
Abstract
Background
Giant cell tumor of the spine has high rate of postoperative recurrence. There are not much published studies on repeatedly recurrent GCTS (RRGCTS). Also, there are controversies as to the prognostic factors and treatment options for RRGCTS.
Methods and materials
A retrospective survival analysis between 2000 and September 2014 was performed on the 74 times of in-hospital treatment of the 21 patients. Recurrence-free survival was defined as the time between the date of surgery and the date of recurrence. Factors with P values <0.05 in univariate analysis were subjected to multivariate analysis by means of proportional hazard analysis.
Result
A total of 21 patients comprising ten males and 11 females with a mean age of 29.7 years (range 15–49) were included, with a total of 74 times of surgery performed. Eighteen patients had no evidence of disease. Univariate and multivariate analysis suggested that total spondylectomy and bisphosphonate therapy were independent prognostic factors for better RFS in RRGCTS patients.
Conclusion
Patients of RRGCTS are suitable for further surgical treatment with relatively good healing process and restoration of nervous function. Early diagnosis of recurrence may be associated with better prognosis. Total spondylectomy in combination with bisphosphonate therapy could reduce postoperative recurrence rate.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Giant cell tumor of the bone (GCT) is a benign bone tumor but with high rate of local recurrence [1]. About 3 to 6 % of patients present with GCT of the spine (GCTS) and the postoperative recurrence rate is reported to be as high as 25 to 50 % [2–4]. Recurrent GCTS (RGCTS), especially repeatedly RGCTS (RRGCTS), requires special attention in that it usually presents with disorganized anatomical structures, heavy neurological deficits and great surgical obstacles because of compromised health state.
The treatment strategy and clinical behaviors of primary GCTS have been well described [5, 6]. As for RRGCTS, there have been only a few published case series of recurrent GCT in the extremities advocating that surgery could achieve reasonable chance of success [6, 7]. However, as for RRGCTS, there has been no case series describing the prognosis or treatment options, probably owing to the rarity of the disease. We retrospectively reviewed all RRGCTS in our center and presented their clinical details, hopefully to shed new light into the treatment options and prognosis of RRGCTS.
Methods and materials
Patients
A retrospective study of 71 patients of RGCTS treated at the spine center, Changzheng Hospital, Shanghai, were performed between 2000 and September 2014 to investigate the incidence of RRGCTS. RRGCTS was diagnosed by clinical and radiological presentation of each patient, and it was confirmed by postoperative pathology. Malignant giant cell tumor was defined as highly invasive and fast growing, and, microscopically, large nuclei and giant atypical mitotic figures can be observed [8]. Of the 71 patients, 50 patients had only one time of recurrence and were thus excluded. Finally a total of 21 patients with at least two times of recurrence (repeated recurrence) were included. The data of all patients were retrieved from the medical database from our hospital. The neurological status of the patients was assessed according to Frankel score [9]. The radiological grading of RRGCTS was based upon Campanacci system [10].
The surgical strategy and pathway for each patient were decided based on the radiological information of the GCTS lesion of each patient. The pathology was verified each time from postoperative specimen.
The study focused on postoperative recurrence and death of disease during the length of follow-up, and the status of recurrence was decided by clinical findings, radiological data and pathology information obtained from the database of the hospital. On condition that the patients with recurrence did not receive surgery, the diagnosis of recurrence was made based on clinical and radiological evidence of disease progression. All patients were followed up on a 3-month basis for 6 months after the last surgery, and on a 6-month basis in the 1.5 years thereafter until yearly. The healing of surgical wound was examined and good healing means the healing process was uneventful and no extra surgical debridement was needed. The time to recurrence was defined as the time from the date of the last surgery till recurrence. Recurrence-free survival (RFS) was defined as the time between the date of surgery and the date of recurrence diagnosis.
Statistical analysis
Qualitative data are described as percentage. Quantitative data are described as mean and median (range). Univariate and multivariate analyses have been performed to identify independent prognostic factors each time a patient received treatment at our center. These factors include: (1) Frankle scores at each presentation; (2) preoperative arterial embolization; (3) mode of spondylectomy; (4) blood loss; (5) bisphosphonate treatment; (6) postoperative radiotherapy. The RFS rate was estimated by Kaplan–Meier method, and the differences were analyzed by long-rank test. Factors with P values ≤0.05 were considered statistically significant for univariate analysis and were subjected to multivariate analysis by proportional hazard analysis [10]. Factors with P values ≤0.05 were considered statistically significant for multivariate analysis. Statistical calculations were performed on SPSS software version 20.0.
