
Abstract
Purpose
To assess the association of gastrointestinal problems, received nutritional care, and nutritional care needs with quality of life (QoL) in patients with advanced cancer.
Methods
A cross-sectional analysis within the observational prospective eQuiPe cohort study on experienced quality of care and QoL in patients with advanced cancer was performed. QoL and gastrointestinal problems were measured using the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ)-C30. Received nutritional care (yes/no) and nutritional care needs (yes/a little bit/no) were measured by two questions. Gastrointestinal problems were categorized as clinically important based on the Giesinger thresholds. Univariable and multivariable linear regression analyses adjusted for age, gender, and treatment were used to analyze the association of gastrointestinal problems, received nutritional care, and nutritional care needs with QoL.
Results
Half of the 1080 patients with advanced cancer had clinically important gastrointestinal problems, 17% experienced nutritional care needs, and 14% received nutritional care. Multivariable analyses revealed that the presence of clinically important gastrointestinal problems (β (95% CI): −13.0 (−15.6; −10.4)), received nutritional care (β (95% CI): −5.1 (−8.5; −1.7)), and nutritional care needs (β (95% CI): −8.7 (−11.9; −5.5)) were associated with a low QoL.
Conclusion
Many patients with advanced cancer experience gastrointestinal problems, while only few patients receive nutritional care. These gastrointestinal problems, nutritional care needs, and nutritional care are associated with lower QoL, probably due to reversed causality or the irreversible nature of these problems in the palliative phase. More research on the relation of nutritional care, gastrointestinal problems, and QoL is needed to optimize nutritional support in end-of-life care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 2020, over 19 million new cases of cancer were diagnosed worldwide [1]. Cancer is still a leading cause of death, accounting for approximately 10 million deaths per year [1]. In the Netherlands, the estimated number of new cancer diagnoses is 115,000 per year [2] and 21,000 persons with a solid cancer diagnosis already have distant metastases at diagnosis. In addition, there are over 38,000 patients annually who develop distant metastases and require palliative care [3]. Studies have shown that early palliative care improves quality of life (QoL) in patients with advanced cancer [4]. In the course of progression of disease, this care gradually moves from a disease-oriented perspective to a more symptom-oriented treatment only [5].
Patients with advanced cancer often suffer from disease- and treatment-related gastrointestinal problems. The most common gastrointestinal symptoms are appetite loss (53%), dry mouth (40%), constipation (34%), and nausea (31%) [6]. Literature shows that these gastrointestinal problems are all associated with lower QoL [7, 8]. From the gastrointestinal problems, appetite loss was most predictive of overall QoL [7].
Due to the high prevalence of gastrointestinal symptoms and weight loss in patients with advanced cancer, nutritional care needs might be high. In line with this, Amano et al. showed that 76% of terminally ill patients had general unmet needs for nutrition therapy for cancer cachexia, and 61% indicated that they needed specific support by health care professionals such as attention and explanation concerning their distress about eating [9].
The role of dieticians in palliative oncology care is important. Dieticians can have a positive impact through nutritional evaluation, counseling, psychosocial support, follow-up, and nutritional interventions [10]. When the focus of palliative care is still on disease-modifying treatment, dieticians contribute to the identification of malnutrition, the treatment of weight loss, and diminishing gastrointestinal problems, which may improve QoL [11]. However, when palliative care shifts from disease-modifying treatment towards the alleviation of symptom burden only, also the role of nutritional care will change in enhancing patient comfort and quality of life.
Few studies have investigated the association between nutritional care needs and nutritional care with QoL in patients with advanced cancer. However, a narrative review described that nutritional care should be integrated into the care for patients with advanced cancer because limited access to nutritional care is a major source of distress for patients and family members [11]. Moreover, some studies have shown the potential benefits of nutritional care, including preventing bedsores, improving performance status in advanced cancer patients [12, 13], but no study has specifically looked at its relation with QoL. Therefore, the aim of this study was to investigate the association of gastrointestinal problems, received nutritional care, and nutritional care needs with QoL in patients with advanced cancer.
