
Abstract
Purposes
Magnetically controlled growing rods (MCGR) allow controlled distraction of the immature spine for the treatment of early onset scoliosis. This study’s primary aim was to determine the disparity between ‘true’ (TD) and ‘intended’ (ID) distraction. The secondary aim was to assess truncal growth and development during sequential lengthening.
Methods
Twenty-one patients with a maximum follow up of 37 months were included in the study. Patients in the study underwent three monthly distractions. The amount of TD was determined by measuring the expansion gap on dedicated fluoroscopic images of the actuator. The total TD to date was compared to the ID measurement reported on the external adjustment device (EAD). Weight, sitting and standing heights were recorded at each distraction.
Results
The average number of three monthly distractions was 8. The true to intended distraction ratio was calculated as 0.33. Patients who had undergone previous surgery gained less distraction with a ratio of 0.30 compared to patients undergoing MCGR as a primary procedure with a ratio of 0.35. Weight, sitting and standing heights increased in all patients by an average of 3.1 kg, 2.3 and 5.2 cm per year. The Cobb angle following surgical correction was maintained in 19 of 21 patients at the latest follow-up.
Conclusions
The TI ratio of 0.33 suggests that for every unit of distraction registered on the EAD approximately 33 % of true distraction occurs in vivo. Increases in sitting and standing heights were observed in all patients in the study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Magnetically controlled growing rods (MCGR) for the treatment of early onset scoliosis (EOS) are gaining popularity. This new device has presented spinal surgeons with a method of correcting spinal deformity, preventing progression and allowing repeated non-invasive lengthening. Traditionally growing rods have required repeated surgical procedures to manually distract the rods at six monthly intervals. This subjects a young population, often with coexisting comorbidities, to repeated invasive procedures and general anesthesia. There is a high complication rate with this method [1]. With each manual distraction the degree of lengthening achieved has been shown to reduce whilst the surgical complications and force required to achieve distraction have increased [1–3]. The new remotely expandable rods allow the operator to control the amount of distraction to each rod to the nearest 0.1 mm. The distraction rod is capable of up to 48 mm of lengthening and can generate a maximum distraction force of 270 N at which point the actuator cuts out. The current external adjustment device (EAD) available does not recognise when the rod has stopped distracting once the maximum force has been reached.
The ability to remotely control the degree of distraction to each rod theoretically allows clinicians to mirror the child’s spinal growth without the need for repeated surgical procedures. Our group has used a protocol (‘Tail-gating’ presented at 6th International Congress on Early Onset Scoliosis, Dublin 2012) for regular remote distractions based on Dimeglio’s age determined spinal growth modifiers [4–7]. The first published reports for MCGR show encouraging results for the first 2 years of follow up; however, there are limited data on formal evaluation of the ability of the implant to lengthen in human subjects as the implant is designed to remain in situ for up to 4 years before the maximum distraction has been achieved [5, 6]. The aim of this study was to radiographically evaluate the true amount of remote distraction achieved with repeated distractions up to 3 years post-implantation and correlate this with clinical growth parameters.
Methods
Scoliosis patients aged between 2 and 12 with potential spinal growth and able to regularly attend lengthenings were considered for the study. Patients with active infection and malignancy were excluded. Twenty-one consecutive patients undergoing insertion of the Magec System (Magec™ Ellipse Technologies) by two surgeons in a single centre were prospectively reviewed. Patients underwent implantation from December 2011 to May 2014. Ten were primary cases and 11 were conversion cases from traditional growing rod systems. The new system comprises two implantable titanium distraction rods and an EAD. Each distraction rod has a non-shapeable actuator section which houses the internal magnets and a shapeable rod section. The actuator section is 9 mm in diameter and 90 mm long. The shapeable rod section comes in diameter sizes of 4.5, 5.5 and 6 mm. The proximal rod end measures 256 mm and the distal rod end measures 109 mm. The rod ends are usually cut and contoured before insertion. They are attached to the spine with rods or hooks. The anchor points were fused in all of our patient group. The EAD is a handheld device which contains permanent magnets that retract or distract the implanted rods when placed against the skin over the rods.
The average age was 7.8 years (3–12 years). Average follow up was 24 months (7–37 months). Nineteen patients had dual rod constructs and two patients had a single rod. After insertion of the rods patients underwent remote distraction at three monthly intervals. The demographics, diagnoses, and levels instrumented for the patient population are shown in Table 1.
