted of 20 patients (5 males, 15 females). Group B (control group) included 22 patients (7 males, 15 females).
In group A, the typically present dorsal capsule tears were debrided during primary surgery, while in group B these were left in place.
To assess the clinical impact of arthroscopic debridement at primary surgery, outcome parameters comprised objective outcomes (ROM, Grip strength), subjective outcomes (VAS, DASH, PRWE) and radiographic examination. These parameters were assessed 3, 6 and 12 months after primary surgery.
At the time of implant removal, the joint was reexamined by arthroscopy and intraarticular adhesions were debrided up to the border of the original capsule.
A subgroup analysis was performed for the parameters patient age (age below or above 60 years), fracture severity (B and C1 fractures vs. C2 and C3 fractures) and immobilization time (more or less than 2 weeks).
Surgical technique
Volar plating was performed over a standard palmar approach using angular stable locking plates (APTUS® Wrist Distal Radius-System, Medartis®, Basel).
Arthroscopy-guided reduction was performed with a 2.7 mm wrist scope in dry technique using the dorsal radiocarpal portals between the third and fourth extensor compartment (3/4) and radial to the sixth extensor compartment (6R).
The dorsal capsule was injured in all cases. Minor injuries to the TFCC or SL ligament were frequently observed but none of these additional injuries required specific treatment.
Arthroscopic debridement was performed with a 2.5 mm shaver according to the randomization following the study protocol. All free floating or protruding capsular flaps were removed up to a stable rim, without a complete resection of the capsule.
The immediate postoperative protocol included elevation, cryotherapy, adequate analgesic therapy and instructions for range-of-motion exercises for joints that were not immobilized. Passive and active wrist motion exercises commenced after cast removal. The duration of immobilization was defined by the treating surgeon according to intraoperative assessment of the risk of secondary dislocation. The mean immobilization time was 18.3 days (min. 0 days, max. 29 days). All patients received hand therapy 2–3 times a week for at least 3 months in an outpatient setting.
Outcomes
The functional objective and subjective outcomes were measured 12 weeks, 6 months and 12 months after primary surgery.
Objective outcomes (ROM, Grip strength)
Range of motion (ROM) measurements were performed using a goniometer.
Measurements of ROM included extension/flexion, radial/ulnar abduction and supination/ pronation of the wrist.
Grip strength was measured with a Baseline Dynamometer (Irvington, NY, USA). Grip strength was calculated as the mean of three measurements and expressed in kilograms.
Subjective outcomes (VAS, DASH, PRWE)
Patients self-reported pain using a visual analog scale (VAS) where zero means no pain and ten the worst pain possible.
Subjective outcomes were assessed using the Disability of Arm, Shoulder and Hand (DASH) and the patient related Wrist Evaluation (PRWE) questionnaires. In the DASH and PRWE surveys, outcomes are measured from 0 to 100 with lower scores corresponding to less disability.
Radiographic examination
Radiographic examination of the wrist was performed in standard posteroanterior projection (shoulder 90° adducted, elbow flexed 90° and forearm in neutral rotation) and lateral projection (shoulder adducted, elbow 90° of flexion, hand positioned in the same plane as the humerus) before and after surgery at all follow-up appointments.
Statistics
All values are expressed as means ± standard deviations. Significance was established at p < 0.05. The data were tested for normal distribution using the Kolmogorov–Smirnov test. Outcome parameters of the two groups were compared using the paired t test for parametric data. Nonparametric data were analyzed by the Wilcoxon signed rank test for paired differences. Statistical analyses were conducted with the SPSS software package (SPSS version 24.0, IBM Corp, Armonk, NY).
Results
Objective outcomes (ROM, grip strength)
ROM and grip strength improved in both groups between 12 weeks postop and the last follow-up before implant removal after 12 months.
Comparing the two groups, ROM in group A showed better results than group B. This was statistically significant for ROM extension at the 12-month follow-up.
A subgroup analysis was performed for the parameters patient age (age below vs. above 60 years), fracture severity (B and C1 fractures vs. C2 and C3 fractures) and immobilization time (more vs. less than 2 weeks).
Table 1 shows the results of the subgroup analysis for the parameter of patient age. Comparing patients above 60 years (17 out of 42), in the debridement group A patients had statistically significant better results at the 12-week follow-up for pronation (0.045), the 6-month follow-up for extension (0.024) flexion (0.015) and ulnar abduction (0.035), and at the 12-month follow-up for the sagittal plane (0.035).
