
Abstract
Purpose
To identify elements of timely integration of palliative care (PC) into hospital oncology care from best practices. Thereafter, to assess the level of consensus among oncology and PC specialists and patient and relative representatives on the characteristics of timely integration of PC.
Methods
A three-round modified Delphi study was conducted. The expert panel consisted of 83 healthcare professionals (HCPs) from 21 Dutch hospitals (43 physicians, 40 nurses), 6 patient and 2 relative representatives. In the first round, four elements of integrated PC were considered: (1) identification of potential PC needs, (2) advance care planning (ACP), (3) routine symptom monitoring and (4) involvement of the specialist palliative care team (SPCT). In subsequent rounds, the panellists assessed which characteristics were triggers for initiating an element. A priori consensus was set at ≥ 70%.
Results
A total of 71 (78%) panellists completed the first questionnaire, 65 (71%) the second and 49 (54%) the third. Panellists agreed that all patients with incurable cancer should have their PC needs assessed (97%), symptoms monitored (91%) and ACP initiated (86%). The SPCT should be involved at the patient’s request (86%) or when patients suffer from increased symptom burden on multiple dimensions (76%). Patients with a life expectancy of less than 3 months should be offered a consultation (71%).
Conclusion
The expert panel agreed that timely integration of PC into oncology is important for all patients with incurable cancer, using early identification, ACP and routine symptom monitoring. Involvement of the SPCT is particularly needed in patients with multidimensional symptom burden and in those nearing death.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite advances in diagnostics and treatment options, cancer remains one of the leading causes of premature death [1]. It is predicted that cancer will cause 11.5 million deaths worldwide in 2030 [2]. This implies that the number of people with palliative care (PC) needs will also increase, with cancer being one of the main drivers [3].
A growing body of literature demonstrates the positive effects of timely integration of PC in the cancer trajectory, including improved quality of life, reduced depressive feelings and symptom burden, increased satisfaction with care and even improved survival rates [4,5,6,7].
This recognition of PC as an integral aspect of oncology care has prompted research into indicators of integration of PC and oncology programmes for patients with advanced cancer. In a previous study, 47 physicians specialised in both oncology and PC reached a consensus on 13 indicators of integration, including the presence of interdisciplinary PC teams, routine symptom monitoring and routine documentation of advance care plans [8]. The Lancet Oncology Commission has identified different models of integration of PC into oncology, including the use of standardised care pathways, systematic assessment, multidisciplinary teams and an interdisciplinary approach [9].
In the Netherlands, a mixed generalist-specialist PC model is used, which means that all HCPs caring for patients with a life-limiting illness are considered PC generalists and provide PC as part of usual care. They are supported by PC specialists when needed. Specialised PC in hospitals is organised in specialist palliative care consultation teams (SPCTs). A SPCT advises HCPs on individual cases and provides a variety of educational activities. Patients and families can also be referred to the team for consultation. A large nationwide study in the Netherlands has shown that improving the access to a SPCT for patients with cancer can reduce the number of patients receiving potentially inappropriate end-of-life care [10].
However, there are no official (inter)national guidelines for the timely integration of PC into hospital oncology care for patients with incurable cancer. Most hospitals focus on different elements of timely integrated care, such as developing standardised integrated pathways [11, 12], using an online symptom-monitoring and management tool [13] or researching prognostic instruments such as the Surprise Question [14], leading to a wide variation in clinical practice. Therefore, the aim of this study was to identify elements of timely integration of PC in oncological hospital care in the Netherlands and to achieve consensus among oncology and PC specialists on the essential characteristics of these identified elements, using the following research questions: (1) How do hospitals with oncology care embed different elements of timely integration of PC in their daily clinical practice? (2) What characteristics of these elements are considered essential for timely integration?