At distraction each rod was expanded by a predetermined amount as displayed on the EAD. This measurement was taken as the intended distraction. The amount of distraction was determined from Dimeglio’s age-based annual growth chart. Incremental distraction of the MAGEC rods was performed at three monthly intervals (4 distractions/year) by the senior author using the EAD. At each visit measurements for weight were taken. The amount of distraction was calculated from the Dimeglio growth charts which describe the relationship between annual growth velocity (AGV) of T1–L5 spinal segments and expected weight for chronological age of the child: (1) birth to 5 years: 20 kg with AGV of 2.2 cm/year (2) 5–10 years: 30 kg at 1.1 cm/year and (3) 10 years to puberty: >30 kg at 1.8 cm/year. These figures are then divided by four to give the incremental distance rounded to the nearest figure by which the rod is distracted at each visit. A ‘catch up’ distraction is performed at the fourth visit. For instance, a patient weighing 20 kg can expect an increment of 4 mm for three visits and then 6 mm at the fourth visit to make up the distraction applied for the year to 22 mm. Weight, standing and sitting heights were recorded preoperatively and before each distraction. On even numbered distraction visits (2nd, 4th, etc.) a full-length spine radiograph was taken to determine the Cobb angle. On odd numbered visits fluoroscopic images of the screws, rods and actuator were taken to assess the integrity of the construct.
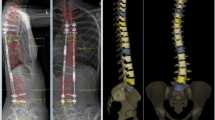
During lengthening an expansion gap within the actuator increases demonstrating that the rod has lengthened (Fig. 1). The true distraction gap (TD) can then be determined using the width of the rod as a conversion factor to allow for magnification. Fluoroscopy allows a focused true image of the distraction gap. The TD was measured from the most recent fluoroscopic image of the actuator and compared with the ID calculated by the cumulative total of lengthenings displayed on the EAD.

a Left fluoroscopic view of the actuator prior to distraction. b Right actuator post-distraction. The true distraction gap can be measured and calculated using the width of the rod (9 mm) to allow for magnification. True gap = 9/width of rod measured on fluoroscopy × distraction gap measured on fluoroscopy
Statistical analysis of the Cobb angles was made using a Student’s t test.
Results
The mean ID for each rod measured on the EAD was 28.1 mm. The mean TD achieved as measured on the fluoroscopic images was 10.1 mm. This gives a TD to ID ratio of 0.36. The difference between the ID and true TD varied from 2 to 44 mm. Conversion patients gained 30 % of predicted distraction compared with 35 % achieved in those having magnetic expansion controlled growth rods as their primary procedure. Table 2 shows the differences between ID on the EAD and TD with the percentage of distraction achieved for each patient. All patients were under distracted. The mean Cobb angle improved from 54° to 39° (p < 0.05) postoperatively which was maintained at the most recent follow up (35° p = 0.01) (Table 3). All patients showed an increase in weight and height (standing/sitting) during treatment (Table 4). The average rate of increase in standing height, sitting height and weight per year was 5.2, 2.3 cm/year and 3.1 kg/year, respectively.
Six patients experienced complications that required unplanned surgery: three for failure of fixation at an anchor point, two for rod breakage and one for skin break down over a prominent metalwork.
Discussion
MCGR works on the principle of controlled distraction to maintain spinal deformity correction in EOS. We have taken advantage of this principle in an attempt to approximate anticipated spinal growth more closely. The tail-gating technique relies on controlled distraction to effect correction of spinal deformity. The difficulty lies in ensuring harmony between the distraction seen on the EAD and that which actually occurs in vivo. The TD achieved by each rod cannot be truly determined until each rod is explanted and compared with its original length. Akbarnia et al. demonstrated from radiographs in a porcine model that 80 % of the intended distraction was achieved [8]. Our results indicate that this figure may be less. The only study to date to comment on the amount of distraction achieved was by Cheung et al. Their study looked at whole spine radiographs taken pre and post-distraction in a bid to detect measurements of less than 2 mm. However, the views may not have been orthogonal to the rod which would impact on the accuracy of measurements [5]. Our method is the first to utilise fluoroscopy to obtain orthogonal views of the actuator so that the true amount of distraction can be calculated. This method also minimises the amount of radiation exposure to a fraction of that encountered with whole spine radiographs [9].
Our study protocol aimed to distract the spine by the growth parameters set out by Dimeglio. The average amount of TD achieved was 33 % of that indicated on the EAD. Our study cohort includes a number of patients with significant comorbidities (Table 1) who would not necessarily be expected to achieve the average physiological spinal growth as set out by Dimeglio. Half of our patient group have undergone previous spinal procedures including traditional growth rods (TGR) and VEPTR. Sankar et al. have shown a ‘law of diminishing returns’ with repeated surgery as the spine becomes stiffer and the amount of lengthening reduces [3]. This is hypothesized to be a result of autofusion of the spine due to repeated surgery, forceful manual distractions or prolonged instrumentation. In our study the percentage of true lengthening to intended lengthening was greater in the patients who have not had previous instrumentation (30 vs 35 %). This disparity could be a result of stiffness induced by repeated surgery, invasive lengthenings or prolonged instrumentation. The resulting stiffness would cause the actuator to fail to achieve the intended distraction cutting out at the maximum force. Two of the conversion patients in the study were noted to have slight worsening of their Cobb angle postoperatively. This could also be due stiffness and inability to achieve further correction at the time MCGR implantation.