Table 2 shows the results of the subgroup analysis of fracture severity. In cases with more severe fractures, types C2 and C3 (27 out of 42) extension was significantly higher in the debridement group A at the 6- and 12-month follow-up (p = 0.041 and p = 0.04), while there was no difference found in other fracture types.
Table 3 shows patients that were immobilized more than 2 weeks after surgery (28 out of 42). Extension at the 6- and 12-month follow-up was significantly higher in the debridement group A (p = 0.039 and p = 0.037).
Subjective outcomes (VAS/DASH/PRWE)
The scores improved in both groups from 12 weeks after surgery to the final follow-up.
Comparing the two groups, VAS, DASH and PRWE scores in group A had better overall results than group B. Only in the subgroup of patients above 60 years, the differences were statistically significant for the DASH score at the 12-month follow-up (p = 0.04) (Table 4).
Radiological outcomes
No loss of reduction occurred in our patient population. In all cases, sufficient quality of reduction could be achieved. It was defined as Radial Inclination > 15°, Dorsal Tilt < 5°, Ulnar Variance ± 2 mm. Between patients of group A and B, no significant differences were found.
Case example
This case example illustrates an AO-type C2 fracture in a 64-year-old female patient. Figure 1 shows a 3D CT reconstruction depicting the intraarticular fracture pattern. Arthroscopic-assisted fracture reduction was performed and residual capsule flaps were left in place according to randomization in control group B (Fig. 2). A cast was applied for 3 weeks.

3D CT reconstruction of a AO23 C2 fracture with direct view on the joint surface from distal. Three-part fracture with a bony avulsion of the long radiolunate ligament at the volar rim

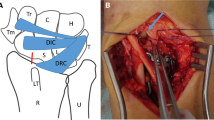
Arthroscopic view on the reduced joint line through the 3/4 portal. Residual capsule flaps (black arrows) are seen on the volar (a) and on the dorsal (b) side
One year after primary surgery, sagittal wrist motion was still impaired in the sagittal plane especially wrist flexion. Implant removal and arthroscopy were performed. Mechanically relevant arthrofibrosis could be found and was debrided (Fig. 3). Debridement increased sagittal ROM shown by intraoperative fluoroscopy (Fig. 4).

Arthroscopic images at the time of implant removal. (a) The view through the 3/4 portal shows fibrous tissue formations along the former fracture line on the volar and on the dorsal side leaving a window in between representing a type 2a arthrofibrosis according to Gabl et al. [8] (b) View from the 6R portal after debridement

Fluoroscopic images of the wrist in a sagittal plane with tension free full extension and flexion, respectively, after implant removal (top row) and after arthroscopic debridement (bottom row)
Discussion
Distal radius fractures are very common injuries. Treatment aims to restore normal anatomy [9]. It has been shown that an articular step-off of 1–2 mm is correlated with the development of degenerative changes, and articular congruity of less than 1 mm reduces the possibility of developing posttraumatic arthritis and hence should be restored [4, 5, 10,11,12,13]. Some studies, however, did not find any correlation between the residual step-off or gap and final outcomes [14, 15].
Arthroscopy
Wrist arthroscopy has emerged as a useful adjunct procedure in the surgical management of distal radius fractures and a method of evaluating and treating many intraarticular wrist conditions [16].
Arthroscopic-assisted reduction is used to reduce gaps and step offs to minimize cartilage free areas that may serve as attachment points for intraarticular scarring. Fracture reduction may be better appreciated during arthroscopy compared to fluoroscopic assessment [13, 17]. Edwards et al. reported that arthroscopy may help to identify residual gapping of the articular surface not detected with fluoroscopy [18]. Abe et al. reported that 35% of patients who seemed to achieve perfect reduction at fluoroscopy in reality had a step-off or gap > 2 mm [19]. Another study reported that arthroscopy after fluoroscopic reduction resulted in a modification of the treatment in five of seven patients [20].
However, the use of arthroscopy in management of DRFs remains controversial and the question remains, whether or not arthroscopically assisted treatment provides better outcomes [21,22,23].
Doi et al. performed a prospective study and reported better results in the arthroscopic-assisted group [24]. Ruch et al. compared 15 fractures treated with arthroscopy-assisted reduction and percutaneous pinning versus 15 fractures with fluoroscopic-assisted reduction and reported better ROM in the arthroscopy group, but no difference in DASH, grip strength and radiographic outcomes [23]. Varitimidis et al [22] compared 20 patients treated with arthroscopy versus 20 fractures treated with fluoroscopic-assisted reduction and reported a better DASH, Mayo Wrist Score, ROM and grip strength in the arthroscopy group. Yamazaki et al. used volar locking plates and identified no difference [25].