Methods
Study design
A secondary analysis was conducted, using the baseline data of the observational prospective eQuiPe cohort study on the experienced quality of care and QoL in patients with advanced cancer and their relatives [14]. Patients were identified and recruited in the departments of medical oncology, pulmonology, or urology of more than 40 hospitals in the Netherlands. Participants in this analysis were recruited between November 2017 and January 2020, and completed questionnaires using the system of the Patient Reported Outcomes Following Initial treatment and Long-term Evaluation of Survivorship (PROFILES) registry. PROFILES is a registry, linked to the Netherlands Cancer Registry (NCR), to collect data of cancer patients and noncancer controls to estimate the impact of cancer, beyond normal aging and the presence of comorbidities. PROFILES enables the investigation of the physical and psychosocial impact of cancer and its treatment in large groups of patients with cancer and is acknowledged as a unique infrastructure for survivorship research [15]. The eQuiPe study was exempted from full medical ethical review according to the Dutch Medical Research Involving Human Subjects Act (WMO), declared by the Medical Research Ethics Committee of the Antoni van Leeuwenhoek hospital (METC17.1491). Informed consent was obtained from all participants.
Participants
All adult patients with advanced cancer were eligible. Advanced cancer was defined as the presence of a solid metastasized tumor, including both synchronous (at diagnose) and metachronous distant metastases without possibilities for cure [14]. Additional criteria for patients with breast cancer were the presence of metastases in multiple organ systems. For patients with metastasized prostate cancer, the tumor had to be castrate-resistant. Patients also had to be able to complete Dutch questionnaires.
Measures
Quality of life
Quality of life (QoL) was assessed using the validated European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 items (EORTC-QLQ-C30) questionnaire [16]. The subscale global QoL was used, consisting of the two following items: “How would you rate your overall health during the past week?” and “How would you rate your overall quality of life during the past week?” with answer options ranging from 1 (very poor) to 7 (excellent). The presence of gastrointestinal problems was derived from the following items and scales of the EORTC-QLQ-C30: appetite loss, constipation, diarrhea, and nausea/vomiting. The mean scores of the subscales of nausea and vomiting and global QoL and the item scores were linearly transformed to a 0–100 scale, with a higher score implying a higher level of symptoms or a higher global quality of life, respectively.
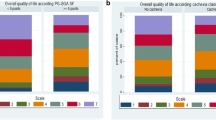
Based on the thresholds for clinical importance of Giesinger et al. [17] for each symptom (score above 8 for nausea/vomiting, above 17 for diarrhea, and above 50 for appetite loss and constipation), patients were categorized into three categories: “No gastrointestinal problems present” (all scores were 0), “Non-clinically important gastrointestinal problems present” (no score higher than the thresholds, but at least one symptom was present), and “Clinically important gastrointestinal problems present” (at least one score higher than the thresholds).
Nutritional care and care needs
Nutritional care by a dietician was assessed with the question “Have you consulted a dietician in the last month?” and the answer options were yes or no. A single item on need for information regarding nutritional care was added to the validated Problems and Needs in Palliative Care short version questionnaire (PNPC-sv) [18]. Patients were asked whether this was a problem, using “yes,” “a little bit,” and “no.” The responses “yes” and “a little bit” were combined. This additional question was tested using the “think-aloud” method and yielded good results in terms of comprehensiveness and appropriateness [14].
Sociodemographic and clinical characteristics
Age, sex, relationship status (having a partner or not), and education were self-reported. Education was categorized into low (no education or primary school), intermediate (lower general secondary education, vocational training or equivalent), and high (pre-university education, high vocational training, university). Tumor type was extracted from the NCR. Moreover, patients were also asked to self-report whether they had received treatment in the last month. The response options included radiotherapy, chemotherapy, surgery, targeted therapy, immunotherapy, or a combination of these treatments.
Statistical methods
Descriptive statistics and univariable linear regression analyses were conducted with gastrointestinal problems, received nutritional care, and nutritional care needs as separate independent variables, and QoL as dependent variable. Dummy variables were used for the categorical variable regarding gastrointestinal problems with the category “No gastrointestinal problems” being the reference category. Next, a multivariable linear regression model was fitted combining the previously mentioned variables and adjusting for age, sex, and treatment, which were selected a priori as confounders. All statistical analyses were performed using STATA version 16 (StataCorp, College Station, TX 77845, USA). p values <0.05 were considered statistically significant.