Methods
Study design
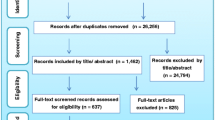
A modified three-round Delphi study was conducted to reach a consensus on the essential characteristics of the timely integration of PC in oncology. This Delphi study followed the process as used to reach a consensus on concepts in the field of PC [15] (Fig. 1). The Guidance on Conducting and Reporting Delphi Studies (CREDES) checklist was used for reporting [16].

Flowchart of the stages of the Delphi process
Panellists
The expert panel consisted of 83 HCPs (physicians and nurses), 6 patient and 2 relative representatives. HCPs were recruited on the basis of their expertise in either oncology or PC. The objective was to recruit at least two HCPs (one physician and one nurse) who were specialists in oncology but had no further specialist training in PC, and one PC specialist (either physician or nurse) per hospital. Attention was paid to include various oncologists (e.g. medical oncologists, radiation oncologists, oncological surgeons). To ensure the involvement of medical associations, six of the HCPs were representatives of the Dutch medical associations related to oncology: Dutch Association of Medical Oncologist (NVMO), Dutch Association of Radiotherapist in Oncology (NVRO), Dutch Association of Oncological Surgery (NVvH) and Dutch Nursing Society (V&VN).
The HCPs were recruited by the regional advisors of the Dutch palliative care consortia. The Netherlands is divided into seven palliative care consortia. These are networks and partnerships of different national and regional organisations that focus on improving and implementing PC. The advisors of the consortia were asked to contact three hospitals in their region (one academic and two non-academic) that they considered having good practice in the timely integration of PC. The patient and relative representatives were recruited through the Dutch Federation of Cancer Patients Organisations (NFK).
Process of development of a questionnaire
Based on key papers in this area of research, such as Kaasa et al. [9] Hui et al. [8], and the domains of PC as defined in the Netherlands Quality Framework for Palliative Care [17], four elements were identified as essential for the timely integration of PC into oncology care: (1) identification of potential PC needs, (2) advance care planning, (3) routine symptom monitoring and (4) involvement of the specialist palliative care team. Identification of palliative care needs was defined as the recognition of patients with a life-threatening illness or frailty with problematic questions and/or needs in physical, social, psychological and/or spiritual areas.
Delphi round 1
The first Delphi round was conducted between October and November 2021. The aim of this round was to identify how HCPs embed the four elements into their daily clinical practice. For each element, three characteristics were collected: (1) for whom (for which patient groups the element is initiated), (2) when (when in the disease trajectory the element is initiated), and (3) by whom (which clinician is responsible for initiating the element). Two versions of the questionnaire were drafted; one for HCPs and one for the patient and relative representatives. HCPs were asked about their own clinical practice and the general practice in their hospital. Patient and relative representatives were asked about their personal experience with (timely) PC and what, according to them, timely PC should look like in general for patients with incurable cancer. The questionnaires were pilot-tested using the think-aloud method (n = 3). The questions included an open-ended text box where panellists could add response categories that were not opted in the multiple choice categories. Panellists were able to select multiple answer categories.
Delphi round 2
The second round was conducted in January 2022. The results of the first round (Table 2) were analysed, and the three to five most selected characteristics per element were used to formulate statements. The response format was a 5-point Likert scale. HCPs and patient and relative representatives received the same questionnaire.
Delphi round 3
The third round was conducted in April 2022 and included 27 additional statements with a 5-point Likert scale as response format. Again HCPs and patient and relative representatives received the same questionnaire.
Data collection
The online questionnaire was sent by email, and panellists were asked to complete the questionnaire within 2 weeks. After 2 weeks, a friendly reminder was sent, and 2 weeks after the reminder, the questionnaire was closed. Each survey round took approximately 4 weeks to complete. To ensure anonymity, no personal information was requested other than socio-demographic characteristics including age, education level, occupation for HCPs and patient diagnosis for patient and relative representatives.