Despite the potential benefits of wrist arthroscopy, one has also to mention potential disadvantages. Complications like infections, nerve or tendon injuries, although very low in number, have been reported [26]. Also, the need for special equipment and expertise as well as an increase of operating time has to be considered. Despite these considerations, wrist arthroscopy as a tool enriches the understanding of wrist pathologies and enables the development of further treatment strategies, with arthroscopic-assisted reduction being only one possible application.
Soft tissue injuries
Arthroscopy allows to visualize acute chondral lesions of the distal radius joint surface, seen as hematomas, cracks, avulsed cartilage flakes or complete avulsions of the cartilage. Arthroscopic debridement is currently the only treatment option in these cases [27].
Wrist arthroscopy has become the gold standard in assessment and management of concomitant injuries such as intercarpal ligament injuries, TFCC injuries and chondral pathology [6, 28,29,30,31]. Without arthroscopy, concomitant ligamentous and TFCC injuries may be misdiagnosed or underestimated [32].
The incidence of associated ligament injuries has been variously reported and is not uniform [1]. TFCC injuries are found in around 60%, lesions of the SL ligament in around 40% of DRFs. LT injuries are less commonly found in 20% of cases [22, 33].
The question remains whether these injuries are clinically relevant and should be addressed at the time of osteosynthesis of the distal radius. Only a small number of studies have investigated outcomes of non-treated soft tissue injuries [32].
A wash out of the fracture hematoma and debris was thought to potentially improve the ROM and reduce the inflammatory response [19, 21, 24].
Selles et al. investigated if arthroscopically assisted debridement of intraarticular fracture hematoma and debris may improve the functional outcomes after operative treatment of intraarticular DRFs in 50 patients. The patients were randomized between ORIF with arthroscopy and conventional ORIF. No significantly differences in PRWE, ROM and Grip strength could be found. Additional soft tissue injuries were left untreated with good functional outcomes [34].
Arthrofibrosis
Wrist stiffness and decreased range of motion are common complications following trauma or surgery of DRFs. This usually resolves with physiotherapy. Cases that remain refractory to this treatment are primarily caused by arthrofibrosis [35].
Arthrofibrosis can develop as an excessive response to trauma. While pathology of primary arthrofibrosis is seen as a general fibrotic reaction, secondary arthrofibrosis leads to reduced motion due to a local fibrotic healing response [36].
To prevent wrist stiffness, reduced immobilization time and early motion are desirable, but not possible or feasible in all cases. This is especially true in older patients with poor quality bone stock and more severe fractures.
Treatments to improve range of motion (ROM) in cases of wrist stiffness are physical therapy or antifibrotic drugs. Surgical procedures include open or arthroscopic debridement, capsular release or wrist arthrolysis [37,38,39].
Several studies have shown that the debridement of arthrofibrosis in patients with restricted wrist motion could improve function [40,41,42].
Verhellen described arthroscopic capsular release in two patients with limited wrist mobility with significant improvement in range of motion [40]. Hattori et al. have reported on arthroscopic treatment of wrist intraarticular adhesions. Arthroscopic release was effective in improving range of wrist motion [41]. Luchetti et al. evaluated 22 patients with stiffness after wrist fracture who underwent arthroscopic arthrolysis. The procedure reduced pain and improved wrist flexion and extension and grip strength significantly [42].
Nevertheless, the main goal of treatment should be to prevent a stiff wrist in the first place. For this, it must be known from where and from which tissue scars originate.
While the extent of cartilage free areas, namely gaps and step offs are minimized as well as intrinsic ligament or TFCC injuries are already addressed by arthroscopic-assisted reduction, non-stability relevant injuries like capsular tears have been neglected so far.
Tears of the dorsal capsule, however, are a characteristic arthroscopic finding in intraarticular DRFs and present in the form of soft tissue flaps that protrude into the joint. These, together with cartilage free areas at the joint line, may form the substrate for the development of arthrofibrosis.
Gabl et al. investigated arthrofibrosis patterns after surgically treated intraarticular DRFs and found the fibrotic tissue exclusively between former fracture gaps, and areas of former soft tissue injury namely the SL ligament and the dorsal capsule, respectively. These structures seem to be involved in the formation of arthrofibrosis causing loss of radiocarpal motion [8].