Results
Baseline characteristics of the patients
The clinical details of the 21 patients have been exhibited in Table 1. There are 21 patients comprising ten males and 11 females with a mean age of 29.7 years (range 15–49). Three patients developed RRGCTS in the cervical spine, 12 in the thoracic spine, three in the lumbar spine and three in the sacrum. During their disease courses, ten patients developed increased vertebral involvement of GCT. Six patients were graded as Campanacci III when admitted for primary GCTS and the other 15 patients were graded as Campanacci II. As for neurological status, two patients were graded as Frankle score of C when admitted for primary GCTS and the other 19 patients were graded as D or E.
As for the treatment, 16 patients received bisphosphonate therapy for 2 years and 13 patients received postoperative adjuvant radiotherapy. Ten patients received both. All patients received preoperative arterial embolization for at least once during the course of disease. Fourteen patients were diagnosed to have benign GCT, and the other seven patients were diagnosed to have malignant GCT, chondroblastoma plus GCT, or other types of complicated pathology postoperatively.
At the end of follow-up, 18 patients had no evidence of disease, two patients alive with disease and one patient dead of disease. The mean time of follow-up from the last surgery date was 41 months (range 10–98). Among the 20 patients alive at the last follow-up, nine patients had neurological status categorized as Frankle E, nine patients Frankle D, one patient Franle C and one patient Frankle B. As for the healing of surgical wound, 18 patients healed well, and three patients healed poorly.
Baseline characteristics of surgery times
Thirteen patients had two times of recurrence since onset, four patients three times of recurrence, two patients four times of recurrence and another two patients five times of recurrence. Collectively, there were 56 times of recurrence for the 21 patients. 36 times of recurrence occurred within 1 year, and the rate was 64.3 %.
All patients received surgery during their disease course. Only one patient (No. 19) received en bloc spondylectomy during the last time of surgery, and surgical strategies for other patients were all piecemeal spondylectomy. Collectively there were 62 times of intralesional subtotal spondylectomy, 11 times of piecemeal total spondylectomy. 48 times of recurrence occurred within 2 years, and the rate was 85.7 %. Eleven times of surgery were performed by anterior route, and 63 times of surgery were performed by posterior route.
Univariate analysis based on surgery times
The results of univariate analysis have been shown in Table 2. The RFS rate is 24.3 %. Patients who received total spondylectomy had significantly better RFS than those receiving subtotal spondylectomy (P = 0.00, Fig. 1). Patients who received bisphosphonate therapy had significantly better RFS than those who did not (P = 0.00, Fig. 2). Other factors had no significant impact on RFS, including Frankle scores, preoperative arterial embolization, adjuvant radiotherapy, and blood loss of each time of treatment (Figs. 3, 4, 5).

Kaplan–Meier Curve of recurrence-free survival rates for resection mode

Kaplan–Meier Curve of recurrence-free survival rates for bisphosphonate therapy

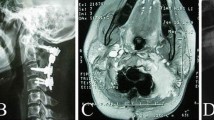
The MRI, CT, X-ray and intraoperative images of the 4th time of admission in one patient: a, b show the preoperative MRI in the sagittal plane; c, d in the coronal plane; e in the horizontal plane

a, b The preoperative X-ray images in the front and oblique position. c The preoperative CT images. d, e The postoperative X-ray images in the front and oblique position

The intraoperative images
Multivariate analysis based on surgery times
The results of multivariate analysis have been shown in Table 2. Univariate analysis indicated that the prognostic factors for RFS were mode of spondylectomy, bisphosphonate usage and adjuvant radiotherapy. The factors were subjected to multivariate analysis and Cox regression model was applied. Patients who received total spondylectomy either by en bloc or by piecemeal strategy had significantly better RFS than patients receiving subtotal spondylectomy. The hazard ratio (HR) was 0.21 [95 % confidence interval (CI) 0.07–0.59] for RFS (P = 0.00). Patients who received bisphosphonate therapy had significantly better RFS than patients who did not. The hazard ratio (HR) was 2.83 [95 % CI 1.40–5.71] for RFS (P = 0.00).