Analysis
The two questionnaires of the first round were merged in Stata (version 17). Stata was used for the analysis and for the recoding of answers submitted in the open-ended text box. When analysing the open field text, we first checked how often the field was filled in. As a guideline, we decided to include a response in the next round when the response was given more often than the least selected pre-defined answer category. However, this was never the case. This suggests that the multiple-choice categories were comprehensive enough. Response categories were listed and ordered using frequency tables. Descriptive statistics were used to summarise the data.
Definition of consensus
Consensus was defined as an agreement of ≥ 70% a priori.
Ethical considerations
This study was assessed by the Medical Ethics Committee of Brabant (METC NW2021-71) and exempt from full approval of an ethics committee due to the fact that there was no invasive intervention nor were there vulnerable patients involved (CCMO, 2020). Informed consent was obtained from all panellists. At the start of each questionnaire, panellists had to give permission for the data to be used for research by checking a box. They were only able to access the questionnaire after checking the box.
Results
In total, the expert panel consisted of 91 panellists of whom 83 (91%) were HCPs, who were oncology specialists either with or without additional PC training, 6 (7%) were patient representatives and 2 (2%) were relative representatives (Table 1). Of the HCPs involved, 47 (52%) were physicians and 36 (40%) were nurses. The first round was completed by 71 panellists (78%), the second round by 65 (71%) and the third by 49 panellists (54%). The expert panel agreed on 34 out of 55 characteristics of timely integration of PC in oncology.
Characteristics of current best practices of timely integration of palliative care in oncology
More than half of the HCPs in the expert panel reported that they pay special attention to identifying potential PC needs in all patients with incurable cancer (66%) or only in patients with incurable cancer who also have a poor performance status (66%) (Table 2). The majority of HCPs reported that they pay particular attention to identifying potential PC needs when patients have an increased symptom burden (65%), shortly after being diagnosed with incurable cancer (61%) and/or when patients have a limited life expectancy (less than 3 or less than 12 months) (59–56%). Advance care planning was initiated within the hospital by the SPCT (58%) or by the treating medical specialists (54%). A trigger for the involvement of the SPCT in the care of patients was when patients with identified PC needs requested the involvement of the SPCT (58%).
Consensus on characteristics of identifying potential palliative care needs
Nearly all panellists agreed that the PC needs should be assessed for the following patient groups: all patients with incurable cancer (97%), patients with incurable cancer and a poor performance status (97%) and/or patients with incurable cancer and comorbidities (92%) (Table 3). All panellists agreed that the potential PC needs should be assessed at least at the following moments in the disease trajectory: when there is a limited life expectancy of less than 3 months or less than 12 months (100–91%), shortly after the diagnosis of incurable cancer (90%) and/or when patients have a high symptom burden (88%).
Consensus on characteristics of advance care planning
The panellists reached a consensus that advance care planning should be initiated for the following patient groups: all patients with identified PC needs (86%) and more specifically for patients with identified PC needs and metastatic disease (77%). Advance care planning should be initiated at least at the following moments in the disease trajectory: when patients with identified PC needs have a life expectancy of less than 12 months (90%), when patients have high symptom burden (79%) and/or when there is a change in the treatment trajectory (70%). The responsibility for initiating advance care planning lies with the treating physician (92%) and nurse practitioner or specialised nurse (80%).
Consensus on routine symptom monitoring
The panellists agreed that it is necessary to routinely monitor symptoms for all patients with incurable cancer and identified PC needs (91%). Additionally, patients with a tumour with an expected life expectancy of less than 12 months (95%), patients with a poor performance status (89%) or patients with identified PC needs and metastatic disease (88%) should also have their symptoms routinely monitored. Triggers for the start of routine symptom monitoring included a high symptom burden (98%), an unexpected hospital admission (98%), a (possible) change in therapy (94%) and a diagnosis of incurable cancer (82%). Symptoms should be routinely monitored by a nurse practitioner or specialised nurse (94%), a nurse (81%) or a physician (47%).