Results
In total, 1695 eligible patients with advanced cancer were invited to participate by phone, 1440 (85%) were enrolled in the study, and 1103 (65%) patients completed the baseline questionnaire. Due to missing data on the global QoL scale, 23 patients had to be excluded, leaving 1080 patients for further analysis (Fig. 1). The mean age of participants was 65 years (SD 9.8), 51% was male, and 74% had received anti-tumor treatment during the past month (Table 1).

Flow diagram of study inclusion
Gastrointestinal problems, nutritional care, and nutritional care needs
Half of all patients had at least one clinically important gastrointestinal problem (nausea/vomiting, loss of appetite, constipation, or diarrhea) whereas 16% reported ≥1 non-clinically important gastrointestinal problems, and 34% reported no gastrointestinal problems. The mean scores were 9.4 (SD 18) for nausea/vomiting, 19 (SD 27) for appetite loss, 13 (SD 23) for constipation, and 12 (SD 23) for diarrhea.
Fourteen percent of all patients had received nutritional care by a dietician during the past month. Patients with clinically important gastrointestinal problems more often received nutritional care compared to patients with no clinically important problems or with no gastrointestinal problems at all, respectively 19%, 14%, and 8% (p < 0.05) (Table 1). Of all patients, 176 patients (17%) had nutritional care needs. The nutritional care needs were similar in patients receiving nutritional care compared to patients receiving no nutritional care. Patients with clinically important gastrointestinal problems more often had (some) nutritional care needs compared to patients with no clinically important problems or with no gastrointestinal problems at all, respectively 21%, 16%, and 12% (p < 0.05) (Table 1).
Association between gastrointestinal problems, nutritional care, and nutritional care needs with QoL
Quality of life was lower in patients with clinically important gastrointestinal problems compared to non-clinically relevant or no gastrointestinal problems, respectively 61.9 (SD 20), 69.4 (SD 19.1), and 76 (SD 17.2). Of the four questions on gastrointestinal problems of the EORTC-QLQ-C30, appetite loss had the highest association with lower QoL (Table 2). Nutritional care needs and receiving nutritional care were also associated with lower QoL. Age, sex, and treatment adjusted multivariable linear regression analysis showed that having clinically important gastrointestinal problems (β = −12.9 (95% CI (−15.5 to −10.3))), receiving nutritional care (β = −5.1 (95% CI (−8.5 to −1.7))), and having nutritional care needs (β = −8.7 (95% CI (−11.9 to −5.5))) were independently associated with a lower QoL. This also holds for non-clinically important gastrointestinal problems, although the association was less strong (Table 2). No collinearity was present in the model (VIF for all variables was <10).
Discussion
This study showed that almost 50% of patients with advanced cancer had clinically important gastrointestinal problems, while only 14% received nutritional care. Having clinically important or non-clinically important gastrointestinal problems, nutritional care needs, and received nutritional care were independently associated with a lower QoL. This might be explained by reverse causality, as patients with more and more severe gastrointestinal symptoms (and associated lower QoL) are more often referred to a dietitian. This reverse causation is also present with the other healthcare professionals, in other words patients receiving care of other healthcare professionals have a lower QoL than patients who did not receive care.
To the best of our knowledge, there are no studies investigating the combined associations of gastrointestinal problems, received nutritional care, and nutritional care needs with QoL in patients with advanced cancer. Only studies investigating the univariable association between gastrointestinal problems or nutritional care needs and QoL were found [7, 8, 19]. Studies investigating the association between gastrointestinal problems and QoL in advanced cancer showed that appetite loss, nausea, vomiting, and constipation were significantly associated with a lower QoL [7, 8, 19]. Compared to our results, the severity of these gastrointestinal problems (mean scores ranging from 7 to 14 for nausea and vomiting, 23–43 for appetite loss, 13–32 for constipation, and 6–19 for diarrhea) was in line for nausea/vomiting and diarrhea but higher for appetite loss and constipation then in our study [20,21,22,23]. Moreover, QoL was also lower when appetite loss and nausea/vomiting occurred concurrently, compared to patients unaffected by these symptoms [24, 25]. Moreover, the difference in global QoL between patients with clinically relevant nutritional problems and no nutritional problems is considered medium, while the difference between clinically and not clinically relevant nutritional problems is small, according to Cocks et al. [26].
In our study, nutritional care needs were also associated with lower QoL which is in line with the results of 18 qualitative studies described in the review of Wheelwright et al. [27]. A study in patients with advanced cancer showed that these patients often seek information regarding nutrition hoping to restore their QoL [28]. Moreover, a study performed in cancer patients undergoing chemotherapy further affirms our findings [29] showing a lower QoL in patients needing nutritional counseling compared to patients who did not need it.