Discussion
Giant cell tumor of the spine is a potentially aggressive tumor of the spine with high rate of recurrence [3, 4]. GCTS that recurred for multiple times requires special attention, in that compromised local anatomical structures, heavy neurological deficits and great surgical obstacles may spell poor prognosis for the patients.
Our data showed that 36 times of recurrence occurred within 1 year, (64.3 %). Forty eight times of recurrence occurred within 2 years (85.7 %). This is in coherence with previous studies on recurrent GCT of the extremities [7, 8, 11], which reported a recurrence rate of 70 % within 2 years. Moreover, 19 patients presented with Frankel D or E at the initial onset, but six of them had deteriorated to Frankel score of C at later presentation of recurrence, and all of the 21 patients recurred as Campanacci III at later stage of recurrence. We hereby recommend serial check-ups for potential recurrence. Thus, early diagnosis and treatment can be achieved to save potential neurological deficits.
At the end of follow-up, 18 patients were rendered free from disease. The mean time of follow-up from the last surgery date was 41 months (range 10–98). There are a total of 74 times of surgery for the 21 patients. One patient had six times of surgery and was free from disease (case no. 12). It was reported by Vult von Steyern et al. [12] that 13 patients with a total of 15 local recurrences were successfully treated by surgery. Prosser et al. [13] performed repeated curettage for 43 patients with local recurrence, and concluded that recurrence of GCT could be surgically treated with reasonable chance of success. In our case series, though local recurrence was high within 2 years, all patients responded well to intralesional excisions, and all patients who had no evidence of disease reported few neurological deficits after treatment in hospital at the end of follow-up (Frankel score of D or E). Also, at the end of follow-up of the 21 patients, 18 patients had good healing process even if they had multiple times of surgery. The result of our data suggested that RRGCTS responded well to surgical intervention, that further treatment in hospital could restore the neurological function of the patients, and that RRGCTS patients proved suitable for further surgery with reasonably good healing process. However, seeing that the sample size of the study is relatively small, we recommend further large-scale studies to elucidate surgical treatment options for RRGTS.
As for the surgical strategies, only one patient received en bloc total spondylectomy for local recurrence, with the rest receiving intralesional excisions. En bloc resection has been reported to result in excellent prognosis because the entire osseous compartment is removed, but en bloc resection could not be applied in all GCTS patients [14–16]. However, should the condition allow, patients with GCTS would benefit from en bloc spondylectomy because it has been evidenced to be the standard procedure for GCTS and en bloc resection of GCTS could reduce recurrence for GCTS [14, 16].
In RRGCTS patients, multiple times of GCT recurrence and surgical intervention may have lead to anatomical compromise of local structure, and thus en bloc resection is even more difficult to perform on such patients. To realize the complete removal of osseous compartment, we performed piecemeal total spondylectomy. A recent study in our center performed by Xu et al. [6] suggested that total spondylectomy, either by en bloc or piecemeal method, proved to significantly reduce the recurrence rate in primary GCTS patients. In our study, of the 74 times of surgery, en bloc or piecemeal spondylectomy was performed for 12 times, and eight of them had no evidence of disease at the end of follow-up. On multivariate analysis, the recurrence-free survival was significantly better for patients receiving total spondylectomy (P = 0.00) and this procedure proved to be one independent better prognostic factor for longer RFS of RRGCTS patients. The result suggested that removal of the entire vertebrae could significantly reduce the recurrence rate of RRGCTS patients. Thus, based on our results and previous studies, we recommend that GCTS patients receive total spondylectomy should the conditions allow.
In vitro studies have exhibited that bisphosphonate could effectively kill GCT stromal and osteoclast-like cells [17] and that bisphosphonate therapy alone could control the progression of GCT [18, 19]. Tse et al. [20] did a study of adjuvant bisphosphonate therapy for GCT of the extremities and found that bisphosphonate therapy could effectively reduce postoperative recurrence rate. The previous study in our center of 102 patients with primary GCTS demonstrated that bisphosphonate could significantly reduce the recurrence rate of GCT in the mobile spine [6]. However, there have been few studies that deal with recurrent GCTS or RRGCTS. In our study, bisphosphonate therapy in combination with surgery could bring about good prognosis for GCT patients. It should also be noted that bisphosphonate therapy was sufficient therapeutic strategy even if subtotal spondylectomy was applied, and that even if no patients experienced significant adverse effects, long-term administration of bisphosphonate could be associated with severe complications [21].