Consensus on characteristics of introducing a Specialist Palliative Care Team
Panellists agreed that patients should be informed about the SPCT in two situations. Firstly, when they experience an increased symptom burden on multiple dimensions (physical, psychological, social or spiritual) (80%). Secondly, when they have a life expectancy of less than 3 months (73%). According to most panellists, this limited life expectancy of less than 3 months was also a trigger for offering patients a consultation with the SPCT (71%). This consultation should be offered by the treating physician (92%) or a nurse practitioner or specialised nurse (86%). Additionally, the SPCT should be involved when patients with identified palliative care needs request their involvement (86%) and/or when patients experience increased symptom burden on multiple dimensions (physical, psychological, social or spiritual) (76%).
Discussion
This Delphi study has identified essential characteristics of four main elements of timely integration of PC into oncology hospital care: identification of potential PC needs, ACP, routine symptom monitoring and the involvement of the SPCT.
Identification of potential palliative care needs
Studies have shown that timely PC has benefits, such as improved quality of life [5, 7]. Although several screening tools are available to help assess potential PC needs, including the Surprise Question (SQ) and the Supportive and PC Indicators Tool (SPICT) [18], structural assessment of PC needs is often not part of daily clinical practice in the Netherlands [19]. The expert panel agreed that the PC needs should indeed be assessed for all patients with incurable cancer, immediately after diagnosis. It is important to note that the PC needs of patients with incurable cancer change over time [20]. Therefore, identifying potential PC needs should be seen as an ongoing process that starts at diagnosis and continues throughout the disease trajectory [9]. In the last 6 months of life, patients often experience a steady increase in physical symptoms such as fatigue, pain and dyspnoea as well as psychological distress [21, 22]. However, identifying PC needs in a timely manner can be challenging due to overly comprehensive tools with many items, administrative burden and time limitations. Developing accurate and practical screening tools is essential for daily clinical care. One such tool is the double surprise question [23].
Advance care planning
There is growing evidence of the beneficial effects of ACP, including less life-sustaining treatment and hospitalisation at the end of life, increased use of hospice and PC, better compliance with patients’ end-of-life wishes and improved concordance between preferences for care and care provided [24, 25]. International recommendations state that ACP should be initiated early in the disease trajectory of patients with a life-threatening disease [26]. This is consistent with the finding that the expert panel fully agreed that ACP should be initiated in all patients with PC needs. According to the panellists, other potential triggers for initiating ACP included a life expectancy of less than 12 months (e.g. identified by using the SQ) and a high symptom burden. However, implementation of ACP in daily oncology practice is challenging, and unfortunately, the uptake is still limited [27]. There are known barriers to the implementation of ACP at the organisational and the individual psychological levels. Barriers at the organisational level include insufficient integration into the workflow, lack of involvement of HCPs in the ACP process and its outcomes [28], lack of a structured place for ACP in the electronic patient record, lack of proper handover of ACP plans between involved HCPs in primary and secondary care [29] and lack of time [30]. Barriers on the individual psychological level are the fear that ACP discussions will lead to depression or loss of hope [31]. Ineffective patient-physician communication [32] may result in infrequent and untimely ACP discussions.
Routine symptom monitoring
The integration of routine symptom monitoring into daily clinical practice is still suboptimal, leading to underestimation of symptoms [33]. Nevertheless, the panellists almost all agreed that symptoms should be monitored for all patients with incurable cancer and identified PC needs (Table 3). This is likely to be influenced by an increasing number of studies showing the negative association between symptom burden and quality of life [34, 35]. Furthermore, the integration of patient-reported outcomes into routine symptom monitoring in oncology care is associated with increased survival rates for patients with metastatic disease [36]. However, there are still barriers to overcome regarding the tool with which symptoms could be monitored. A tool should not be burdensome for patients, families and HCPs [37]; it should take all four dimensions into account (physical, social, psychological and spiritual) [38] and should be accessible to patients from different backgrounds and with different levels of language proficiency and health literacy. In the case of a digital tool, the well-known barriers are the costs of a system, storage and data security [39].