Only preliminary studies have shown that nutritional support may be associated with beneficial effects, i.e., prevented bedsores [12], improved performance status [13] in the very advanced cancer patients but these studies have not specifically looked at QoL. The intervention consisted of providing individualized and tailored nutritional support to meet or exceed the energy and protein requirements. Besides nutritional advice to improve nutritional intake, dietitians may also play an important role in supporting psychosocial consequences of nutritional problems of patients and their informal caregivers especially when emotions lead to conflicts in the patient-informal caregiver relationship. In a pilot randomized controlled trial [30], advanced cancer patients and family caregivers were randomized either to receive 2–3 h of direct dietitian contact time over a 4–6-week period, or to the control group receiving only usual care. During the intervention, issues with nutrition impact symptoms and food or eating-related psychosocial concerns were addressed through nutrition counseling, with a focus on improving nutrition-related communication between the dyads. Results showed improvement in quality of life, eating-related distress, and eating-related enjoyment in a subgroup of patients. However, these preliminary results should be interpreted with caution because compliance in this pilot study was poor; of the 89 eligible patients, 42 were randomized and only 20 finished the 5-week assessment.
The present work covers a novel topic of research showing that gastrointestinal problems (both severe and less severe) and nutritional care needs are independently associated with lower QoL. These findings highlight the importance of addressing gastrointestinal problems as a standard part of daily care for advanced cancer patients in order to optimize symptom management probably by a combination of nutritional care, pharmacological and psychosocial interventions.
Some limitations of this study need to be addressed. First, although the response rate was high (65%), generalizability of our results may be limited because compared to all patients who died of cancer in the Netherlands, patients in our study were more often male, younger, and more likely to have been diagnosed with prostate or breast cancer. Also, patients with worse health status might be less often included in our study (selection bias), leading to a potential overestimation of QoL and underestimation of symptoms [31]. Second, due to the cross-sectional character of the study, this study cannot investigate causality. It is possible that the observed associations of gastrointestinal problems, lack of nutritional care, and nutritional care needs with QoL might be bidirectional. Third, some residual confounding is to be expected. Studies show that weight loss, physical function, physical activity, and systemic inflammatory response in patients with advanced cancer may have an effect on QoL and be associated with gastrointestinal problems [32, 33]. Unfortunately, no information about these factors was available.
Future research should further investigate the relationship between gastrointestinal problems, nutritional care, and nutritional care needs with QoL in a longitudinal setting, including all relevant information. Next, specifically the effect of symptom management strategies for gastrointestinal problems such as nutritional care (e.g., diet modifications), but also pharmacological and psychosocial interventions for nutritional issues, should be investigated in prospective randomized trials, as these problems are of paramount importance for the QoL of patients with advanced cancer.
Conclusion
More than half of all patients with advanced cancer experience gastrointestinal problems, while only few patients receive nutritional care. These gastrointestinal problems, nutritional care needs, and received nutritional care are associated with lower quality of life. More prospective cohort studies and randomized studies are needed to clarify the role of nutritional counseling on gastrointestinal problems, psychosocial well-being, and QoL in patients with incurable cancer.