Low-dose adjuvant RT has been evidenced to be effective in local control of GCTS [22–24]. In our study, adjuvant radiotherapy was prescribed for 17 times, to result in a RFS rate of 41.2 %. It was not found to be a significant factor for better RFS on multivariate analysis. One study by Chen et al. suggested that even if radiation is an option for GCTS, secondary malignancies could ensue, with post-RT malignancy rate of 33 % during follow-up visit [25]. A previous systemic review on radiotherapy demonstrated that no patient was found to have malignant transformation during follow-up [23]. In this study, pn univariate analysis, we identified that adjuvant radiotherapy was not significant enough (P = 0.07) to offer conclusive suggestion for local control. Collectively speaking, we recommend that radiotherapy could be applied to patients with GCTS that did not respond to surgical treatment.
Along with traditional therapies of GCTS comes with novel approaches. Bisphosphonate therapy may not be the only successful medication for GCT treatment. Interferon alfa-2b has been evidenced to be effective in scattered cases to treat GCT, yet adverse effects have been reported [26]. Recently, a fully human monoclonal antibody to receptor activator of nuclear factor kappa B ligand (RANKL) inhibitor, denosumab, has been used to treat GCT that cannot be surgically resected [27], which may well be a potential therapeutic modality for RRGCTS cases where surgery may not always be possible, and further investigations are needed for evaluation of the effects of novel treatment on RRGCTS.
There are some limitations for the study. First, it was a retrospective study of RRGCTS, though to our knowledge it was the largest case series that specifically studied RRGCTS. Second, the follow-up period of the last treatment for the case is relatively short, and thus follow-up for treatment of each time was recorded as an adjustment.
Conclusion
In conclusion, patients of RRGCTS are suitable for further surgical treatment with relatively good healing process and restoration of nervous function. Early diagnosis of recurrence may be associated with better prognosis. Total spondylectomy in combination with bisphosphonate therapy could reduce postoperative recurrence rate.
References
Unni KK (1996) Dahlin’s bone tumors: general aspects and data on 11,087 cases. Lippincott-Raven, New York. 5(1):234–254
Dahlin DC, Cupps RE, Johnson EW (1970) Giant cell tumor: a study of 195 cases. Cancer 25(4):1061–1070
Marcove RC, Weiss LD, Vaghaiwalla MR (1978) Cryosurgery in the treatment of giant cell tumors of bone. Cancer 41(2):957–969
O’Donnell RJ, Springfield DS, Motwani HK (1994) Recurrence of giant cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg 76(A):1827–1833
Sanjay BK, Sim FH, Unni KK, McLeod RA, Klassen RA (1993) Giant-cell tumours of the spine. J Bone Joint Surg Br 75(5):148–154
Wei Xu, Li Xiang, Huang Wending (2013) Factors affecting prognosis of patients with giant cell tumors of the mobile spine: retrospective analysis of 102 patients in a single center. Ann Surg Oncol 23(2):134–141
Takeuchi Akihiko, Tsuchiya Hiroyuki (2010) The prognostic factors of recurrent GCT: a cooperative study by the Eastern Asian Musculoskeletal Oncology Group. J Orthop Sci 24(4):431–441
Stew Fri W, Coley Badleyl (1938) Malignant giant cell tumor of bone. Am J Pathol 5(4):529–531
Frankel HL, Hancock DO, Hyslop G (1969) The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia. Spinal Cord 12(7):179–192
Song S, Hong JC, McDonnell SE et al (2012) Combined modality therapy for rectal cancer: the relative value of posttreatment versus pretreatment CEA as a prognostic marker for disease recurrence. Ann Surg Oncol 23(1):654–667