Specialist palliative care (consultation) team
According to our expert panel, a short life expectancy (less than 3 months) seems to be the trigger to inform all patients with identified PC needs about the SPCT team or to offer them a consultation. It is important to realise that this is set as a minimum use of specialist palliative care; more is possible if needed. This minimal use of SPCT in the Dutch setting is important to ensure equal access to SPCT for all patients with incurable cancer. From previous studies in the Netherlands, we know that SPCTs are still involved (too) late and to a limited extent [19]. The results of this study could be a first step in the right direction, which means a minimum use and therefore access for all cancer patients with a limited life expectancy. Despite it being rather late, this trigger of a short life expectancy is in line with current practice, which shows that most referrals concern patients in the last weeks before their death [19]. This late referral may be related to the disease trajectory of incurable cancer patients, with a rather steep decline in (health-related) quality of life in the last 3 months [40].
The panellists also indicated that the SPCT should be consulted when patients with cancer have an increased symptom burden on multiple dimensions, indicating complexity. This is in line with the mixed generalist-specialist model of PC in the Netherlands. However, defining the complexity in patients with incurable cancer is challenging. A recent systematic review identified different classification systems for the complexity of patient needs in PC and concluded that more research is needed to integrate these classification systems into clinical cancer care [41].
Overall, there appears to be some reluctance to define triggers for standard involvement of the SPCT, as the expert panel only reached consensus on two statements: the SPCT should be involved when patients request their involvement, and when patients with identified PC needs have an increased symptom burden on multiple dimensions. The expert panel did not consider disease progression without other treatment options, an imminent death or an increased symptom burden of two or more symptoms to be reasons for standard involvement of the SPCT in patients with identified PC needs. The diagnosis of incurable cancer, a life expectancy of less than 12 months and increased symptom burden (of two or more symptoms) were also not found to be moments when patients should be informed about or offered a consultation with the SPCT. A possible explanation could be that in the generalist-specialist model, the PC generalist should be well equipped to provide PC to patients whose disease trajectory is without major complications. For more complex palliative care needs, general practitioners can consult palliative care specialists. Therefore, our results may not be consistent with other international publications as our results are tailored to current clinical practice in the Netherlands. Furthermore, the majority of European and American medical oncologists consider end-of-life care to be an integral part of their work [42]. However, this means that PC generalists must have a sound knowledge of PC and communicative skills [43]. In addition to communication skills, there are still some other barriers that need to be overcome for PC generalists to effectively integrate PC into their clinical work, such as lack of time and lack of formal training [44].
Strengths and limitations
This modified Delphi study used a multidisciplinary expert panel, including the patients’ perspective, to identify elements and essential characteristics of the timely integration of PC into oncological care. The study had a high response rate. Some limitations need to be considered. The convenience sampling method used to recruit panellists may have introduced some selection bias. The regional PC consortia were asked to contact the hospitals through their contact person. This person was often a member of the SPCT. This person then contacted the PC generalists, which is likely to result in panellists who are aware of PC in general and of the SPCT and its role. The response rate was good, but it declined towards the third round which may have slightly biased the results. In addition, the questionnaires used were designed and pilot-tested by the researchers, but not validated. Finally, there is no official guideline or definition of consensus. Therefore, this study uses the definition of consensus based on other studies within PC research [8, 45].