References
Cancer today. http://gco.iarc.fr/today/home. Accessed 10 Feb 2021
IKNL, Incidence, number. Available from: https://iknl.nl/nkr-cijfers. Accessed 15 Mar 2021
Fransen H (2020) Advanced cancer in numbers “Uitgezaaide kanker in beeld”. IKNL, Utrecht
Haun MW, Estel S, Rücker G et al (2017) Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev 2017(6):CD011129. https://doi.org/10.1002/14651858.CD011129.pub2
Kaasa S, Loge JH, Aapro M et al (2018) Integration of oncology and palliative care: a Lancet Oncology Commission. Lancet Oncol 19:e588–e653. https://doi.org/10.1016/S1470-2045(18)30415-7
Teunissen SCCM, Wesker W, Kruitwagen C et al (2007) Symptom prevalence in patients with incurable cancer: a systematic review. J Pain Symptom Manage 34:94–104. https://doi.org/10.1016/j.jpainsymman.2006.10.015
Cramarossa G, Chow E, Zhang L et al (2013) Predictive factors for overall quality of life in patients with advanced cancer. Support Care Cancer 21:1709–1716. https://doi.org/10.1007/s00520-013-1717-7
van den Beuken-van Everdingen MHJ, de Rijke JM, Kessels AG et al (2009) Quality of life and non-pain symptoms in patients with cancer. J Pain Symptom Manage 38:216–233. https://doi.org/10.1016/j.jpainsymman.2008.08.014
Amano K, Maeda I, Morita T et al (2016) Need for nutritional support, eating-related distress and experience of terminally ill patients with cancer: a survey in an inpatient hospice. BMJ Support Palliat Care 6:373–376. https://doi.org/10.1136/bmjspcare-2014-000783
Tchekmedyian NS, Zahyna D, Halpert C, Heber D (1992) Clinical aspects of nutrition in advanced cancer. Oncology 49(Suppl 2):3–7. https://doi.org/10.1159/000227118
Amano K, Baracos VE, Hopkinson JB (2019) Integration of palliative, supportive, and nutritional care to alleviate eating-related distress among advanced cancer patients with cachexia and their family members. Crit Rev Oncol Hematol 143:117–123. https://doi.org/10.1016/j.critrevonc.2019.08.006
Amano K, Morita T, Baba M et al (2013) Effect of nutritional support on terminally ill patients with cancer in a palliative care unit. Am J Hosp Palliat Care 30:730–733. https://doi.org/10.1177/1049909112469273
Amano K, Maeda I, Ishiki H et al (2016) A feasibility study to investigate the effect of nutritional support for advanced cancer patients in an inpatient hospice in Japan. Palliat Med Hosp Care - Open J 2:37–45
van Roij J, Zijlstra M, Ham L et al (2020) Prospective cohort study of patients with advanced cancer and their relatives on the experienced quality of care and life (eQuiPe study): a study protocol. BMC Palliat Care 19:139. https://doi.org/10.1186/s12904-020-00642-w
van de Poll-Franse LV, Horevoorts N, Schoormans D et al (2022) Measuring clinical, biological, and behavioral variables to elucidate trajectories of patient-reported outcomes: the PROFILES registry. J Natl Cancer Inst 114(6):800–807. https://doi.org/10.1093/jnci/djac047
Aaronson NK, Ahmedzai S, Bergman B et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376. https://doi.org/10.1093/jnci/85.5.365
Giesinger JM, Loth FLC, Aaronson NK et al (2020) Thresholds for clinical importance were established to improve interpretation of the EORTC QLQ-C30 in clinical practice and research. J Clin Epidemiol 118:1–8. https://doi.org/10.1016/j.jclinepi.2019.10.003
Osse BHP, Vernooij MJFJ, Schadé E, Grol RPTM (2004) Towards a new clinical tool for needs assessment in the palliative care of cancer patients: the PNPC instrument. J Pain Symptom Manage 28:329–341. https://doi.org/10.1016/j.jpainsymman.2004.01.010
Cramarossa G, Zeng L, Zhang L et al (2014) Predictive factors of overall quality of life in advanced cancer patients using EORTC QLQ-C30. Expert Rev Pharmacoecon Outcomes Res 14:139–146. https://doi.org/10.1586/14737167.2014.864560
Augustussen M, Pedersen ML, Hounsgaard L et al (2018) Development of health-related quality of life and symptoms in patients with advanced cancer in Greenland. Eur J Cancer Care (Engl) 27:e12843. https://doi.org/10.1111/ecc.12843
Iwase S, Kawaguchi T, Tokoro A et al (2015) Assessment of cancer-related fatigue, pain, and quality of life in cancer patients at palliative care team referral: a multicenter observational study (JORTC PAL-09). PloS One 10:e0134022. https://doi.org/10.1371/journal.pone.0134022
Lee CK, Novello S, Rydén A et al (2018) Patient-reported symptoms and impact of treatment with osimertinib versus chemotherapy in advanced non-small-cell lung cancer: the AURA3 trial. J Clin Oncol 36:1853–1860. https://doi.org/10.1200/JCO.2017.77.2293
Leighl NB, Karaseva N, Nakagawa K et al (2020) Patient-reported outcomes from FLAURA: osimertinib versus erlotinib or gefitinib in patients with EGFR-mutated advanced non-small-cell lung cancer. Eur J Cancer 1990 125:49–57. https://doi.org/10.1016/j.ejca.2019.11.006