Of the few studies that have reported on the early results from the MCGR systems, few have formally commented on the amount of true distraction achieved with respect to the rod. Cheung et al. obtained pre- and post-distraction whole spine radiographs at one monthly intervals in two patients with 24 months follow up [5]. The three rods distracted had an ID vs TD distraction ratio of 0.60, 0.95 and 0.81. The lower values presented in our study may represent a difference in initial diagnosis and previous surgery.
All of the patients in our cohort increased in standing height and weight. The measurement of these clinical variables is of more significance and importance to the patient and their family than arbitrary radiographic parameters. This study is the first to comment on weight and height gain through the course of this treatment. A significant number of children in our study have complex needs and comorbidities which make replicating the posture and position of their whole spine radiographs extremely challenging. The ability to demonstrate on height and weight centile charts that the child is maintaining their rate of growth and in many cases increasing their centile value during the key developmental years is reassuring in evaluating their response to this novel technique. One child with VACTER syndrome in our group required repeated surgical procedures due to recurrent implant failure with VEPTR. After implantation of MCGR his rate of growth rose steeply without the need for repeated hospital admissions and invasive procedures.
This study includes a relatively small number of patients with a number of different primary pathologies and previous treatment modalities. As the length of follow increases and the number of patients in our cohort climbs we hope to gain more information about the individual success and failures experienced with this technique.
The introduction of any new implant or technique requires close follow up for complications such as anchor or implant related failure. Our group has incorporated fluoroscopy as part of the diagnostic follow up. This allows us to obtain orthogonal views of the actuator to quantify the amount of distraction achieved and to formally evaluate the implant for problems. Regular distractions every 3 months have the potential to expose a young population to high levels of ionising radiation with regular radiographs. The radiation dose from fluoroscopy is a fraction of the amount from plain radiographs. We have managed to reduce the number of whole spine radiographs performed on each patient to one every 6 months and the radiation dose by a factor of over 20 [9].
Conclusion
Our study demonstrates that the MCGR system successfully lengthens by an average of 0.5 of the intended measurement on the EAD. The amount of distraction appears to be reduced in those patients who have undergone previous instrumentation. The Tail-Gating method takes into account the expected spinal growth rates and attempts to mirror physiological growth. It does not aim to stimulate growth by maximal distraction as with TGR. The afflicted spines have inherent growth potential which is what exacerbates the deformity in the first place. Despite the disparity between ID and TD all patients in this study demonstrated height and weight gains with the maintenance of the Cobb angle correction through the course of follow up.
References
Bess S, Akbarnia BA, Thompson GH et al (2010) Complications of growing-rod treatment for early-onset scoliosis: analysis of one hundred and forty patients. J Bone Joint Surg Am 92:2533–2543. doi:10.2106/JBJS.I.01471
Noordeen HM, Shah SA, Elsebaie HB et al (2011) In vivo distraction force and length measurements of growing rods: which factors influence the ability to lengthen? Spine 36:2299–2303. doi:10.1097/BRS.0b013e31821b8e16
Sankar WN, Skaggs DL, Yazici M et al (2011) Lengthening of dual growing rods and the law of diminishing returns. Spine 36:806–809. doi:10.1097/BRS.0b013e318214d78f
Dimeglio A (2001) Growth in pediatric orthopaedics. J Pediatr Orthop 21:549–555
Cheung KM-C, Cheung JP-Y, Samartzis D et al (2012) Magnetically controlled growing rods for severe spinal curvature in young children: a prospective case series. Lancet 379:1967–1974. doi:10.1016/S0140-6736(12)60112-3
Dannawi Z, Altaf F, Harshavardhana NS et al (2013) Early results of a remotely-operated magnetic growth rod in early-onset scoliosis. Bone Joint J 95-B:75–80. doi:10.1302/0301-620X.95B1.29565
Akbarnia BA, Cheung K, Noordeen H et al (2013) Next generation of growth-sparing techniques: preliminary clinical results of a magnetically controlled growing rod in 14 patients with early-onset scoliosis. Spine 38:665–670. doi:10.1097/BRS.0b013e3182773560
Akbarnia BA, Mundis GM, Salari P et al (2012) Innovation in growing rod technique: a study of safety and efficacy of a magnetically controlled growing rod in a porcine model. Spine 37:1109–1114. doi:10.1097/BRS.0b013e318240ff67
Thakar C, Sonecha S, Rolton D (2014) The fluoroscopic technique for monitoring distraction of a non-invasive lengthening device in early onset scoliosis. Open Med 1:23–28
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Rolton, D., Thakar, C., Wilson-MacDonald, J. et al. Radiological and clinical assessment of the distraction achieved with remotely expandable growing rods in early onset scoliosis. Eur Spine J 25, 3371–3376 (2016). https://doi.org/10.1007/s00586-015-4223-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4223-4