Conclusion
Panellists agreed that for all patients with incurable cancer, potential PC needs should be assessed soon after patients are diagnosed with incurable cancer. Panellists also agreed that once patients’ PC needs have been identified, ACP and routine symptom monitoring should be initiated. SPCTs should be involved when patients have a high symptom burden on multiple dimensions or when patients have a short life expectancy of less than 3 months. In terms of future research, a deeper understanding of how to structurally integrate the assessment of potential PC needs, ACP and symptom management into oncology care is needed. It also calls for more educational resources on PC for all HCPs to enable them to provide generalist PC for patients with incurable cancer.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin 71:209–249
Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 3:e442
Etkind SN, Bone AE, Gomes B, Lovell N, Evans CJ, Higginson IJ, Murtagh FEM (2017) How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med 15:102
Vanbutsele G, Pardon K, Van Belle S, Surmont V, De Laat M, Colman R, Eecloo K, Cocquyt V, Geboes K, Deliens L (2018) Effect of early and systematic integration of palliative care in patients with advanced cancer: a randomised controlled trial. Lancet Oncol 19:394–404
Zimmermann C, Swami N, Krzyzanowska M, Hannon B, Leighl N, Oza A, Moore M, Rydall A, Rodin G, Tannock I, Donner A, Lo C (2014) Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. The Lancet 383:1721–1730
Bakitas MA, Tosteson TD, Li Z, Lyons KD, Hull JG, Li Z, Dionne-Odom JN, Frost J, Dragnev KH, Hegel MT, Azuero A, Ahles TA (2015) Early versus delayed initiation of concurrent palliative oncology care: patient outcomes in the ENABLE III randomized controlled trial. J Clin Oncol 33:1438–1445
Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, Dahlin CM, Blinderman CD, Jacobsen J, Pirl WF (2010) Early palliative care for patients with metastatic non–small-cell lung cancer. New Engl J Med 363:733–742
Hui D, Bansal S, Strasser F, Morita T, Caraceni A, Davis M, Cherny N, Kaasa S, Currow D, Abernethy A (2015) Indicators of integration of oncology and palliative care programs: an international consensus. Ann Oncol 26:1953–1959
Kaasa S, Loge JH, Aapro M, Albreht T, Anderson R, Bruera E, Brunelli C, Caraceni A, Cervantes A, Currow DC (2018) Integration of oncology and palliative care: a Lancet Oncology Commission. Lancet Oncol 19:e588–e653
Boddaert MS, Pereira C, Adema J, Vissers KC, van der Linden YM, Raijmakers NJ, Fransen HP (2022) Inappropriate end-of-life cancer care in a generalist and specialist palliative care model: a nationwide retrospective population-based observational study. BMJ supportive & palliative care 12(e1):e137–e145
van der Padt-Pruijsten A, Leys MBL, Oomen-de Hoop E, van der Heide A, van der Rijt CCD (2021) Effects of implementation of a standardized palliative care pathway for patients with advanced cancer in a hospital: a prospective pre- and postintervention study. J Pain Symptom Manage 62:451–459
Groenewoud AS, Wichmann AB, Dijkstra L, Knapen E, Warmerdam F, De Weerdt-Spaetgens C, Dominicus W, Akkermans R, Meijers J (2021) Effects of an integrated palliative care pathway: more proactive GPs, well timed, and less acute care: a clustered, partially controlled before-after study. J Am Med Dir Assoc 22:297–304
Schuit AS, Holtmaat K, Lissenberg-Witte BI, Eerenstein SEJ, Zijlstra JM, Eeltink C, Becker-Commissaris A, van Zuylen L, van Linde ME, der Houven Menke-van, van Oordt CW, Sommeijer DW, Verbeek N, Bosscha K, Tewarie RN, Sedee R-J, de Bree R, de Graeff A, de Vos F, Cuijpers P, Verdonck-de Leeuw IM (2022) Efficacy of the eHealth application Oncokompas, facilitating incurably ill cancer patients to self-manage their palliative care needs: a randomized controlled trial. Lancet Reg Health - Europe 18