Barajas Galindo DE, Vidal-Casariego A, Calleja-Fernández A et al (2017) Appetite disorders in cancer patients: impact on nutritional status and quality of life. Appetite 114:23–27. https://doi.org/10.1016/j.appet.2017.03.020
Pirri C, Bayliss E, Trotter J et al (2013) Nausea still the poor relation in antiemetic therapy? The impact on cancer patients’ quality of life and psychological adjustment of nausea, vomiting and appetite loss, individually and concurrently as part of a symptom cluster. Support Care Cancer 21:735–748. https://doi.org/10.1007/s00520-012-1574-9
Cocks K, King MT, Velikova G et al (2021) Evidence-based guidelines for interpreting change scores for the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. Eur J Cancer 48(11):1713–1721. https://doi.org/10.1016/j.ejca.2012.02.059
Wheelwright SJ, Darlington A-S, Hopkinson JB et al (2016) A systematic review to establish health-related quality-of-life domains for intervention targets in cancer cachexia. BMJ Support Palliat Care 6:307–314. https://doi.org/10.1136/bmjspcare-2014-000680
Pyo J, Ock M, Lee M et al (2021) Unmet needs related to the quality of life of advanced cancer patients in Korea: a qualitative study. BMC Palliat Care 20:58. https://doi.org/10.1186/s12904-021-00749-8
Prevost V, Grach M-C (2012) Nutritional support and quality of life in cancer patients undergoing palliative care. Eur J Cancer Care (Engl) 21:581–590. https://doi.org/10.1111/j.1365-2354.2012.01363.x
Molassiotis A, Brown T, Cheng HL et al (2021) The effects of a family-centered psychosocial-based nutrition intervention in patients with advanced cancer: the PiCNIC2 pilot randomised controlled trial. Nutr J 20:2. https://doi.org/10.1186/s12937-020-00657-2
de Rooij BH, Ezendam NPM, Mols F et al (2018) Cancer survivors not participating in observational patient-reported outcome studies have a lower survival compared to participants: the population-based PROFILES registry. Qual Life Res 27:3313–3324. https://doi.org/10.1007/s11136-018-1979-0
Daly LE, Dolan RD, Power DG et al (2020) Determinants of quality of life in patients with incurable cancer. Cancer 126:2872–2882. https://doi.org/10.1002/cncr.32824
Dittus KL, Gramling RE, Ades PA (2017) Exercise interventions for individuals with advanced cancer: a systematic review. Prev Med 104:124–132. https://doi.org/10.1016/j.ypmed.2017.07.015
Acknowledgements
We thank all patients for their time and effort in participating in our study while being in an uncertain situation. We also want to thank the participating hospitals for recruiting and informing patients and relatives about the eQuiPe study.
Data availability
Since 2011, PROFILES registry data is freely available according to the FAIR (Findable, Accessible, Interoperable, Reusable) data principles for non-commercial (international) scientific research, subject only to privacy and confidentiality restrictions. The datasets analyzed during the current study are available through Questacy (DDI 3.x XML) and can be accessed by our website (www.profilesregistry.nl). In order to arrange optimal long-term data warehousing and dissemination, we follow the quality guidelines that are formulated in the “Data Seal of Approval” (www.datasealofapproval.org) document, developed by Data Archiving and Networked Services (DANS). The data reported in this manuscript will be made available when the eQuiPe study is completed.
Funding
The eQuiPe study is funded by the Roparun Foundation.
Author information
Authors and Affiliations
Contributions
SP, NL, SE, SB, LP, and NR were involved in the study design. SP drafted the manuscript and performed the statistical analysis. All authors reviewed the manuscript and gave final approval of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. The study was reviewed by the Medical Research Ethics Committee of the Antoni van Leeuwenhoek hospital in the Netherlands (METC17.1491).
Consent to participate
Written informed consent was obtained from all individual participants included in the study.
Consent for publication
Written informed consent was obtained from all individual participants included in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Paschos, S., Lize, N., Eussen, S. et al. Are gastrointestinal problems, nutritional care, and nutritional care needs associated with quality of life in patients with advanced cancer? Results of the observational eQuiPe study. Support Care Cancer 31, 189 (2023). https://doi.org/10.1007/s00520-023-07646-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-023-07646-1