Malek F, Krueger P, Hatmi ZN, Malayeri AA, Faezipour H, O’Donnell RJ (2006) Local control of long bone giant cell tumour using curettage, burring and bone grafting without adjuvant therapy. Int Orthop 30(6):495–498
Vult von Steyern F, Bauer HC, Trovik C, Kivioja A, Bergh P, Holmberg Jorgensen P, Follerås G, Rydholm A (2006) Treatment of local recurrences of giant cell tumour in long bones after curettage and cementing. A Scandinavian Sarcoma Group study. J Bone Jt Surg Br 5(3):1–5
Prosser GH, Baloch KG, Tillman RM, Carter SR, Grimer RJ (2005) Does curettage without adjuvant therapy provide low recurrence rates in giant-cell tumors of bone? Clin Orthop Relat Res 43(5):211–218
Boriani S, Bandiera S, Casadei R (2012) Giant cell tumor of the mobile spine: a review of 49 cases. Spine 37(122):37–45 (Phila Pa 1976)
Hart RA, Boriani S, Biagini R, Currier B, Weinstein JN (1997) A system for surgical staging and management of spine tumors. A clinical outcome study of giant cell tumors of the spine. Spine 22(17):73–82 (Phila Pa 1976)
Tomita K, Kawahara N, Baba H, Tsuchiya H, Fujita T, Toribatake Y (1997) Total en bloc spondylectomy. A new surgical technique for primary malignant vertebral tumors. Spine 22(3):24–33 (Phila Pa 1976)
Cheng YY, Huang L, Lee KM, Xu JK, Zheng MH, Kumta SM (2004) Bisphosphonates induce apoptosis of stromal tumor cells in giant cell tumor of bone. Calcif Tissue Int 75(7):1–7
Balke M (2010) Bisphosphonate treatment of aggressive primary, recurrent and metastatic giant cell tumour of bone. BMC Cancer 10(4):62
Zhang W, Zhang Y, Li P (2011) Administration of sodium ibandronate in the treatment of complicated giant cell tumor of the spine. Spine 36(11):66–72 (Phila Pa 1976)
Tse LF, Wong KC, Kumta SM, Huang L, Chow TC, Griffith JF (2008) Bisphosphonates reduce local recurrence in extremity giant cell tumor of bone: a case–control study. Bone 4(2):68–73
Otto S, Sotlar K, Ehrenfeld M, Pautke C (2011) Osteonecrosis of the jaw as a possible rare side effect of annual bisphosphonate administration for osteoporosis: a case report. J Med Case Rep 5(4):77
Malone Shawn (1995) Long-term follow-up of efficacy and safety of megavoltage radiotherapy in high-risk giant cell tumors of bone. Int J Radiat Oncol Biol Phys 33(3):689–694
Ma Y, Xu W, Yin H, Huang Q, Liu T, Yang X, Wei H, Xiao J (2015) Therapeutic radiotherapy for giant cell tumor of the spine: a systemic review. Eur Spine J 24(8):1754–1760 (Epub 6 May 2015)
Nair MK, Jyothirmayi R (1999) Radiation therapy in the treatment of giant cell tumor of bone. Int J Radiat Oncol Biol Phys 4(3):1065–1069
Chen ZX, Gu DZ, Yu ZH, Qian TN, Huang YR, Hu YH, Gu XZ (1987) Radiation therapy of giant cell tumor of bone: analysis of 35 patients. Int J Radiat Oncol Biol Phys 12(3):329–334
Wei F, Liu X, Liu Z (2010) Interferon alfa-2b for recurrent and metastatic giant cell tumor of the spine: report of two cases. Spine 35(14):18–22 (Phila Pa 1976)
Thomas D, Henshaw R, Skubitz K (2010) Denosumab in patients with giant-cell tumour of bone: an open-label, phase 2 study. Lancet Oncol 11(2):75–80
Acknowledgments
This study was supported by Shanghai youth science and technology talent sailing program (Grant 14YF1405900).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors disclose no conflicts.
Additional information
Yifei Ma, Jialin Li and Jun Pan contributed equally to this study.
Rights and permissions
About this article

Cite this article
Ma, Y., Li, J., Pan, J. et al. Treatment options and prognosis for repeatedly recurrent giant cell tumor of the spine. Eur Spine J 25, 4033–4042 (2016). https://doi.org/10.1007/s00586-015-4348-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4348-5