Stoppelenburg A, Arslan M, Owusuaa C, Gunnink N, van der Linden YM, Luelmo SA, van der Heide A (2022) The prognostic value of the 12-, 6-, 3-and 1-month ‘Surprise Question’in cancer patients: A prospective cohort study in three hospitals. Eur J Cancer Care 31(6):e13551
Junger S, Payne S, Brearley S, Ploenes V, Radbruch L (2012) Consensus building in palliative care: a Europe-wide delphi study on common understandings and conceptual differences. J Pain Symptom Manage 44:192–205
Junger S, Payne SA, Brine J, Radbruch L, Brearley SG (2017) Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med 31:684–706
Boddaert M, Douma J, Dijxhoorn F, Bijkerk M (2017) Netherlands quality framework for palliative care. IKNL/Palliactief
Walsh RI, Mitchell G, Francis L, van Driel ML (2015) What diagnostic tools exist for the early identification of palliative care patients in general practice? A systematic review. J Palliat Care 31:118–123
Boddaert MS, Stoppelenburg A, Hasselaar J, van der Linden YM, Vissers KCP, Raijmakers NJH, Brom L (2021) Specialist palliative care teams and characteristics related to referral rate: a national cross-sectional survey among hospitals in the Netherlands. BMC Palliat Care 20:175
Vogt J, Beyer F, Sistermanns J, Kuon J, Kahl C, Alt-Epping B, Stevens S, Ahlborn M, George C, Heider A, Tienken M, Loquai C, Stahlhut K, Ruellan A, Kubin T, Dietz A, Oechsle K, Mehnert-Theuerkauf A, van Oorschot B, Thomas M, Ortmann O, Engel C, Lordick F, ArbeitsgemeinschaftPalliativmedizin of the German Cancer S (2021) Symptom burden and palliative care needs of patients with incurable cancer at diagnosis and during the disease course. Oncologist 26:e1058–e1065
Verkissen MN, Hjermstad MJ, Van Belle S, Kaasa S, Deliens L, Pardon K (2019) Quality of life and symptom intensity over time in people with cancer receiving palliative care: results from the international European Palliative Care Cancer Symptom study. PLoS ONE 14:e0222988
Beernaert K, Pardon K, Van den Block L, Devroey D, De Laat M, Geboes K, Surmont V, Deliens L, Cohen J (2016) Palliative care needs at different phases in the illness trajectory: a survey study in patients with cancer. Eur J Cancer Care (Engl) 25:534–543
Veldhoven CMM, Nutma N, De Graaf W, Schers H, Verhagen C, Vissers KCP, Engels Y (2019) Screening with the double surprise question to predict deterioration and death: an explorative study. BMC Palliat Care 18:118
Houben CHM, Spruit MA, Groenen MTJ, Wouters EFM, Janssen DJA (2014) Efficacy of advance care planning: a systematic review and meta-analysis. J Am Med Dir Assoc 15:477–489
Brinkman-Stoppelenburg A, Rietjens JA, Van der Heide A (2014) The effects of advance care planning on end-of-life care: a systematic review. Palliat Med 28:1000–1025
Schrijvers D, Cherny NI, Group EGW (2014) ESMO clinical practice guidelines on palliative care: advanced care planning. Ann Oncol 25(Suppl 3):iii138-142
Bestvina CM, Polite BN (2017) Implementation of advance care planning in oncology: a review of the literature. J Oncol Pract 13:657–662
Seifart C, Koch M, Leppin N, Nagelschmidt K, Knorrenschild JR, Timmesfeld N, Rief W, von Blanckenburg P (2020) Collaborative advance care planning in advanced cancer patients: col-ACP -study - study protocol of a randomised controlled trial. BMC Palliat Care 19:134
Ermers DJ, van Bussel KJ, Perry M, Engels Y, Schers HJ (2019) Advance care planning for patients with cancer in the palliative phase in Dutch general practices. Fam Pract 36:587–593
Chandar M, Brockstein B, Zunamon A, Silverman I, Dlouhy S, Ashlevitz K, Tabachow C, Lapin B, Ewigman B, Mazzone T, Obel J (2017) Perspectives of health-care providers toward advance care planning in patients with advanced cancer and congestive heart failure. Am J Hosp Palliat Care 34:423–429
Mack JW, Smith TJ (2012) Reasons why physicians do not have discussions about poor prognosis, why it matters, and what can be improved. J Clin Oncol 30:2715–2717
Agarwal R, Epstein AS (2018) Advance care planning and end-of-life decision making for patients with cancer. Semin Oncol Nurs 34:316–326