In our study, we investigated whether primary arthroscopic debridement of dorsal capsular flaps in the acute treatment of DRFs improves outcomes. The goal was to debride unstable flaps that are likely to catch on surrounding tissue and hereby reduce the substrate for scarring.
Prolonged immobilization is seen as a main risk factor for the development of arthrofibrosis. According to a recent study by Zeckey et al., it does not improve the outcome of most patients and should remain reserved to a patient group with a high risk of secondary dislocation [43]. Accordingly, we found that for the subgroup of patients with an age above 60 years, more severe fractures (AO types C2 and C3) and immobilization for more than two weeks the debridement of the injured dorsal capsule could improve functional outcomes. The debridement seems to impede intraarticular scar formation and counteracts the development of clinically relevant arthrofibrosis and its negative effects on wrist motion and pain. This approach may lead to equally good functional results under worse starting conditions.
In patients below 60 years of age with good bone stock and simple fractures where an exercise stable osteosynthesis can be achieved after arthroscopic-assisted reduction, short-term splinting until suture removal and early motion exercises may achieve favorable results. In this patient group, no effect of arthroscopic debridement can be expected.
If no primary debridement is performed, secondary arthroscopic debridement at the time of implant removal is able to improve the functional outcome after intraarticular DRFs, as has been shown in our case example and previous studies [40,41,42].
A limitation of our study is the low patient number, which is nevertheless within the range of comparable research.
Conclusion
Debridement of the injured dorsal capsule in arthroscopy-assisted volar plating of intraarticular DRFs had encouraging results in improving outcomes in a specific subset of patients.
References
Smeraglia F, Del Buono A, Maffulli N (2016) Wrist arthroscopy in the management of articular distal radius fractures. Br Med Bull 119(1):157–165. https://doi.org/10.1093/bmb/ldw032
Bentohami A, Bosma J, Akkersdijk GJ, van Dijkman B, Goslings JC, Schep NW (2014) Incidence and characteristics of distal radial fractures in an urban population in The Netherlands. Eur J Trauma Emerg Surg 40(3):357–361. https://doi.org/10.1007/s00068-014-0394-7
Pechlaner S, Gabl M, Lutz M, Krappinger D, Leixnering M, Krulis B, Ulmer H, Rudisch A, Arbeitsgruppe A (2007) Distal radius fractures–aetiology, treatment and outcome. Handchir Mikrochir Plast Chir 39(1):19–28. https://doi.org/10.1055/s-2007-964920
Knirk JL, Jupiter JB (1986) Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 68(5):647–659
Fernandez DL, Geissler WB (1991) Treatment of displaced articular fractures of the radius. J Hand Surg Am 16(3):375–384. https://doi.org/10.1016/0363-5023(91)90001-r
Geissler WB, Freeland AE, Savoie FH, McIntyre LW, Whipple TL (1996) Intracarpal soft-tissue lesions associated with an intra-articular fracture of the distal end of the radius. J Bone Jt Surg Am 78(3):357–365. https://doi.org/10.2106/00004623-199603000-00006
Swart E, Tang P (2017) The effect of ligament injuries on outcomes of operatively treated distal radius fractures. Am J Orthop (Belle Mead NJ) 46(1):E41–E46
Gabl M, Arora R, Klauser AS, Schmidle G (2016) Characteristics of secondary arthrofibrosis after intra-articular distal radius fracture. Arch Orthop Trauma Surg 136(8):1181–1188. https://doi.org/10.1007/s00402-016-2490-0
Anderson DD, Bell AL, Gaffney MB, Imbriglia JE (1996) Contact stress distributions in malreduced intraarticular distal radius fractures. J Orthop Trauma 10(5):331–337. https://doi.org/10.1097/00005131-199607000-00007
Geissler WB, Fernandez DL (1991) Percutaneous and limited open reduction of the articular surface of the distal radius. J Orthop Trauma 5(3):255–264. https://doi.org/10.1097/00005131-199109000-00002