de Graaf E, Zweers D, de Graeff A, Stellato RK, Teunissen S (2018) Symptom intensity of hospice patients: a longitudinal analysis of concordance between patients’ and nurses’ outcomes. J Pain Symptom Manage 55:272–281
Hamer J, McDonald R, Zhang L, Verma S, Leahey A, Ecclestone C, Bedard G, Pulenzas N, Bhatia A, Chow R, DeAngelis C, Ellis J, Rakovitch E, Lee J, Chow E (2017) Quality of life (QOL) and symptom burden (SB) in patients with breast cancer. Supp Care Cancer 25:409–419
Deshields TL, Potter P, Olsen S, Liu J (2014) The persistence of symptom burden: symptom experience and quality of life of cancer patients across one year. Support Care Cancer 22:1089–1096
Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, Rogak L, Bennett AV, Dueck AC, Atkinson TM, Chou JF, Dulko D, Sit L, Barz A, Novotny P, Fruscione M, Sloan JA, Schrag D (2016) Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol 34:557–565
Antunes B, Harding R, Higginson IJ, Euroimpact (2014) Implementing patient-reported outcome measures in palliative care clinical practice: a systematic review of facilitators and barriers. Palliat Med 28:158–175
de Vries S, Lormans T, de Graaf E, Leget C, Teunissen S (2021) the content validity of the items related to the social and spiritual dimensions of the Utrecht symptom diary-4 dimensional from a patient’s perspective: a qualitative study. J Pain Symptom Manage 61:287-294.e282
Hui D, Bruera E (2017) The Edmonton Symptom Assessment System 25 years later: past, present, and future developments. J Pain Symptom Manage 53:630–643
Raijmakers NJH, Zijlstra M, van Roij J, Husson O, Oerlemans S, van de Poll-Franse LV (2018) Health-related quality of life among cancer patients in their last year of life: results from the PROFILES registry. Support Care Cancer 26:3397–3404
Grant M, de Graaf E, Teunissen S (2021) A systematic review of classifications systems to determine complexity of patient care needs in palliative care. Palliat Med 35:636–650
Cherny NI, Catane R, European Society of Medical Oncology Taskforce on P, Supportive C (2003) Attitudes of medical oncologists toward palliative care for patients with advanced and incurable cancer: report on a survery by the European Society of Medical Oncology Taskforce on Palliative and Supportive Care. Cancer 98:2502–2510
Quill TE, Abernethy AP (2013) Generalist plus specialist palliative care—creating a more sustainable model. New Engl J Med 368:1173–1175
Hui D, Bruera E (2015) Models of integration of oncology and palliative care Ann. Palliat Med 4:89–98
Hui D, Mori M, Meng Y-C, Watanabe SM, Caraceni A, Strasser F, Saarto T, Cherny N, Glare P, Kaasa S (2018) Automatic referral to standardize palliative care access: an international Delphi survey. Support Care Cancer 26:175–180
Funding
This work was supported by the Maarten van der Weijden Foundation.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. CH, NR and LB conducted the data collection and analysis. YL, DR and AR contributed to the interpretation. CH drafted the manuscript. All authors were involved in the critical revision of the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was carried out in line with the principles of the Declaration of Helsinki. The Medical Ethics Committee of Brabant (METC NW2021-71) assessed the study and granted it exemption from full approval of an ethics committee due to the fact that there was no invasive intervention nor were there vulnerable patients involved (CCMO, 2020).
Consent to participate
Informed consent was obtained from all panellists included in the study.
Consent for publication
N/a.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Heipon, C.S., Brom, L., van der Linden, Y.M. et al. Characteristics of timely integration of palliative care into oncology hospital care for patients with incurable cancer: results of a Delphi Study. Support Care Cancer 32, 324 (2024). https://doi.org/10.1007/s00520-024-08508-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-024-08508-0