Trumble TE, Schmitt SR, Vedder NB (1994) Factors affecting functional outcome of displaced intra-articular distal radius fractures. J Hand Surg Am 19(2):325–340. https://doi.org/10.1016/0363-5023(94)90028-0
Trumble TE, Wagner W, Hanel DP, Vedder NB, Gilbert M (1998) Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 23(3):381–394. https://doi.org/10.1016/S0363-5023(05)80455-1
Ono H, Katayama T, Furuta K, Suzuki D, Fujitani R, Akahane M (2012) Distal radial fracture arthroscopic intraarticular gap and step-off measurement after open reduction and internal fixation with a volar locked plate. J Orthop Sci 17(4):443–449. https://doi.org/10.1007/s00776-012-0226-8
Catalano LW 3rd, Cole RJ, Gelberman RH, Evanoff BA, Gilula LA, Borrelli J Jr (1997) Displaced intra-articular fractures of the distal aspect of the radius. Long-term results in young adults after open reduction and internal fixation. J Bone Jt Surg Am 79(9):1290–1302. https://doi.org/10.2106/00004623-199709000-00003
Goldfarb CA, Rudzki JR, Catalano LW, Hughes M, Borrelli J Jr (2006) Fifteen-year outcome of displaced intra-articular fractures of the distal radius. J Hand Surg Am 31(4):633–639. https://doi.org/10.1016/j.jhsa.2006.01.008
Geissler WB, Freeland AE (1999) Arthroscopic management of intra-articular distal radius fractures. Hand Clin 15(3):455–465 (viii)
Lutsky K, Boyer MI, Steffen JA, Goldfarb CA (2008) Arthroscopic assessment of intra-articular distal radius fractures after open reduction and internal fixation from a volar approach. J Hand Surg Am 33(4):476–484. https://doi.org/10.1016/j.jhsa.2007.12.009
Edwards CC 2nd, Haraszti CJ, McGillivary GR, Gutow AP (2001) Intra-articular distal radius fractures: arthroscopic assessment of radiographically assisted reduction. J Hand Surg Am 26(6):1036–1041. https://doi.org/10.1053/jhsu.2001.28760
Abe Y, Yoshida K, Tominaga Y (2013) Less invasive surgery with wrist arthroscopy for distal radius fracture. J Orthop Sci 18(3):398–404. https://doi.org/10.1007/s00776-013-0371-8
Auge WK 2nd, Velazquez PA (2000) The application of indirect reduction techniques in the distal radius: the role of adjuvant arthroscopy. Arthroscopy 16(8):830–835. https://doi.org/10.1053/jars.2000.17717
Geissler WB (2005) Intra-articular distal radius fractures: the role of arthroscopy? Hand Clin 21(3):407–416. https://doi.org/10.1016/j.hcl.2005.02.009
Varitimidis SE, Basdekis GK, Dailiana ZH, Hantes ME, Bargiotas K, Malizos K (2008) Treatment of intra-articular fractures of the distal radius: fluoroscopic or arthroscopic reduction? J Bone Jt Surg Br 90(6):778–785. https://doi.org/10.1302/0301-620X.90B6.19809
Ruch DS, Vallee J, Poehling GG, Smith BP, Kuzma GR (2004) Arthroscopic reduction versus fluoroscopic reduction in the management of intra-articular distal radius fractures. Arthroscopy 20(3):225–230. https://doi.org/10.1016/j.arthro.2004.01.010
Doi K, Hattori Y, Otsuka K, Abe Y, Yamamoto H (1999) Intra-articular fractures of the distal aspect of the radius: arthroscopically assisted reduction compared with open reduction and internal fixation. J Bone Jt Surg Am 81(8):1093–1110. https://doi.org/10.2106/00004623-199908000-00005
Yamazaki H, Uchiyama S, Komatsu M, Hashimoto S, Kobayashi Y, Sakurai T, Kato H (2015) Arthroscopic assistance does not improve the functional or radiographic outcome of unstable intra-articular distal radial fractures treated with a volar locking plate: a randomised controlled trial. Bone Jt J 97-B(7):957–962. https://doi.org/10.1302/0301-620X.97B7.35354
Leclercq C, Mathoulin C, Members of E (2016) Complications of wrist arthroscopy: a multicenter study based on 10,107 arthroscopies. J Wrist Surg 5(4):320–326. https://doi.org/10.1055/s-0036-1584163
Lindau T (2017) Arthroscopic evaluation of associated soft tissue injuries in distal radius fractures. Hand Clin 33(4):651–658. https://doi.org/10.1016/j.hcl.2017.07.015
Adolfsson L, Jorgsholm P (1998) Arthroscopically-assisted reduction of intra-articular fractures of the distal radius. J Hand Surg Br 23(3):391–395. https://doi.org/10.1016/s0266-7681(98)80065-x
Richards RS, Bennett JD, Roth JH, Milne K Jr (1997) Arthroscopic diagnosis of intra-articular soft tissue injuries associated with distal radial fractures. J Hand Surg Am 22(5):772–776. https://doi.org/10.1016/S0363-5023(97)80068-8
Lindau T, Adlercreutz C, Aspenberg P (2000) Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am 25(3):464–468. https://doi.org/10.1053/jhsu.2000.6467
Forward DP, Lindau TR, Melsom DS (2007) Intercarpal ligament injuries associated with fractures of the distal part of the radius. J Bone Joint Surg Am 89(11):2334–2340. https://doi.org/10.2106/JBJS.F.01537
Shkolnikova J, Harvey J (2018) Wrist arthroscopy in the management of distal radius fractures. Annal Jt 3:77
Khanchandani P, Badia A (2013) Functional outcome of arthroscopic assisted fixation of distal radius fractures. Indian J Orthop 47(3):288–294. https://doi.org/10.4103/0019-5413.109872
Selles CA, Mulders MAM, Colaris JW, van Heijl M, Cleffken BI, Schep NWL (2020) Arthroscopic debridement does not enhance surgical treatment of intra-articular distal radius fractures: a randomized controlled trial. J Hand Surg Eur 45(4):327–332. https://doi.org/10.1177/1753193419866128
Bain GI, Munt J, Turner PC, Bergman J (2008) Arthroscopic dorsal capsular release in the wrist: a new technique. Tech Hand Up Extrem Surg 12(3):191–194. https://doi.org/10.1097/BTH.0b013e3181839bb4
Bosch U (2002) Arthrofibrosis. Orthopade 31(8):785–790. https://doi.org/10.1007/s00132-002-0336-7
Lee SK, Gargano F, Hausman MR (2006) Wrist arthrofibrosis. Hand Clin 22(4):529–538. https://doi.org/10.1016/j.hcl.2006.09.002 (abstract vii)
Steplewski A, Fertala J, Beredjiklian PK, Abboud JA, Wang MLY, Namdari S, Barlow J, Rivlin M, Arnold WV, Kostas J, Hou C, Fertala A (2017) Blocking collagen fibril formation in injured knees reduces flexion contracture in a rabbit model. J Orthop Res 35(5):1038–1046. https://doi.org/10.1002/jor.23369
Tang X, Teng S, Petri M, Krettek C, Liu C, Jagodzinski M (2018) The effect of anti-inflammatory and antifibrotic agents on fibroblasts obtained from arthrofibrotic tissue: an in vitro and in vivo study. Bone Jt Res 7(3):213–222. https://doi.org/10.1302/2046-3758.73.BJR-2017-0219.R2
Verhellen R, Bain GI (2000) Arthroscopic capsular release for contracture of the wrist: a new technique. Arthroscopy 16(1):106–110. https://doi.org/10.1016/s0749-8063(00)90137-3
Hattori T, Tsunoda K, Watanabe K, Nakao E, Hirata H, Nakamura R (2006) Arthroscopic mobilization for contracture of the wrist. Arthroscopy 22(8):850–854. https://doi.org/10.1016/j.arthro.2006.04.099
Luchetti R, Atzei A, Fairplay T (2007) Arthroscopic wrist arthrolysis after wrist fracture. Arthroscopy 23(3):255–260. https://doi.org/10.1016/j.arthro.2006.11.001
Zeckey C, Spath A, Kieslich S, Kammerlander C, Bocker W, Weigert M, Neuerburg C (2020) Early mobilization versus splinting after surgical management of distal radius fractures. Dtsch Arztebl Int 117(26):445–451. https://doi.org/10.3238/arztebl.2020.0445
Funding
No disclosures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Gernot Schmidle, Stefan Benedikt, Tobias Kastenberger, Peter Kaiser, Rohit Arora, and Markus Gabl declare that they have no conflict of interest.
Ethical approval
The study was approved by the local ethics committee (ethics committee of the Medical University Innsbruck, AN 20131161 323/4.2).
Informed consent
Informed consent was obtained from all study participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 222501 KB)
Rights and permissions
About this article

Cite this article
Schmidle, G., Benedikt, S., Kastenberger, T. et al. Arthroscopic debridement of the dorsal capsule in intraarticular distal radius fractures: does it provide superior outcomes?. Arch Orthop Trauma Surg 142, 691–699 (2022). https://doi.org/10.1007/s00402-021-04246-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-04246-8